- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 42(6); 2018 > Article
-
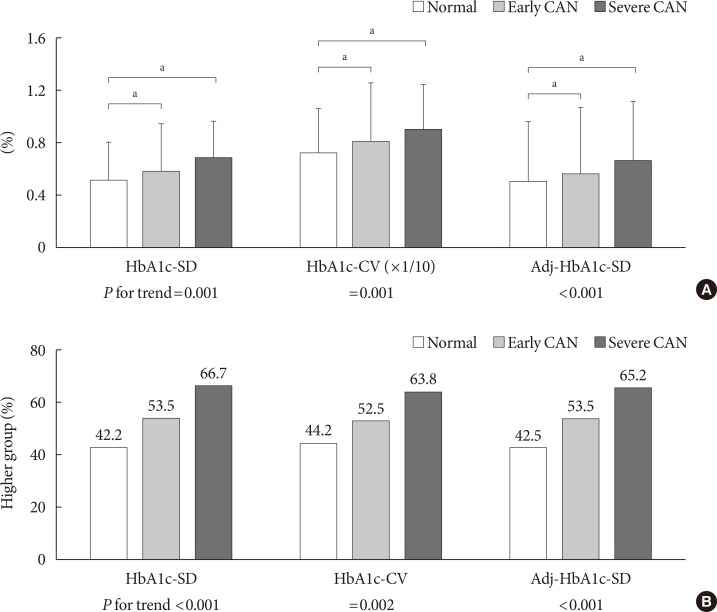
Original ArticleComplications Cardiovascular Autonomic Neuropathy Predicts Higher HbA1c Variability in Subjects with Type 2 Diabetes Mellitus
-
Yeoree Yang1, Eun-Young Lee1, Jae-Hyoung Cho1, Yong-Moon Park2, Seung-Hyun Ko3, Kun-Ho Yoon1,4, Moo-Il Kang1, Bong-Yun Cha1, Seung-Hwan Lee1

-
Diabetes & Metabolism Journal 2018;42(6):496-512.
DOI: https://doi.org/10.4093/dmj.2018.0026
Published online: September 28, 2018
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
2Epidemiology Branch, National Institute of Environmental Health Sciences, National Institutes of Health, Research Triangle Park, NC, USA.
3Division of Endocrinology and Metabolism, Department of Internal Medicine, St. Vincent's Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea.
4Department of Medical Informatics, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- Corresponding author: Seung-Hwan Lee. Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea. hwanx2@catholic.ac.kr
Copyright © 2018 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

Figure & Data
References
Citations
- Intensified glycemic control by HbA1c for patients with coronary heart disease and Type 2 diabetes: a review of findings and conclusions
Jingyang Chen, Dong Yin, Kefei Dou
Cardiovascular Diabetology.2023;[Epub] CrossRef - Long-Term Risk of Cardiovascular Disease Among Type 2 Diabetes Patients According to Average and Visit-to-Visit Variations of HbA1c Levels During the First 3 Years of Diabetes Diagnosis
Hyunah Kim, Da Young Jung, Seung-Hwan Lee, Jae-Hyoung Cho, Hyeon Woo Yim, Hun-Sung Kim
Journal of Korean Medical Science.2023;[Epub] CrossRef - Factors Associated with Diabetic Complication Index among Type 2 Diabetes Patients: Focusing on Regular Outpatient Follow-up and HbA1c Variability
Haejung Lee, Gaeun Park, Ah Reum Khang
Asian Nursing Research.2023; 17(5): 259. CrossRef - The Association of Postprandial Triglyceride Variability with Renal Dysfunction and Microalbuminuria in Patients with Type 2 Diabetic Mellitus: A Retrospective and Observational Study
Natsumi Matsuoka-Uchiyama, Haruhito A. Uchida, Shugo Okamoto, Yasuhiro Onishi, Katsuyoshi Katayama, Mariko Tsuchida-Nishiwaki, Hidemi Takeuchi, Rika Takemoto, Yoshiko Hada, Ryoko Umebayashi, Naoko Kurooka, Kenji Tsuji, Jun Eguchi, Hirofumi Nakajima, Kenic
Journal of Diabetes Research.2022; 2022: 1. CrossRef - Perspectives of glycemic variability in diabetic neuropathy: a comprehensive review
Xiaochun Zhang, Xue Yang, Bao Sun, Chunsheng Zhu
Communications Biology.2021;[Epub] CrossRef - Assessment of Functions of the Autonomic Nervous System in the Elderly with Different Comorbid Factors
Sushma S., Medha Y. Rao, Shaikh Mohammed Aslam
Journal of Neurosciences in Rural Practice.2020; 12: 80. CrossRef - Prognostic irrelevance of plaque vulnerability following plaque sealing in high-risk patients with type 2 diabetes: an optical coherence tomography study
Rosalia Dettori, Andrea Milzi, Kathrin Burgmaier, Mohammad Almalla, Martin Hellmich, Nikolaus Marx, Sebastian Reith, Mathias Burgmaier
Cardiovascular Diabetology.2020;[Epub] CrossRef - HbA1C Variability Is Strongly Associated With the Severity of Cardiovascular Autonomic Neuropathy in Patients With Type 2 Diabetes After Longer Diabetes Duration
Yun-Ru Lai, Chih-Cheng Huang, Wen-Chan Chiu, Rue-Tsuan Liu, Nai-Wen Tsai, Hung-Chen Wang, Wei-Che Lin, Ben-Chung Cheng, Yu-Jih Su, Chih-Min Su, Sheng-Yuan Hsiao, Pei-Wen Wang, Jung-Fu Chen, Cheng-Hsien Lu
Frontiers in Neuroscience.2019;[Epub] CrossRef - Polyscore of Non-invasive Cardiac Risk Factors
Alexander Steger, Alexander Müller, Petra Barthel, Michael Dommasch, Katharina Maria Huster, Katerina Hnatkova, Daniel Sinnecker, Alexander Hapfelmeier, Marek Malik, Georg Schmidt
Frontiers in Physiology.2019;[Epub] CrossRef
 PubReader
PubReader Cite
Cite