- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 44(3); 2020 > Article
-
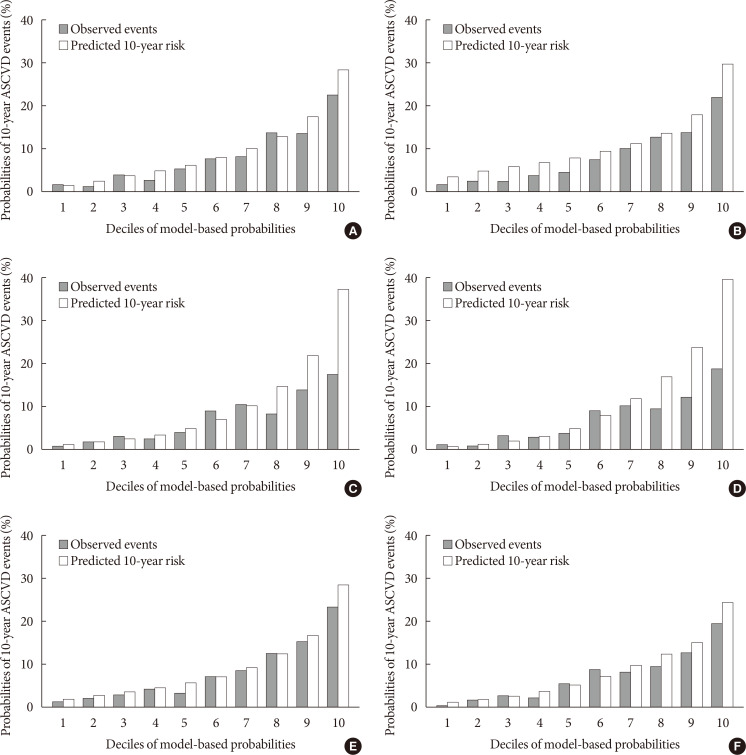
Original ArticleCardiovascular Risk/Epidemiology Validation of Risk Prediction Models for Atherosclerotic Cardiovascular Disease in a Prospective Korean Community-Based Cohort
-
Jae Hyun Bae1
 , Min Kyong Moon2, Sohee Oh3, Bo Kyung Koo2, Nam Han Cho4, Moon-Kyu Lee5
, Min Kyong Moon2, Sohee Oh3, Bo Kyung Koo2, Nam Han Cho4, Moon-Kyu Lee5 -
Diabetes & Metabolism Journal 2020;44(3):458-469.
DOI: https://doi.org/10.4093/dmj.2019.0061
Published online: January 13, 2020
1Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
2Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
3Department of Biostatistics, Seoul National University Boramae Medical Center, Seoul, Korea.
4Department of Preventive Medicine, Ajou University School of Medicine, Suwon, Korea.
5Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding author: Moon-Kyu Lee. Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea. leemk@skku.edu
- *Jae Hyun Bae and Min Kyong Moon contributed equally to this study as first authors.
Copyright © 2020 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
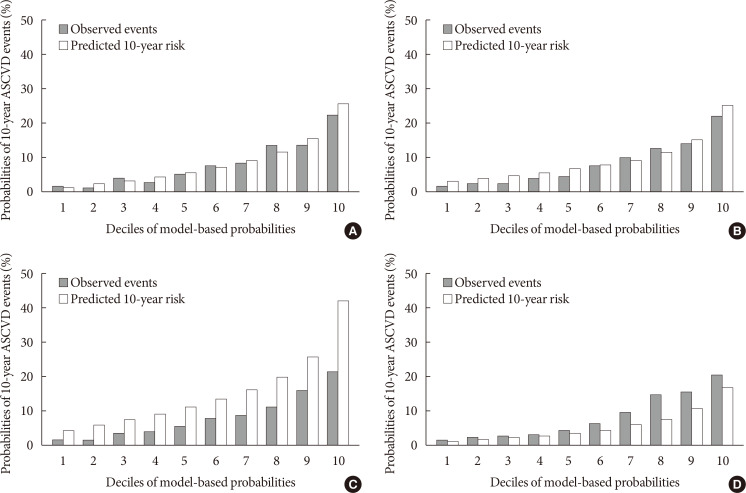
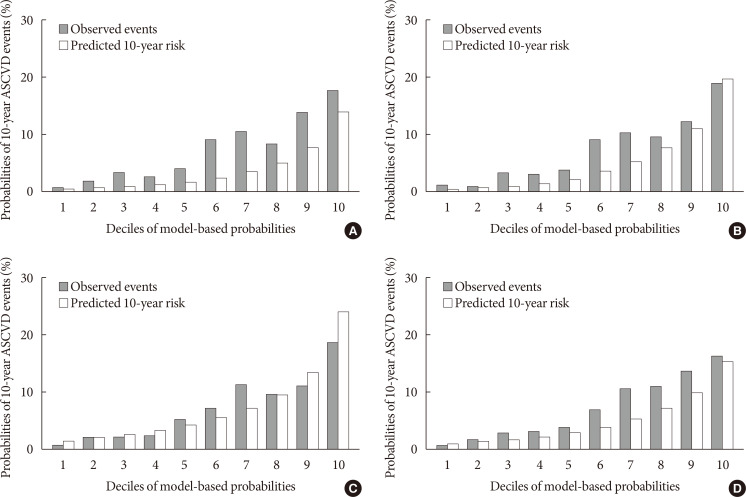
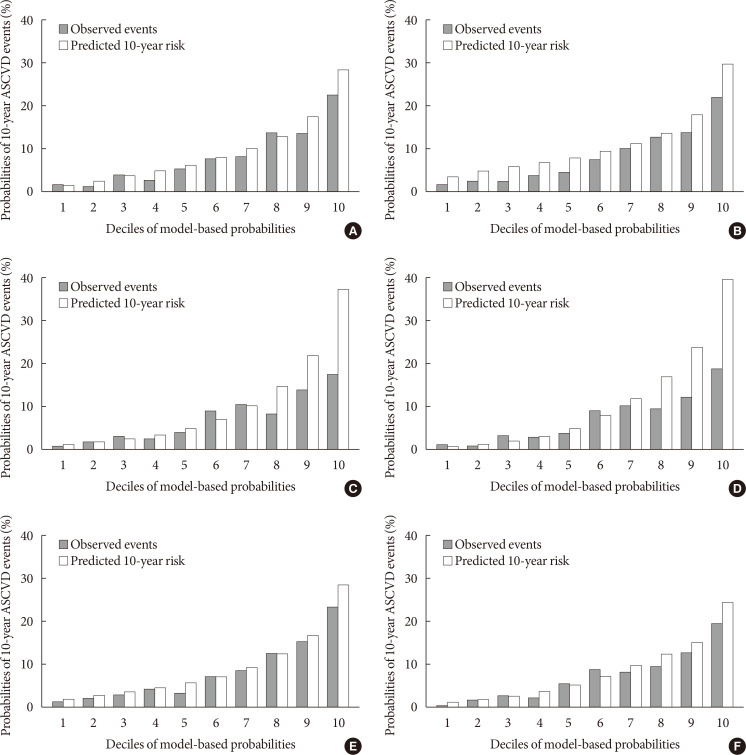
Figure & Data
References
Citations
- Risk Factors for Infertility in Korean Women
Juyeon Lee, Chang-Woo Choo, Kyoung Yong Moon, Sang Woo Lyu, Hoon Kim, Joong Yeup Lee, Jung Ryeol Lee, Byung Chul Jee, Kyungjoo Hwang, Seok Hyun Kim, Sue K. Park
Journal of Korean Medical Science.2024;[Epub] CrossRef - Evaluating cardiovascular disease risk stratification using multiple-polygenic risk scores and pooled cohort equations: insights from a 17-year longitudinal Korean cohort study
Yi Seul Park, Hye-Mi Jang, Ji Hye Park, Bong-Jo Kim, Hyun-Young Park, Young Jin Kim
Frontiers in Genetics.2024;[Epub] CrossRef - Moderation of Weight Misperception on the Associations Between Obesity Indices and Estimated Cardiovascular Disease Risk
Kayoung Lee
International Journal of Behavioral Medicine.2023; 30(1): 89. CrossRef - Validation of the general Framingham Risk Score (FRS), SCORE2, revised PCE and WHO CVD risk scores in an Asian population
Sazzli Shahlan Kasim, Nurulain Ibrahim, Sorayya Malek, Khairul Shafiq Ibrahim, Muhammad Firdaus Aziz, Cheen Song, Yook Chin Chia, Anis Safura Ramli, Kazuaki Negishi, Nafiza Mat Nasir
The Lancet Regional Health - Western Pacific.2023; 35: 100742. CrossRef - Principles of cardiovascular risk management in perimenopausal women with type 2 diabetes
F. O. Ushanova, T. Yu. Demidova, T. N. Korotkova
FOCUS. Endocrinology.2023; 4(2): 19. CrossRef - Prediction of the 10-year risk of atherosclerotic cardiovascular disease in the Korean population
Sangwoo Park, Yong-Giun Kim, Soe Hee Ann, Young-Rak Cho, Shin-Jae Kim, Seungbong Han, Gyung-Min Park
Epidemiology and Health.2023; 45: e2023052. CrossRef - Triglyceride-Glucose Index Predicts Future Atherosclerotic Cardiovascular Diseases: A 16-Year Follow-up in a Prospective, Community-Dwelling Cohort Study
Joon Ho Moon, Yongkang Kim, Tae Jung Oh, Jae Hoon Moon, Soo Heon Kwak, Kyong Soo Park, Hak Chul Jang, Sung Hee Choi, Nam H. Cho
Endocrinology and Metabolism.2023; 38(4): 406. CrossRef - Validity of the models predicting 10-year risk of cardiovascular diseases in Asia: A systematic review and prediction model meta-analysis
Mahin Nomali, Davood Khalili, Mehdi Yaseri, Mohammad Ali Mansournia, Aryan Ayati, Hossein Navid, Saharnaz Nedjat, Hean Teik Ong
PLOS ONE.2023; 18(11): e0292396. CrossRef - Assessing the Validity of the Criteria for the Extreme Risk Category of Atherosclerotic Cardiovascular Disease: A Nationwide Population-Based Study
Kyung-Soo Kim, Sangmo Hong, Kyungdo Han, Cheol-Young Park
Journal of Lipid and Atherosclerosis.2022; 11(1): 73. CrossRef - Mediation of Grip Strength on the Association Between Self-Rated Health and Estimated Cardiovascular Disease Risk
Kayoung Lee
Metabolic Syndrome and Related Disorders.2022; 20(6): 344. CrossRef - Implications of the heterogeneity between guideline recommendations for the use of low dose aspirin in primary prevention of cardiovascular disease
Xiao-Ying Li, Li Li, Sang-Hoon Na, Francesca Santilli, Zhongwei Shi, Michael Blaha
American Journal of Preventive Cardiology.2022; 11: 100363. CrossRef - The Risk of Cardiovascular Disease According to Chewing Status Could Be Modulated by Healthy Diet in Middle-Aged Koreans
Hyejin Chun, Jongchul Oh, Miae Doo
Nutrients.2022; 14(18): 3849. CrossRef - Management of Cardiovascular Risk in Perimenopausal Women with Diabetes
Catherine Kim
Diabetes & Metabolism Journal.2021; 45(4): 492. CrossRef - Comparative performance of the two pooled cohort equations for predicting atherosclerotic cardiovascular disease
Alessandra M. Campos-Staffico, David Cordwin, Venkatesh L. Murthy, Michael P. Dorsch, Jasmine A. Luzum
Atherosclerosis.2021; 334: 23. CrossRef - Usefulness of Relative Handgrip Strength as a Simple Indicator of Cardiovascular Risk in Middle-Aged Koreans
Won Bin Kim, Jun-Bean Park, Yong-Jin Kim
The American Journal of the Medical Sciences.2021; 362(5): 486. CrossRef
 PubReader
PubReader Cite
Cite