
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Search
- Page Path
- HOME > Search
- Lifestyle
- Associations of Ultra-Processed Food Intake with Body Fat and Skeletal Muscle Mass by Sociodemographic Factors
- Sukyoung Jung, Jaehee Seo, Jee Young Kim, Sohyun Park
- Received September 19, 2023 Accepted November 7, 2023 Published online February 2, 2024
- DOI: https://doi.org/10.4093/dmj.2023.0335 [Epub ahead of print]
- 1,247 View
- 76 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
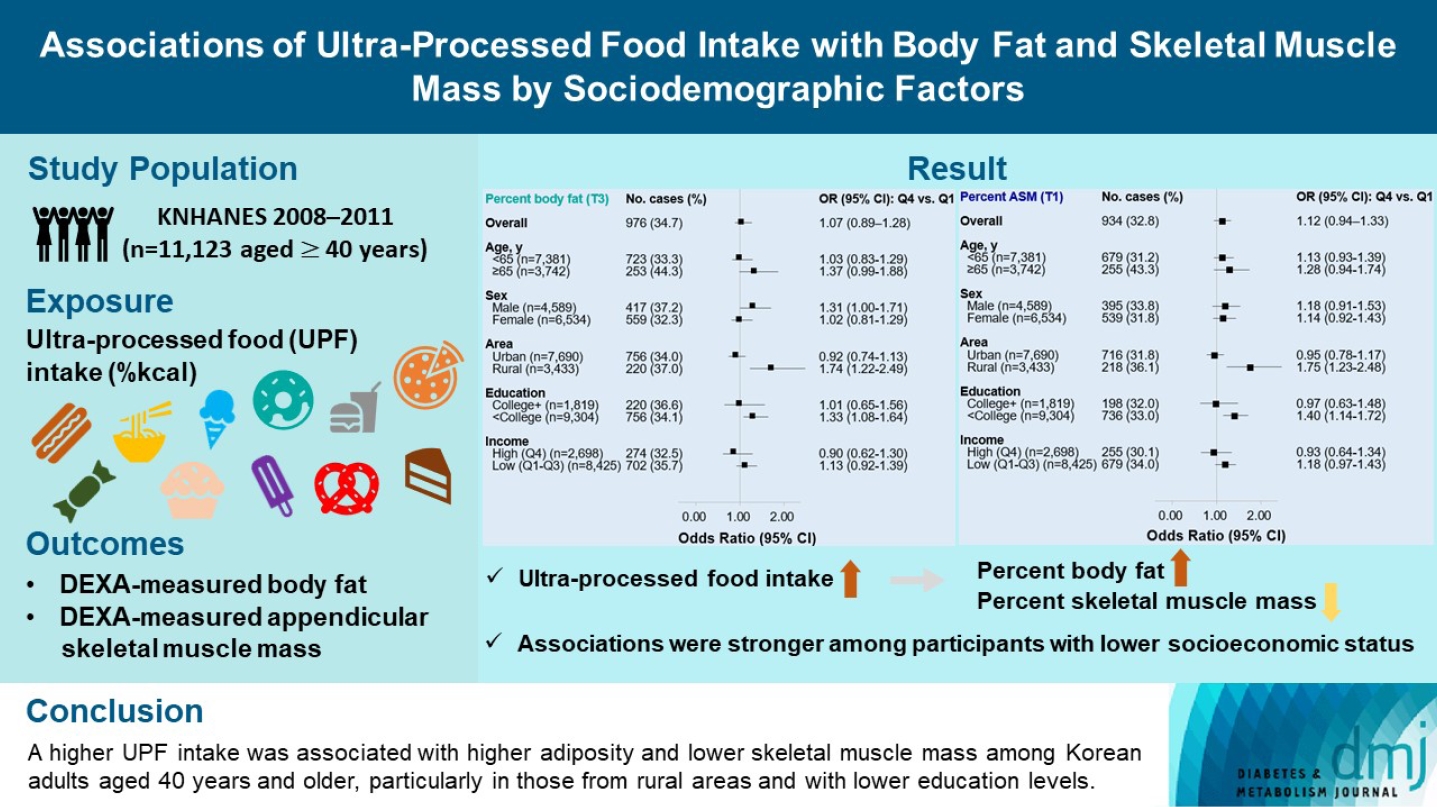
The effects of excessive ultra-processed food (UPF) consumption on body composition measures or sociodemographic disparities are understudied in Korea. We aimed to investigate the association of UPF intake with percent body fat (PBF) and percent appendicular skeletal muscle mass (PASM) by sociodemographic status in adults.
Methods
This study used data from the Korea National Health and Nutrition Examination Survey 2008–2011 (n=11,123 aged ≥40 years). We used a NOVA system to classify all foods reported in a 24-hour dietary recall, and the percentage of energy intake (%kcal) from UPFs was estimated. PBF and PASM were measured by dual-energy X-ray absorptiometry. Tertile (T) 3 of PBF indicated adiposity and T1 of PASM indicated low skeletal muscle mass, respectively. Multinomial logistic regression models were used to estimate odds ratios (OR) with 95% confidence interval (CI) after adjusting covariates.
Results
UPF intake was positively associated with PBF-defined adiposity (ORper 10% increase, 1.04; 95% CI, 1.002 to 1.08) and low PASM (ORper 10% increase, 1.05; 95% CI, 1.01 to 1.09). These associations were stronger in rural residents (PBF: ORper 10% increase, 1.14; 95% CI, 1.06 to 1.23; PASM: ORper 10% increase, 1.15; 95% CI, 1.07 to 1.23) and not college graduates (PBF: ORper 10% increase, 1.06; 95% CI, 1.02 to 1.11; PASM: ORper 10% increase, 1.07; 95% CI, 1.03 to 1.12) than their counterparts.
Conclusion
A higher UPF intake was associated with higher adiposity and lower skeletal muscle mass among Korean adults aged 40 years and older, particularly in those from rural areas and with lower education levels.
- Complications
- Association of Muscle Mass Loss with Diabetes Development in Liver Transplantation Recipients
- Sejeong Lee, Minyoung Lee, Young-Eun Kim, Hae Kyung Kim, Sook Jung Lee, Jiwon Kim, Yurim Yang, Chul Hoon Kim, Hyangkyu Lee, Dong Jin Joo, Myoung Soo Kim, Eun Seok Kang
- Diabetes Metab J. 2024;48(1):146-156. Published online January 3, 2024
- DOI: https://doi.org/10.4093/dmj.2022.0100

- 936 View
- 120 Download
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Post-transplant diabetes mellitus (PTDM) is one of the most significant complications after transplantation. Patients with end-stage liver diseases requiring transplantation are prone to sarcopenia, but the association between sarcopenia and PTDM remains to be elucidated. We aimed to investigate the effect of postoperative muscle mass loss on PTDM development.
Methods
A total of 500 patients who underwent liver transplantation at a tertiary care hospital between 2005 and 2020 were included. Skeletal muscle area at the level of the L3–L5 vertebrae was measured using computed tomography scans performed before and 1 year after the transplantation. The associations between the change in the muscle area after the transplantation and the incidence of PTDM was investigated using a Cox proportional hazard model.
Results
During the follow-up period (median, 4.9 years), PTDM occurred in 165 patients (33%). The muscle mass loss was greater in patients who developed PTDM than in those without PTDM. Muscle depletion significantly increased risk of developing PTDM after adjustment for other confounding factors (hazard ratio, 1.50; 95% confidence interval, 1.23 to 1.84; P=0.001). Of the 357 subjects who had muscle mass loss, 124 (34.7%) developed PTDM, whereas of the 143 patients in the muscle mass maintenance group, 41 (28.7%) developed PTDM. The cumulative incidence of PTDM was significantly higher in patients with muscle loss than in patients without muscle loss (P=0.034).
Conclusion
Muscle depletion after liver transplantation is associated with increased risk of PTDM development.
- Metabolic Risk/Epidemiology
- Association of Myosteatosis with Nonalcoholic Fatty Liver Disease, Severity, and Liver Fibrosis Using Visual Muscular Quality Map in Computed Tomography
- Hwi Seung Kim, Jiwoo Lee, Eun Hee Kim, Min Jung Lee, In Young Bae, Woo Je Lee, Joong-Yeol Park, Hong-Kyu Kim, Chang Hee Jung
- Diabetes Metab J. 2023;47(1):104-117. Published online January 26, 2023
- DOI: https://doi.org/10.4093/dmj.2022.0081
- 3,244 View
- 176 Download
- 7 Web of Science
- 6 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
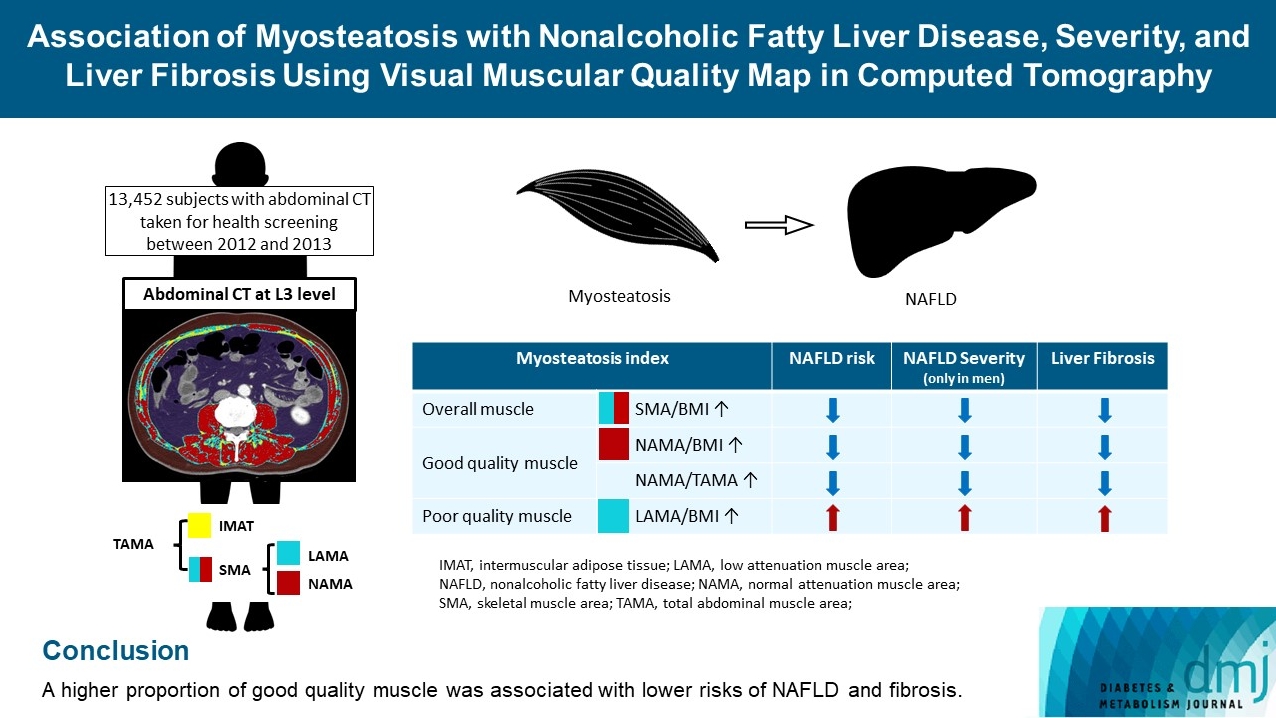
The association of myosteatosis measured using visual muscular quality map in computed tomography (CT) with nonalcoholic fatty liver disease (NAFLD), its severity, and fibrosis was analyzed in a large population.
Methods
Subjects (n=13,452) with abdominal CT between 2012 and 2013 were measured total abdominal muscle area (TAMA) at L3 level. TAMA was segmented into intramuscular adipose tissue and skeletal muscle area (SMA), which was further classified into normal attenuation muscle area (NAMA) and low attenuation muscle area (LAMA). The following variables were adopted as indicators of myosteatosis: SMA/body mass index (BMI), NAMA/BMI, NAMA/TAMA, and LAMA/BMI. NAFLD and its severity were assessed by ultrasonography, and liver fibrosis was measured by calculating the NAFLD fibrosis score (NFS) and fibrosis-4 index (FIB-4) scores.
Results
According to multiple logistic regression analyses, as quartiles of SMA/BMI, NAMA/BMI, and NAMA/TAMA increased, the odds ratios (ORs) for NAFLD decreased in each sex (P for trend <0.001 for all). The ORs of moderate/severe NAFLD were significantly higher in the Q1 group than in the Q4 group for SMA/BMI, NAMA/BMI, and NAMA/TAMA in men. The ORs of intermediate/high liver fibrosis scores assessed by NFS and FIB-4 scores increased linearly with decreasing quartiles for SMA/BMI, NAMA/BMI, and NAMA/TAMA in each sex (P for trend <0.001 for all). Conversely, the risk for NAFLD and fibrosis were positively associated with LAMA/BMI quartiles in each sex (P for trend <0.001 for all).
Conclusion
A higher proportion of good quality muscle was associated with lower risks of NAFLD and fibrosis. -
Citations
Citations to this article as recorded by
- Association of Myosteatosis with Nonalcoholic Fatty Liver Disease, Severity, and Liver Fibrosis Using Visual Muscular Quality Map in Computed Tomography (Diabetes Metab J 2023;47:104-17)
Hwi Seung Kim, Hong-Kyu Kim, Chang Hee Jung
Diabetes & Metabolism Journal.2023; 47(2): 304. CrossRef - Association of Myosteatosis with Nonalcoholic Fatty Liver Disease, Severity, and Liver Fibrosis Using Visual Muscular Quality Map in Computed Tomography (Diabetes Metab J 2023;47:104-17)
Eun Roh
Diabetes & Metabolism Journal.2023; 47(2): 301. CrossRef - Sarcopenia, a condition shared by various diseases: can we alleviate or delay the progression?
Giovanni Tarantino, Gaia Sinatti, Vincenzo Citro, Silvano Santini, Clara Balsano
Internal and Emergency Medicine.2023; 18(7): 1887. CrossRef - Association of Visceral Fat Obesity, Sarcopenia, and Myosteatosis with Non-Alcoholic Fatty Liver Disease without Obesity
Hong-Kyu Kim, Sung-Jin Bae, Min Jung Lee, Eun Hee Kim, Hana Park, Hwi Seung Kim, Yun Kyung Cho, Chang Hee Jung, Woo Je Lee, Jaewon Choe
Clinical and Molecular Hepatology.2023; 29(4): 987. CrossRef - Current view of the surgical anatomy of the anterolateral abdominal wall muscles and their aponeuroses
A.V. Pavlov, A.S. Baranova, A.V. Fedoseyev, A.I. Vvedensky, G.S. Lazutina, N.V. Ovchinnikova, I.V. Bakharev
Operativnaya khirurgiya i klinicheskaya anatomiya (Pirogovskii nauchnyi zhurnal).2023; 7(3): 44. CrossRef - Muscle Fat Content Is Associated with Nonalcoholic Fatty Liver Disease and Liver Fibrosis in Chinese Adults
W. Guo, X. Zhao, D. Cheng, X. Liang, M. Miao, X. Li, J. Lu, N. Xu, Shuang Hu, Qun Zhang
The Journal of nutrition, health and aging.2023; 27(11): 960. CrossRef
- Association of Myosteatosis with Nonalcoholic Fatty Liver Disease, Severity, and Liver Fibrosis Using Visual Muscular Quality Map in Computed Tomography (Diabetes Metab J 2023;47:104-17)
- Metabolic Risk/Epidemiology
- Higher Muscle Mass Protects Women with Gestational Diabetes Mellitus from Progression to Type 2 Diabetes Mellitus
- Yujin Shin, Joon Ho Moon, Tae Jung Oh, Chang Ho Ahn, Jae Hoon Moon, Sung Hee Choi, Hak Chul Jang
- Diabetes Metab J. 2022;46(6):890-900. Published online April 28, 2022
- DOI: https://doi.org/10.4093/dmj.2021.0334
- 4,759 View
- 228 Download
- 2 Web of Science
- 3 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
We evaluated whether postpartum muscle mass affects the risk of type 2 diabetes mellitus (T2DM) in Korean women with gestational diabetes mellitus (GDM).
Methods
A total of 305 women with GDM (mean age, 34.9 years) was prospectively evaluated for incident prediabetes and T2DM from 2 months after delivery and annually thereafter. Appendicular skeletal muscle mass (ASM) was assessed with bioelectrical impedance analysis at the initial postpartum visit, and ASM, either divided by body mass index (BMI) or squared height, and the absolute ASM were used as muscle mass indices. The risk of incident prediabetes and T2DM was assessed according to tertiles of these indices using a logistic regression model.
Results
After a mean follow-up duration of 3.3 years, the highest ASM/BMI tertile group had a 61% lower risk of incident prediabetes and T2DM compared to the lowest tertile group, and this remained significant after we adjusted for covariates (adjusted odds ratio, 0.37; 95% confidence interval [CI], 0.15 to 0.92; P=0.032). Equivalent findings were observed in normal weight women (BMI <23 kg/m2), but this association was not significant for overweight women (BMI ≥23 kg/m2). Absolute ASM or ASM/height2 was not associated with the risk of postpartum T2DM.
Conclusion
A higher muscle mass, as defined by the ASM/BMI index, was associated with a lower risk of postpartum prediabetes and T2DM in Korean women with GDM. -
Citations
Citations to this article as recorded by- More appendicular lean mass relative to body mass index is associated with lower incident diabetes in middle-aged adults in the CARDIA study
Melanie S. Haines, Aaron Leong, Bianca C. Porneala, Victor W. Zhong, Cora E. Lewis, Pamela J. Schreiner, Karen K. Miller, James B. Meigs, Mercedes R. Carnethon
Nutrition, Metabolism and Cardiovascular Diseases.2023; 33(1): 105. CrossRef - The Association of the Triglyceride and Muscle to Fat Ratio During Early Pregnancy with the Development of Gestational Diabetes Mellitus
Fang Wang, Yuan-Yuan Bao, Kang Yu
Diabetes, Metabolic Syndrome and Obesity.2023; Volume 16: 3187. CrossRef - Correlation of body composition in early pregnancy on gestational diabetes mellitus under different body weights before pregnancy
Li Xintong, Xu Dongmei, Zhang Li, Cao Ruimin, Hao Yide, Cui Lingling, Chen Tingting, Guo Yingying, Li Jiaxin
Frontiers in Endocrinology.2022;[Epub] CrossRef
- More appendicular lean mass relative to body mass index is associated with lower incident diabetes in middle-aged adults in the CARDIA study
- Metabolic Risk/Epidemiology
- Computed Tomography-Derived Myosteatosis and Metabolic Disorders
- Iva Miljkovic, Chantal A. Vella, Matthew Allison
- Diabetes Metab J. 2021;45(4):482-491. Published online July 30, 2021
- DOI: https://doi.org/10.4093/dmj.2020.0277
- 6,213 View
- 236 Download
- 41 Web of Science
- 44 Crossref
-
 Graphical Abstract
Abstract
PDFPubReader ePub
Graphical Abstract
Abstract
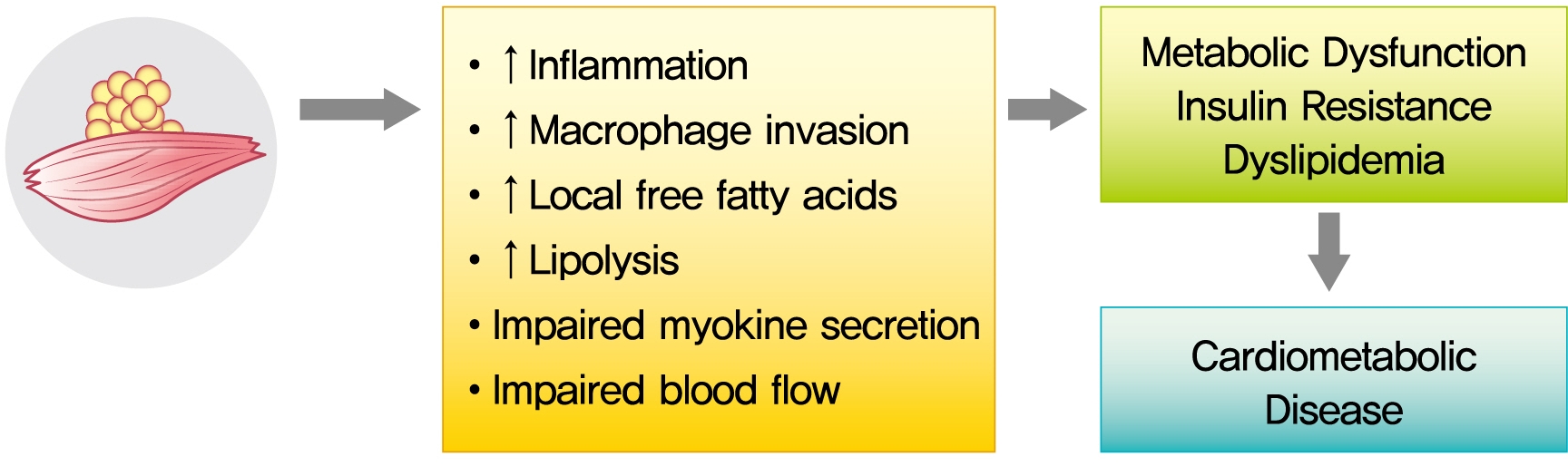
PDFPubReader ePub - The role of ectopic adipose tissue infiltration into skeletal muscle (i.e., myosteatosis) for metabolic disorders has received considerable and increasing attention in the last 10 years. The purpose of this review was to evaluate and summarize existing studies focusing on computed tomography (CT)-derived measures of myosteatosis and metabolic disorders. There is consistent evidence that CT-derived myosteatosis contributes to dysglycemia, insulin resistance, type 2 diabetes mellitus, and inflammation, and, to some extent, dyslipidemia, independent of general obesity, visceral fat, and other relevant risk factors, suggesting that it may serve as a tool for metabolic risk prediction. Identification of which muscles should be examined, and the standardized CT protocols to be employed, are necessary to enhance the applicability of findings from epidemiologic studies of myosteatosis. Additional and longer longitudinal studies are necessary to confirm a role of myosteatosis in the development of type 2 diabetes mellitus, and examine these associations in a variety of muscles across multiple race/ethnic populations. Given the emerging role of myosteatosis in metabolic health, well-designed intervention studies are needed to investigate relevant lifestyle and pharmaceutical approaches.
-
Citations
Citations to this article as recorded by- Association of Muscle Fat Content and Muscle Mass With Impaired Lung Function in Young Adults With Obesity: Evaluation With MRI
Xin Yu, Yan-Hao Huang, You-Zhen Feng, Zhong-Yuan Cheng, Cun-Chuan Wang, Xiang-Ran Cai
Academic Radiology.2024; 31(1): 9. CrossRef - Skeletal muscle alterations indicate poor prognosis in cirrhotic patients: a multicenter cohort study in China
Xin Zeng, Zhi-Wen Shi, Jia-Jun Yu, Li-Fen Wang, Chun-Yan Sun, Yuan-Yuan Luo, Pei-Mei Shi, Yong Lin, Yue-Xiang Chen, Jia Guo, Chun-Qing Zhang, Wei-Fen Xie
Hepatology International.2024; 18(2): 673. CrossRef - Subtype-specific Body Composition and Metabolic Risk in Patients With Primary Aldosteronism
Seung Shin Park, Chang Ho Ahn, Sang Wan Kim, Ji Won Yoon, Jung Hee Kim
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e788. CrossRef - Myosteatosis as a novel predictor of new‐onset diabetes mellitus after kidney transplantation
Takahito Wakamiya, Takuya Fujimoto, Takahito Endo, Shun Nishioka, Naoki Yokoyama, Shimpei Yamashita, Kazuro Kikkawa, Yoji Hyodo, Takeshi Ishimura, Yasuo Kohjimoto, Isao Hara, Masato Fujisawa
International Journal of Urology.2024; 31(1): 39. CrossRef - Predictors of visceral and subcutaneous adipose tissue and muscle density: The ShapeUp! Kids study
Gertraud Maskarinec, Yurii Shvetsov, Michael C. Wong, Devon Cataldi, Jonathan Bennett, Andrea K. Garber, Steven D. Buchthal, Steven B. Heymsfield, John A. Shepherd
Nutrition, Metabolism and Cardiovascular Diseases.2024; 34(3): 799. CrossRef - Association of daily carbohydrate intake with intermuscular adipose tissue in Korean individuals with obesity: a cross-sectional study
Ha-Neul Choi, Young-Seol Kim, Jung-Eun Yim
Nutrition Research and Practice.2024; 18(1): 78. CrossRef - Myosteatosis is associated with poor survival after kidney transplantation: a large retrospective cohort validation
Jie Chen, Yue Li, Chengjie Li, Turun Song
Abdominal Radiology.2024; 49(4): 1210. CrossRef - Regenerative rehabilitation measures to restore tissue function after arsenic exposure
Adam A. Jasper, Kush H. Shah, Helmet Karim, Swathi Gujral, Iva Miljkovic, Caterina Rosano, Aaron Barchowsky, Amrita Sahu
Current Opinion in Biomedical Engineering.2024; 30: 100529. CrossRef - Impact of CFTR modulator therapy on body composition as assessed by thoracic computed tomography: A follow-up study
Víctor Navas-Moreno, Fernando Sebastian-Valles, Víctor Rodríguez-Laval, Carolina Knott-Torcal, Mónica Marazuela, Nuria Sánchez de la Blanca, Jose Alfonso Arranz Martín, Rosa María Girón, Miguel Antonio Sampedro-Núñez
Nutrition.2024; 123: 112425. CrossRef - Myosteatosis predicts postoperative complications and long‐term survival in robotic gastrectomy for gastric cancer: A propensity score analysis
Pingan Ding, Jiaxiang Wu, Haotian Wu, Tongkun Li, Jiaxuan Yang, Li Yang, Honghai Guo, Yuan Tian, Peigang Yang, Lingjiao Meng, Qun Zhao
European Journal of Clinical Investigation.2024;[Epub] CrossRef - A multifaceted and inclusive methodology for the detection of sarcopenia in patients undergoing bariatric surgery: an in-depth analysis of current evidence
Eunhye Seo, Yeongkeun Kwon, Ahmad ALRomi, Mohannad Eledreesi, Sungsoo Park
Reviews in Endocrine and Metabolic Disorders.2024;[Epub] CrossRef - Body Composition at CT and Risk of Future Disease
Michael A. Ohliger
Radiology.2023;[Epub] CrossRef - Association between hypertension and myosteatosis evaluated by abdominal computed tomography
Han Na Jung, Yun Kyung Cho, Hwi Seung Kim, Eun Hee Kim, Min Jung Lee, Woo Je Lee, Hong-Kyu Kim, Chang Hee Jung
Hypertension Research.2023; 46(4): 845. CrossRef - Muscle fat infiltration in chronic kidney disease: a marker related to muscle quality, muscle strength and sarcopenia
Carla Maria Avesani, Aline Miroski de Abreu, Heitor S. Ribeiro, Torkel B. Brismar, Peter Stenvinkel, Alice Sabatino, Bengt Lindholm
Journal of Nephrology.2023; 36(3): 895. CrossRef - Myosteatosis: a potential missing link between hypertension and metabolic disorder in the Asian population
Minyoung Lee, Sungha Park
Hypertension Research.2023; 46(6): 1603. CrossRef - Interplay of skeletal muscle and adipose tissue: sarcopenic obesity
Min Jeong Park, Kyung Mook Choi
Metabolism.2023; 144: 155577. CrossRef - Association between sarcopenic obesity and poor muscle quality based on muscle quality map and abdominal computed tomography
Yun Kyung Cho, Han Na Jung, Eun Hee Kim, Min Jung Lee, Joong‐Yeol Park, Woo Je Lee, Hong‐Kyu Kim, Chang Hee Jung
Obesity.2023; 31(6): 1547. CrossRef - Chest CT opportunistic biomarkers for phenotyping high-risk COVID-19 patients: a retrospective multicentre study
Anna Palmisano, Chiara Gnasso, Alberto Cereda, Davide Vignale, Riccardo Leone, Valeria Nicoletti, Simone Barbieri, Marco Toselli, Francesco Giannini, Marco Loffi, Gianluigi Patelli, Alberto Monello, Gianmarco Iannopollo, Davide Ippolito, Elisabetta Maria
European Radiology.2023; 33(11): 7756. CrossRef - Early menopause and premature ovarian insufficiency may increase the risk of sarcopenia: A systematic review and meta-analysis
Efstathios Divaris, Panagiotis Anagnostis, Nifon K. Gkekas, Evangelia Kouidi, Dimitrios G. Goulis
Maturitas.2023; 175: 107782. CrossRef - The Important Role of Intermuscular Adipose Tissue on Metabolic Changes Interconnecting Obesity, Ageing and Exercise: A Systematic Review
I Gusti Putu Suka Aryana, Ivana Beatrice Paulus, Sanjay Kalra, Dian Daniella, Raden Ayu Tuty Kuswardhani, Ketut Suastika, Sony Wibisono
European Endocrinology.2023; 19(1): 54. CrossRef - Increase in skeletal muscular adiposity and cognitive decline in a biracial cohort of older men and women
Caterina Rosano, Anne Newman, Adam Santanasto, Xiaonan Zhu, Bret Goodpaster, Iva Miljkovic
Journal of the American Geriatrics Society.2023; 71(9): 2759. CrossRef - Myosteatosis and bone marrow adiposity are not associated among postmenopausal women with fragility fractures
Sammy Badr, Héloïse Dapvril, Daniela Lombardo, Huda Khizindar, Claire Martin, Bernard Cortet, Anne Cotten, Julien Paccou
Frontiers in Endocrinology.2023;[Epub] CrossRef - Relationship between trunk intramuscular adipose tissue content and prevalence of metabolic syndrome in middle-aged Japanese men
Noriko I. Tanaka, Masataka Suwa, Hisashi Maeda, Aya Tomita, Takayuki Imoto, Hiroshi Akima
Nutrition.2023; 113: 112083. CrossRef - Sarcopenic obesity and its relation with muscle quality and mortality in patients on chronic hemodialysis
Alice Sabatino, Carla Maria Avesani, Giuseppe Regolisti, Marianna Adinolfi, Giuseppe Benigno, Marco Delsante, Enrico Fiaccadori, Ilaria Gandolfini
Clinical Nutrition.2023; 42(8): 1359. CrossRef - Skeletal muscle adiposity is a novel risk factor for poor cognition in African Caribbean women
Adrianna I. Acevedo‐Fontánez, Ryan K. Cvejkus, Joseph M. Zmuda, Allison L. Kuipers, Emma Barinas‐Mitchell, Akira Sekikawa, Victor Wheeler, Caterina Rosano, Iva Miljkovic
Obesity.2023; 31(9): 2398. CrossRef - Obesity, Sarcopenia and Myosteatosis: Impact on Clinical Outcomes in the Operative Management of Crohn’s Disease
Mark Donnelly, Dorothee Driever, Éanna J Ryan, Jessie A Elliott, John Finnegan, Deirdre McNamara, Ian Murphy, Kevin C Conlon, Paul C Neary, Dara O Kavanagh, James M O’Riordan
Inflammatory Bowel Diseases.2023;[Epub] CrossRef - Meld-sarcopenia score and skeletal muscle density predicts short-term readmission of patients with hepatic encephalopathy
Shuo Yang, Lin Zhang, Qian Jin, Jian Wang, Danli Ma, Jie Gao, Rui Huang
European Journal of Radiology.2023; 169: 111178. CrossRef - Muscle Fat Content Is Associated with Nonalcoholic Fatty Liver Disease and Liver Fibrosis in Chinese Adults
W. Guo, X. Zhao, D. Cheng, X. Liang, M. Miao, X. Li, J. Lu, N. Xu, Shuang Hu, Qun Zhang
The Journal of nutrition, health and aging.2023; 27(11): 960. CrossRef - Association between relative muscle strength and hypertension in middle-aged and older Chinese adults
Jin-hua Luo, Tu-ming Zhang, Lin-lin Yang, Yu-ying Cai, Yu Yang
BMC Public Health.2023;[Epub] CrossRef - Dynapenic Abdominal Obesity as a Risk Factor for Metabolic Syndrome in Individual 50 Years of Age or Older: English Longitudinal Study of Ageing
P.C. Ramírez, R. de Oliveira Máximo, D. Capra de Oliveira, A.F. de Souza, M. Marques Luiz, M. L. Bicigo Delinocente, A. Steptoe, C. de Oliveira, Tiago da Silva Alexandre
The Journal of nutrition, health and aging.2023; 27(12): 1188. CrossRef - Editorial Comment to Myosteatosis as a novel predictor of urinary incontinence after robot‐assisted radical prostatectomy
Nobuhiro Haga, Naotaka Gunge, Hiroshi Matsuzaki, Yu Okabe, Takeshi Miyazaki
International Journal of Urology.2022; 29(1): 40. CrossRef - Ammonia and the Muscle: An Emerging Point of View on Hepatic Encephalopathy
Simone Di Cola, Silvia Nardelli, Lorenzo Ridola, Stefania Gioia, Oliviero Riggio, Manuela Merli
Journal of Clinical Medicine.2022; 11(3): 611. CrossRef - Single skeletal muscle fiber mechanical properties: a muscle quality biomarker of human aging
Jae-Young Lim, Walter R. Frontera
European Journal of Applied Physiology.2022; 122(6): 1383. CrossRef - Sarcopenia in Patients with Cirrhosis after Transjugular Intrahepatic Portosystemic Shunt Placement
Jiacheng Liu, Jinqiang Ma, Chongtu Yang, Manman Chen, Qin Shi, Chen Zhou, Songjiang Huang, Yang Chen, Yingliang Wang, Tongqiang Li, Bin Xiong
Radiology.2022; 303(3): 711. CrossRef - Myosteatosis Significantly Predicts Persistent Dyspnea and Mobility Problems in COVID-19 Survivors
Rebecca De Lorenzo, Anna Palmisano, Antonio Esposito, Chiara Gnasso, Valeria Nicoletti, Riccardo Leone, Davide Vignale, Elisabetta Falbo, Marica Ferrante, Marta Cilla, Cristiano Magnaghi, Sabina Martinenghi, Giordano Vitali, Alessio Molfino, Patrizia Rove
Frontiers in Nutrition.2022;[Epub] CrossRef - Prognostic value of myosteatosis in patients with lung cancer: a systematic review and meta-analysis
Shaofang Feng, Huiwen Mu, Rong Hou, Yunxin Liu, Jianjun Zou, Zheng Zhao, Yubing Zhu
International Journal of Clinical Oncology.2022; 27(7): 1127. CrossRef - Muscle Fat Content Is Strongly Associated With Hyperuricemia: A Cross-Sectional Study in Chinese Adults
Ningxin Chen, Tingting Han, Hongxia Liu, Jie Cao, Wenwen Liu, Didi Zuo, Ting Zhang, Xiucai Lan, Xian Jin, Yurong Weng, Yaomin Hu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Advances in muscle health and nutrition: A toolkit for healthcare professionals
Carla M. Prado, Francesco Landi, Samuel T.H. Chew, Philip J. Atherton, Jeroen Molinger, Tobias Ruck, Maria Cristina Gonzalez
Clinical Nutrition.2022; 41(10): 2244. CrossRef - Factors related to trunk intramuscular adipose tissue content – A comparison of younger and older men
Funa Kitagawa, Madoka Ogawa, Akito Yoshiko, Yoshiharu Oshida, Teruhiko Koike, Hiroshi Akima, Noriko I. Tanaka
Experimental Gerontology.2022; 168: 111922. CrossRef - Association of myosteatosis with various body composition abnormalities and longer length of hospitalization in patients with decompensated cirrhosis
Xiaoyu Wang, Mingyu Sun, Yifan Li, Gaoyue Guo, Wanting Yang, Lihong Mao, Zihan Yu, Yangyang Hui, Xiaofei Fan, Binxin Cui, Kui Jiang, Chao Sun
Frontiers in Nutrition.2022;[Epub] CrossRef - Peripheral bone structure, geometry, and strength and muscle density as derived from peripheral quantitative computed tomography and mortality among rural south Indian older adults
Guru Rajesh Jammy, Robert M. Boudreau, Iva Miljkovic, Pawan Kumar Sharma, Sudhakar Pesara Reddy, Susan L. Greenspan, Anne B. Newman, Jane A. Cauley, Bert B. Little
PLOS Global Public Health.2022; 2(10): e0000333. CrossRef - Muscle fat contents rather than muscle mass determines nonalcoholic steatohepatitis and liver fibrosis in patients with severe obesity
Eugene Han, Mi Kyung Kim, Hye Won Lee, Seungwan Ryu, Hye Soon Kim, Byoung Kuk Jang, Youngsung Suh
Obesity.2022; 30(12): 2440. CrossRef - Sex- and region-specific associations of skeletal muscle mass with metabolic dysfunction-associated fatty liver disease
Pei Xiao, Pu Liang, Panjun Gao, Jinyi Wu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Imaging based body composition profiling and outcomes after oncologic liver surgery
Lorenzo Bernardi, Raffaello Roesel, Filippo Vagelli, Pietro Majno-Hurst, Alessandra Cristaudi
Frontiers in Oncology.2022;[Epub] CrossRef
- Association of Muscle Fat Content and Muscle Mass With Impaired Lung Function in Young Adults With Obesity: Evaluation With MRI
- Basic Research
-
- The Effects of Exercise and Restriction of Sugar-Sweetened Beverages on Muscle Function and Autophagy Regulation in High-Fat High-Sucrose-Fed Obesity Mice
- Didi Zhang, Ji Hyun Lee, Hyung Eun Shin, Seong Eun Kwak, Jun Hyun Bae, Liang Tang, Wook Song
- Diabetes Metab J. 2021;45(5):773-786. Published online March 25, 2021
- DOI: https://doi.org/10.4093/dmj.2020.0157
- 7,091 View
- 252 Download
- 5 Web of Science
- 6 Crossref
-
Graphical Abstract
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
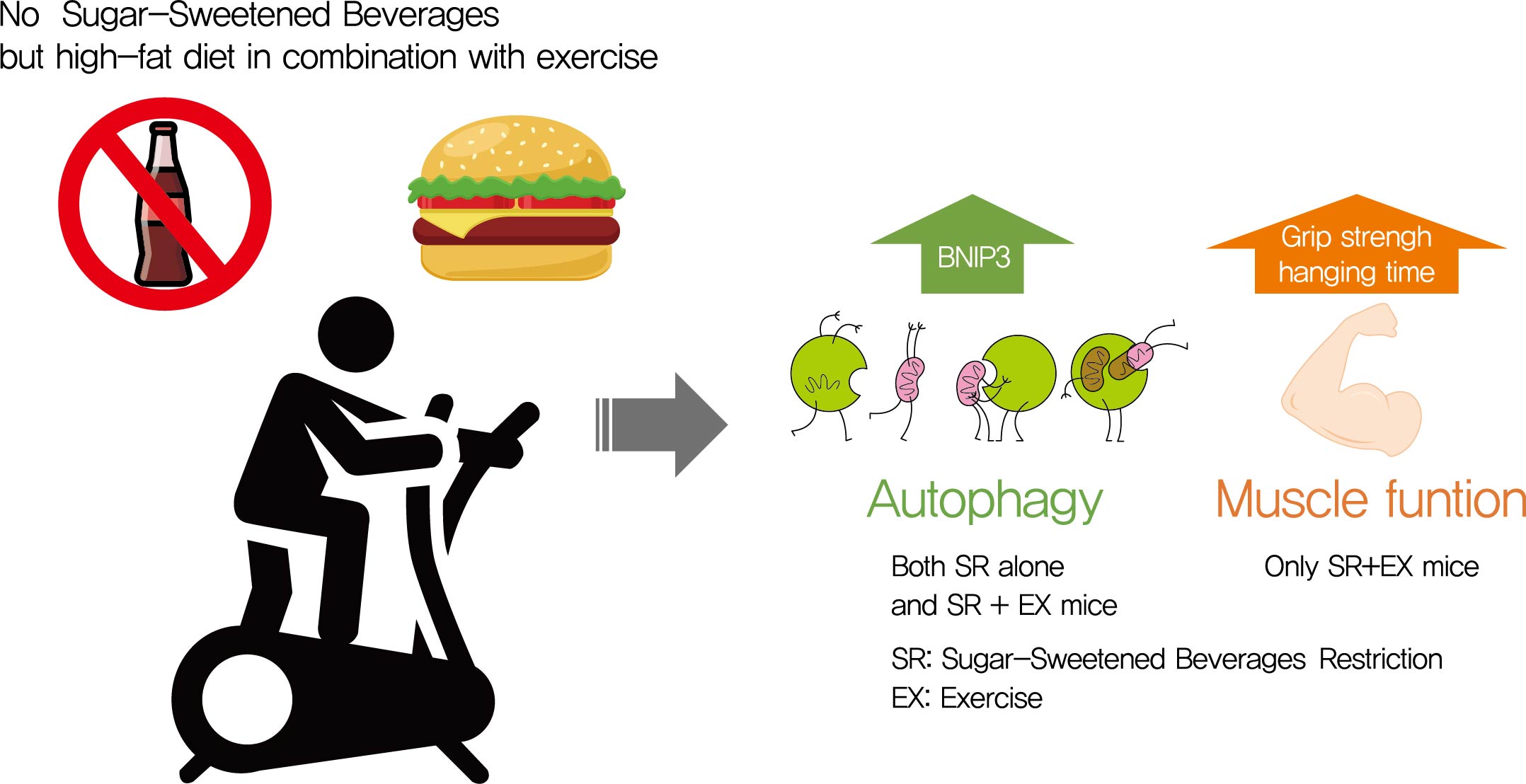
Autophagy maintains muscle mass and healthy skeletal muscles. Several recent studies have associated sugar-sweetened beverage (SSB) consumption with diseases. We investigated whether muscle dysfunction due to obesity could be restored by SSB restriction (SR) alone or in combination with exercise (EX) training.
Methods
Obese mice were subjected to SR combined with treadmill EX. Intraperitoneal glucose tolerance test, grip strength test, hanging time test, and body composition analysis were performed. Triglyceride (TG) and total cholesterol (TC) serum concentrations and TG concentrations in quadriceps muscles were analyzed. Western blot and reverse transcription-quantitative polymerase chain reaction helped analyze autophagy-related protein and mRNA expression, respectively.
Results
SR alone had no significant effect on fasting blood glucose levels, glucose tolerance, and muscle function. However, it had effect on serum TC, serum TG, and BCL2 interacting protein 3 expression. SR+EX improved glucose tolerance and muscle function and increased serum TC utilization than SR alone. SR+EX reduced P62 levels, increased glucose transporter type 4 and peroxisome proliferator-activated receptor γ coactivator-1α protein expression, and improved grip strength relative to the high-fat and high-sucrose liquid (HFHS) group, and this was not observed in the HFHS+EX group.
Conclusion
SR induced mitophagy-related protein expression in quadriceps, without affecting muscle function. And, the combination of SR and EX activated mitophagy-related proteins and improved muscle function. -
Citations
Citations to this article as recorded by- Mitochondrial Dysfunction, Oxidative Stress, and Inter-Organ Miscommunications in T2D Progression
Rajakrishnan Veluthakal, Diana Esparza, Joseph M. Hoolachan, Rekha Balakrishnan, Miwon Ahn, Eunjin Oh, Chathurani S. Jayasena, Debbie C. Thurmond
International Journal of Molecular Sciences.2024; 25(3): 1504. CrossRef - The association between healthy beverage index and sarcopenia in Iranian older adults: a case-control study
Marzieh Mahmoodi, Zainab Shateri, Mehran Nouri, Mohebat Vali, Nasrin Nasimi, Zahra Sohrabi, Mohammad Hossein Dabbaghmanesh, Maede Makhtoomi
BMC Geriatrics.2024;[Epub] CrossRef - Interplay of skeletal muscle and adipose tissue: sarcopenic obesity
Min Jeong Park, Kyung Mook Choi
Metabolism.2023; 144: 155577. CrossRef - Association between sugar-sweetened beverage consumption frequency and muscle strength: results from a sample of Chinese adolescents
Yunjie Zhang, Pan Xu, Yongjing Song, Nan Ma, Jinkui Lu
BMC Public Health.2023;[Epub] CrossRef - Muscle strength and prediabetes progression and regression in middle‐aged and older adults: a prospective cohort study
Shanhu Qiu, Xue Cai, Yang Yuan, Bo Xie, Zilin Sun, Duolao Wang, Tongzhi Wu
Journal of Cachexia, Sarcopenia and Muscle.2022; 13(2): 909. CrossRef - INTENSITY OF FREE RADICAL PROCESSES IN RAT SKELETAL MUSCLES UNDER THE CONDITIONS OF DIFFERENT DIETARY SUPPLY WITH NUTRIENTS
O.M. Voloshchuk, Н.P. Kopylchuk
Fiziolohichnyĭ zhurnal.2022; 68(4): 48. CrossRef
- Mitochondrial Dysfunction, Oxidative Stress, and Inter-Organ Miscommunications in T2D Progression
- Metabolic Risk/Epidemiology
- Age- and Sex-Related Differential Associations between Body Composition and Diabetes Mellitus
- Eun Roh, Soon Young Hwang, Jung A Kim, You-Bin Lee, So-hyeon Hong, Nam Hoon Kim, Ji A Seo, Sin Gon Kim, Nan Hee Kim, Kyung Mook Choi, Sei Hyun Baik, Hye Jin Yoo
- Diabetes Metab J. 2021;45(2):183-194. Published online June 16, 2020
- DOI: https://doi.org/10.4093/dmj.2019.0171
- 7,442 View
- 236 Download
- 3 Web of Science
- 5 Crossref
-
Graphical Abstract
Abstract
PDFSupplementary MaterialPubReader ePub
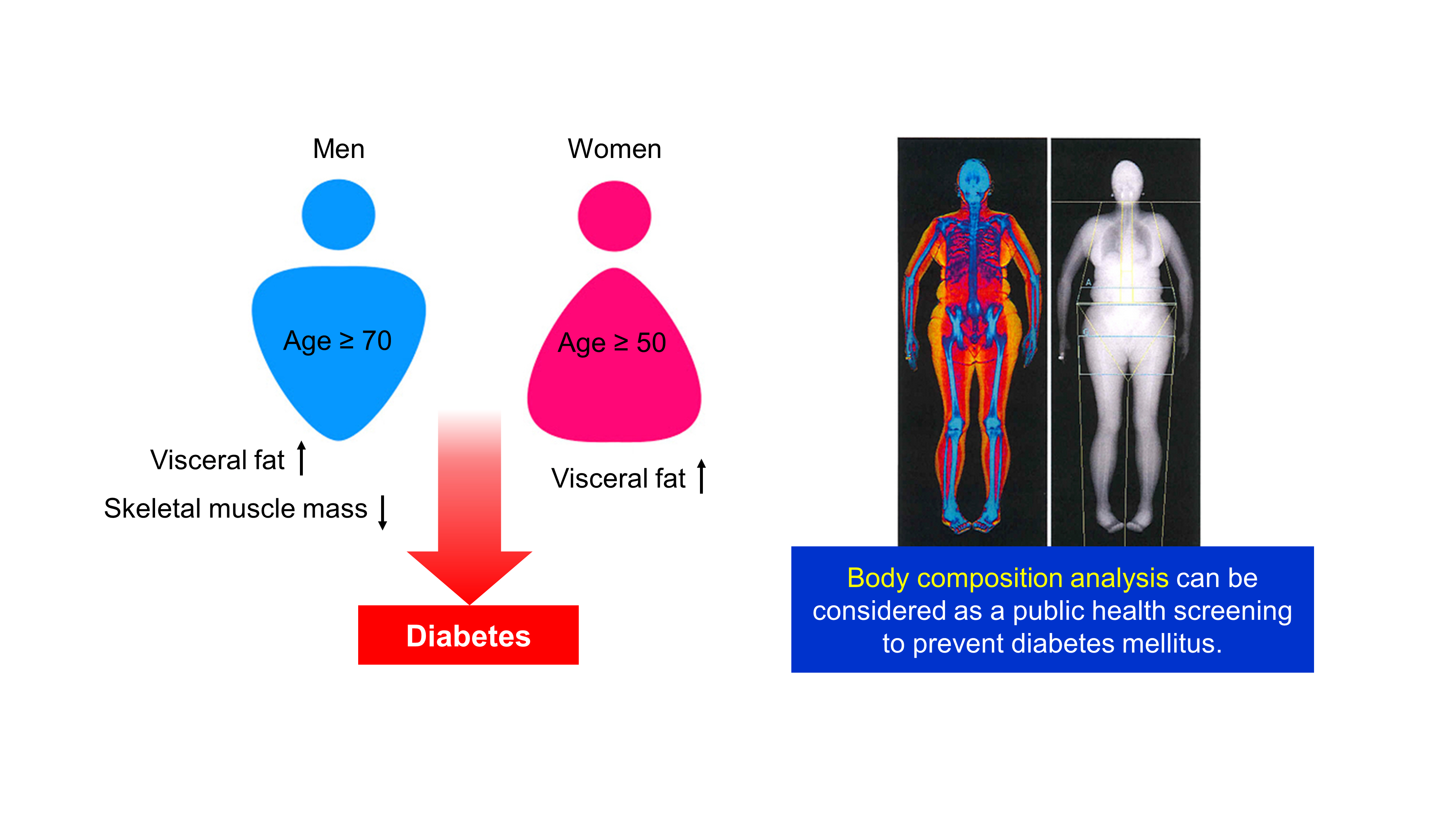
Background The age- and sex-related differences on the impacts of body composition on diabetes mellitus (DM) remain uncertain.
Methods The fourth and fifth Korea National Health and Nutrition Examination Survey included 15,586 subjects over 30 years of age who completed dual-energy X-ray absorptiometry. We conducted a cross-sectional study to investigate whether muscle mass index (MMI), defined as appendicular skeletal muscle divided by body mass index (BMI), and fat mass index (FMI), defined as trunk fat mass divided by BMI, were differently associated with DM according to age and sex.
Results In multivariate logistic regression, the risk for DM significantly increased across quartiles of FMI in men aged ≥70. Meanwhile, MMI showed a protective association with DM in men of the same age. The odds ratios (ORs) for the highest quartile versus the lowest quartile of FMI and MMI were 3.116 (95% confidence interval [CI], 1.405 to 6.914) and 0.295 (95% CI, 0.157 to 0.554), respectively. In women, the ORs of DM was significantly different across FMI quartiles in those over age 50. The highest quartile of FMI exhibited increased ORs of DM in subjects aged 50 to 69 (OR, 1.891; 95% CI, 1.229 to 2.908) and ≥70 (OR, 2.275; 95% CI, 1.103 to 4.69) compared to lowest quartile. However, MMI was not significantly associated with DM in women of all age groups.
Conclusion Both FMI and MMI were independent risk factors for DM in men aged 70 years or more. In women over 50 years, FMI was independently associated with DM. There was no significant association between MMI and DM in women.
-
Citations
Citations to this article as recorded by- Research Progress on Correlation between Body Composition Changes and Disease Pro-gression of Type 2 Diabetes
敏 张
Advances in Clinical Medicine.2024; 14(03): 936. CrossRef - Low Skeletal Muscle Mass Accompanied by Abdominal Obesity Additively Increases the Risk of Incident Type 2 Diabetes
Ji Eun Jun, Seung-Eun Lee, You-Bin Lee, Gyuri Kim, Sang-Man Jin, Jae Hwan Jee, Jae Hyeon Kim
The Journal of Clinical Endocrinology & Metabolism.2023; 108(5): 1173. CrossRef - Is imaging-based muscle quantity associated with risk of diabetes? A meta-analysis of cohort studies
Shanhu Qiu, Xue Cai, Yang Yuan, Bo Xie, Zilin Sun, Tongzhi Wu
Diabetes Research and Clinical Practice.2022; 189: 109939. CrossRef - Whole and segmental body composition changes during mid-follicular and mid-luteal phases of the menstrual cycle in recreationally active young women
Şükran Nazan Koşar, Yasemin Güzel, Mehmet Gören Köse, Ayşe Kin İşler, Tahir Hazır
Annals of Human Biology.2022; 49(2): 124. CrossRef - Body Composition and Diabetes
Hye Jin Yoo
The Journal of Korean Diabetes.2021; 22(4): 238. CrossRef
- Research Progress on Correlation between Body Composition Changes and Disease Pro-gression of Type 2 Diabetes
- Basic Research
- MondoA Is Required for Normal Myogenesis and Regulation of the Skeletal Muscle Glycogen Content in Mice
- Hui Ran, Yao Lu, Qi Zhang, Qiuyue Hu, Junmei Zhao, Kai Wang, Xuemei Tong, Qing Su
- Diabetes Metab J. 2021;45(3):439-451. Published online May 18, 2020
- DOI: https://doi.org/10.4093/dmj.2019.0212
- Correction in: Diabetes Metab J 2021;45(5):797
- 6,162 View
- 191 Download
- 4 Web of Science
- 3 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
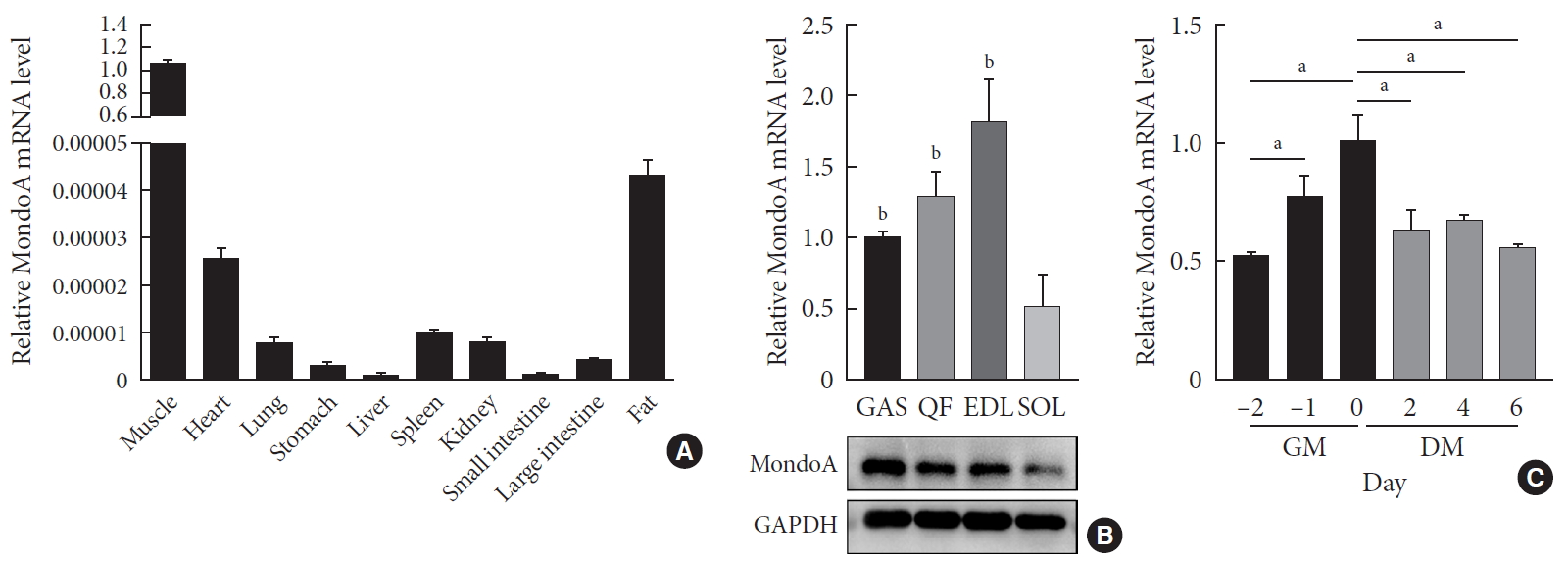
Background Skeletal muscle is the largest tissue in the human body, and it plays a major role in exerting force and maintaining metabolism homeostasis. The role of muscle transcription factors in the regulation of metabolism is not fully understood. MondoA is a glucose-sensing transcription factor that is highly expressed in skeletal muscle. Previous studies suggest that MondoA can influence systemic metabolism homeostasis. However, the function of MondoA in the skeletal muscle remains unclear.
Methods We generated muscle-specific MondoA knockout (MAKO) mice and analyzed the skeletal muscle morphology and glycogen content. Along with skeletal muscle from MAKO mice, C2C12 myocytes transfected with small interfering RNA against MondoA were also used to investigate the role and potential mechanism of MondoA in the development and glycogen metabolism of skeletal muscle.
Results MAKO caused muscle fiber atrophy, reduced the proportion of type II fibers compared to type I fibers, and increased the muscle glycogen level. MondoA knockdown inhibited myoblast proliferation, migration, and differentiation by inhibiting the phosphatase and tensin homolog (PTEN)/phosphoinositide 3-kinase (PI3K)/Akt pathway. Further mechanistic experiments revealed that the increased muscle glycogen in MAKO mice was caused by thioredoxin-interacting protein (TXNIP) downregulation, which led to upregulation of glucose transporter 4 (GLUT4), potentially increasing glucose uptake.
Conclusion MondoA appears to mediate mouse myofiber development, and MondoA decreases the muscle glycogen level. The findings indicate the potential function of MondoA in skeletal muscle, linking the glucose-related transcription factor to myogenesis and skeletal myofiber glycogen metabolism.
-
Citations
Citations to this article as recorded by- The Function of MondoA and ChREBP Nutrient—Sensing Factors in Metabolic Disease
Byungyong Ahn
International Journal of Molecular Sciences.2023; 24(10): 8811. CrossRef - Normal and Neoplastic Growth Suppression by the Extended Myc Network
Edward V. Prochownik, Huabo Wang
Cells.2022; 11(4): 747. CrossRef - The Role of Mondo Family Transcription Factors in Nutrient-Sensing and Obesity
Huiyi Ke, Yu Luan, Siming Wu, Yemin Zhu, Xuemei Tong
Frontiers in Endocrinology.2021;[Epub] CrossRef
- The Function of MondoA and ChREBP Nutrient—Sensing Factors in Metabolic Disease
- Epidemiology
- Longitudinal Changes of Body Composition Phenotypes and Their Association with Incident Type 2 Diabetes Mellitus during a 5-Year Follow-up in Koreans
- Hong-Kyu Kim, Min Jung Lee, Eun-Hee Kim, Sung-Jin Bae, Jaewon Choe, Chul-Hee Kim, Joong-Yeol Park
- Diabetes Metab J. 2019;43(5):627-639. Published online April 19, 2019
- DOI: https://doi.org/10.4093/dmj.2018.0141
- 5,095 View
- 65 Download
- 19 Web of Science
- 19 Crossref
-
Abstract
PDFSupplementary MaterialPubReader
Background To elucidate longitudinal changes of complex body composition phenotypes and their association with incident type 2 diabetes mellitus.
Methods A total of 17,280 (mean age, 48.1±8.2 years) Korean adults who underwent medical check-ups were included. The mean follow-up duration was 5.5±0.5 years. Body compositions were assessed using a bioelectrical impedance analysis. Four body composition phenotypes were defined using the median of appendicular skeletal muscle mass (ASM) index and fat mass index: low muscle/low fat (LM/LF); high muscle (HM)/LF; LM/high fat (HF); and HM/HF groups.
Results Of the individuals in the LM/LF or HM/HF groups, over 60% remained in the same group, and over 30% were moved to the LM/HF group. Most of the LM/HF group remained in this group. In the baseline HM/LF group, approximately 30% stayed in the group, and the remaining individuals transitioned to the three other groups in similar proportions. Incident diabetes was significantly lower in participants who remained in the HM/LF group than those who transitioned to the LM/LF or LM/HF group from the baseline HM/LF group in men. ASM index was significantly associated with a decreased risk for incident diabetes in men regardless of obesity status (adjusted odds ratio [OR], 0.71 per kg/m2; 95% confidence interval [CI], 0.52 to 0.97 in non-obese) (adjusted OR, 0.87; 95% CI, 0.77 to 0.98 in obese) after adjusting for other strong risk factors (e.g., baseline glycosylated hemoglobin and homeostasis model assessment of insulin resistance).
Conclusion Maintenance of ASM may be protective against the development of type 2 diabetes mellitus in men, regardless of obesity status.
-
Citations
Citations to this article as recorded by- Metabolically healthy obese individuals are still at high risk for diabetes: Application of the marginal structural model
Hye Ah Lee, Hyesook Park
Diabetes, Obesity and Metabolism.2024; 26(2): 431. CrossRef - Association of serum gamma-glutamyl transferase with myosteatosis assessed by muscle quality mapping using abdominal computed tomography
Han Na Jung, Yun Kyung Cho, Hwi Seung Kim, Eun Hee Kim, Min Jung Lee, Joong-Yeol Park, Woo Je Lee, Hong-Kyu Kim, Chang Hee Jung
Clinical Imaging.2023; 93: 4. CrossRef - More appendicular lean mass relative to body mass index is associated with lower incident diabetes in middle-aged adults in the CARDIA study
Melanie S. Haines, Aaron Leong, Bianca C. Porneala, Victor W. Zhong, Cora E. Lewis, Pamela J. Schreiner, Karen K. Miller, James B. Meigs, Mercedes R. Carnethon
Nutrition, Metabolism and Cardiovascular Diseases.2023; 33(1): 105. CrossRef - Association between hypertension and myosteatosis evaluated by abdominal computed tomography
Han Na Jung, Yun Kyung Cho, Hwi Seung Kim, Eun Hee Kim, Min Jung Lee, Woo Je Lee, Hong-Kyu Kim, Chang Hee Jung
Hypertension Research.2023; 46(4): 845. CrossRef - Longitudinal association between adiposity changes and lung function deterioration
Youngmok Park, Jiyoung Kim, Young Sam Kim, Ah Young Leem, Jinyeon Jo, Kyungsoo Chung, Moo Suk Park, Sungho Won, Ji Ye Jung
Respiratory Research.2023;[Epub] CrossRef - Relevance of body composition in phenotyping the obesities
Laura Salmón-Gómez, Victoria Catalán, Gema Frühbeck, Javier Gómez-Ambrosi
Reviews in Endocrine and Metabolic Disorders.2023; 24(5): 809. CrossRef - Association of Visceral Fat Obesity, Sarcopenia, and Myosteatosis with Non-Alcoholic Fatty Liver Disease without Obesity
Hong-Kyu Kim, Sung-Jin Bae, Min Jung Lee, Eun Hee Kim, Hana Park, Hwi Seung Kim, Yun Kyung Cho, Chang Hee Jung, Woo Je Lee, Jaewon Choe
Clinical and Molecular Hepatology.2023; 29(4): 987. CrossRef - Association between type 2 diabetes and skeletal muscle quality assessed by abdominal computed tomography scan
Eun Hee Kim, Hong‐Kyu Kim, Min Jung Lee, Sung‐Jin Bae, Kyung Won Kim, Jaewon Choe
Diabetes/Metabolism Research and Reviews.2022;[Epub] CrossRef - Association between fat mass index, fat‐free mass index and hemoglobin A1c in a Japanese population: The Tohoku Medical Megabank Community‐based Cohort Study
Masato Takase, Tomohiro Nakamura, Takumi Hirata, Naho Tsuchiya, Mana Kogure, Fumi Itabashi, Naoki Nakaya, Yohei Hamanaka, Junichi Sugawara, Kichiya Suzuki, Nobuo Fuse, Akira Uruno, Eiichi N Kodama, Shinichi Kuriyama, Ichiro Tsuji, Shigeo Kure, Atsushi Hoz
Journal of Diabetes Investigation.2022; 13(5): 858. CrossRef - Relationship between low skeletal muscle mass, sarcopenic obesity and left ventricular diastolic dysfunction in Korean adults
Jee Hee Yoo, Sung Woon Park, Ji Eun Jun, Sang‐Man Jin, Kyu Yeon Hur, Moon‐Kyu Lee, Mira Kang, Gyuri Kim, Jae Hyeon Kim
Diabetes/Metabolism Research and Reviews.2021;[Epub] CrossRef - Reference Data and T-Scores of Lumbar Skeletal Muscle Area and Its Skeletal Muscle Indices Measured by CT Scan in a Healthy Korean Population
Eun Hee Kim, Kyung Won Kim, Yongbin Shin, Jiwoo Lee, Yousun Ko, Ye-Jee Kim, Min Jung Lee, Sung-Jin Bae, Sung Won Park, Jaewon Choe, Hong-Kyu Kim, Anne Newman
The Journals of Gerontology: Series A.2021; 76(2): 265. CrossRef - Age- and Sex-Related Differential Associations between Body Composition and Diabetes Mellitus
Eun Roh, Soon Young Hwang, Jung A Kim, You-Bin Lee, So-hyeon Hong, Nam Hoon Kim, Ji A Seo, Sin Gon Kim, Nan Hee Kim, Kyung Mook Choi, Sei Hyun Baik, Hye Jin Yoo
Diabetes & Metabolism Journal.2021; 45(2): 183. CrossRef - Cardiometabolic Profile of Different Body Composition Phenotypes in Children
Yi Ying Ong, Jonathan Y Huang, Navin Michael, Suresh Anand Sadananthan, Wen Lun Yuan, Ling-Wei Chen, Neerja Karnani, S Sendhil Velan, Marielle V Fortier, Kok Hian Tan, Peter D Gluckman, Fabian Yap, Yap-Seng Chong, Keith M Godfrey, Mary F-F Chong, Shiao-Yn
The Journal of Clinical Endocrinology & Metabolism.2021; 106(5): e2015. CrossRef - Age-related changes in muscle quality and development of diagnostic cutoff points for myosteatosis in lumbar skeletal muscles measured by CT scan
Hong-Kyu Kim, Kyung Won Kim, Eun Hee Kim, Min Jung Lee, Sung-Jin Bae, Yousun Ko, Taeyoung Park, Yongbin Shin, Ye-Jee Kim, Jaewon Choe
Clinical Nutrition.2021; 40(6): 4022. CrossRef - Comparison of muscle mass and quality between metabolically healthy and unhealthy phenotypes
Hong‐Kyu Kim, Min Jung Lee, Eun Hee Kim, Sung‐Jin Bae, Kyung Won Kim, Chul‐Hee Kim
Obesity.2021; 29(8): 1375. CrossRef - Association between muscle mass and insulin sensitivity independent of detrimental adipose depots in young adults with overweight/obesity
Melanie S. Haines, Laura E. Dichtel, Kate Santoso, Martin Torriani, Karen K. Miller, Miriam A. Bredella
International Journal of Obesity.2020; 44(9): 1851. CrossRef - Impact of Social Jetlag on Weight Change in Adults: Korean National Health and Nutrition Examination Survey 2016–2017
Jin Hwa Kim, Young Sang Lyu, Sang Yong Kim
International Journal of Environmental Research and Public Health.2020; 17(12): 4383. CrossRef - The relationships between sarcopenic skeletal muscle loss during ageing and macronutrient metabolism, obesity and onset of diabetes
Ailsa A. Welch, Richard P. G. Hayhoe, Donnie Cameron
Proceedings of the Nutrition Society.2020; 79(1): 158. CrossRef - Impact of the Dynamic Change of Metabolic Health Status on the Incident Type 2 Diabetes: A Nationwide Population-Based Cohort Study
Jung A Kim, Da Hye Kim, Seon Mee Kim, Yong Gyu Park, Nan Hee Kim, Sei Hyun Baik, Kyung Mook Choi, Kyungdo Han, Hye Jin Yoo
Endocrinology and Metabolism.2019; 34(4): 406. CrossRef
- Metabolically healthy obese individuals are still at high risk for diabetes: Application of the marginal structural model
- Obesity and Metabolic Syndrome
- Proportion and Characteristics of the Subjects with Low Muscle Mass and Abdominal Obesity among the Newly Diagnosed and Drug-Naïve Type 2 Diabetes Mellitus Patients
- Jung A Kim, Soon Young Hwang, Hye Soo Chung, Nam Hoon Kim, Ji A Seo, Sin Gon Kim, Nan Hee Kim, Kyung Mook Choi, Sei Hyun Baik, Hye Jin Yoo
- Diabetes Metab J. 2019;43(1):105-113. Published online September 28, 2018
- DOI: https://doi.org/10.4093/dmj.2018.0036
- 4,898 View
- 70 Download
- 12 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader
Background Sarcopenic obesity (SO) is a serious public health concern, few studies have examined the clinical implications of SO in newly-diagnosed type 2 diabetes mellitus (T2DM) patients. We evaluated the prevalence of the newly diagnosed, drug-naïve T2DM patients with low muscle mass with abdominal obesity and its association with insulin resistance and other diabetic complications.
Methods We classified 233 drug-naïve T2DM subjects into four groups according to abdominal obesity (waist circumference ≥90 cm in men and ≥85 cm in women) and low muscle mass status (appendicular skeletal muscle <7.0 kg/m2 for men and <5.4 kg/m2 for women).
Results The proportion of the subjects with low muscle mass and abdominal obesity among the newly diagnosed, drug-naïve T2DM patients was 8.2%. Homeostasis model assessment of insulin resistance (HOMA-IR) increased linearly according to body composition group from normal to abdominal obesity to both low muscle mass and abdominal obesity. The multiple logistic regression analysis indicated that subjects with low muscle mass and abdominal obesity (odds ratio [OR], 9.39; 95% confidence interval [CI], 2.41 to 36.56) showed a higher risk for insulin resistance, defined as HOMA-IR ≥3, than those with abdominal obesity (OR, 5.36; 95% CI, 2.46 to 11.69), even after adjusting for other covariates. However, there were no differences in lipid profiles, microalbuminuria, or various surrogate markers for atherosclerosis among the four groups.
Conclusion Subjects with both low muscle mass and abdominal obesity had a higher risk of insulin resistance than those with low muscle mass or abdominal obesity only.
-
Citations
Citations to this article as recorded by- Clinical observation on acupuncture for 80 patients with abdominal obesity in Germany: based on the theory of unblocking and regulating the Belt Vessel
Yuanyuan Li, Hang Xiong, Shuhui Ma, Jingzhang Dai
Journal of Acupuncture and Tuina Science.2023; 21(2): 137. CrossRef - Waist circumference and end‐stage renal disease based on glycaemic status: National Health Insurance Service data 2009–2018
Yun Kyung Cho, Ji Hye Huh, Shinje Moon, Yoon Jung Kim, Yang‐Hyun Kim, Kyung‐do Han, Jun Goo Kang, Seong Jin Lee, Sung‐Hee Ihm
Journal of Cachexia, Sarcopenia and Muscle.2023; 14(1): 585. CrossRef - Incidence of sarcopenic obesity in older patients with diabetes and association between sarcopenic obesity and higher-level functional capacity: evaluation based on a consensus statement
Satoshi Ida, Ryutaro Kaneko, Kanako Imataka, Kaoru Okubo, Kentaro Azuma, Kazuya Murata
Endocrine Journal.2023; 70(6): 591. CrossRef - A Novel Anthropometric Parameter, Weight-Adjusted Waist Index Represents Sarcopenic Obesity in Newly Diagnosed Type 2 Diabetes Mellitus
Min Jeong Park, Soon Young Hwang, Nam Hoon Kim, Sin Gon Kim, Kyung Mook Choi, Sei Hyun Baik, Hye Jin Yoo
Journal of Obesity & Metabolic Syndrome.2023; 32(2): 130. CrossRef - Prevalence of sarcopenic obesity in patients with diabetes and adverse outcomes: A systematic review and meta-analysis
Yuan-yuan Zhou, Jin-feng Wang, Qian Yao, Qiu-feng Jian, Zhi-peng Luo
Clinical Nutrition ESPEN.2023; 58: 128. CrossRef - The Correlation Between Leg Muscle Mass Index and Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus
Menggege Liu, Qing Zhang, Juan Liu, Huiling Bai, Ping Yang, Xinhua Ye, Xiaoqing Yuan
Diabetes, Metabolic Syndrome and Obesity.2023; Volume 16: 4169. CrossRef - Sarcopenic Obesity with Normal Body Size May Have Higher Insulin Resistance in Elderly Patients with Type 2 Diabetes Mellitus
Tingting Han, Ting Yuan, Xinyue Liang, Ningxin Chen, Jia Song, Xin Zhao, Yurong Weng, Yaomin Hu
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2022; Volume 15: 1197. CrossRef - Relationship between Visceral Adipose Index, Lipid Accumulation Product and Type 2 Diabetes Mellitus
停停 陈
Advances in Clinical Medicine.2022; 12(04): 3350. CrossRef - Assessment of the relationship between prediabetes and low skeletal mass based on blood creatinine level
S. I. Ibragimova, G. O. Nuskabayeva, Z. N. Shalkharova, K. Zh. Sadykova, G. A. Junusbekova, M. Oran
Diabetes mellitus.2022; 25(3): 226. CrossRef - Changes in body composition and low blood urea nitrogen level related to an increase in the prevalence of fatty liver over 20 years: A cross‐sectional study
Yasushi Imamura, Seiichi Mawatari, Kohei Oda, Kotaro Kumagai, Yasunari Hiramine, Akiko Saishoji, Atsuko Kakihara, Mai Nakahara, Manei Oku, Kaori Hosoyamada, Shuji Kanmura, Akihiro Moriuchi, Hironori Miyahara, Akio ido
Hepatology Research.2021; 51(5): 570. CrossRef - Body Composition and Diabetes
Hye Jin Yoo
The Journal of Korean Diabetes.2021; 22(4): 238. CrossRef - Reduced Skeletal Muscle Volume and Increased Skeletal Muscle Fat Deposition Characterize Diabetes in Individuals after Pancreatitis: A Magnetic Resonance Imaging Study
Andre E. Modesto, Juyeon Ko, Charlotte E. Stuart, Sakina H. Bharmal, Jaelim Cho, Maxim S. Petrov
Diseases.2020; 8(3): 25. CrossRef - Low alanine aminotransferase levels predict low muscle strength in older patients with diabetes: A nationwide cross‐sectional study in Korea
Seung Min Chung, Jun Sung Moon, Ji Sung Yoon, Kyu Chang Won, Hyoung Woo Lee
Geriatrics & Gerontology International.2020; 20(4): 271. CrossRef - Association between sarcopenic obesity and higher risk of type 2 diabetes in adults: A systematic review and meta-analysis
Dima Khadra, Leila Itani, Hana Tannir, Dima Kreidieh, Dana El Masri, Marwan El Ghoch
World Journal of Diabetes.2019; 10(5): 311. CrossRef
- Clinical observation on acupuncture for 80 patients with abdominal obesity in Germany: based on the theory of unblocking and regulating the Belt Vessel
- Epidemiology
- Association of Thigh Muscle Mass with Insulin Resistance and Incident Type 2 Diabetes Mellitus in Japanese Americans
- Seung Jin Han, Edward J. Boyko, Soo-Kyung Kim, Wilfred Y. Fujimoto, Steven E. Kahn, Donna L. Leonetti
- Diabetes Metab J. 2018;42(6):488-495. Published online September 5, 2018
- DOI: https://doi.org/10.4093/dmj.2018.0022
- 4,600 View
- 63 Download
- 34 Web of Science
- 34 Crossref
-
Abstract
PDFPubReader
Background Skeletal muscle plays a major role in glucose metabolism. We investigated the association between thigh muscle mass, insulin resistance, and incident type 2 diabetes mellitus (T2DM) risk. In addition, we examined the role of body mass index (BMI) as a potential effect modifier in this association.
Methods This prospective study included 399 Japanese Americans without diabetes (mean age 51.6 years) who at baseline had an estimation of thigh muscle mass by computed tomography and at baseline and after 10 years of follow-up a 75-g oral glucose tolerance test and determination of homeostasis model assessment of insulin resistance (HOMA-IR). We fit regression models to examine the association between thigh muscle area and incidence of T2DM and change in HOMA-IR, both measured over 10 years.
Results Thigh muscle area was inversely associated with future HOMA-IR after adjustment for age, sex, BMI, HOMA-IR, fasting plasma glucose, total abdominal fat area, and thigh subcutaneous fat area at baseline (
P =0.033). The 10-year cumulative incidence of T2DM was 22.1%. A statistically significant interaction between thigh muscle area and BMI was observed, i.e., greater thigh muscle area was associated with lower risk of incident T2DM for subjects at lower levels of BMI, but this association diminished at higher BMI levels.Conclusion Thigh muscle mass area was inversely associated with future insulin resistance. Greater thigh muscle area predicts a lower risk of incident T2DM for leaner Japanese Americans.
-
Citations
Citations to this article as recorded by- Shape phenotype of thigh fat and muscle and risk of major adverse cardiovascular events after fragility hip fracture
Sheen‐Woo Lee, Seung‐Chan Kim, Jeong‐Eun Yi
Journal of Cachexia, Sarcopenia and Muscle.2024; 15(1): 331. CrossRef - CD36 gene variant rs1761667(G/A) as a biomarker in obese type 2 diabetes mellitus cases
Ashwin Kumar Shukla, Amreen Shamsad, Atar Singh Kushwah, Shalini Singh, Kauser Usman, Monisha Banerjee
Egyptian Journal of Medical Human Genetics.2024;[Epub] CrossRef - Association between macro- and microvascular damage and sarcopenia index in individuals with type 2 diabetes mellitus
Hui Xu, Qun-Yan Xiang, Jun-Kun Zhan, Yi Wang, Yan-Jiao Wang, Shuang Li, You-Shuo Liu
Applied Physiology, Nutrition, and Metabolism.2024;[Epub] CrossRef - More appendicular lean mass relative to body mass index is associated with lower incident diabetes in middle-aged adults in the CARDIA study
Melanie S. Haines, Aaron Leong, Bianca C. Porneala, Victor W. Zhong, Cora E. Lewis, Pamela J. Schreiner, Karen K. Miller, James B. Meigs, Mercedes R. Carnethon
Nutrition, Metabolism and Cardiovascular Diseases.2023; 33(1): 105. CrossRef - Involvement of the fecal amino acid profile in a clinical and anthropometric study of Mexican patients with insulin resistance and type 2 diabetes mellitus
Mayra Paloma Macías-Acosta, Lorena Valerdi-Contreras, Ericka Denise Bustos-Angel, Rudy Antonio García-Reyes, Monserrat Alvarez-Zavala, Marisela González-Ávila
Amino Acids.2022; 54(1): 47. CrossRef - Association of serum creatinine levels and risk of type 2 diabetes mellitus in Korea: a case control study
Do Kyeong Song, Young Sun Hong, Yeon-Ah Sung, Hyejin Lee
BMC Endocrine Disorders.2022;[Epub] CrossRef - The Relationship Between Fat-Free Mass and Glucose Metabolism in Children and Adolescents: A Systematic Review and Meta-Analysis
Lijun Wu, Fangfang Chen, Junting Liu, Dongqing Hou, Tao Li, Yiren Chen, Zijun Liao
Frontiers in Pediatrics.2022;[Epub] CrossRef - Is imaging-based muscle quantity associated with risk of diabetes? A meta-analysis of cohort studies
Shanhu Qiu, Xue Cai, Yang Yuan, Bo Xie, Zilin Sun, Tongzhi Wu
Diabetes Research and Clinical Practice.2022; 189: 109939. CrossRef - Effects of Exercise Intervention on Type 2 Diabetes Patients With Abdominal Obesity and Low Thigh Circumference (EXTEND): Study Protocol for a Randomized Controlled Trial
Dan Liu, Ying Zhang, Liang Wu, Jingyi Guo, Xiangtian Yu, Huasheng Yao, Rui Han, Tianshu Ma, Yuchan Zheng, Qiongmei Gao, Qichen Fang, Yan Zhao, Yanan Zhao, Biao Sun, Weiping Jia, Huating Li
Frontiers in Endocrinology.2022;[Epub] CrossRef - Association between diabetic peripheral neuropathy and sarcopenia: A systematic review and meta‐analysis
Thapat Wannarong, Persen Sukpornchairak, Weerakit Naweera, Christopher D. Geiger, Patompong Ungprasert
Geriatrics & Gerontology International.2022; 22(9): 785. CrossRef - Synergistic Interaction between Hyperuricemia and Abdominal Obesity as a Risk Factor for Metabolic Syndrome Components in Korean Population
Min Jin Lee, Ah Reum Khang, Yang Ho Kang, Mi Sook Yun, Dongwon Yi
Diabetes & Metabolism Journal.2022; 46(5): 756. CrossRef - HOMA-IR as a predictor of Health Outcomes in Patients with Metabolic Risk Factors: A Systematic Review and Meta-analysis
José G. González-González, Jorge R. Violante-Cumpa, Miguel Zambrano-Lucio, Erick Burciaga-Jimenez, Patricia L. Castillo-Morales, Mariano Garcia-Campa, Ricardo César Solis, Alejandro D González-Colmenero, René Rodríguez-Gutiérrez
High Blood Pressure & Cardiovascular Prevention.2022; 29(6): 547. CrossRef - Maternal height as a predictor of glucose intolerance in the postpartum and its relationship with maternal pre-gestational weight
Catarina Cidade-Rodrigues, Filipe M. Cunha, Catarina Chaves, Fabiana Castro, Catarina Pereira, Sílvia Paredes, Margarida Silva-Vieira, Anabela Melo, Odete Figueiredo, Cláudia Nogueira, Ana Morgado, Mariana Martinho, Maria C. Almeida, Margarida Almeida
Archives of Gynecology and Obstetrics.2022; 307(2): 601. CrossRef - Correlation of body composition in early pregnancy on gestational diabetes mellitus under different body weights before pregnancy
Li Xintong, Xu Dongmei, Zhang Li, Cao Ruimin, Hao Yide, Cui Lingling, Chen Tingting, Guo Yingying, Li Jiaxin
Frontiers in Endocrinology.2022;[Epub] CrossRef - Relationship between low skeletal muscle mass, sarcopenic obesity and left ventricular diastolic dysfunction in Korean adults
Jee Hee Yoo, Sung Woon Park, Ji Eun Jun, Sang‐Man Jin, Kyu Yeon Hur, Moon‐Kyu Lee, Mira Kang, Gyuri Kim, Jae Hyeon Kim
Diabetes/Metabolism Research and Reviews.2021;[Epub] CrossRef - Skeletal Muscle and Metabolic Health: How Do We Increase Muscle Mass and Function in People with Type 2 Diabetes?
Ebaa Al-Ozairi, Dalal Alsaeed, Dherar Alroudhan, Nia Voase, Amal Hasan, Jason M R Gill, Naveed Sattar, Paul Welsh, Cindy M Gray, Jirapitcha Boonpor, Carlos Celis-Morales, Stuart R Gray
The Journal of Clinical Endocrinology & Metabolism.2021; 106(2): 309. CrossRef - Association of the triglyceride and glucose index with low muscle mass: KNHANES 2008–2011
Jung A. Kim, Soon Young Hwang, Ji Hee Yu, Eun Roh, So-hyeon Hong, You-Bin Lee, Nam Hoon Kim, Hye Jin Yoo, Ji A. Seo, Nan Hee Kim, Sin Gon Kim, Sei Hyun Baik, Kyung Mook Choi
Scientific Reports.2021;[Epub] CrossRef - ADAS-viewer: web-based application for integrative analysis of multi-omics data in Alzheimer’s disease
Seonggyun Han, Jaehang Shin, Hyeim Jung, Jane Ryu, Habtamu Minassie, Kwangsik Nho, Insong Koh, Younghee Lee
npj Systems Biology and Applications.2021;[Epub] CrossRef - Relative associations of abdominal and thigh compositions with cardiometabolic diseases in African Caribbean men
Curtis Tilves, Joseph M. Zmuda, Allison L. Kuipers, Sangeeta Nair, John Jeffrey Carr, James G. Terry, Shyamal Peddada, Victor Wheeler, Iva Miljkovic
Obesity Science & Practice.2021; 7(6): 738. CrossRef - Changes in creatinine‐to‐cystatin C ratio over 4 years, risk of diabetes, and cardiometabolic control: The China Health and Retirement Longitudinal Study
Shanhu Qiu, Xue Cai, Yang Yuan, Bo Xie, Zilin Sun, Tongzhi Wu
Journal of Diabetes.2021; 13(12): 1025. CrossRef - Associations Between Glucose Tolerance, Insulin Secretion, Muscle and Fat Mass in Cystic Fibrosis
Bibi Uhre Nielsen, Daniel Faurholt-Jepsen, Peter Sandor Oturai, Tavs Qvist, Rikke Krogh-Madsen, Terese Lea Katzenstein, James Shaw, Christian Ritz, Tacjana Pressler, Thomas Peter Almdal, Inger Hee Mabuza Mathiesen
Clinical Medicine Insights: Endocrinology and Diabetes.2021; 14: 117955142110382. CrossRef - Total and regional fat‐to‐muscle mass ratio measured by bioelectrical impedance and risk of incident type 2 diabetes
Ningjian Wang, Ying Sun, Haojie Zhang, Chi Chen, Yuying Wang, Jihui Zhang, Fangzhen Xia, Christian Benedict, Xiao Tan, Yingli Lu
Journal of Cachexia, Sarcopenia and Muscle.2021; 12(6): 2154. CrossRef - How was the Diabetes Metabolism Journal added to MEDLINE?
Hye Jin Yoo
Science Editing.2020; 7(2): 201. CrossRef - An update on nutrient modulation in the management of disease-induced muscle wasting: evidence from human studies
Matthew S. Brook, Daniel J. Wilkinson, Philip J. Atherton
Current Opinion in Clinical Nutrition & Metabolic Care.2020; 23(3): 174. CrossRef - The functional nutritional and regulatory activities of calcium supplementation from eggshell for obesity disorders management
Marwa El‐Zeftawy, Samar Abd‐El Mohsen Ali, Sally Salah, Hani S. Hafez
Journal of Food Biochemistry.2020;[Epub] CrossRef - Dose‐response associations between serum creatinine and type 2 diabetes mellitus risk: A Chinese cohort study and meta‐analysis of cohort studies
Pei Qin, Yanmei Lou, Liming Cao, Jing Shi, Gang Tian, Dechen Liu, Qionggui Zhou, Chunmei Guo, Quanman Li, Yang Zhao, Feiyan Liu, Xiaoyan Wu, Ranran Qie, Minghui Han, Shengbing Huang, Ping Zhao, Changyi Wang, Jianping Ma, Xiaolin Peng, Shan Xu, Hongen Chen
Journal of Diabetes.2020; 12(8): 594. CrossRef - Caloric restriction in heart failure: A systematic review
Vittorio Emanuele Bianchi
Clinical Nutrition ESPEN.2020; 38: 50. CrossRef - Association between the Thigh Muscle and Insulin Resistance According to Body Mass Index in Middle-Aged Korean Adults
Ji Eun Heo, Jee-Seon Shim, Hokyou Lee, Hyeon Chang Kim
Diabetes & Metabolism Journal.2020; 44(3): 446. CrossRef - Joint impact of muscle mass and waist circumference on type 2 diabetes in Japanese middle‐aged adults: The Circulatory Risk in Communities Study (CIRCS)
Mikako Yasuoka, Isao Muraki, Hironori Imano, Hiroshige Jinnouchi, Yasuhiko Kubota, Mina Hayama‐Terada, Mitsumasa Umesawa, Kazumasa Yamagishi, Tetsuya Ohira, Akihiko Kitamura, Takeo Okada, Masahiko Kiyama, Hiroyasu Iso
Journal of Diabetes.2020; 12(9): 677. CrossRef - Catch-Up Growth in Children Born Small for Gestational Age Related to Body Composition and Metabolic Risk at Six Years of Age in the UK
M. Loredana Marcovecchio, Samantha Gorman, Laura P.E. Watson, David B. Dunger, Kathryn Beardsall
Hormone Research in Paediatrics.2020; 93(2): 119. CrossRef - Response: Association of Thigh Muscle Mass with Insulin Resistance and Incident Type 2 Diabetes Mellitus in Japanese Americans (Diabetes Metab J 2018;42:488–95)
Seung Jin Han, Edward J. Boyko
Diabetes & Metabolism Journal.2019; 43(1): 125. CrossRef - Berberine chloride ameliorated PI3K/Akt‐p/SIRT‐1/PTEN signaling pathway in insulin resistance syndrome induced in rats
Marwa El‐Zeftawy, Doaa Ghareeb, Eman R. ElBealy, Rasha Saad, Salma Mahmoud, Nihal Elguindy, Attalla F. El‐kott, Mohamed El‐Sayed
Journal of Food Biochemistry.2019;[Epub] CrossRef - Letter: Association of Thigh Muscle Mass with Insulin Resistance and Incident Type 2 Diabetes Mellitus in Japanese Americans (Diabetes Metab J 2018;42:488–95)
Nan Hee Cho, Hye Soon Kim
Diabetes & Metabolism Journal.2019; 43(1): 123. CrossRef - Asian Indians With Prediabetes Have Similar Skeletal Muscle Mass and Function to Those With Type 2 Diabetes
Sucharita Sambashivaiah, Stephen D. R. Harridge, Nidhi Sharma, Sumithra Selvam, Priyanka Rohatgi, Anura V. Kurpad
Frontiers in Nutrition.2019;[Epub] CrossRef
- Shape phenotype of thigh fat and muscle and risk of major adverse cardiovascular events after fragility hip fracture
- Clinical Care/Education
- Hyperglycemia Is Associated with Impaired Muscle Quality in Older Men with Diabetes: The Korean Longitudinal Study on Health and Aging
- Ji Won Yoon, Yong-Chan Ha, Kyoung Min Kim, Jae Hoon Moon, Sung Hee Choi, Soo Lim, Young Joo Park, Jae Young Lim, Ki Woong Kim, Kyong Soo Park, Hak Chul Jang
- Diabetes Metab J. 2016;40(2):140-146. Published online March 31, 2016
- DOI: https://doi.org/10.4093/dmj.2016.40.2.140
- 7,307 View
- 78 Download
- 86 Web of Science
- 89 Crossref
-
Abstract
PDFPubReader
Background The study aimed to investigate the influence of hyperglycemia on muscle quality in older men with type 2 diabetes.
Methods This was a subsidiary study of the Korean Longitudinal Study of Health and Aging. Among 326 older men consenting to tests of body composition and muscle strength, 269 men were ultimately analyzed after the exclusion because of stroke (
n =30) and uncertainty about the diagnosis of diabetes (n =27). Body composition was measured using dual-energy X-ray absorptiometry and computed tomography. Muscle strength for knee extension was measured using an isokinetic dynamometer. Muscle quality was assessed from the ratio of leg strength to the entire corresponding leg muscle mass.Results The muscle mass, strength, and quality in patients with type 2 diabetes did not differ significantly from controls. However, when patients with diabetes were subdivided according to their glycemic control status, patients with a glycosylated hemoglobin (HbA1c) level of ≥8.5% showed significantly decreased leg muscle quality by multivariate analysis (odds ratio, 4.510;
P =0.045) after adjustment for age, body mass index, smoking amount, alcohol consumption, physical activity, and duration of diabetes. Physical performance status was also impaired in subjects with an HbA1c of ≥8.5%.Conclusion Poor glycemic control in these older patients with diabetes was associated with significant risk of decreased muscle quality and performance status. Glycemic control with an HbA1c of <8.5% might be needed to reduce the risk of adverse skeletal and functional outcomes in this population.
-
Citations
Citations to this article as recorded by- Downhill running and caloric restriction attenuate insulin resistance associated skeletal muscle atrophy via the promotion of M2-like macrophages through TRIB3-AKT pathway
Wei Luo, Yue Zhou, Qiang Tang, Yuhang Wang, Yansong Liu, Lei Ai
Free Radical Biology and Medicine.2024; 210: 271. CrossRef - Diabetic Sarcopenia. A proposed muscle screening protocol in people with diabetes
Daniel de Luis Román, Juana Carretero Gómez, José Manuel García-Almeida, Fernando Garrachón Vallo, German Guzmán Rolo, Juan José López Gómez, Francisco José Tarazona-Santabalbina, Alejandro Sanz-Paris
Reviews in Endocrine and Metabolic Disorders.2024;[Epub] CrossRef - Dynapenia and sarcopenia: association with the diagnosis, duration and complication of type 2 diabetes mellitus in ELSA-Brasil
Débora Noara Duarte dos Santos, Carolina Gomes Coelho, Maria de Fátima Haueisen Sander Diniz, Bruce Bartholow Duncan, Maria Inês Schmidt, Isabela Judith Martins Bensenor, Claudia Szlejf, Rosa Weiss Telles, Sandhi Maria Barreto
Cadernos de Saúde Pública.2024;[Epub] CrossRef - Breaking Down Cachexia: A Narrative Review on the Prevalence of Cachexia in Cancer Patients and Its Associated Risk Factors
Mahmathi Karuppannan, Fares M. S. Muthanna, Fazlin Mohd Fauzi
Nutrition and Cancer.2024; 76(5): 404. CrossRef - Mechanism of muscle atrophy in a normal-weight rat model of type 2 diabetes established by using a soft-pellet diet
Sayaka Akieda-Asai, Hao Ma, Wanxin Han, Junko Nagata, Fumitake Yamaguchi, Yukari Date
Scientific Reports.2024;[Epub] CrossRef - Morphological and functional changes in skeletal muscle in type 2 diabetes mellitus: A systematic review and meta-analysis
Jardeson Rocha Filgueiras, Cleudiane Pereira Sales, Ivanilson Gomes da Silva, Cristiana Maria Dos Santos, Elias de Carvalho Magalhães Neto, Rebeca Barbosa da Rocha, Vinicius Saura Cardoso
Physiotherapy Theory and Practice.2023; 39(9): 1789. CrossRef - Hypoglycemic drug liraglutide alleviates low muscle mass by inhibiting the expression of MuRF1 and MAFbx in diabetic muscle atrophy
Dongmei Fan, Yue Wang, Bowei Liu, Fuzai Yin
Journal of the Chinese Medical Association.2023; 86(2): 166. CrossRef - Mechanisms underlying altered neuromuscular function in people with DPN
Antonin Le Corre, Nathan Caron, Nicolas A. Turpin, Georges Dalleau
European Journal of Applied Physiology.2023; 123(7): 1433. CrossRef - Effects of body compositions on the associations between ferritin and diabetes parameters among Japanese community dwellers
Kyi Mar Wai, Rei Akuzawa, Yoko Umeda, Wataru Munakata, Yoshiko Takahashi, Shigeyuki Nakaji, Kazushige Ihara
Journal of Trace Elements in Medicine and Biology.2023; 78: 127174. CrossRef - Effects of glycemic control on frailty: a multidimensional perspective
Ahmed H Abdelhafiz
Hospital Practice.2023; 51(3): 124. CrossRef - Hand grip strength is inversely associated with total daily insulin dose requirement in patients with type 2 diabetes mellitus: a cross-sectional study
Da-shuang Chen, Yun-qing Zhu, Wen-ji Ni, Yu-jiao Li, Guo-ping Yin, Zi-yue Shao, Jian Zhu
PeerJ.2023; 11: e15761. CrossRef - Sarcopenia in Type 2 Diabetes Mellitus: Study of the Modifiable Risk Factors Involved
Surapaneni Lakshmi Sravya, Jayshree Swain, Abhay Kumar Sahoo, Swayamsidha Mangaraj, Jayabhanu Kanwar, Pooja Jadhao, Srijit Das
Journal of Clinical Medicine.2023; 12(17): 5499. CrossRef - Salbutamol ameliorates skeletal muscle wasting and inflammatory markers in streptozotocin (STZ)-induced diabetic rats
Anand Kumar, Priyanka Prajapati, Vinit Raj, Seong-Cheol Kim, Vikas Mishra, Chaitany Jayprakash Raorane, Ritu Raj, Dinesh Kumar, Sapana Kushwaha
International Immunopharmacology.2023; 124: 110883. CrossRef - Decreased serum musclin concentration is independently associated with the high prevalence of sarcopenia in Chinese middle‐elderly patients with type 2 diabetes mellitus
Lei Fu, Qing Zhang, Juan Liu, Xiaoqing Yuan, Xinhua Ye
Journal of Diabetes Investigation.2023; 14(12): 1412. CrossRef - Association between relative muscle strength and hypertension in middle-aged and older Chinese adults
Jin-hua Luo, Tu-ming Zhang, Lin-lin Yang, Yu-ying Cai, Yu Yang
BMC Public Health.2023;[Epub] CrossRef - Diabetes Mellitus in the Elderly Adults in Korea: Based on Data from the Korea National Health and Nutrition Examination Survey 2019 to 2020
Seung-Hyun Ko, Kyung Do Han, Yong-Moon Park, Jae-Seung Yun, Kyuho Kim, Jae-Hyun Bae, Hyuk-Sang Kwon, Nan-Hee Kim
Diabetes & Metabolism Journal.2023; 47(5): 643. CrossRef - Management of Hyperglycemia in Older Adults with Type 2 Diabetes
Gunjan Y. Gandhi, Arshag D. Mooradian
Drugs & Aging.2022; 39(1): 39. CrossRef - Deleterious Effect of High-Fat Diet on Skeletal Muscle Performance Is Prevented by High-Protein Intake in Adult Rats but Not in Old Rats
Eleonora Poggiogalle, Fanny Rossignon, Aude Carayon, Fréderic Capel, Jean-Paul Rigaudière, Sarah De Saint Vincent, Olivier Le-Bacquer, Jérôme Salles, Christophe Giraudet, Véronique Patrac, Patrice Lebecque, Stéphane Walrand, Yves Boirie, Vincent Martin, C
Frontiers in Physiology.2022;[Epub] CrossRef - Metabolic phenotypes explain the relationship between dysglycaemia and frailty in older people with type 2 diabetes
A.H. Abdelhafiz, A.J. Sinclair
Journal of Diabetes and its Complications.2022; 36(4): 108144. CrossRef - Altered features of body composition in older adults with type 2 diabetes and prediabetes compared with matched controls
Kirsten E. Bell, Michael T. Paris, Egor Avrutin, Marina Mourtzakis
Journal of Cachexia, Sarcopenia and Muscle.2022; 13(2): 1087. CrossRef - A modern approach to glucose-lowering therapy in frail older people with type 2 diabetes mellitus
Ahmed H. Abdelhafiz, Daniel Pennells, Alan J. Sinclair
Expert Review of Endocrinology & Metabolism.2022; 17(2): 95. CrossRef - Metabolic syndrome and its association with components of sarcopenia in older community-dwelling Chinese
Qiangwei Tong, Xiao Wang, Yunlu Sheng, Shu Chen, Bin Lai, Rong Lv, Jing Yu
The Journal of Biomedical Research.2022; 36(2): 120. CrossRef - Sarcopenia is associated with the Geriatric Nutritional Risk Index in elderly patients with poorly controlled type 2 diabetes mellitus
Shun Matsuura, Koji Shibazaki, Reiko Uchida, Yukiko Imai, Takuya Mukoyama, Shoko Shibata, Hiroshi Morita
Journal of Diabetes Investigation.2022; 13(8): 1366. CrossRef - Increased serum levels of advanced glycation end products are negatively associated with relative muscle strength in patients with type 2 diabetes mellitus
Tsung-Hui Wu, Shiow-Chwen Tsai, Hsuan-Wei Lin, Chiao-Nan Chen, Chii-Min Hwu
BMC Endocrine Disorders.2022;[Epub] CrossRef - Clinical outcomes of multidimensional association of type 2 diabetes mellitus, COVID-19 and sarcopenia: an algorithm and scoping systematic evaluation
Anmar Al-Taie, Oritsetimeyin Arueyingho, Jalal Khoshnaw, Abdul Hafeez
Archives of Physiology and Biochemistry.2022; : 1. CrossRef - Hypoglycaemic therapy in frail older people with type 2 diabetes mellitus—a choice determined by metabolic phenotype
Alan J. Sinclair, Daniel Pennells, Ahmed H. Abdelhafiz
Aging Clinical and Experimental Research.2022; 34(9): 1949. CrossRef - Insulin in Frail, Older People with Type 2 Diabetes—Low Threshold for Therapy
Ahmed Abdelhafiz, Shail Bisht, Iva Kovacevic, Daniel Pennells, Alan Sinclair
Diabetology.2022; 3(2): 369. CrossRef - Sex-Specific Associations Between Low Muscle Mass and Glucose Fluctuations in Patients With Type 2 Diabetes Mellitus
Xiulin Shi, Wenjuan Liu, Lulu Zhang, Fangsen Xiao, Peiying Huang, Bing Yan, Yiping Zhang, Weijuan Su, Qiuhui Jiang, Mingzhu Lin, Wei Liu, Xuejun Li
Frontiers in Endocrinology.2022;[Epub] CrossRef - Lifestyle factors associated with muscle quality in community‐dwelling older people with type 2 diabetes in Japan and Taiwan: a cross‐sectional study
Yuko Yamaguchi, Chieko Greiner, Shu‐Chun Lee, Hirochika Ryuno, Hsin‐Yen Yen, Chiou‐Fen Lin, Ting‐I Lee, Pi‐Hsia Lee
Psychogeriatrics.2022; 22(5): 736. CrossRef - Relationship between Echo Intensity of Vastus Lateralis and Knee Extension Strength in Patients with Type 2 Diabetes Mellitus
Yoshikazu HIRASAWA, Ryosuke MATSUKI, Hideaki TANINA
Physical Therapy Research.2022; 25(3): 113. CrossRef - Time trends (2012–2020) in glycated hemoglobin and adherence to the glycemic targets recommended for elderly patients by the Japan Diabetes Society/Japan Geriatrics Society Joint Committee among memory clinic patients with diabetes mellitus
Taiki Sugimoto, Hisashi Noma, Yujiro Kuroda, Nanae Matsumoto, Kazuaki Uchida, Yoshinobu Kishino, Naoki Saji, Shumpei Niida, Takashi Sakurai
Journal of Diabetes Investigation.2022; 13(12): 2038. CrossRef - Relationship between Diabetes Status and Sarcopenia in Community-Dwelling Older Adults
Kazuhei Nishimoto, Takehiko Doi, Kota Tsutsumimoto, Sho Nakakubo, Satoshi Kurita, Yuto Kiuchi, Hiroyuki Shimada
Journal of the American Medical Directors Association.2022; 23(10): 1718.e7. CrossRef - Low relative hand grip strength is associated with a higher risk for diabetes and impaired fasting glucose among the Korean population
Min Jin Lee, Ah Reum Khang, Dongwon Yi, Yang Ho Kang, Giacomo Pucci
PLOS ONE.2022; 17(10): e0275746. CrossRef - Association between Lower-to-Upper Ratio of Appendicular Skeletal Muscle and Metabolic Syndrome
Hyun Eui Moon, Tae Sic Lee, Tae-Ha Chung
Journal of Clinical Medicine.2022; 11(21): 6309. CrossRef - Association of plasma brain-derived neurotrophic factor levels and frailty in community-dwelling older adults
Eun Roh, Soon Young Hwang, Eyun Song, Min Jeong Park, Hye Jin Yoo, Sei Hyun Baik, Miji Kim, Chang Won Won, Kyung Mook Choi
Scientific Reports.2022;[Epub] CrossRef - Organokines, Sarcopenia, and Metabolic Repercussions: The Vicious Cycle and the Interplay with Exercise
Giulia Minniti, Letícia Maria Pescinini-Salzedas, Guilherme Almeida dos Santos Minniti, Lucas Fornari Laurindo, Sandra Maria Barbalho, Renata Vargas Sinatora, Lance Alan Sloan, Rafael Santos de Argollo Haber, Adriano Cressoni Araújo, Karina Quesada, Jesse
International Journal of Molecular Sciences.2022; 23(21): 13452. CrossRef - Multimorbidity, Frailty and Diabetes in Older People–Identifying Interrelationships and Outcomes
Alan J. Sinclair, Ahmed H. Abdelhafiz
Journal of Personalized Medicine.2022; 12(11): 1911. CrossRef - Determinants of High-Dose Insulin Usage and Upper Extremity Muscle Strength in Adult Patients With Type 2 Diabetes
Eren Imre, Tugce Apaydin, Hatice Gizem Gunhan, Dilek Gogas Yavuz
Canadian Journal of Diabetes.2021; 45(4): 341. CrossRef - Glycemic Control and Insulin Improve Muscle Mass and Gait Speed in Type 2 Diabetes: The MUSCLES-DM Study
Ken Sugimoto, Hiroshi Ikegami, Yasunori Takata, Tomohiro Katsuya, Masahiro Fukuda, Hiroshi Akasaka, Yasuharu Tabara, Haruhiko Osawa, Yoshihisa Hiromine, Hiromi Rakugi
Journal of the American Medical Directors Association.2021; 22(4): 834. CrossRef - A Narrative Review on Sarcopenia in Type 2 Diabetes Mellitus: Prevalence and Associated Factors
Anna Izzo, Elena Massimino, Gabriele Riccardi, Giuseppe Della Pepa
Nutrients.2021; 13(1): 183. CrossRef - Decreased handgrip strength in patients with type 2 diabetes: A cross-sectional study in a tertiary care hospital in north India
Parjeet Kaur, Ritesh Bansal, Bharti Bhargava, Sunil Mishra, Harmandeep Gill, Ambrish Mithal
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2021; 15(1): 325. CrossRef - Factors associated with relative muscle strength in patients with type 2 diabetes mellitus
Chiao-Nan Chen, Ting-Chung Chen, Shiow-Chwen Tsai, Chii-Min Hwu
Archives of Gerontology and Geriatrics.2021; 95: 104384. CrossRef - Newer anti-diabetic therapies with low hypoglycemic risk-potential advantages for frail older people
Demelza Emmerton, Ahmed Abdelhafiz
Hospital Practice.2021; 49(3): 164. CrossRef - Influence of glucose, insulin fluctuation, and glycosylated hemoglobin on the outcome of sarcopenia in patients with type 2 diabetes mellitus
Yuxi Lin, Yongze Zhang, Ximei Shen, Lingning Huang, Sunjie Yan
Journal of Diabetes and its Complications.2021; 35(6): 107926. CrossRef - Presence and Implications of Sarcopenia in Non-alcoholic Steatohepatitis
Gregory Habig, Christa Smaltz, Dina Halegoua-DeMarzio
Metabolites.2021; 11(4): 242. CrossRef - Sensory-Motor Mechanisms Increasing Falls Risk in Diabetic Peripheral Neuropathy
Neil D. Reeves, Giorgio Orlando, Steven J. Brown
Medicina.2021; 57(5): 457. CrossRef - Impact of frailty metabolic phenotypes on the management of older people with type 2 diabetes mellitus
Ahmed H Abdelhafiz, Demelza Emmerton, Alan J Sinclair
Geriatrics & Gerontology International.2021; 21(8): 614. CrossRef - Type 2 diabetes mellitus in older adults: clinical considerations and management
Srikanth Bellary, Ioannis Kyrou, James E. Brown, Clifford J. Bailey
Nature Reviews Endocrinology.2021; 17(9): 534. CrossRef - Metabolic Syndrome and Sarcopenia
Hiroki Nishikawa, Akira Asai, Shinya Fukunishi, Shuhei Nishiguchi, Kazuhide Higuchi
Nutrients.2021; 13(10): 3519. CrossRef - Angiotensin II inhibition: a potential treatment to slow the progression of sarcopenia
Jeffrey Kingsley, Keiichi Torimoto, Tomoki Hashimoto, Satoru Eguchi
Clinical Science.2021; 135(21): 2503. CrossRef - Muscle strength, an independent determinant of glycemic control in older adults with long-standing type 2 diabetes: a prospective cohort study
Bo Kyung Koo, Seoil Moon, Min Kyong Moon
BMC Geriatrics.2021;[Epub] CrossRef - Associations between homocysteine, inflammatory cytokines and sarcopenia in Chinese older adults with type 2 diabetes
Zhi-Jing Mu, Jun-Ling Fu, Li-Na Sun, Piu Chan, Shuang-Ling Xiu
BMC Geriatrics.2021;[Epub] CrossRef - The Association Between Diabetes Mellitus and Risk of Sarcopenia: Accumulated Evidences From Observational Studies
Yu-Shun Qiao, Yin-He Chai, Hong-Jian Gong, Zhiyessova Zhuldyz, Coen D. A. Stehouwer, Jian-Bo Zhou, Rafael Simó
Frontiers in Endocrinology.2021;[Epub] CrossRef - The utility of the ultrasonographic assessment of the lower leg muscles to evaluate sarcopenia and muscle quality in older adults
Masaaki Isaka, Ken Sugimoto, Taku Fujimoto, Yukiko Yasunobe, Keyu Xie, Yuri Onishi, Shino Yoshida, Toshimasa Takahashi, Hitomi Kurinami, Hiroshi Akasaka, Yasushi Takeya, Koichi Yamamoto, Hiromi Rakugi
JCSM Clinical Reports.2021; 6(2): 53. CrossRef - Associations between grip strength and glycemic control in type 2 diabetes mellitus: an analysis of data from the 2014-2019 Korea National Health and Nutrition Examination Survey
Harim Choe, Hoyong Sung, Geon Hui Kim, On Lee, Hyo Youl Moon, Yeon Soo Kim
Epidemiology and Health.2021; 43: e2021080. CrossRef - Uncontrolled Diabetes as an Associated Factor with Dynapenia in Adults Aged 50 Years or Older: Sex Differences
Clarice Cavalero Nebuloni, Roberta de Oliveira Máximo, Cesar de Oliveira, Tiago da Silva Alexandre, Anne Newman
The Journals of Gerontology: Series A.2020; 75(6): 1191. CrossRef - Identification and prevalence of frailty in diabetes mellitus and association with clinical outcomes: a systematic review protocol
Peter Hanlon, Isabella Fauré, Neave Corcoran, Elaine Butterly, Jim Lewsey, David A McAllister, Frances S Mair
BMJ Open.2020; 10(9): e037476. CrossRef - Longitudinal association of type 2 diabetes and insulin therapy with muscle parameters in the KORA-Age study
Uta Ferrari, Cornelia Then, Marietta Rottenkolber, Canan Selte, Jochen Seissler, Romy Conzade, Birgit Linkohr, Annette Peters, Michael Drey, Barbara Thorand
Acta Diabetologica.2020; 57(9): 1057. CrossRef - Triad of impairment in older people with diabetes-reciprocal relations and clinical implications
A.H. Abdelhafiz, P.C. Davies, A.J. Sinclair
Diabetes Research and Clinical Practice.2020; 161: 108065. CrossRef - Physical activity and exercise: Strategies to manage frailty
Javier Angulo, Mariam El Assar, Alejandro Álvarez-Bustos, Leocadio Rodríguez-Mañas
Redox Biology.2020; 35: 101513. CrossRef - Handgrip measurement as a useful benchmark for locomotive syndrome in patients with type 2 diabetes mellitus: A KAMOGAWA‐DM cohort study
Noriyuki Kitagawa, Takuro Okamura, Nobuko Kitagawa, Yoshitaka Hashimoto, Masahide Hamaguchi, Michiaki Fukui
Journal of Diabetes Investigation.2020; 11(6): 1602. CrossRef - Edmonton frail score is associated with diabetic control in elderly type 2 diabetic subjects
Satilmis Bilgin, Gulali Aktas, Ozge Kurtkulagi, Burcin M. Atak, Tuba T. Duman
Journal of Diabetes & Metabolic Disorders.2020; 19(1): 511. CrossRef - Comparison of field- and laboratory-based estimates of muscle quality index between octogenarians and young older adults: an observational study
Dahan da Cunha Nascimento, Jonato Prestes, Joyce de Sousa Diniz, Pedro Rodrigues Beal, Vicente Paulo Alves, Whitley Stone, Fabiani Lage Rodrigues Beal
Journal of Exercise Rehabilitation.2020; 16(5): 458. CrossRef - Tip 2 Diyabetli Hastalarda Kan Glukoz Seviyesi ile Kas Gücü, Propriosepsiyon ve Vücut Kompozisyonu Arasındaki İlişki
Zahide Betül TAYFUR, Esra ATILGAN
Turkish Journal of Diabetes and Obesity.2020; 4(3): 207. CrossRef - Challenges and Strategies for Diabetes Management in Community-Living Older Adults
Alan J. Sinclair, Ahmed H. Abdelhafiz
Diabetes Spectrum.2020; 33(3): 217. CrossRef - Association between deterioration in muscle strength and peripheral neuropathy in people with diabetes
Tae Jung Oh, Sunyoung Kang, Jie-Eun Lee, Jae Hoon Moon, Sung Hee Choi, Soo Lim, Hak Chul Jang
Journal of Diabetes and its Complications.2019; 33(8): 598. CrossRef - The Association between Body Composition using Dual energy X-ray Absorptiometry and Type-2 Diabetes: A Systematic Review and Meta-Analysis of Observational studies
Preeti Gupta, Carla Lanca, Alfred T. L. Gan, Pauline Soh, Sahil Thakur, Yijin Tao, Neelam Kumari, Ryan E. K. Man, Eva K. Fenwick, Ecosse L. Lamoureux
Scientific Reports.2019;[Epub] CrossRef - MECHANISMS OF ENDOCRINE DISEASE: Sarcopenia in endocrine and non-endocrine disorders
Victoria Zeghbi Cochenski Borba, Tatiana Lemos Costa, Carolina Aguiar Moreira, Cesar Luiz Boguszewski
European Journal of Endocrinology.2019; 180(5): R185. CrossRef - Hyperglycemia induces skeletal muscle atrophy via a WWP1/KLF15 axis
Yu Hirata, Kazuhiro Nomura, Yoko Senga, Yuko Okada, Kenta Kobayashi, Shiki Okamoto, Yasuhiko Minokoshi, Michihiro Imamura, Shin’ichi Takeda, Tetsuya Hosooka, Wataru Ogawa
JCI Insight.2019;[Epub] CrossRef - Hyperglycemia in non‐obese patients with type 2 diabetes is associated with low muscle mass: The Multicenter Study for Clarifying Evidence for Sarcopenia in Patients with Diabetes Mellitus
Ken Sugimoto, Yasuharu Tabara, Hiroshi Ikegami, Yasunori Takata, Kei Kamide, Tome Ikezoe, Eri Kiyoshige, Yukako Makutani, Hiroshi Onuma, Yasuyuki Gondo, Kazunori Ikebe, Noriaki Ichihashi, Tadao Tsuboyama, Fumihiko Matsuda, Katsuhiko Kohara, Mai Kabayama,
Journal of Diabetes Investigation.2019; 10(6): 1471. CrossRef - Diabetic Peripheral Neuropathy as a Risk Factor for Sarcopenia
Tae Jung Oh, Yoojung Song, Jae Hoon Moon, Sung Hee Choi, Hak Chul Jang
Annals of Geriatric Medicine and Research.2019; 23(4): 170. CrossRef - Diabetes and frailty
Mariam El Assar, Olga Laosa, Leocadio Rodríguez Mañas
Current Opinion in Clinical Nutrition & Metabolic Care.2019; 22(1): 52. CrossRef - Association of Glucose Fluctuations with Sarcopenia in Older Adults with Type 2 Diabetes Mellitus
Noriko Ogama, Takashi Sakurai, Shuji Kawashima, Takahisa Tanikawa, Haruhiko Tokuda, Shosuke Satake, Hisayuki Miura, Atsuya Shimizu, Manabu Kokubo, Shumpei Niida, Kenji Toba, Hiroyuki Umegaki, Masafumi Kuzuya
Journal of Clinical Medicine.2019; 8(3): 319. CrossRef - Diabetes in the elderly
Ahmed H. Abdelhafiz, Alan J. Sinclair
Medicine.2019; 47(2): 119. CrossRef - Diabetes and Muscle Dysfunction in Older Adults
Hak Chul Jang
Annals of Geriatric Medicine and Research.2019; 23(4): 160. CrossRef - Factors influencing safe glucose-lowering in older adults with type 2 diabetes: A PeRsOn-centred ApproaCh To IndiVidualisEd (PROACTIVE) Glycemic Goals for older people
C.E. Hambling, K. Khunti, X. Cos, J. Wens, L. Martinez, P. Topsever, S. Del Prato, A. Sinclair, G. Schernthaner, G. Rutten, S. Seidu
Primary Care Diabetes.2019; 13(4): 330. CrossRef - Effects of resistance training on neuromuscular parameters in elderly with type 2 diabetes mellitus: A randomized clinical trial
Cíntia E. Botton, Daniel Umpierre, Anderson Rech, Lucinéia O. Pfeifer, Carlos L.F. Machado, Juliana L. Teodoro, Alexandre S. Dias, Ronei S. Pinto
Experimental Gerontology.2018; 113: 141. CrossRef - Management of Elderly Diabetes Patients Who Are Unable to Self-Care
Bok Rye Song
The Journal of Korean Diabetes.2018; 19(4): 232. CrossRef - Decreased Muscle Strength and Quality in Diabetes-Related Dementia
Akito Tsugawa, Yusuke Ogawa, Naoto Takenoshita, Yoshitsugu Kaneko, Hirokuni Hatanaka, Eriko Jaime, Raita Fukasawa, Haruo Hanyu
Dementia and Geriatric Cognitive Disorders Extra.2017; 7(3): 454. CrossRef - Diabetes and Sarcopenia
Dong Hyun Kim, Tae Yang Yu
The Journal of Korean Diabetes.2017; 18(4): 239. CrossRef - Frailty and sarcopenia - newly emerging and high impact complications of diabetes
Alan J. Sinclair, Ahmed H. Abdelhafiz, Leocadio Rodríguez-Mañas
Journal of Diabetes and its Complications.2017; 31(9): 1465. CrossRef - Association of diabetic retinopathy with both sarcopenia and muscle quality in patients with type 2 diabetes: a cross-sectional study
Tatsuya Fukuda, Ryotaro Bouchi, Takato Takeuchi, Yujiro Nakano, Masanori Murakami, Isao Minami, Hajime Izumiyama, Koshi Hashimoto, Takanobu Yoshimoto, Yoshihiro Ogawa
BMJ Open Diabetes Research & Care.2017; 5(1): e000404. CrossRef - Practical considerations for managing patients with diabetes and dementia
Michelle L Mair, Rohin Athavale, Ahmed H Abdelhafiz
Expert Review of Endocrinology & Metabolism.2017; 12(6): 429. CrossRef - Sarcopenia: An Endocrine Disorder?
Alexis McKee, John E. Morley, Alvin M. Matsumoto, Aaron Vinik
Endocrine Practice.2017; 23(9): 1143. CrossRef - Response: Hyperglycemia Is Associated with Impaired Muscle Quality in Older Men with Diabetes: The Korean Longitudinal Study on Health and Aging (Diabetes Metab J 2016;40:140-6)
Ji Won Yoon, Hak Chul Jang
Diabetes & Metabolism Journal.2016; 40(3): 250. CrossRef - Salivary lactate dehydrogenase and aminotransferases in diabetic patients
Barbara Malicka, Katarzyna Skoskiewicz-Malinowska, Urszula Kaczmarek
Medicine.2016; 95(47): e5211. CrossRef - Explanatory models of muscle performance in acromegaly patients evaluated by knee isokinetic dynamometry: Implications for rehabilitation
Agnaldo José Lopes, Arthur Sá Ferreira, Evelyn Mendes Walchan, Mauricio Santos Soares, Priscila Santos Bunn, Fernando Silva Guimarães
Human Movement Science.2016; 49: 160. CrossRef - Letter: Hyperglycemia Is Associated with Impaired Muscle Quality in Older Men with Diabetes: The Korean Longitudinal Study on Health and Aging (Diabetes Metab J 2016;40:140-6)
Jun Sung Moon
Diabetes & Metabolism Journal.2016; 40(3): 248. CrossRef - Sarcopenia, Frailty, and Diabetes in Older Adults
Hak Chul Jang
Diabetes & Metabolism Journal.2016; 40(3): 182. CrossRef
- Downhill running and caloric restriction attenuate insulin resistance associated skeletal muscle atrophy via the promotion of M2-like macrophages through TRIB3-AKT pathway
- Relative Skeletal Muscle Mass Is Associated with Development of Metabolic Syndrome
- Byung Sam Park, Ji Sung Yoon
- Diabetes Metab J. 2013;37(6):458-464. Published online December 12, 2013
- DOI: https://doi.org/10.4093/dmj.2013.37.6.458
- 5,629 View
- 104 Download
- 73 Crossref
-
Abstract
PDFPubReader
Background Visceral adiposity is related to insulin resistance. Skeletal muscle plays a central role in insulin-mediated glucose disposal; however, little is known about the association between muscle mass and metabolic syndrome (MS). This study is to clarify the clinical role of skeletal muscle mass in development of MS.
Methods A total of 1,042 subjects were enrolled. Subjects with prior MS and chronic diseases were excluded. After 24 months, development of MS was assessed using NCEP-ATP III criteria. Skeletal muscle mass (SMM; kg), body fat mass (BFM; kg), and visceral fat area (VFA; cm2) were obtained from bioelectrical analysis. Then, the following values were calculated as follows: percent of SMM (SMM%; %): SMM (kg)/weight (kg), skeletal muscle index (SMI; kg/m2): SMM (kg)/height (m2), skeletal muscle to body fat ratio (MFR): SMM (kg)/BFM (kg), and skeletal muscle to visceral fat ratio (SVR; kg/cm2): SMM (kg)/VFA (cm2).
Results Among 838 subjects, 88 (10.5%) were newly diagnosed with MS. Development of MS increased according to increasing quintiles of BMI, SMM, VFA, and SMI, but was negatively associated with SMM%, MFR, and SVR. VFA was positively associated with high waist circumference (WC), high blood pressure (BP), dysglycemia, and high triglyceride (TG). In contrast, MFR was negatively associated with high WC, high BP, dysglycemia, and high TG. SVR was negatively associated with all components of MS.
Conclusion Relative SMM ratio to body composition, rather than absolute mass, may play a critical role in development of MS and could be used as a strong predictor.
-
Citations
Citations to this article as recorded by- Relationship between adiponectin and muscle mass in patients with metabolic syndrome and obesity
Daniel de Luis, David Primo, Olatz Izaola, Juan José Lopez Gomez
Journal of Diabetes and its Complications.2024; 38(4): 108706. CrossRef - The longitudinal association of adipose-to-lean ratio with incident cardiometabolic morbidity: The CARDIA study
Robert Booker, Mandy Wong, Michael P. Bancks, Mercedes R. Carnethon, Lisa S. Chow, Cora E. Lewis, Pamela J. Schreiner, Shaina J. Alexandria
Journal of Diabetes and its Complications.2024; 38(5): 108725. CrossRef - Assessing Sarcopenic Obesity Risk in Children During the COVID-19 Pandemic: Grip-to-BMI Ratio
Bahar Öztelcan Gündüz, Aysu Duyan Çamurdan, Mücahit Yıldız, F. Nur Baran Aksakal, Emine Nüket Ünsal
Medical Research Reports.2024; 7(1): 18. CrossRef - Sex differences in body composition in youth with type 1 diabetes and its predictive value in cardiovascular disease risk assessment
Avivit Brener, Sandy Hamama, Hagar Interator, Asaf Ben Simon, Irina Laurian, Anna Dorfman, Efrat Chorna, Michal Yackobovitch‐Gavan, Asaf Oren, Ori Eyal, Yael Lebenthal
Diabetes/Metabolism Research and Reviews.2023;[Epub] CrossRef - Epidemiological, mechanistic, and practical bases for assessment of cardiorespiratory fitness and muscle status in adults in healthcare settings
Jaime A. Gallo-Villegas, Juan C. Calderón
European Journal of Applied Physiology.2023; 123(5): 945. CrossRef - The Effect of Childhood Obesity or Sarcopenic Obesity on Metabolic Syndrome Risk in Adolescence: The Ewha Birth and Growth Study
Hyunjin Park, Seunghee Jun, Hye-Ah Lee, Hae Soon Kim, Young Sun Hong, Hyesook Park
Metabolites.2023; 13(1): 133. CrossRef - Relationships of BMI, muscle-to-fat ratio, and handgrip strength-to-BMI ratio to physical fitness in Spanish children and adolescents
Samuel Manzano-Carrasco, Jorge Garcia-Unanue, Eero A. Haapala, Jose Luis Felipe, Leonor Gallardo, Jorge Lopez-Fernandez
European Journal of Pediatrics.2023; 182(5): 2345. CrossRef - Body physique rating as a factor to identify at-risk Mexicans for Metabolic Syndrome
Oscar Herrera-Fomperosa, Sergio K. Bustamante-Villagomez, Sarahí Vazquez-Álvarez, Gabriela Vázquez-Marroquín, Leonardo M. Porchia, Enrique Torres-Rasgado, Ricardo Pérez-Fuentes, M. Elba Gonzalez-Mejia
Human Nutrition & Metabolism.2023; 33: 200206. CrossRef - The association between creatinine to body weight ratio and the risk of progression to diabetes from pre-diabetes: a 5-year cohort study in Chinese adults
Tong Li, Changchun Cao, Xuan Xuan, Wenjing Liu, Xiaohua Xiao, Cuimei Wei
BMC Endocrine Disorders.2023;[Epub] CrossRef - Muscle-to-Fat Ratio for Predicting Metabolic Syndrome Components in Children with Overweight and Obesity
Noga Salton, Sharona Kern, Hagar Interator, Adar Lopez, Hadar Moran-Lev, Yael Lebenthal, Avivit Brener
Childhood Obesity.2022; 18(2): 132. CrossRef - Mentale Gesundheit und physische Aktivität
Wolfgang Laube
Manuelle Medizin.2022; 60(1): 13. CrossRef - Increased odds of having the metabolic syndrome with greater fat‐free mass: counterintuitive results from the National Health and Nutrition Examination Survey database
Jean‐Christophe Lagacé, Alexis Marcotte‐Chenard, Jasmine Paquin, Dominic Tremblay, Martin Brochu, Isabelle J. Dionne
Journal of Cachexia, Sarcopenia and Muscle.2022; 13(1): 377. CrossRef - Lipoprotein subfractions in patients with sarcopenia and their relevance to skeletal muscle mass and function
Hui Gong, Yang Liu, Xing Lyu, Lini Dong, Xiangyu Zhang
Experimental Gerontology.2022; 159: 111668. CrossRef - Health Risks of Sarcopenic Obesity in Overweight Children and Adolescents: Data from the CHILT III Programme (Cologne)
Carolin Sack, Nina Ferrari, David Friesen, Fabiola Haas, Marlen Klaudius, Lisa Schmidt, Gabriel Torbahn, Hagen Wulff, Christine Joisten
Journal of Clinical Medicine.2022; 11(1): 277. CrossRef - Creatinine-to-body weight ratio is a predictor of incident diabetes: a population-based retrospective cohort study
Jiacheng He
Diabetology & Metabolic Syndrome.2022;[Epub] CrossRef - Relative low muscle mass and muscle strength is associated with the prevalence of metabolic syndrome in patients with type 2 diabetes
Maya Takegami, Yoshitaka Hashimoto, Masahide Hamaguchi, Ayumi Kaji, Ryosuke Sakai, Takuro Okamura, Noriyuki Kitagawa, Takafumi Osaka, Hiroshi Okada, Naoko Nakanishi, Saori Majima, Takafumi Senmaru, Emi Ushigome, Mai Asano, Masahiro Yamazaki, Michiaki Fuku
Journal of Clinical Biochemistry and Nutrition.2022; 71(2): 136. CrossRef - “Big Data” Approaches for Prevention of the Metabolic Syndrome
Xinping Jiang, Zhang Yang, Shuai Wang, Shuanglin Deng
Frontiers in Genetics.2022;[Epub] CrossRef - Teil 2: Muskeldysfunktionen – mit Training gegen Schmerz
Wolfgang Laube
Manuelle Medizin.2022; 60(3): 129. CrossRef - Impact of Low Skeletal Muscle Mass and Obesity on Hearing Loss in Asymptomatic Individuals: A Population-Based Study
Chul-Hyun Park, Kyung Jae Yoon, Yong-Taek Lee, Sung Min Jin, Sang Hyuk Lee, Tae Hwan Kim
Healthcare.2022; 10(10): 2022. CrossRef - Physical activity level, sitting time, and skeletal muscle mass between esports players and non-esports players
Zhi H. SEE, Mohamad S. ABDUL HAMID
Gazzetta Medica Italiana Archivio per le Scienze Mediche.2022;[Epub] CrossRef - Associations of changes in fat free mass with risk for type 2 diabetes: Hispanic Community Health Study/Study of Latinos
M.N. LeCroy, S. Hua, R.C. Kaplan, D. Sotres-Alvarez, Q. Qi, B. Thyagarajan, L.C. Gallo, A. Pirzada, M.L. Daviglus, N. Schneiderman, G.A. Talavera, C.R. Isasi
Diabetes Research and Clinical Practice.2021; 171: 108557. CrossRef - The phospholipase A2 family’s role in metabolic diseases: Focus on skeletal muscle
Iris Prunonosa Cervera, Brendan M. Gabriel, Peter Aldiss, Nicholas M. Morton
Physiological Reports.2021;[Epub] CrossRef - Bone Health in Aging Men: Does Zinc and Cuprum Level Matter?
Aleksandra Rył, Tomasz Miazgowski, Aleksandra Szylińska, Agnieszka Turoń-Skrzypińska, Alina Jurewicz, Andrzej Bohatyrewicz, Iwona Rotter
Biomolecules.2021; 11(2): 237. CrossRef - Animal Protein versus Plant Protein in Supporting Lean Mass and Muscle Strength: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Meng Thiam Lim, Bernice Jiaqi Pan, Darel Wee Kiat Toh, Clarinda Nataria Sutanto, Jung Eun Kim
Nutrients.2021; 13(2): 661. CrossRef - Effects of Exercise Intervention on Mitochondrial Stress Biomarkers in Metabolic Syndrome Patients: A Randomized Controlled Trial
Jae Seung Chang, Jun Namkung
International Journal of Environmental Research and Public Health.2021; 18(5): 2242. CrossRef - Association between sarcopenia level and metabolic syndrome
Su Hwan Kim, Ji Bong Jeong, Jinwoo Kang, Dong-Won Ahn, Ji Won Kim, Byeong Gwan Kim, Kook Lae Lee, Sohee Oh, Soon Ho Yoon, Sang Joon Park, Doo Hee Lee, Masaki Mogi
PLOS ONE.2021; 16(3): e0248856. CrossRef - Sarcopenia and Appendicular Muscle Mass as Predictors of Impaired Fasting Glucose/Type 2 Diabetes in Elderly Women
Carola Buscemi, Yvelise Ferro, Roberta Pujia, Elisa Mazza, Giada Boragina, Angela Sciacqua, Salvatore Piro, Arturo Pujia, Giorgio Sesti, Silvio Buscemi, Tiziana Montalcini
Nutrients.2021; 13(6): 1909. CrossRef - Low muscle mass in older adults and mortality: A systematic review and meta-analysis
Felipe M. de Santana, Melissa O. Premaor, Nicolas Y. Tanigava, Rosa M.R. Pereira
Experimental Gerontology.2021; 152: 111461. CrossRef - Association of obesity, visceral adiposity, and sarcopenia with an increased risk of metabolic syndrome: A retrospective study
Su Hwan Kim, Hyoun Woo Kang, Ji Bong Jeong, Dong Seok Lee, Dong-Won Ahn, Ji Won Kim, Byeong Gwan Kim, Kook Lae Lee, Sohee Oh, Soon Ho Yoon, Sang Joon Park, Mauro Lombardo
PLOS ONE.2021; 16(8): e0256083. CrossRef - Der Muskulatur mehr Aufmerksamkeit schenken!
Wolfgang Laube
Manuelle Medizin.2021; 59(4): 302. CrossRef - Dietary Protein Requirement Threshold and Micronutrients Profile in Healthy Older Women Based on Relative Skeletal Muscle Mass
Praval Khanal, Lingxiao He, Hans Degens, Georgina K. Stebbings, Gladys L. Onambele-Pearson, Alun G. Williams, Martine Thomis, Christopher I. Morse
Nutrients.2021; 13(9): 3076. CrossRef - Effects of different definitions of low muscle mass on its association with metabolic syndrome in older adults: A Korean nationwide study
Yerim Jeon, Ki Young Son
Geriatrics & Gerontology International.2021; 21(11): 1003. CrossRef - Musclin Is Related to Insulin Resistance and Body Composition, but Not to Body Mass Index or Cardiorespiratory Capacity in Adults
Yeliana L. Sánchez, Manuela Yepes-Calderón, Luis Valbuena, Andrés F. Milán, María C. Trillos-Almanza, Sergio Granados, Miguel Peña, Mauricio Estrada-Castrillón, Juan C. Aristizábal, Raúl Narvez-Sanchez, Jaime Gallo-Villegas, Juan C. Calderón
Endocrinology and Metabolism.2021; 36(5): 1055. CrossRef - Relative Lean Body Mass and Waist Circumference for the Identification of Metabolic Syndrome in the Korean General Population
Eunjoo Kwon, Eun-Hee Nah, Suyoung Kim, Seon Cho
International Journal of Environmental Research and Public Health.2021; 18(24): 13186. CrossRef - Impact of Skeletal Muscle Mass on Metabolic Health
Gyuri Kim, Jae Hyeon Kim
Endocrinology and Metabolism.2020; 35(1): 1. CrossRef - Skeletal muscle area and density are associated with lipid and lipoprotein cholesterol levels: The Multi-Ethnic Study of Atherosclerosis
Chantal A. Vella, Megan C. Nelson, Jonathan T. Unkart, Iva Miljkovic, Matthew A. Allison
Journal of Clinical Lipidology.2020; 14(1): 143. CrossRef - Creatinine/(cystatin C × body weight) ratio is associated with skeletal muscle mass index
Kensuke Nishida, Yoshitaka Hashimoto, Ayumi Kaji, Takuro Okamura, Ryousuke Sakai, Noriyuki Kitagawa, Takafumi Osaka, Masahide Hamaguchi, Michiaki Fukui
Endocrine Journal.2020; 67(7): 733. CrossRef - Testosterone Therapy for Prevention and Treatment of Obesity in Men
Monica Caliber, Farid Saad
Androgens: Clinical Research and Therapeutics.2020; 1(1): 40. CrossRef - Creatinine to Body Weight Ratio Is Associated with Incident Diabetes: Population-Based Cohort Study
Yoshitaka Hashimoto, Takuro Okamura, Masahide Hamaguchi, Akihiro Obora, Takao Kojima, Michiaki Fukui
Journal of Clinical Medicine.2020; 9(1): 227. CrossRef - Skeletal muscle – A bystander or influencer of metabolic syndrome?
Gina L. Richter-Stretton, Andrew S. Fenning, Rebecca K. Vella
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2020; 14(5): 867. CrossRef - Using relative handgrip strength to identify children at risk of sarcopenic obesity
Seryozha Gontarev, Mirko Jakimovski, Georgi Georgiev
Nutrición Hospitalaria.2020;[Epub] CrossRef - Nonalcoholic Fatty Liver Disease Is Associated With Low Skeletal Muscle Mass in Overweight/Obese Youths
Lucia Pacifico, Francesco Massimo Perla, Gianmarco Andreoli, Rosangela Grieco, Pasquale Pierimarchi, Claudio Chiesa
Frontiers in Pediatrics.2020;[Epub] CrossRef - Independent and combined associations of cardiorespiratory fitness and muscle strength with metabolic syndrome in older adults: A cross-sectional study
Marcyo Câmara, Rodrigo Alberto Vieira Browne, Gabriel Costa Souto, Daniel Schwade, Ludmila Pereira Lucena Cabral, Geovani Araújo Dantas Macêdo, Luiz Fernando Farias-Junior, Fabíola Leite Gouveia, Telma Maria Araújo Moura Lemos, Kenio Costa Lima, Todd A. D
Experimental Gerontology.2020; 135: 110923. CrossRef - A counterintuitive perspective for the role of fat‐free mass in metabolic health
Jean‐Christophe Lagacé, Martin Brochu, Isabelle J. Dionne
Journal of Cachexia, Sarcopenia and Muscle.2020; 11(2): 343. CrossRef - Response: The way fat‐free mass is reported may change the conclusions regarding its protective effect on metabolic health
Jean‐Christophe Lagace, Martin Brochu, Isabelle J. Dionne
Clinical Endocrinology.2020; 92(1): 79. CrossRef - The Association between Major Dietary Pattern and Low Muscle Mass in Korean Middle-Aged and Elderly Populations: Based on the Korea National Health and Nutrition Examination Survey
Seong-Ah Kim, Jinwoo Ha, Byeonghwi Lim, Jun-Mo Kim, Sangah Shin
Nutrients.2020; 12(11): 3543. CrossRef - Total body skeletal muscle mass and diet in children aged 6–8 years: ANIVA Study
Maria Morales-Suarez-Varela, Isabel Peraita-Costa, Carlos Guillamon Escudero, Agustin Llopis-Morales, Agustin Llopis-Gonzalez
Applied Physiology, Nutrition, and Metabolism.2019; 44(9): 944. CrossRef - The way fat‐free mass is reported may change the conclusions regarding its protective effect on metabolic health
Jean‐Christophe Lagacé, Dominic Tremblay, Jasmine Paquin, Alexis Marcotte‐Chénard, Martin Brochu, Isabelle J. Dionne
Clinical Endocrinology.2019; 91(6): 903. CrossRef - Components of Metabolic Syndrome in Korean Adults: A Hospital-Based Cohort at Seoul National University Bundang Hospital
Soo Lim, Se Hee Min, Ji Hyun Lee, Lee Kyung Kim, Dong-Hwa Lee, Jie-Eun Lee, Kyoung Min Kim, Sunmi Lee, Kyoung-Chan Park, Yun Jong Lee
Journal of Obesity & Metabolic Syndrome.2019; 28(2): 118. CrossRef - Skeletal muscle as a protagonist in the pregnancy metabolic syndrome
Raul Narvaez-Sanchez, Juan C. Calderón, Gloria Vega, Maria Camila Trillos, Sara Ospina
Medical Hypotheses.2019; 126: 26. CrossRef - Increase in relative skeletal muscle mass over time and its inverse association with metabolic syndrome development: a 7-year retrospective cohort study
Gyuri Kim, Seung-Eun Lee, Ji Eun Jun, You-Bin Lee, Jiyeon Ahn, Ji Cheol Bae, Sang-Man Jin, Kyu Yeon Hur, Jae Hwan Jee, Moon-Kyu Lee, Jae Hyeon Kim
Cardiovascular Diabetology.2018;[Epub] CrossRef - Association of Age-Related Trends in Blood Pressure and Body Composition Indices in Healthy Adults
Wei Li, Yan He, Lili Xia, Xinghua Yang, Feng Liu, Jingang Ma, Zhiping Hu, Yajun Li, Dongxue Li, Jiajia Jiang, Guangliang Shan, Changlong Li
Frontiers in Physiology.2018;[Epub] CrossRef - Metabolic syndrome and body shape predict differences in health parameters in farm working women
Ilze Mentoor, Maritza Kruger, Theo Nell
BMC Public Health.2018;[Epub] CrossRef - Associations of stunting in early childhood with cardiometabolic risk factors in adulthood
Emanuella De Lucia Rolfe, Giovanny Vinícius Araújo de França, Carolina Avila Vianna, Denise P. Gigante, J. Jaime Miranda, John S. Yudkin, Bernardo Lessa Horta, Ken K. Ong, C. Mary Schooling
PLOS ONE.2018; 13(4): e0192196. CrossRef - Relationship Between Relative Skeletal Muscle Mass and Nonalcoholic Fatty Liver Disease: A 7‐Year Longitudinal Study
Gyuri Kim, Seung‐Eun Lee, You‐Bin Lee, Ji Eun Jun, Jiyeon Ahn, Ji Cheol Bae, Sang‐Man Jin, Kyu Yeon Hur, Jae Hwan Jee, Moon‐Kyu Lee, Jae Hyeon Kim
Hepatology.2018; 68(5): 1755. CrossRef - Relationships among Skeletal Muscle Mass, Health Related Factors, Nutrient Intake, and Physical Activities in Male Adolescents: Based on the 5th (2009-2011) Korean National Health and Nutrition Examination Survey (KNHANES)
In-Kyung Jung, Jung-Hyun Kim
The Korean Journal of Community Living Science.2018; 29(2): 185. CrossRef - Using relative handgrip strength to identify children at risk of sarcopenic obesity
Michal Steffl, Jan Chrudimsky, James J. Tufano, Masaki Mogi
PLOS ONE.2017; 12(5): e0177006. CrossRef - International society of sports nutrition position stand: diets and body composition
Alan A. Aragon, Brad J. Schoenfeld, Robert Wildman, Susan Kleiner, Trisha VanDusseldorp, Lem Taylor, Conrad P. Earnest, Paul J. Arciero, Colin Wilborn, Douglas S. Kalman, Jeffrey R. Stout, Darryn S. Willoughby, Bill Campbell, Shawn M. Arent, Laurent Banno
Journal of the International Society of Sports Nutrition.2017;[Epub] CrossRef - Relationship between rectus abdominis muscle thickness and metabolic syndrome in middle-aged men
Eun Sil Choi, Soo Hyun Cho, Jung-Ha Kim, Etsuro Ito
PLOS ONE.2017; 12(9): e0185040. CrossRef - Health-related quality of life and activity limitation in an elderly Korean population with sarcopenia: The Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV-2, 3), 2008–2009
T.H. Kim, S.-H. Kim, J. Kim, H.-J. Hwang
European Geriatric Medicine.2017; 8(4): 360. CrossRef - Differential association between sarcopenia and metabolic phenotype in Korean young and older adults with and without obesity
You‐Cheol Hwang, In‐Jin Cho, In‐Kyung Jeong, Kyu Jeung Ahn, Ho Yeon Chung
Obesity.2017; 25(1): 244. CrossRef - Reference Values of Skeletal Muscle Mass for Korean Children and Adolescents Using Data from the Korean National Health and Nutrition Examination Survey 2009-2011
Kirang Kim, Sangmo Hong, Eun Young Kim, Bin He
PLOS ONE.2016; 11(4): e0153383. CrossRef - Insulin sensitivity, body composition and adipose depots following 12 w combined endurance and strength training in dysglycemic and normoglycemic sedentary men
Torgrim Mikal Langleite, Jørgen Jensen, Frode Norheim, Hanne Løvdal Gulseth, Daniel Steensen Tangen, Kristoffer Jensen Kolnes, Ansgar Heck, Tryggve Storås, Guro Grøthe, Marius Adler Dahl, Anders Kielland, Torgeir Holen, Hans Jørgen Noreng, Hans Kristian S
Archives of Physiology and Biochemistry.2016; 122(4): 167. CrossRef - Association between fat free mass and glucose homeostasis: Common knowledge revisited
Karine Perreault, Jean-Christophe Lagacé, Martin Brochu, Isabelle J. Dionne
Ageing Research Reviews.2016; 28: 46. CrossRef - Low skeletal muscle mass is associated with non-alcoholic fatty liver disease in Korean adults: the Fifth Korea National Health and Nutrition Examination Survey
Hee Yeon Kim, Chang Wook Kim, Chung-Hwa Park, Jong Young Choi, Kyungdo Han, Anwar T Merchant, Yong-Moon Park
Hepatobiliary & Pancreatic Diseases International.2016; 15(1): 39. CrossRef - The ratio of skeletal muscle mass to visceral fat area is a main determinant linking circulating irisin to metabolic phenotype
You-Cheol Hwang, Won Seon Jeon, Cheol-Young Park, Byung-Soo Youn
Cardiovascular Diabetology.2016;[Epub] CrossRef - Effects of a weight loss program on body composition and the metabolic profile in obese postmenopausal women displaying various obesity phenotypes: a MONET group study
Eve Normandin, Eric Doucet, Rémi Rabasa-Lhoret, Martin Brochu
Applied Physiology, Nutrition, and Metabolism.2015; 40(7): 695. CrossRef - Analytic morphomics identifies predictors of new‐onset diabetes after liver transplantation
Valerie M. Vaughn, David C. Cron, Michael N. Terjimanian, Zachary S. Gala, Stewart C. Wang, Grace L. Su, Michael L. Volk
Clinical Transplantation.2015; 29(5): 458. CrossRef - Reduced Flexibility Associated with Metabolic Syndrome in Community-Dwelling Elders
Ke-Vin Chang, Chen-Yu Hung, Chia-Ming Li, Yu-Hung Lin, Tyng-Guey Wang, Keh-Sung Tsai, Der-Sheng Han, Diego Fraidenraich
PLOS ONE.2015; 10(1): e0117167. CrossRef - Metabolic risk factors in U.S. youth with low relative muscle mass
Sunkyung Kim, Rodolfo Valdez
Obesity Research & Clinical Practice.2015; 9(2): 125. CrossRef - Comparison of waist to height ratio and body indices for prediction of metabolic disturbances in the Korean population: the Korean National Health and Nutrition Examination Survey 2008–2011
Seok Hui Kang, Kyu Hyang Cho, Jong Won Park, Jun Young Do
BMC Endocrine Disorders.2015;[Epub] CrossRef - N-3 fatty acid intake altered fat content and fatty acid distribution in chicken breast muscle, but did not influence mRNA expression of lipid-related enzymes
Anna Haug, Nicole F Nyquist, Magny Thomassen, Arne T Høstmark, Tone-Kari Knutsdatter Østbye
Lipids in Health and Disease.2014;[Epub] CrossRef - Métodos de análise da composição corporal em adultos obesos
Rávila Graziany Machado de Souza, Aline Corado Gomes, Carla Marques Maia do Prado, João Felipe Mota
Revista de Nutrição.2014; 27(5): 569. CrossRef
- Relationship between adiponectin and muscle mass in patients with metabolic syndrome and obesity
- The Role of Skeletal Muscle in Development of Nonalcoholic Fatty Liver Disease
- Jun Sung Moon, Ji Sung Yoon, Kyu Chang Won, Hyoung Woo Lee
- Diabetes Metab J. 2013;37(4):278-285. Published online August 14, 2013
- DOI: https://doi.org/10.4093/dmj.2013.37.4.278
- 4,637 View
- 49 Download
- 58 Crossref
-
Abstract
PDFPubReader
Background Nonalcoholic fatty liver disease (NAFLD) is closely correlated with abnormal accumulation of visceral fat, but the role of skeletal muscle remains unclear. The aim of this study was to elucidate the role of skeletal muscle in development of NAFLD.
Methods Among 11,116 subjects (6,242 males), we examined the effects of skeletal muscle mass and visceral fat area (VFA, by bioelectric impedance analysis) on NAFLD using by the fatty liver index (FLI).
Results Of the total subjects (9,565 total, 5,293 males) included, 1,848 were classified as having NALFD (FLI ≥60). Body mass index, lipid profile, fasting plasma glucose, hemoglobin A1c, prevalence of type 2 diabetes (DM), hypertension (HTN), and metabolic syndrome were higher in males than females, but FLI showed no significant difference. The low FLI group showed the lowest VFA and highest skeletal muscle mass of all the groups. Skeletal muscle to visceral fat ratio (SVR) and skeletal muscle index had inverse correlations with FLI, when adjusted for age and gender. In multivariate regression analysis, SVR was negatively associated with FLI. Among SVR quartiles, the highest quartile showed very low risk of NAFLD when adjusted for age, gender, lipid profile, DM, HTN, and high sensitivity C-reactive protein from the lowest quartiles (odds ratio, 0.037; 95% confidence interval, 0.029 to 0.049).
Conclusion Skeletal muscle mass was inversely associated with visceral fat area, and higher skeletal muscle mass may have a beneficial effect in preventing NAFLD. These results suggest that further studies are needed to ameliorate or slow the progression of sarcopenia.
-
Citations
Citations to this article as recorded by- Effects of nonalcoholic fatty liver disease on sarcopenia: evidence from genetic methods
Jiaqin Yuan, Jinglin Zhang, Qiang Luo, Lipeng Peng
Scientific Reports.2024;[Epub] CrossRef - Influence of Sugar-Sweetened Beverages Intake on Sarcopenic Obesity, Visceral Obesity, and Sarcopenia in Lebanese Patients with MASLD: A Case-Control Study
Maha Hoteit, Myriam Dagher, Nikolaos Tzenios, Najat Al Kaaki, Ghadir Rkein, Abdul Rahman Chahine, Yonna Sacre, Samer Hotayt, Rami Matar, Mahmoud Hallal, Micheal Maitar, Bilal Hotayt
Healthcare.2024; 12(5): 591. CrossRef - Increased visceral fat area to skeletal muscle mass ratio is positively associated with the risk of metabolic dysfunction-associated steatotic liver disease in a Chinese population
Chenbing Liu, Nan Li, Di Sheng, Yahong Shao, Lihong Qiu, Chao Shen, Zhong Liu
Lipids in Health and Disease.2024;[Epub] CrossRef - Using hyperhomocysteinemia and body composition to predict the risk of non-alcoholic fatty liver disease in healthcare workers
Xiaoyan Hao, Honghai He, Liyuan Tao, Peng Wang
Frontiers in Endocrinology.2023;[Epub] CrossRef - Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review
Claudia-Gabriela Potcovaru, Petruța Violeta Filip, Oana-Maria Neagu, Laura Sorina Diaconu, Teodor Salmen, Delia Cinteză, Anca Pantea Stoian, Florin Bobirca, Mihai Berteanu, Corina Pop
Journal of Clinical Medicine.2023; 12(14): 4713. CrossRef - Association between Muscle Mass Deficits and Metabolic Dysfunction-Associated Fatty Liver Disease in Adults with Body Mass Index Less than 23 kg/m2
Mi Young Lee, Hee Jeong Choi, Han Jin Oh
Korean Journal of Family Practice.2023; 13(3): 171. CrossRef - Sex influences the association between appendicular skeletal muscle mass to visceral fat area ratio and non-alcoholic steatohepatitis in patients with biopsy-proven non-alcoholic fatty liver disease
Gang Li, Rafael S. Rios, Xin-Xin Wang, Yue Yu, Kenneth I. Zheng, Ou-Yang Huang, Liang-Jie Tang, Hong-Lei Ma, Yi Jin, Giovanni Targher, Christopher D. Byrne, Xiao-Yan Pan, Ming-Hua Zheng
British Journal of Nutrition.2022; 127(11): 1613. CrossRef - 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis
Michael H. Le, Yee Hui Yeo, Xiaohe Li, Jie Li, Biyao Zou, Yuankai Wu, Qing Ye, Daniel Q. Huang, Changqing Zhao, Jie Zhang, Chenxi Liu, Na Chang, Feng Xing, Shiping Yan, Zi Hui Wan, Natasha Sook Yee Tang, Maeda Mayumi, Xinting Liu, Chuanli Liu, Fajuan Rui,
Clinical Gastroenterology and Hepatology.2022; 20(12): 2809. CrossRef - Impact of Sarcopenia and Myosteatosis in Non-Cirrhotic Stages of Liver Diseases: Similarities and Differences across Aetiologies and Possible Therapeutic Strategies
Annalisa Cespiati, Marica Meroni, Rosa Lombardi, Giovanna Oberti, Paola Dongiovanni, Anna Ludovica Fracanzani
Biomedicines.2022; 10(1): 182. CrossRef - Impact of Sarcopenia on the Severity of the Liver Damage in Patients With Non-alcoholic Fatty Liver Disease
Vittoria Zambon Azevedo, Cristina Alina Silaghi, Thomas Maurel, Horatiu Silaghi, Vlad Ratziu, Raluca Pais
Frontiers in Nutrition.2022;[Epub] CrossRef - Fatty Liver Index and Skeletal Muscle Density
Julie A. Pasco, Sophia X. Sui, Emma C. West, Kara B. Anderson, Pamela Rufus-Membere, Monica C. Tembo, Natalie K. Hyde, Lana J. Williams, Zoe S. J. Liu, Mark A. Kotowicz
Calcified Tissue International.2022; 110(6): 649. CrossRef - Skeletal muscle mass to visceral fat area ratio as a predictor of NAFLD in lean and overweight men and women with effect modification by sex
Yoosun Cho, Yoosoo Chang, Seungho Ryu, Hyun‐Suk Jung, Chan‐won Kim, Hyungseok Oh, Mi Kyung Kim, Won Sohn, Hocheol Shin, Sarah H. Wild, Christopher D. Byrne
Hepatology Communications.2022; 6(9): 2238. CrossRef - Association of Low Skeletal Muscle Mass with the Phenotype of Lean Non-Alcoholic Fatty Liver Disease
Jun-Hyeon Byeon, Min-Kyu Kang, Min-Cheol Kim
Healthcare.2022; 10(5): 850. CrossRef - Muscle strength, but not body mass index, is associated with mortality in patients with non‐alcoholic fatty liver disease
Phunchai Charatcharoenwitthaya, Khemajira Karaketklang, Wichai Aekplakorn
Journal of Cachexia, Sarcopenia and Muscle.2022; 13(5): 2393. CrossRef - Effect of progressive resistance training with weight loss compared with weight loss alone on the fatty liver index in older adults with type 2 diabetes: secondary analysis of a 12-month randomized controlled trial
Christine L Freer, Elena S George, Sze-Yen Tan, Gavin Abbott, David W Dunstan, Robin M Daly
BMJ Open Diabetes Research & Care.2022; 10(5): e002950. CrossRef - Muscle Krüppel-like factor 15 regulates lipid flux and systemic metabolic homeostasis
Liyan Fan, David R. Sweet, Domenick A. Prosdocimo, Vinesh Vinayachandran, Ernest R. Chan, Rongli Zhang, Olga Ilkayeva, Yuan Lu, Komal S. Keerthy, Chloe E. Booth, Christopher B. Newgard, Mukesh K. Jain
Journal of Clinical Investigation.2021;[Epub] CrossRef - “Bioelectrical impedance analysis in managing sarcopenic obesity in NAFLD”
David J. Hanna, Scott T. Jamieson, Christine S. Lee, Christopher A. Pluskota, Nicole J. Bressler, Peter N. Benotti, Sandeep Khurana, David D. K. Rolston, Christopher D. Still
Obesity Science & Practice.2021; 7(5): 629. CrossRef - Decreased Muscle-to-Fat Mass Ratio Is Associated with Low Muscular Fitness and High Alanine Aminotransferase in Children and Adolescent Boys in Organized Sports Clubs
Kai Ushio, Yukio Mikami, Hiromune Obayashi, Hironori Fujishita, Kouki Fukuhara, Tetsuhiko Sakamitsu, Kazuhiko Hirata, Yasunari Ikuta, Hiroaki Kimura, Nobuo Adachi
Journal of Clinical Medicine.2021; 10(11): 2272. CrossRef - Association of Skeletal Muscle and Adipose Tissue Distribution with Histologic Severity of Non-Alcoholic Fatty Liver
Min-Kyu Kang, Jung-Hun Baek, Young-Oh Kweon, Won-Young Tak, Se-Young Jang, Yu-Rim Lee, Keun Hur, Gyeonghwa Kim, Hye-Won Lee, Man-Hoon Han, Joon-Hyuk Choi, Soo-Young Park, Jung-Gil Park
Diagnostics.2021; 11(6): 1061. CrossRef - Association of Body Composition and Sarcopenia with NASH in Obese Patients
Sophia Marie-Therese Schmitz, Lena Schooren, Andreas Kroh, Alexander Koch, Christine Stier, Ulf Peter Neumann, Tom Florian Ulmer, Patrick Hamid Alizai
Journal of Clinical Medicine.2021; 10(15): 3445. CrossRef - Patchouli alcohol ameliorates skeletal muscle insulin resistance and NAFLD via AMPK/SIRT1-mediated suppression of inflammation
Do Hyeon Pyun, Tae Jin Kim, Seung Yeon Park, Hyun Jung Lee, A.M. Abd El-Aty, Ji Hoon Jeong, Tae Woo Jung
Molecular and Cellular Endocrinology.2021; 538: 111464. CrossRef - Hepatic Steatosis Contributes to the Development of Muscle Atrophy via Inter-Organ Crosstalk
Kenneth Pasmans, Michiel E. Adriaens, Peter Olinga, Ramon Langen, Sander S. Rensen, Frank G. Schaap, Steven W. M. Olde Damink, Florian Caiment, Luc J. C. van Loon, Ellen E. Blaak, Ruth C. R. Meex
Frontiers in Endocrinology.2021;[Epub] CrossRef - Muscle mass and cellular membrane integrity assessment in patients with nonalcoholic fatty liver disease
Iasmin dos Santos Barreto, Raquel Oliveira dos Santos, Raquel Rocha, Claudineia de Souza, Naiade Almeida, Luiza Valois Vieira, Rafael Leiróz, Manoel Sarno, Carla Daltro, Helma Pinchemel Cotrim
Revista da Associação Médica Brasileira.2021; 67(9): 1233. CrossRef - A significant association of non-obese non-alcoholic fatty liver disease with sarcopenic obesity
Kazuhiro Kashiwagi, Michiyo Takayama, Kayoko Fukuhara, Ryoko Shimizu-Hirota, Po-Sung Chu, Nobuhiro Nakamoto, Nagamu Inoue, Yasushi Iwao, Takanori Kanai
Clinical Nutrition ESPEN.2020; 38: 86. CrossRef - Improvement in Menopause-Associated Hepatic Lipid Metabolic Disorders by Herbal Formula HPC03 on Ovariectomized Rats
BoYoon Chang, Dae Sung Kim, SungYeon Kim
Evidence-Based Complementary and Alternative Medicine.2020; 2020: 1. CrossRef - Sarcopenia is associated with non-alcoholic fatty liver disease in men with type 2 diabetes
D.H. Seo, Y.-h. Lee, S.W. Park, Y.J. Choi, B.W. Huh, E. Lee, K.B. Huh, S.H. Kim, B.-S. Cha
Diabetes & Metabolism.2020; 46(5): 362. CrossRef - Nonalcoholic fatty liver disease and sarcopenia: pathophysiological connections and therapeutic implications
Tiziana Fernández-Mincone, Felipe Contreras-Briceño, Maximiliano Espinosa-Ramírez, Patricio García-Valdés, Antonio López-Fuenzalida, Arnoldo Riquelme, Juan Pablo Arab, Daniel Cabrera, Marco Arrese, Francisco Barrera
Expert Review of Gastroenterology & Hepatology.2020; 14(12): 1141. CrossRef - Association between Atrial Fibrillation and Advanced Liver Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease
Min Kyu Kang, Jung Gil Park, Min Cheol Kim
Yonsei Medical Journal.2020; 61(10): 860. CrossRef - Relative fat mass at baseline and its early change may be a predictor of incident nonalcoholic fatty liver disease
Hwi Young Kim, Su Jung Baik, Hye Ah Lee, Byoung Kwon Lee, Hye Sun Lee, Tae Hun Kim, Kwon Yoo
Scientific Reports.2020;[Epub] CrossRef - Fisetin Alleviates Hepatic and Adipocyte Fibrosis and Insulin Resistance in Diet-Induced Obese Mice
Myung-Sook Choi, Ji-Young Choi, Eun-Young Kwon
Journal of Medicinal Food.2020; 23(10): 1019. CrossRef - Relationship between relative skeletal muscle mass and nonalcoholic fatty liver disease: a systematic review and meta-analysis
Changzhou Cai, Xin Song, Yishu Chen, Xueyang Chen, Chaohui Yu
Hepatology International.2020; 14(1): 115. CrossRef - Sarcopenia Is a New Risk Factor of Nonalcoholic Fatty Liver Disease in Patients with Inflammatory Bowel Disease
Min Kyu Kang, Kyeong Ok Kim, Min Cheol Kim, Jung Gil Park, Byung Ik Jang
Digestive Diseases.2020; 38(6): 507. CrossRef - Relationship between Muscle Mass/Strength and Hepatic Fat Content in Post-Menopausal Women
Yajie Zhang, Dajiang Lu, Renwei Wang, Weijie Fu, Shengnian Zhang
Medicina.2019; 55(10): 629. CrossRef - Lower hand grip strength in older adults with non-alcoholic fatty liver disease: a nationwide population-based study
Beom-Jun Kim, Seong Hee Ahn, Seung Hun Lee, Seongbin Hong, Mark W. Hamrick, Carlos M. Isales, Jung-Min Koh
Aging.2019; 11(13): 4547. CrossRef - Nonalcoholic Fatty Liver Disease in Nonobese Subjects of African Origin Has Atypical Metabolic Characteristics
Debbie S Thompson, Ingrid A Tennant, Deanne P Soares, Clive Osmond, Chris D Byrne, Terrence E Forrester, Michael S Boyne
Journal of the Endocrine Society.2019; 3(11): 2051. CrossRef - Sarcopenia in patients with non‐alcoholic fatty liver disease: is it a clinically significant entity?
C. H. De Fré, M. A. De Fré, W. J. Kwanten, B. J. Op de Beeck, L. F. Van Gaal, S. M. Francque
Obesity Reviews.2019; 20(2): 353. CrossRef - Nonalcoholic Fatty Liver Disease in The Rotterdam Study: About Muscle Mass, Sarcopenia, Fat Mass, and Fat Distribution
Louise Johanna Maria Alferink, Katerina Trajanoska, Nicole Stephanie Erler, Josje Dorothea Schoufour, Robert Jacobus de Knegt, M. Arfan Ikram, Harry Leonardus Antonius Janssen, Oscar H. Franco, Herold J. Metselaar, Fernando Rivadeneira, Sarwa Darwish Mura
Journal of Bone and Mineral Research.2019; 34(7): 1254. CrossRef - Sarcopenia Is Significantly Associated with Presence and Severity of Nonalcoholic Fatty Liver Disease
Goh Eun Chung, Min Joo Kim, Jeong Yoon Yim, Joo Sung Kim, Ji Won Yoon
Journal of Obesity & Metabolic Syndrome.2019; 28(2): 129. CrossRef - Association of low skeletal muscle mass with advanced liver fibrosis in patients with non‐alcoholic fatty liver disease
Min Kyu Kang, Jung Gil Park, Heon Ju Lee, Min Cheol Kim
Journal of Gastroenterology and Hepatology.2019; 34(9): 1633. CrossRef - Whole‐body vibration for patients with nonalcoholic fatty liver disease: a 6‐month prospective study
Sechang Oh, Natsumi Oshida, Noriko Someya, Tsuyoshi Maruyama, Tomonori Isobe, Yoshikazu Okamoto, Taeho Kim, Bokun Kim, Junichi Shoda
Physiological Reports.2019; 7(9): e14062. CrossRef - L-Lysine Attenuates Hepatic Steatosis in Senescence-Accelerated Mouse Prone 8 Mice
Tomonori SATO, Nao MURAMATSU, Yoshiaki ITO, Yoshio YAMAMOTO, Takashi NAGASAWA
Journal of Nutritional Science and Vitaminology.2018; 64(3): 192. CrossRef - Short-term treatment with metformin reduces hepatic lipid accumulation but induces liver inflammation in obese mice
Alexandre Abilio de Souza Teixeira, Camila O. Souza, Luana A. Biondo, Loreana Sanches Silveira, Edson A. Lima, Helena A. Batatinha, Adriane Pereira Araujo, Michele Joana Alves, Sandro Massao Hirabara, Rui Curi, José Cesar Rosa Neto
Inflammopharmacology.2018; 26(4): 1103. CrossRef - Vitamin D and Related Deficiencies, Sarcopenia and Visceral Obesity in Obese People with NAFLD
Mihaela Petrova
Gastroenterology & Hepatology: Open Access.2018;[Epub] CrossRef - Grip Strength Moderates the Association between Anthropometric and Body Composition Indicators and Liver Fat in Youth with an Excess of Adiposity
Robinson Ramírez-Vélez, Mikel Izquierdo, Jorge Correa-Bautista, Alejandra Tordecilla-Sanders, María Correa-Rodríguez, Jacqueline Schmidt Rio-Valle, Emilio González-Jiménez, Katherine González-Ruíz
Journal of Clinical Medicine.2018; 7(10): 347. CrossRef - Longitudinal Changes in Muscle Mass and Strength, and Bone Mass in Older Adults: Gender-Specific Associations Between Muscle and Bone Losses
Kyoung Min Kim, Soo Lim, Tae Jung Oh, Jae Hoon Moon, Sung Hee Choi, Jae Young Lim, Ki Woong Kim, Kyong Soo Park, Hak Chul Jang
The Journals of Gerontology: Series A.2018; 73(8): 1062. CrossRef - Non-alcoholic fatty liver disease connections with fat-free tissues: A focus on bone and skeletal muscle
Eleonora Poggiogalle, Lorenzo Maria Donini, Andrea Lenzi, Claudio Chiesa, Lucia Pacifico
World Journal of Gastroenterology.2017; 23(10): 1747. CrossRef - Sarcopenia and non-alcoholic fatty liver disease: Is there a relationship? A systematic review
Cristiane V Tovo, Sabrina A Fernandes, Caroline Buss, Angelo A de Mattos
World Journal of Hepatology.2017; 9(6): 326. CrossRef - Multiple molecular targets in the liver, adipose tissue and skeletal muscle in ginger-elicited amelioration of nonalcoholic fatty liver disease
Chunxia Wang, Robert Batey, Johji Yamahara, Yuhao Li
Journal of Functional Foods.2017; 36: 43. CrossRef - Importance of Lean Muscle Maintenance to Improve Insulin Resistance by Body Weight Reduction in Female Patients with Obesity
Yaeko Fukushima, Satoshi Kurose, Hiromi Shinno, Ha Cao Thu, Nana Takao, Hiromi Tsutsumi, Yutaka Kimura
Diabetes & Metabolism Journal.2016; 40(2): 147. CrossRef - Fatty Liver Index Associates with Relative Sarcopenia and GH/ IGF- 1 Status in Obese Subjects
Eleonora Poggiogalle, Carla Lubrano, Lucio Gnessi, Stefania Mariani, Andrea Lenzi, Lorenzo Maria Donini, Rasheed Ahmad
PLOS ONE.2016; 11(1): e0145811. CrossRef - The relationship between hepatic steatosis and skeletal muscle mass index in men with type 2 diabetes
Yoshitaka Hashimoto, Takafumi Osaka, Takuya Fukuda, Muhei Tanaka, Masahiro Yamazaki, Michiaki Fukui
Endocrine Journal.2016; 63(10): 877. CrossRef - Sarcopenia and the cardiometabolic syndrome: A narrative review
G. Bahat, B. İlhan
European Geriatric Medicine.2016; 7(3): 220. CrossRef - Low skeletal muscle mass is associated with non-alcoholic fatty liver disease in Korean adults: the Fifth Korea National Health and Nutrition Examination Survey
Hee Yeon Kim, Chang Wook Kim, Chung-Hwa Park, Jong Young Choi, Kyungdo Han, Anwar T Merchant, Yong-Moon Park
Hepatobiliary & Pancreatic Diseases International.2016; 15(1): 39. CrossRef - Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications
Sven M. Francque, Denise van der Graaff, Wilhelmus J. Kwanten
Journal of Hepatology.2016; 65(2): 425. CrossRef - Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia
Kyoung Min Kim, Hak Chul Jang, Soo Lim
The Korean Journal of Internal Medicine.2016; 31(4): 643. CrossRef - Relationship between grip strength and newly diagnosed nonalcoholic fatty liver disease in a large-scale adult population
Ge Meng, Hongmei Wu, Liyun Fang, Chunlei Li, Fei Yu, Qing Zhang, Li Liu, Huanmin Du, Hongbin Shi, Yang Xia, Xiaoyan Guo, Xing Liu, Xue Bao, Qian Su, Yeqing Gu, Huijun Yang, Bin Yu, Yuntang Wu, Zhong Sun, Kaijun Niu
Scientific Reports.2016;[Epub] CrossRef - Volume-dependent effect of supervised exercise training on fatty liver and visceral adiposity index in subjects with type 2 diabetes The Italian Diabetes Exercise Study (IDES)
Stefano Balducci, Patrizia Cardelli, Luca Pugliese, Valeria D’Errico, Jonida Haxhi, Elena Alessi, Carla Iacobini, Stefano Menini, Lucilla Bollanti, Francesco G. Conti, Antonio Nicolucci, Giuseppe Pugliese
Diabetes Research and Clinical Practice.2015; 109(2): 355. CrossRef - Sarcopenia is a risk factor for elevated aminotransferase in men independently of body mass index, dietary habits, and physical activity
Ki Deok Yoo, Dae Won Jun, Kang Nyeong Lee, Hang Lak Lee, Oh Young Lee, Byung Chul Yoon, Ho Soon Choi
Digestive and Liver Disease.2015; 47(4): 303. CrossRef
- Effects of nonalcoholic fatty liver disease on sarcopenia: evidence from genetic methods
- Effects of Rosiglitazone on Inflammation in Otsuka Long-Evans Tokushima Fatty Rats
- Jin Woo Lee, Il Seong Nam-Goong, Jae Geun Kim, Chang Ho Yun, Se Jin Kim, Jung Il Choi, Young IL Kim, Eun Sook Kim
- Korean Diabetes J. 2010;34(3):191-199. Published online June 30, 2010
- DOI: https://doi.org/10.4093/kdj.2010.34.3.191
- 4,524 View
- 25 Download
- 7 Crossref
-
Abstract
PDFPubReader
Background Inflammation plays a role in the response to metabolic stress in type 2 diabetes. However, the effects of rosiglitazone on inflammation of skeletal muscle have not been fully examined in type 2 diabetes.
Methods We investigated the effects of the insulin-sensitizing anti-diabetic agent, rosiglitazone, on the progression of skeletal muscle inflammation in Otsuka Long-Evans Tokushima Fatty (OLETF) type 2 diabetic rats. We examined the expression of serologic markers (serum glucose, insulin and free fatty acid) and inflammatory cytokines (tumor-necrosis factor-α, interleukin [IL]-1β and IL-6) in OLETF rats from early to advanced diabetic stage (from 28 to 40 weeks of age).
Results Serum glucose and insulin concentrations were significantly decreased in rosiglitazone-treated OLETF rats compared to untreated OLETF rats. Rosiglitazone treatment significantly decreased the concentrations of serum inflammatory cytokines from 28 to 40 weeks of age. The mRNA expression of various cytokines in skeletal muscle was reduced in rosiglitazone-treated OLETF rats compared with untreated OLETF rats. Furthermore, rosiglitazone treatment resulted in the downregulation of ERK1/2 phosphorylation and NF-κB expression in the skeletal muscle of OLETF rats.
Conclusion These results suggest that rosiglitazone may improve insulin sensitivity with its anti-inflammatory effects on skeletal muscle.
-
Citations
Citations to this article as recorded by- Rosiglitazone Elicits an Adiponectin-Mediated Insulin-Sensitizing Action at the Adipose Tissue-Liver Axis in Otsuka Long-Evans Tokushima Fatty Rats
Jia Li, Yao-Ming Xue, Bo Zhu, Yong-Hua Pan, Yan Zhang, Chunxia Wang, Yuhao Li
Journal of Diabetes Research.2018; 2018: 1. CrossRef - Sirt1 and Sirt6 Mediate Beneficial Effects of Rosiglitazone on Hepatic Lipid Accumulation
Soo Jin Yang, Jung Mook Choi, Eugene Chang, Sung Woo Park, Cheol-Young Park, Aimin Xu
PLoS ONE.2014; 9(8): e105456. CrossRef - Beneficial effects of co-enzyme Q10 and rosiglitazone in fructose-induced metabolic syndrome in rats
Suzan M. Mansour, Hala F. Zaki, Ezz-El-Din S. El-Denshary
Bulletin of Faculty of Pharmacy, Cairo University.2013; 51(1): 13. CrossRef - Chromium Picolinate and Rosiglitazone Improve Biochemical Derangement in a Rat Model of Insulin Resistance: Role of TNF-a and Leptin
Suzan M. Mansour, Hala F. Zaki, Ezz-El-Din El-Denshar
Pharmacologia.2013; 4(3): 186. CrossRef - Angiotensin Receptor Blockade Increases Pancreatic Insulin Secretion and Decreases Glucose Intolerance during Glucose Supplementation in a Model of Metabolic Syndrome
Ruben Rodriguez, Jose A. Viscarra, Jacqueline N. Minas, Daisuke Nakano, Akira Nishiyama, Rudy M. Ortiz
Endocrinology.2012; 153(4): 1684. CrossRef - Rodent Models for Metabolic Syndrome Research
Sunil K. Panchal, Lindsay Brown
Journal of Biomedicine and Biotechnology.2011; 2011: 1. CrossRef - Letter: Effects of Rosiglitazone on Inflammation in Otsuka Long-Evans Tokushima Fatty Rats (Korean Diabetes J 2010;34:191-9)
Soo Jin Yang, Cheol-Young Park
Korean Diabetes Journal.2010; 34(4): 261. CrossRef
- Rosiglitazone Elicits an Adiponectin-Mediated Insulin-Sensitizing Action at the Adipose Tissue-Liver Axis in Otsuka Long-Evans Tokushima Fatty Rats
 First
First Prev
Prev




