- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 36(3); 2012 > Article
-
Sulwon Lecture 2011Pathophysiology Post-Renal Transplant Diabetes Mellitus in Korean Subjects: Superimposition of Transplant-Related Immunosuppressant Factors on Genetic and Type 2 Diabetic Risk Factors
- Hyun Chul Lee
-
Diabetes & Metabolism Journal 2012;36(3):199-206.
DOI: https://doi.org/10.4093/dmj.2012.36.3.199
Published online: June 14, 2012
Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- Corresponding author: Hyun Chul Lee. Department of Internal Medicine, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea. endohclee@yuhs.ac
Copyright © 2012 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- ABSTRACT
- INTRODUCTION
- INCIDENCE OF POSTRENAL TRANSPLANTATION DIABETES MELLITUS
- TRANSPLANT-ASSOCIATED RISK FACTORS AND TRADITIONAL TYPE 2 DIABETES RISK FACTORS OF PTDM
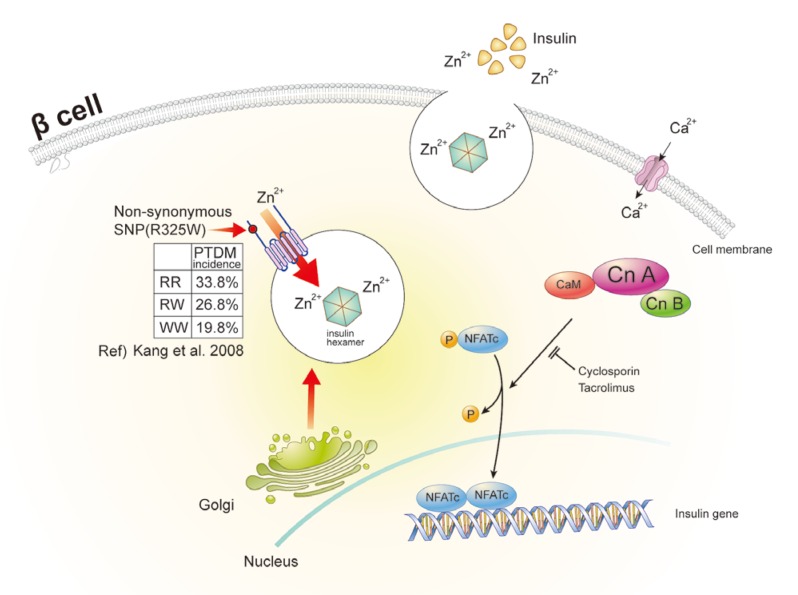
- PATHOPHYSIOLOGY OF PTDM: β-CELL DYSFUNCTION RATHER THAN INSULIN RESISTANCE
- GENETIC RISK FACTORS OF PTDM AND CLINICAL IMPLICATIONS OF ZINC TRANSPORTER-8 GENE IN RENAL TRANSPLANTATION
- CONCLUSIONS
- NOTES
- REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Risk Factors Related to New-Onset Diabetes after Renal Transplantation in Patients of a High Complexity University Hospital in Colombia, 20 Years of Experience
Guillermo E. Guzmán, Angela M. Victoria, Isabella Ramos, Alejandro Maldonado, Eliana Manzi, Juan F. Contreras-Valero, Liliana Mesa, Johanna Schweineberg, Juan G. Posada, Jorge I. Villegas, Luis A. Caicedo, Carlos E. Durán
International Journal of Endocrinology.2020; 2020: 1. CrossRef - Synthesis of Fructose Biosensors and Progressing Their Efficiency Using Californium Colloidal Nanoparticles for Detecting Fructose and Triglycerides
Alireza Heidari
Advanced Science, Engineering and Medicine.2020; 12(8): 1002. CrossRef - Comparison of Glucose Tolerance between Kidney Transplant Recipients and Healthy Controls
Hisao Shimada, Junji Uchida, Shunji Nishide, Kazuya Kabei, Akihiro Kosoku, Keiko Maeda, Tomoaki Iwai, Toshihide Naganuma, Yoshiaki Takemoto, Tatsuya Nakatani
Journal of Clinical Medicine.2019; 8(7): 920. CrossRef - Diabètes post-transplantation rénale
Danièle Dubois-Laforgue
Néphrologie & Thérapeutique.2017; 13: S137. CrossRef - Risk assessment and management of post-transplant diabetes mellitus
Eugene Han, Myoung Soo Kim, Yu Seun Kim, Eun Seok Kang
Metabolism.2016; 65(10): 1559. CrossRef - Renal posttransplantation diabetes mellitus: An overview
Ana Laura Pimentel, Andrea Carla Bauer, Joíza Lins Camargo
Clinica Chimica Acta.2015; 450: 327. CrossRef - HMG CoA Reductase Inhibitor Treatment Induces Dysglycemia in Renal Allograft Recipients
Eun Yeong Choe, Hye Jin Wang, Obin Kwon, Yongin Cho, Kyu Ha Huh, Myoung Soo Kim, Yu Seun Kim, Chul Woo Ahn, Bong Soo Cha, Hyun Chul Lee, Eun Seok Kang
Transplantation.2014; 97(4): 419. CrossRef - Statin therapy is associated with the development of new-onset diabetes after transplantation in liver recipients with high fasting plasma glucose levels
Yongin Cho, Min Jung Lee, Eun Yeong Choe, Chang Hee Jung, Dong Jin Joo, Myoung Soo Kim, Bong Soo Cha, Joong-Yeol Park, Eun Seok Kang
Liver Transplantation.2014; 20(5): 557. CrossRef - Post-Transplant Diabetes Mellitus: Is It Associated With Poor Allograft Outcomes in Renal Transplants?
J.Y. Choi, O.J. Kwon
Transplantation Proceedings.2013; 45(8): 2892. CrossRef
 PubReader
PubReader Cite
Cite