- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 44(1); 2020 > Article
-
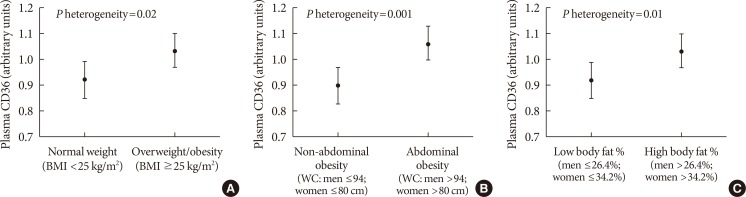
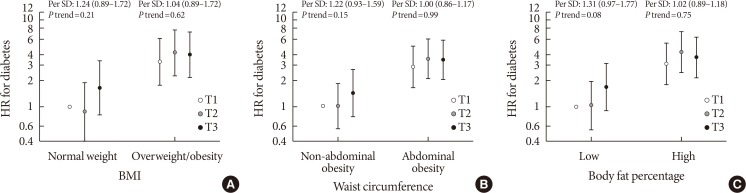
Original ArticleMetabolic Risk/Epidemiology Plasma CD36 and Incident Diabetes: A Case-Cohort Study in Danish Men and Women
-
Yeli Wang1
 , Jingwen Zhu2, Sarah Aroner2, Kim Overvad3,4, Tianxi Cai5, Ming Yang5, Anne Tjønneland6, Aase Handberg7,8, Majken K. Jensen2,9
, Jingwen Zhu2, Sarah Aroner2, Kim Overvad3,4, Tianxi Cai5, Ming Yang5, Anne Tjønneland6, Aase Handberg7,8, Majken K. Jensen2,9 -
Diabetes & Metabolism Journal 2020;44(1):134-142.
DOI: https://doi.org/10.4093/dmj.2018.0273
Published online: October 18, 2019
1Health Services and Systems Research, Duke-NUS Medical School, Singapore.
2Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
3Department of Cardiology, Aalborg University Hospital, Aalborg, Denmark.
4Section for Epidemiology, Department of Public Health, Aarhus University, Aarhus, Denmark.
5Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
6Danish Cancer Society Research Center, Copenhagen, Denmark.
7Department of Clinical Biochemistry, Aalborg University Hospital, Aalborg, Denmark.
8Department of Clinical Medicine, Faculty of Medicine, Aalborg University, Aalborg, Denmark.
9Channing Division of Network Medicine, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
- Corresponding author: Majken K. Jensen. Department of Nutrition, Harvard T.H. Chan School of Public Health, 677 Huntington Avenue, Boston, MA 02115, USA. mkjensen@hsph.harvard.edu
- *Yeli Wang and Jingwen Zhu contributed equally to this study as first authors.
Copyright © 2020 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
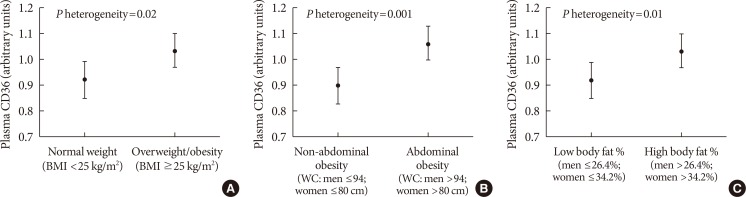
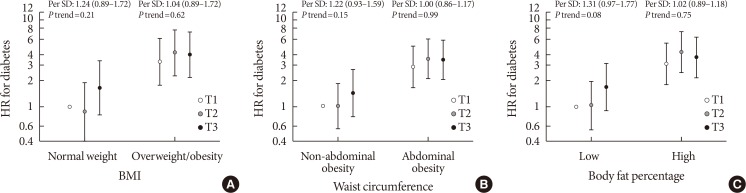
Figure & Data
References
Citations
- The Multifunctionality of CD36 in Diabetes Mellitus and Its Complications—Update in Pathogenesis, Treatment and Monitoring
Kamila Puchałowicz, Monika Ewa Rać
Cells.2020; 9(8): 1877. CrossRef - The Role of CD36 in Type 2 Diabetes Mellitus: β-Cell Dysfunction and Beyond
Jun Sung Moon, Udayakumar Karunakaran, Elumalai Suma, Seung Min Chung, Kyu Chang Won
Diabetes & Metabolism Journal.2020; 44(2): 222. CrossRef
 PubReader
PubReader Cite
Cite