
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 38(2); 2014 > Article
-
Original ArticleOthers Factors Associated for Mild Cognitive Impairment in Older Korean Adults with Type 2 Diabetes Mellitus
- Yun Jeong Lee, Hye Mi Kang, Na Kyung Kim, Ju Yeon Yang, Jung Hyun Noh, Kyung Soo Ko, Byoung Doo Rhee, Dong-Jun Kim
-
Diabetes & Metabolism Journal 2014;38(2):150-157.
DOI: https://doi.org/10.4093/dmj.2014.38.2.150
Published online: April 18, 2014
Department of Internal Medicine, Inje University College of Medicine, Busan, Korea.
- Corresponding author: Dong-Jun Kim. Department of Internal Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, 170 Juhwa-ro, Ilsanseo-gu, Goyang 411-706, Korea. djkim@paik.ac.kr
- *These authors are contributed equally to this work.
• Received: May 16, 2013 • Accepted: September 6, 2013
Copyright © 2014 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
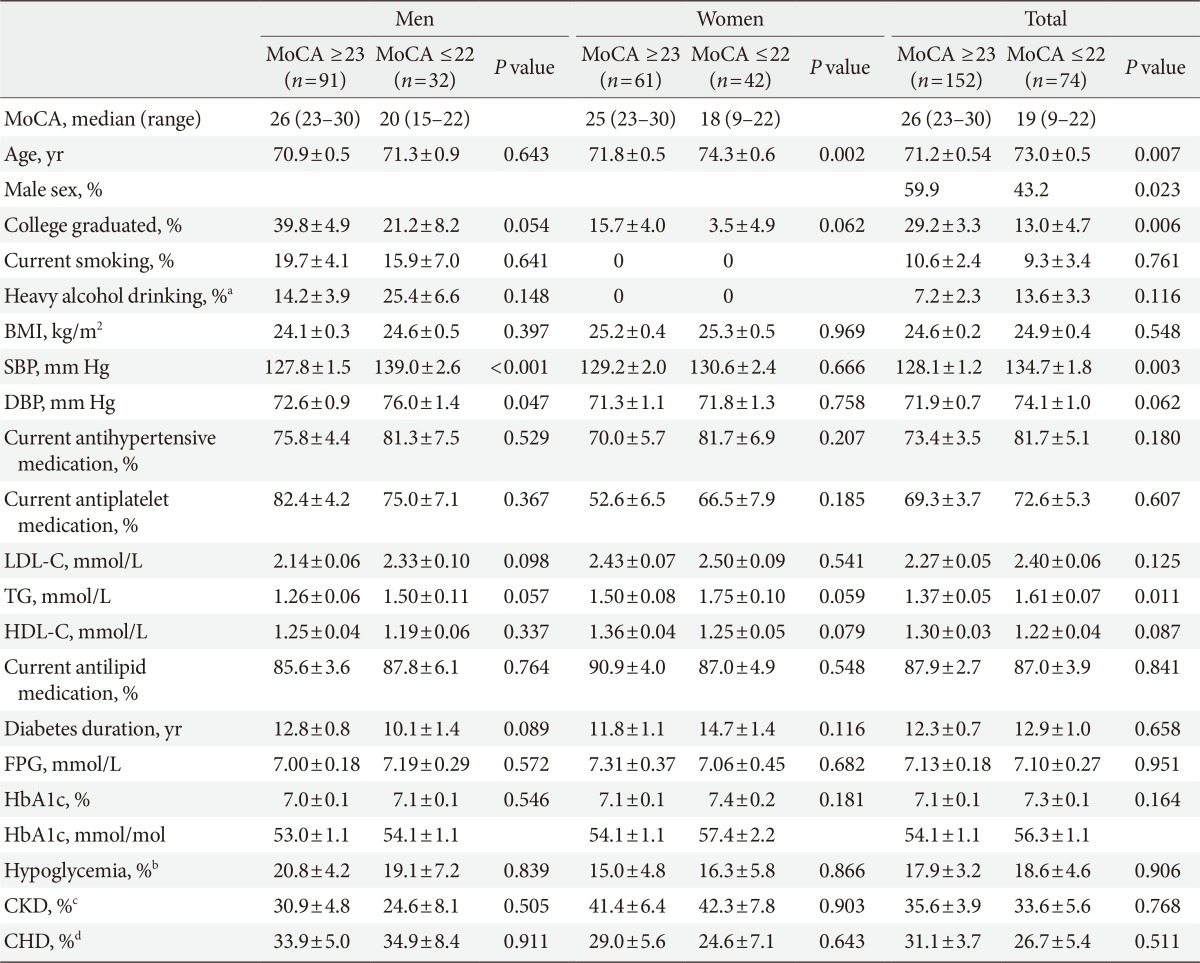
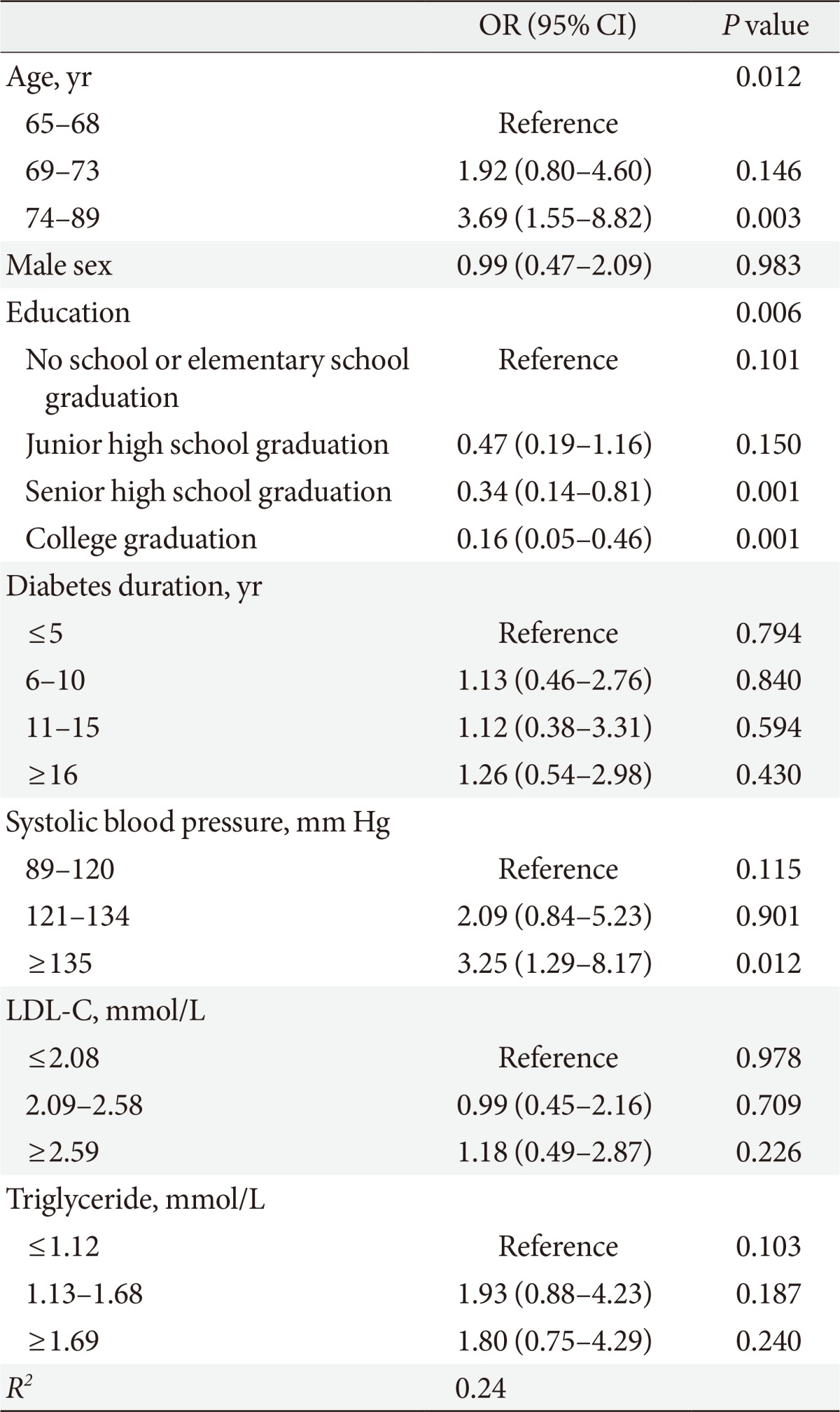
Figure & Data
References
Citations
Citations to this article as recorded by 
- Prediction model for mild cognitive impairment in patients with type 2 diabetes using the autonomic function test
Heeyoung Kang, Juhyeon Kim, Minkyeong Kim, Jin Hyun Kim, Gu Seob Roh, Soo Kyoung Kim
Neurological Sciences.2024;[Epub] CrossRef - Cognitive screening among older adults with diabetes across diverse clinic settings
Deepashree Gupta, Holly Wilhalme, Gabriela Sauder, Tannaz Moin
Diabetes Research and Clinical Practice.2023; 196: 110184. CrossRef - Occurrence of mild cognitive impairment with hyperinsulinaemia in Africans with advanced type 2 diabetes mellitus
J. Bashir, I.U. Yarube
IBRO Neuroscience Reports.2022; 12: 182. CrossRef - Risk factors for cognitive decline in type 2 diabetes mellitus patients in Brazil: a prospective observational study
Ana Cristina Ravazzani de Almeida Faria, Joceline Franco Dall’Agnol, Aline Maciel Gouveia, Clara Inácio de Paiva, Victoria Chechetto Segalla, Cristina Pellegrino Baena
Diabetology & Metabolic Syndrome.2022;[Epub] CrossRef - The TELE-DD project on treatment nonadherence in the population with type 2 diabetes and comorbid depression
Juan Francisco Roy, María Luisa Lozano del Hoyo, Fernando Urcola-Pardo, Alicia Monreal-Bartolomé, Diana Cecilia Gracia Ruiz, María Mercedes Gómez Borao, Ana Belén Artigas Alcázar, José Pedro Martínez Casbas, Alexandra Aceituno Casas, María Teresa Andaluz
Scientific Reports.2021;[Epub] CrossRef - Potential roles of Glucagon-like peptide-1 and its analogues in cognitive impairment associated with type 2 diabetes mellitus
Zi-Wei Yu, Rong Liu, Xin Li, Ying Wang, Yu-Hong Fu, Hui-Yao Li, Yue Yuan, Xin-Yuan Gao
Mechanisms of Ageing and Development.2020; 190: 111294. CrossRef - Predictors of Quality of Life among Older People with Mild Cognitive Impairment Attending Urban Primary Care Clinics
Alexander Lourdes Samy, Shahrul Bahyah Kamaruzzaman, Saroja Krishnaswamy, Wah-Yun Low
Clinical Gerontologist.2020; 43(4): 441. CrossRef - Influence of the Mediterranean and Ketogenic Diets on Cognitive Status and Decline: A Narrative Review
Federica Vinciguerra, Marco Graziano, Maria Hagnäs, Lucia Frittitta, Andrea Tumminia
Nutrients.2020; 12(4): 1019. CrossRef -
ASSOCIATION BETWEEN CHANGES IN THE PSYCHOLOGICAL STATUS AND METABOLIC DISORDERS IN WOMEN WITH ARTERIAL HYPERTENSION, OBESITY AND LEFT VENTRICULAR DIASTOLIC DYSFUNCTION
N. M. Kyrychenko
Bulletin of Problems Biology and Medicine.2020; 4(2): 102. CrossRef - Insulin resistance is a risk factor for mild cognitive impairment in elderly adults with T2DM
Hongjun Zhao, Chenglong Wu, Xiaoping Zhang, Liping Wang, Jianhong Sun, Fuyuan Zhuge
Open Life Sciences.2019; 14(1): 255. CrossRef - Oral diabetes medication and risk of dementia in elderly patients with type 2 diabetes
Ju Young Kim, Young Sook Ku, Hyun Jeong Kim, Nga Thi Trinh, Woorim Kim, Bomi Jeong, Tae Young Heo, Myung Koo Lee, Kyung Eun Lee
Diabetes Research and Clinical Practice.2019; 154: 116. CrossRef - Biomarkers for cognitive decline in patients with diabetes mellitus: evidence from clinical studies
Xue Zhao, Qing Han, You Lv, Lin Sun, Xiaokun Gang, Guixia Wang
Oncotarget.2018; 9(7): 7710. CrossRef - Low education and lack of spousal relationship are associated with dementia in older adults with diabetes mellitus in Nigeria
Abdulkareem J. Yusuf, Olusegun Baiyewu, Adamu G. Bakari, Sani B. Garko, Mohammed E.‐B. Jibril, Aishatu M. Suleiman, Haruna M. Muktar, Micheal A. Amedu
Psychogeriatrics.2018; 18(3): 216. CrossRef - Prevalence and risk factors of cognitive dysfunction in patients with type 2 diabetes mellitus receiving care in a reference hospital in Cameroon: a cross-sectional study
Zainab I. Abba, Yannick Mboue-Djieka, Yacouba N. Mapoure, Cyrille Nkouonlack, Henry N. Luma, Simeon-Pierre Choukem
International Journal of Diabetes in Developing Countries.2018; 38(2): 158. CrossRef - Cognitive impairment among type 2 diabetes mellitus patients at Jimma University Specialized Hospital, Southwest Ethiopia
Dagnew Baye, Desalegn Wolide Amare, Mossie Andualem
Journal of Public Health and Epidemiology.2017; 9(11): 300. CrossRef - Association of metabolic syndrome and 25‐hydroxyvitamin D with cognitive impairment among elderly Koreans
Eun Young Lee, Su Jin Lee, Kyoung Min Kim, Young Mi Yun, Bo Mi Song, Jong Eun Kim, Hyeon Chang Kim, Yumie Rhee, Yoosik Youm, Chang Oh Kim
Geriatrics & Gerontology International.2017; 17(7): 1069. CrossRef - Serum uric acid and impaired cognitive function in community-dwelling elderly in Beijing
Shuangling Xiu, Zheng Zheng, Shaochen Guan, Jin Zhang, Jinghong Ma, Piu Chan
Neuroscience Letters.2017; 637: 182. CrossRef - Assessment of relationship on excess arsenic intake from drinking water and cognitive impairment in adults and elders in arsenicosis areas
Jiayong Liu, Yanhui Gao, Hongxu Liu, Jing Sun, Yang Liu, Junhua Wu, Dandan Li, Dianjun Sun
International Journal of Hygiene and Environmental Health.2017; 220(2): 424. CrossRef - An Update on Type 2 Diabetes Mellitus as a Risk Factor for Dementia
Wei Li, Edgar Huang
Journal of Alzheimer's Disease.2016; 53(2): 393. CrossRef - Current status of managing diabetes mellitus in Korea
Kyoung Hwa Ha, Dae Jung Kim
The Korean Journal of Internal Medicine.2016; 31(5): 845. CrossRef - Type 2 diabetes mellitus is associated with brain atrophy and hypometabolism in the ADNI cohort
Wei Li, Shannon L. Risacher, Edgar Huang, Andrew J. Saykin
Neurology.2016; 87(6): 595. CrossRef - Cardiovascular risk factors and cognitive decline in older people with type 2 diabetes
Insa Feinkohl, Markéta Keller, Christine M. Robertson, Joanne R. Morling, Stela McLachlan, Brian M. Frier, Ian J. Deary, Mark W. J. Strachan, Jackie F. Price
Diabetologia.2015; 58(7): 1637. CrossRef - Association between obesity and depression in patients with diabetes mellitus type 2; a study protocol
Eduardo De la Cruz-Cano, Carlos Alfonso Tovilla-Zarate, Emilio Reyes-Ramos, Thelma Beatriz Gonzalez-Castro, Isela Juarez-Castro, Maria Lilia López-Narváez, Ana Fresan
F1000Research.2015; 4: 7. CrossRef
 PubReader
PubReader Cite
Cite- Related articles
-
- Risk Prediction and Management of Chronic Kidney Disease in People Living with Type 2 Diabetes Mellitus
- Optimal Low-Density Lipoprotein Cholesterol Level for Primary Prevention in Koreans with Type 2 Diabetes Mellitus
- Intensified Multifactorial Intervention in Patients with Type 2 Diabetes Mellitus
- Blood Pressure Target in Type 2 Diabetes Mellitus
- Not Control but Conquest: Strategies for the Remission of Type 2 Diabetes Mellitus



