
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 47(2); 2023 > Article
-
Original ArticleComplications Non-Alcoholic Fatty Liver Disease with Sarcopenia and Carotid Plaque Progression Risk in Patients with Type 2 Diabetes Mellitus
-
Yongin Cho1*
 , Hye-Sun Park2*, Byung Wook Huh3, Yong-ho Lee4, Seong Ha Seo1, Da Hea Seo1, Seong Hee Ahn1, Seongbin Hong1, So Hun Kim1
, Hye-Sun Park2*, Byung Wook Huh3, Yong-ho Lee4, Seong Ha Seo1, Da Hea Seo1, Seong Hee Ahn1, Seongbin Hong1, So Hun Kim1 -
Diabetes & Metabolism Journal 2023;47(2):232-241.
DOI: https://doi.org/10.4093/dmj.2021.0355
Published online: January 19, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Inha University College of Medicine, Incheon, Korea
2Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
3Huh’s Diabetes Center and the 21st Century Diabetes and Vascular Research Institute, Seoul, Korea
4Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea
-
Corresponding author: So Hun Kim Division of Endocrinology and Metabolism, Department of Internal Medicine, Inha University College of Medicine, 27 Inhang-ro, Jung-gu, Incheon 22332, Korea E-mail: shoney@inha.ac.kr
- *Yongin Cho and Hye-Sun Park contributed equally to this study as first authors.
Copyright © 2023 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- We aimed to evaluate whether non-alcoholic fatty liver disease (NAFLD) with or without sarcopenia is associated with progression of carotid atherosclerosis in patients with type 2 diabetes mellitus (T2DM).
-
Methods
- We investigated 852 T2DM patients who underwent abdominal ultrasonography, bioelectrical impedance analysis, and carotid artery ultrasonography at baseline and repeated carotid ultrasonography after 6 to 8 years. NAFLD was confirmed by abdominal ultrasonography, and sarcopenia was defined as a sex-specific skeletal muscle mass index (SMI) value <2 standard deviations below the mean for healthy young adults. SMI was calculated by dividing the sum of appendicular skeletal mass by body weight. We investigated the association between NAFLD with or without sarcopenia and the progression of carotid atherosclerosis.
-
Results
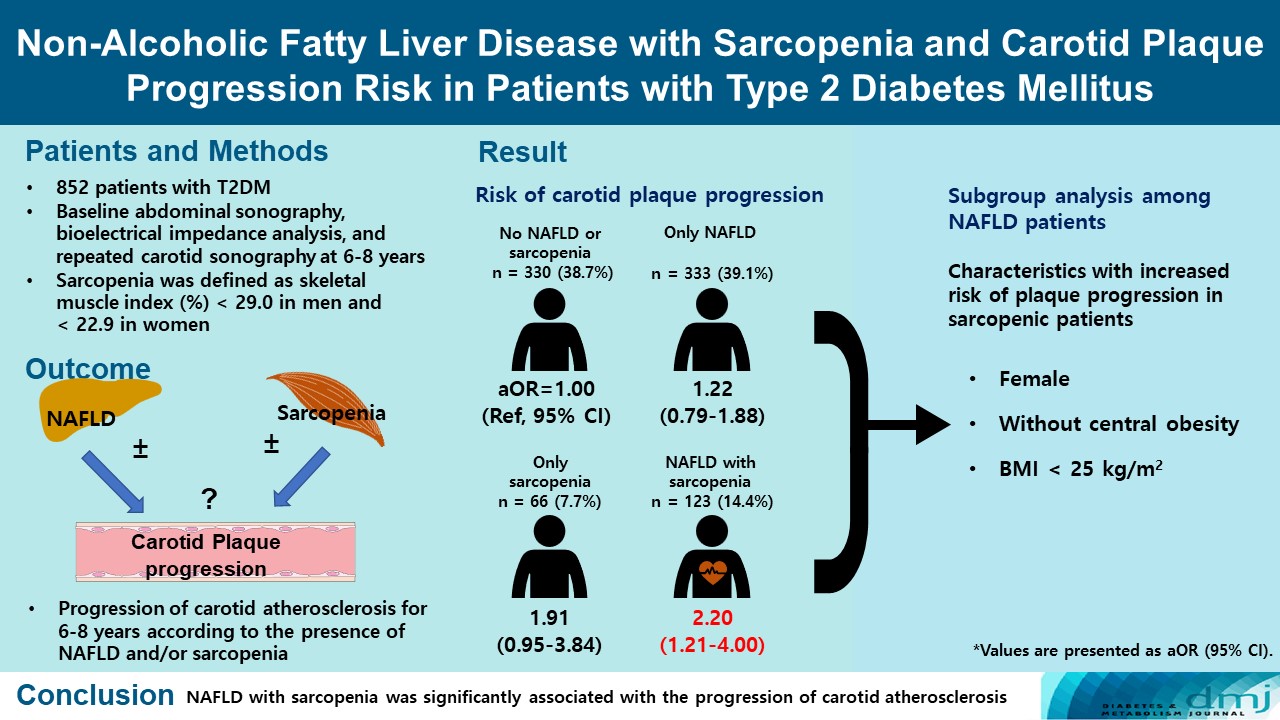
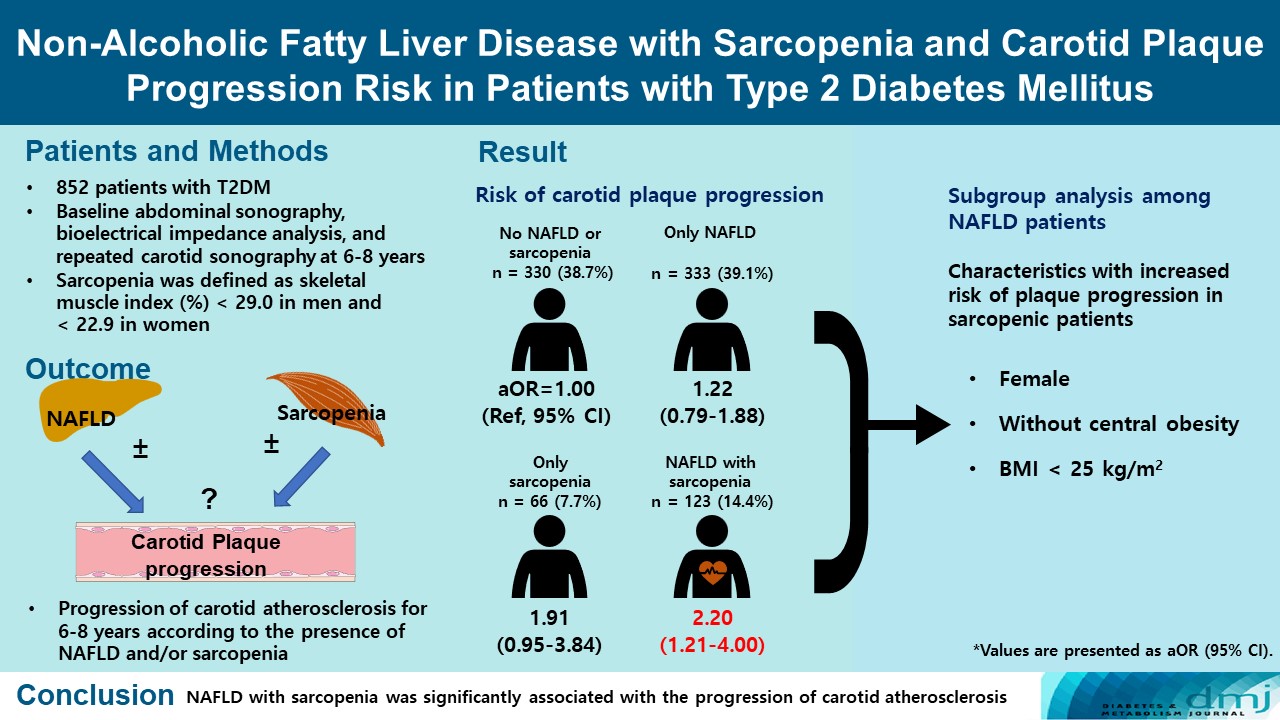
- Of the 852 patients, 333 (39.1%) were classified as NAFLD without sarcopenia, 66 (7.7%) were classified as sarcopenia without NAFLD, and 123 (14.4%) had NAFLD with sarcopenia at baseline. After 6 to 8 years, patients with both NAFLD and sarcopenia had a higher risk of atherosclerosis progression (adjusted odds ratio, 2.20; P<0.009) than controls without NAFLD and sarcopenia. When a subgroup analysis was performed on only patients with NAFLD, female sex, absence of central obesity, and non-obesity were significant factors related to increased risk of plaque progression risk in sarcopenic patients.
-
Conclusion
- NAFLD with sarcopenia was significantly associated with the progression of carotid atherosclerosis in T2DM patients.
- Non-alcoholic fatty liver disease (NAFLD), the hepatic manifestation of ectopic fat accumulation caused by abdominal obesity and insulin resistance, is a well-known risk factor for cardiovascular disease (CVD), which is the leading cause of death in patients with steatohepatitis [1,2]. In particular, the risk of NAFLD increases in patients with type 2 diabetes mellitus (T2DM); NAFLD affects approximately 70% of the T2DM population [3]. However, it is currently unclear whether simple steatosis without hepatic fibrosis is associated with a higher CVD risk [4]. In a previous study of patients with T2DM, the risk of atherosclerosis progression was significantly higher in NAFLD patients with advanced liver fibrosis; however, no significant increase in risk was identified in simple steatosis without advanced liver fibrosis [5]. Therefore, the selection of patients with high CVD risk within the T2DM patient group with NAFLD can be an important clinical issue. However, it is not easy to determine whether hepatic fibrosis, the representative risk factor of high CVD risk, exists because of limited diagnostic modalities, such as liver biopsy or magnetic resonance elastography.
- The loss of muscle mass and muscle function, known as sarcopenia, is part of a physiologic aging process, and is usually exacerbated by low physical activity, malnutrition, and inflammatory conditions [6]. Recent studies revealed a close relationship between NAFLD and sarcopenia, suggesting that sarcopenia is an independent risk factor for NAFLD [7]. Han et al. [8] reported that NAFLD and sarcopenia were independently associated with an increased risk of atherosclerotic CVD in a large-scale cross-sectional study. The risk of subclinical atherosclerosis assessed by carotid ultrasonography has also been reported to increase with sarcopenia in patients with NAFLD in a cross-sectional analysis [9].
- Because muscle is the major organ for glucose disposal after a meal, the loss of muscle mass consequently results in insulin resistance [10,11], and insulin resistance is a characteristic feature of both T2DM and NAFLD [12]. However, although NAFLD and sarcopenia share a common mechanism in the pathogenesis of insulin resistance, little is known about the longitudinal effects of NAFLD with or without sarcopenia on systemic atherosclerosis in T2DM. In this study, we aimed to evaluate whether sarcopenia with NAFLD leads to an increased risk of CVD in an Asian population with T2DM. To evaluate the CVD risk, the progression of carotid atherosclerosis for 6 to 8 years was evaluated.
INTRODUCTION
- In this study, we analyzed data from the Seoul Metabolic Syndrome Cohort, wherein 13,296 patients were diagnosed and treated for T2DM from November 1997 to September 2016 at Huh’s Diabetes Center as previously described [13,14]. The patients were diagnosed with T2DM according to the American Diabetes Association criteria [15]. Among T2DM patients in the cohort, those aged ≥19 years who had undergone carotid artery ultrasonography repeatedly for up to 6–8 years were enrolled. Patients with bilateral carotid artery plaques at baseline were excluded because it was difficult to confirm new-onset plaques during the follow-up period in those patients. Patients were also excluded based on the following criteria: (1) age <19 years; (2) diagnosis of type 1 diabetes mellitus; (3) pregnancy; (4) diagnosis of liver disease other than NAFLD, such as viral or autoimmune hepatitis and hepatocellular carcinoma; and (5) history of heavy alcohol consumption (>140 g/week).
- The final participants included 852 patients who underwent abdominal ultrasonography, bioelectrical impedance analysis, and carotid artery ultrasonography at baseline and repeated carotid artery ultrasonography after 6 to 8 years. Written informed consent was obtained from all participants, and the Ethics Committee of Inha University Hospital approved this study (2021-08-026).
- Measurements and definitions of clinical and laboratory parameters
- We collected baseline information of the patients, including their medical and family history, smoking and alcohol consumption history, medication use, and physical activity level per week. Anthropometric measurements, including weight, height, and waist circumference (WC) were performed. Venous blood samples were drawn from participants (1) after 8 hours of fasting, and (2) 2 hours after a meal. The metabolic parameters including glycosylated hemoglobin (HbA1c), lipid profiles (total cholesterol, triglyceride, high-density lipoprotein cholesterol [HDL-C], and low-density lipoprotein cholesterol [LDL-C]), blood urea nitrogen, creatinine, aspartate aminotransferase/alanine aminotransferase (AST/ALT), and albumin were measured using routine laboratory methods on fresh samples on the same day of collection. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation [16]. Patients underwent a short insulin tolerance test to calculate the rate constant for plasma glucose disappearance (KITT; %/min), which is a marker of insulin sensitivity [17]. Regular alcohol consumers were defined as individuals who drank twice a month or more, and those who had ever smoked five or more packs of cigarettes were considered ever-smokers. Regular exercise was defined as moderate to vigorous physical activity at least once per month for at least 30 minutes. Obesity was defined as a body mass index (BMI) ≥25 kg/m2 according to a scientific statement from the World Health Organization [18]. Central obesity was defined as WC ≥90 cm for men and ≥85 cm for women according to the Korean standard for central obesity [19].
- Liver status and body composition measurements
- Participants underwent abdominal ultrasonography after 8 hours of fasting to assess whether they had hepatic steatosis (iU22, Philips Healthcare, Andover, MA, USA, using a 3.5- MHz transducer after 8 hours of fasting). As previously described, the degree of steatosis was assessed semi-quantitatively (absent, mild, moderate, or severe), and NAFLD was defined as the presence of hepatic steatosis on ultrasound [7]. The body composition of the participants was assessed using a segmental multi-frequency bioelectrical impedance analysis system (InBody 4.0, InBody Co. Ltd., Seoul, Korea). The appendicular skeletal mass (ASM) was calculated as the sum of lean muscle mass in bilateral upper and lower limbs, and the skeletal muscle mass index (SMI) was calculated by dividing the ASM by body weight in kg (SMI=ASM/body weight×100%) and subsequently expressed as a percentage [20]. Sarcopenia was defined as an SMI (%) <2 standard deviations (SDs) below the gender-specific mean for healthy young adults in the Korean population: SMI (%) <29.0 in men and <22.9 in women was considered as sarcopenia [21].
- For sensitivity analysis, a different definition of sarcopenia, sarcopeniaheight, which was calculated by dividing the ASM by height2 in m2 was used. Sarcopeniaheight was defined as an ASM/height2 <7.0 in men and <5.7 in women [22].
- Carotid atherosclerosis measurements
- All participants underwent repeated carotid ultrasonography to assess the carotid atherosclerosis status. We compared the progression of atherosclerosis at baseline and at 6 to 8 years. Both common carotid arteries were examined using high-resolution ultrasonography (LOGIQ7, GE Healthcare, Chicago, IL, USA) by trained technicians who were blinded to the patients’ clinical and laboratory data. The middle and distal common carotid arteries were scanned as described previously [5]. The presence of carotid plaque was defined as meeting any one of the following criteria: (1) carotid intima-media thickness (CIMT) of 1.5 mm or higher; (2) protrusion of atherosclerosis into the lumen of the artery with ≥50% thickness compared to the surrounding area; and (3) presence of distinct areas of hyperechogenicity [23]. The progression of carotid atherosclerosis was defined as the appearance of newly developed carotid plaque lesions on repeated ultrasonography.
- Statistical analysis
- The baseline characteristics of the study participants were analyzed according to the presence of NAFLD and sarcopenia. The patients were divided into four groups: no NAFLD or sarcopenia, NAFLD only, sarcopenia only, and NAFLD with sarcopenia. All categorical variables were expressed as numbers (proportions) and compared using the chi-square test. Continuous variables were expressed as mean±SD and analyzed with one-way analysis of variance (ANOVA) for intergroup comparison, followed by the Bonferroni test for post hoc analysis. Multivariable logistic regression analysis was performed to calculate the odds ratio (OR) of carotid atherosclerosis progression according to the presence of NAFLD with or without sarcopenia. Various confounding factors were adjusted in a stepwise manner: age and sex were adjusted in Model 2; BMI, follow-up duration, smoking, alcohol consumption, history of hypertension, and exercise were adjusted in Model 3; eGFR, diabetes mellitus (DM) duration, and HbA1c were adjusted in Model 4; use of statins, LDL-C, triglycerides, HDL-C, and history of cardio-cerebrovascular disease in Model 5. In addition, a subgroup analysis was performed to assess the factors influencing the association between the coexistence of sarcopenia in patients with NAFLD and carotid atherosclerosis progression. A logistic regression analysis was performed to detect the association between sarcopenia and carotid atherosclerosis progression after dividing patients with NAFLD into two subgroups by age (60 years), sex, DM duration (6 years, median value of study population), central obesity (WC; 90 cm for men and 85 cm for women), and BMI (obesity: 25.0 kg/m2). Statistical significance was set at P<0.05; additionally, all statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA).
METHODS
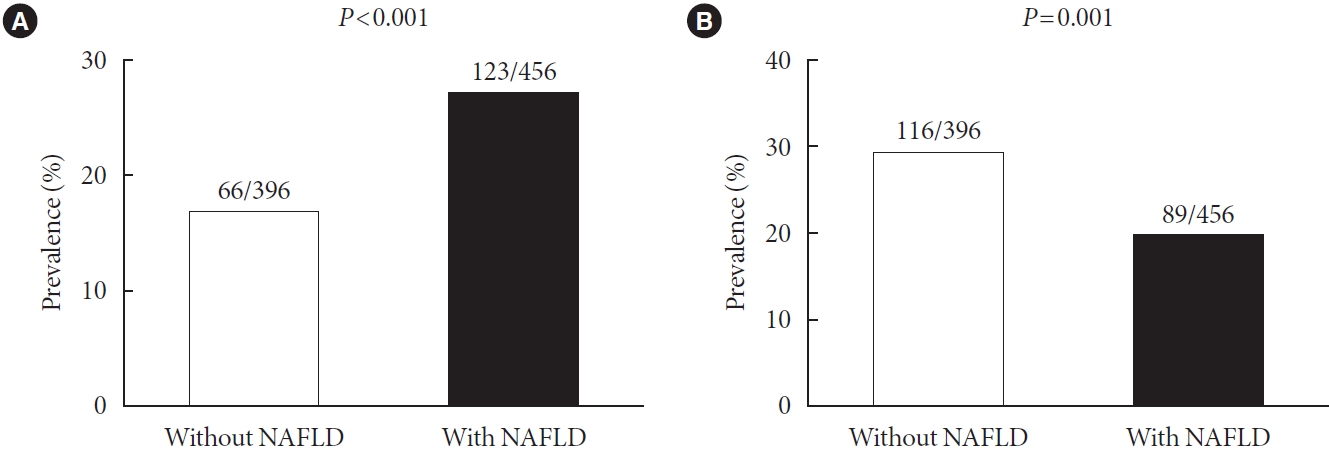
- A total of 852 patients with T2DM were enrolled in this study. Of the 852 patients, 456 had NAFLD and 189 had sarcopenia. Patients with NAFLD showed a higher prevalence of sarcopenia than those without NAFLD (27.0% vs. 16.7%, P<0.001) (Fig. 1A). However, the difference of prevalence of sarcopenia between the groups was inverse when we used another definition of sarcopenia (19.5% vs. 29.3%, P=0.001) (Fig. 1B). The baseline characteristics of the participants are shown in Table 1. Patients with both NAFLD and sarcopenia showed significantly greater body weight, BMI, WC, and visceral fat than those in the other groups (all P<0.05). In addition, the proportion of central obesity and hypertension was significantly higher in patients with both NAFLD and sarcopenia (all P<0.05). AST and ALT were significantly greater and insulin sensitivity measured by KITT was significantly lower in those with NAFLD, regardless of sarcopenia (all P<0.05).
- The mean CIMTs (mm) at baseline were 0.76±0.15, 0.77±0.15, 0.74±0.14, and 0.79±0.14 in patients with no NAFLD/sarcopenia, NAFLD only, sarcopenia only, and NAFLD with sarcopenia, respectively (P=0.042). The numbers of participants with carotid plaques at baseline were 115 (34.8%), 107 (32.1%), 19 (28.8%), and 46 (37.4%) in patients with no NAFLD/sarcopenia, NAFLD only, sarcopenia only, and NAFLD with sarcopenia. It was not significantly different among the four subgroups (P=0.567).
- After a mean of 7 years of follow-up, plaque progression was confirmed in 291 of 852 participants, and the number in each group were 86 (26.1%), 109 (32.7%), 35 (53.0%), and 61 (49.6%) in patients with no NAFLD/sarcopenia, NAFLD only, sarcopenia only, and NAFLD with sarcopenia, respectively (P<0.001). The association between the presence of NAFLD/sarcopenia and carotid plaque progression after multistep adjustments is shown in Table 2. Age, sex, BMI, follow-up duration, smoking, alcohol consumption, history of hypertension, exercise, eGFR, T2DM duration, HbA1c, use of statins, LDLC, triglyceride, HDL-C, and history of cardio-cerebrovascular disease were sequentially adjusted. In the NAFLD with sarcopenia group, a consistently significantly higher OR was confirmed compared to the control group (no NAFLD or sarcopenia) after adjustment (adjusted OR [aOR], 2.2; 95% confidence interval, 1.21 to 4.00; P=0.01). In addition, the same result was also confirmed in the sensitivity analysis which used a different definition (sarcopeniaheight) (Table 2).
- There were 271 patients who followed both abdominal ultrasonography and segmental multi-frequency bioelectrical impedance analysis simultaneously after 6 to 8 years of follow-up. There was no change in group classification in most patients, however, a high proportion of patients with sarcopenia without NAFLD developed new NAFLD (Supplementary Table 1).
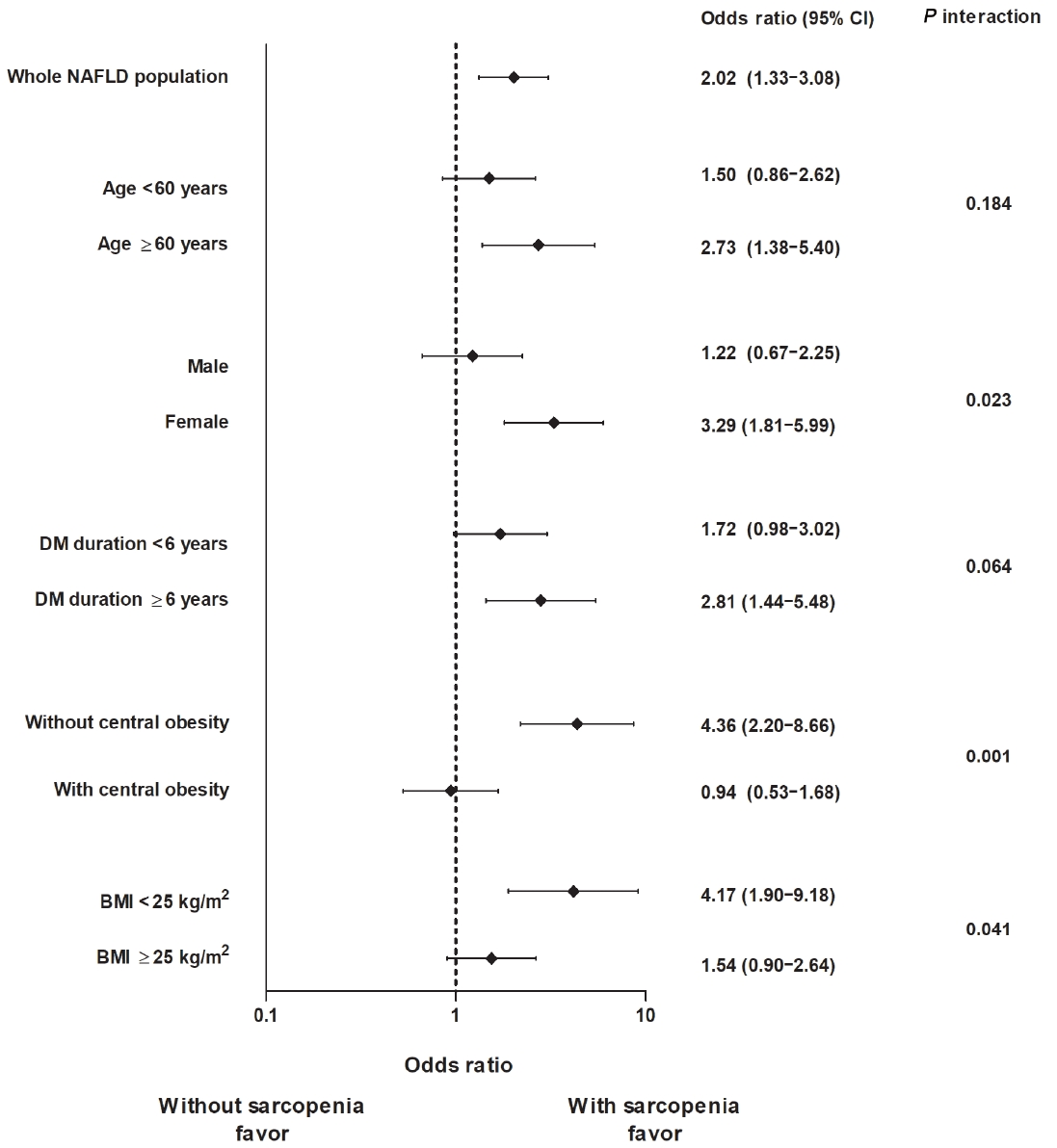
- In the subgroup analysis that included only patients with NAFLD, we further analyzed the relative risk of carotid plaque progression depending on the presence of sarcopenia after dividing the patients into two subgroups by other clinical characteristics, such as age, sex, diabetes duration, presence of central obesity, and BMI. As shown in Fig. 2, patients with sarcopenia had a significantly higher risk of carotid plaque progression in women, non-obese patients (BMI <25 kg/m2), and patients without central obesity (all P interaction <0.05).
RESULTS
- This study included repeated carotid ultrasonography data of 852 T2DM patients for up to 6–8 years and demonstrated sarcopenia as an important risk factor for CVD in T2DM patients with NAFLD. T2DM patients with NAFLD had a higher prevalence of sarcopenia than those without NAFLD. When sarcopenia was accompanied by NAFLD in T2DM patients, the risk of carotid artery plaque progression was higher than when both NAFLD and sarcopenia were not present. In a subgroup analysis that included only patients with NAFLD, patients with sarcopenia who were women, without central obesity, and non-obese showed significant association with a high-risk of carotid plaque progression.
- Previous studies have shown that sarcopenia and NAFLD are closely associated, and that patients with sarcopenia have an increased risk of NAFLD [24-26]. Although the causal relationship between NAFLD and sarcopenia is still unclear, it has been suggested that they share a similar mechanism that facilitates metabolic abnormalities [7]. Skeletal muscle is the primary tissue responsible for peripheral glucose disposal, and loss of muscle mass can lead to high insulin resistance. Insulin resistance subsequently increases adipocyte lipolysis, aggravates lipotoxicity, and accelerates the development of steatohepatitis [27]. In turn, the accumulation of fatty acids within the liver induces hepatic insulin resistance, creating a vicious cycle between insulin resistance and fatty liver. In this study, patients with both NAFLD and sarcopenia had the highest homeostatic model assessment for insulin resistance and lowest KITT, suggesting impaired insulin sensitivity. However, the prevalence of sarcopenia according to the presence of NAFLD in this study was different depending on the definition of sarcopenia. Therefore, the association between sarcopenia and NAFLD may vary according to the adjustment method used to define sarcopenia and cautious interpretation may be needed.
- The measurement of CIMT has been widely used to assess atherosclerosis and to evaluate CVD risk [28,29]. Additionally, there have been some reports that carotid plaque burden assessment can be superior to CIMT for predicting CVD events [30]. The evaluation of carotid plaques may be more clinically useful, especially in studying longitudinal changes in carotid atherosclerosis [31,32]. In this study, we evaluated the prevalence of carotid plaques and their subsequent progression. Patients with both NAFLD and sarcopenia had a significantly higher risk of carotid plaque progression; however, those with NAFLD without sarcopenia did not have any significantly meaningful results compared to the control group without NAFLD or sarcopenia. The underlying mechanism has not been elucidated; however, the chronic inflammation observed with sarcopenia could be a possible explanation. In previous studies, appendicular skeletal muscle mass had an inverse correlation with the high-sensitivity C-reactive protein level, the biomarker for inflammation [33,34]. The reactive oxygen species produced in inflammatory conditions mediates a number of signaling pathways that promote atherogenesis [35]. Additionally, visceral obesity, NAFLD, and atherosclerosis are closely related [36]. In this study, the patients with both NAFLD and sarcopenia had the highest visceral fat area. This could be a major mechanism of NAFLD with sarcopenia leading to carotid atherosclerosis. A number of studies have reported that sarcopenia is related to significant hepatic fibrosis in patients with hepatic steatosis [37,38], and hepatic fibrosis is known to be a more potent risk factor for CVD [39]. We can speculate that patients with sarcopenia are prone to have hepatic fibrosis, which leads to carotid atherosclerosis. In a previous cross-sectional study, the combination of hepatic fibrosis and sarcopenia additively increased the risk of CVD in the NAFLD population [8].
- In patients with NAFLD in this study, those who were female, without central obesity, and were non-obese were likely to have increased carotid artery plaque progression risk, when presented with sarcopenia. Without central obesity, which is the well-known CVD risk factor, the presence of sarcopenia significantly contributed to an increased risk of atherosclerosis progression. Therefore, concurrent measurements of sarcopenia might offer an advantage in predicting high CVD risk in patients with T2DM and NAFLD, particularly in lean women without obesity. Obesity is independently associated with CVD and accelerates atherosclerosis even without other risk factors [40,41], and the role of sarcopenia in carotid plaque progression could be attenuated in these obese patients. In addition, Asians tend to have lower skeletal muscle mass, but have more visceral fat compared with other ethnicities with similar BMIs [42]. Fracanzani et al. [43] reported that nonobese NAFLD is associated with visceral obesity and insulin resistance. Although non-obese patients with NAFLD might not be obese according to BMI cut-offs, they still have metabolic derangements that result in NAFLD, and may even have a more aggressive form of NAFLD with a worse clinical outcome, including mortality [44].
- Our study had several strengths. First, we obtained the long-term follow-up results of carotid ultrasonography in patients with T2DM. Although previous studies also analyzed carotid ultrasonographic results, most of the study designs were crosssectional and, thus, it was difficult to demonstrate a longitudinal association. Second, because this hospital-based cohort study was conducted at a single institution, all the patients were managed and evaluated under the same standardized conditions and practices. As a limitation of the current study, the evaluation of NAFLD or sarcopenia was conducted only at baseline in most subjects. Therefore, the effects of changes in NAFLD status or muscle mass could not be analyzed. In addition, adjustments to other metabolic indicators and several event variables that changed during the study period may not be sufficient. Variables such as the use of anti-platelet agents that were not collected in this database may also affect the final result. Although ultrasonographic examination used in the diagnosis of NAFLD is not a highly accurate method, it can be effectively used in a large population-based cohort. However, it was difficult to determine the relationship with hepatic fibrosis owing to the absence of histological information.
- In conclusion, sarcopenia combined with NAFLD was an independent risk factor for carotid artery plaque progression in patients with T2DM. This increased risk was more prominent and significant in women, without central obesity, and in non-obese patients. Screening for NAFLD and sarcopenia would contribute to the prediction of high-risk groups for CVD in patients with T2DM, even in the absence of obesity.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: Y.C., H.S.P., S.H.K.
Acquisition, analysis, or interpretation of data: Y.C., H.S.P., B.W.H., Y.L., S.H.S., D.H.S., S.H.A., S.H., S.H.K.
Drafting the work or revising: Y.C., H.S.P., S.H.K.
Final approval of the manuscript: Y.C., H.S.P., B.W.H., Y.L., S.H.S., D.H.S., S.H.A., S.H., S.H.K.
-
FUNDING
This work was supported by a research grant from the Inha University.
NOTES
-
Acknowledgements
- None

| Study population | No NAFLD or sarcopenia | Only NAFLD | Only sarcopenia | NAFLD with sarcopenia | P value |
|---|---|---|---|---|---|
| Number | 330 (38.7) | 333 (39.1) | 66 (7.7) | 123 (14.4) | |
| Women | 180 (54.5) | 184 (55.3) | 44 (66.7) | 61 (49.6) | 0.163 |
| Age, yr | 55.0±9.3 | 54.5±8.8 | 59.5±9.5a,b | 56.5±11.1 | 0.001 |
| Body weight, kg | 60.5±9.1 | 67.1±9.9a | 63.5±10.4 | 72.0±14.0a,b,c | <0.001 |
| BMI, kg/m2 | 22.8±2.5 | 25.1±2.5a | 25.2±4.0a | 27.4±3.6a,b,c | <0.001 |
| Waist circumference, cm | 78.2±7.0 | 84.7±7.0a | 82.8±8.8a | 90.2±8.8a,b,c | <0.001 |
| Systolic BP, mm Hg | 130.1±18.1 | 133.6±17.6 | 139.0±18.4a | 138.5±16.7a | <0.001 |
| Diastolic BP, mm Hg | 83.6±11.6 | 86.3±10.2a | 88.3±10.7a | 89.5±11.4a,b | <0.001 |
| History of hypertension | 90/330 (27.3) | 108/333 (32.4) | 23/66 (34.8) | 56/123 (45.5) | 0.003d |
| History of cardio-cerebrovascular disease | 3/330 (0.9) | 5/333 (1.5) | 0/66 (0) | 3/123 (2.4) | 0.452 |
| Smoking, current | 45/290 (15.5) | 56/300 (18.7) | 6/57 (10.5) | 17/108 (15.7) | 0.111 |
| Regular alcohol consumption | 146/296 (49.3) | 149/306 (48.7) | 21/59 (35.6) | 45/105 (42.9) | 0.188 |
| Regular exercise | 182/253 (71.9) | 160/273 (58.6) | 30/47 (63.8) | 54/94 (57.4) | 0.007d |
| Statin use | 51/330 (15.5) | 45/333 (13.5) | 7/66 (10.6) | 12/123 (9.8) | 0.387 |
| Duration of diabetes, yr | 7.4±7.2 | 6.2±5.5 | 6.6±6.8 | 5.4±5.2a | 0.011 |
| HbA1c, % | 8.1±2.2 | 8.3±1.7 | 8.4±2.5 | 8.6±2.1 | 0.117 |
| KITT, %/min | 2.5±1.0 | 1.9±0.8a | 2.3±1.2b | 1.7±0.8a,c | <0.001 |
| HOMA-IR | 2.5±1.4 | 3.4±2.5a | 2.8±1.5 | 3.6±2.9a | <0.001 |
| AST, IU/L | 25.4±13.0 | 29.0±13.0a | 23.5±12.1b | 29.7±14.9a,c | <0.001 |
| ALT, IU/L | 23.6±15.9 | 32.1±17.8a | 23.7±18.6b | 35.7±21.9a,c | <0.001 |
| LDL-C, mg/dL | 109.0±31.8 | 112.4±38.6 | 118.3±38.5 | 124.8±40.7a,b | <0.001 |
| Triglyceride, mg/dL | 110.2±57.5 | 170.2±149.7a | 129.0±60.0b | 160.2±93.3a | <0.001 |
| HDL-C, mg/dL | 54.5±14.9 | 49.9±12.3a | 51.7±10.7 | 49.5±17.7a | <0.001 |
| eGFR-EPI, mL/min/1.73 m2 | 86.2±11.4 | 85.6±12.8 | 80.5±16.0a,b | 84.3±12.2 | 0.008 |
| Visceral fat area, cm2 | 33.6±13.6 | 48.7±15.8a | 48.3±16.2a | 60.6±20.6a,b,c | <0.001 |
Values are presented as number (%), mean±standard deviation, or number/total number (%).
NAFLD, non-alcoholic fatty liver disease; BMI, body mass index; BP, blood pressure; HbA1c, glycosylated hemoglobin; KITT, rate constant for plasma glucose disappearance; HOMA-IR, homeostatic model assessment for insulin resistance; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; eGFR-EPI, estimated glomerular filtration rate-Epidemiology Collaboration creatinine equation.
a P<0.05, vs. group 1, by post hoc analyses (Bonferroni tests),
b P<0.05, vs. group 2, by post hoc analyses (Bonferroni tests),
c P<0.05, vs. group 3, by post hoc analyses (Bonferroni tests),
d Significant chi-square test, P<0.05.
Sarcopeniaweight was defined as skeletal muscle mass index (SMI, %) <2 standard deviations below the gender-specific mean for healthy young adults in the Korean population: SMI (%) <29.0 in men and <22.9 in women was considered as sarcopenia. In sensitivity analysis, sarcopeniaheight was defined as an appendicular skeletal mass/height2 ratio <7.0 in men and <5.7 in women. Model 1: crude model without any adjustment; Model 2=Model 1+age, sex; Model 3=Model 2+body mass index, follow-up duration, smoking, alcohol consumption, history of hypertension, exercise; Model 4=Model 3+estimated glomerular filtration rate, diabetes mellitus duration, glycosylated hemoglobin; Model 5=Model 4+use of statin, low-density lipoprotein cholesterol, triglyceride, high-density lipoprotein cholesterol, history of cardio-cerebrovascular disease (logistic regression analysis).
NAFLD, non-alcoholic fatty liver disease.
- 1. Arulanandan A, Ang B, Bettencourt R, Hooker J, Behling C, Lin GY, et al. Association between quantity of liver fat and cardiovascular risk in patients with nonalcoholic fatty liver disease independent of nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 2015;13:1513-20.ArticlePubMed
- 2. Ekstedt M, Franzen LE, Mathiesen UL, Thorelius L, Holmqvist M, Bodemar G, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006;44:865-73.ArticlePubMed
- 3. Lee YH, Cho Y, Lee BW, Park CY, Lee DH, Cha BS, et al. Nonalcoholic fatty liver disease in diabetes. Part I: epidemiology and diagnosis. Diabetes Metab J 2019;43:31-45.ArticlePubMedPMCPDF
- 4. Day CP. Natural history of NAFLD: remarkably benign in the absence of cirrhosis. Gastroenterology 2005;129:375-8.ArticlePubMed
- 5. Lee HH, Cho Y, Choi YJ, Huh BW, Lee BW, Kang ES, et al. Non-alcoholic steatohepatitis and progression of carotid atherosclerosis in patients with type 2 diabetes: a Korean cohort study. Cardiovasc Diabetol 2020;19:81.ArticlePubMedPMCPDF
- 6. Hong SH, Choi KM. Sarcopenic obesity, insulin resistance, and their implications in cardiovascular and metabolic consequences. Int J Mol Sci 2020;21:494.ArticlePubMedPMC
- 7. Seo DH, Lee YH, Park SW, Choi YJ, Huh BW, Lee E, et al. Sarcopenia is associated with non-alcoholic fatty liver disease in men with type 2 diabetes. Diabetes Metab 2020;46:362-9.ArticlePubMed
- 8. Han E, Lee YH, Kim YD, Kim BK, Park JY, Kim DY, et al. Nonalcoholic fatty liver disease and sarcopenia are independently associated with cardiovascular risk. Am J Gastroenterol 2020;115:584-95.ArticlePubMed
- 9. Kang MK, Park JG. Low skeletal muscle mass is a risk factor for subclinical atherosclerosis in patients with nonalcoholic fatty liver disease. Diagnostics (Basel) 2021;11:854.ArticlePubMedPMC
- 10. Fukuda T, Bouchi R, Takeuchi T, Tsujimoto K, Minami I, Yoshimoto T, et al. Sarcopenic obesity assessed using dual energy X-ray absorptiometry (DXA) can predict cardiovascular disease in patients with type 2 diabetes: a retrospective observational study. Cardiovasc Diabetol 2018;17:55.ArticlePubMedPMCPDF
- 11. Heo JE, Shim JS, Lee H, Kim HC. Association between the thigh muscle and insulin resistance according to body mass index in middle-aged Korean adults. Diabetes Metab J 2020;44:446-57.ArticlePubMedPMCPDF
- 12. Baek JH, Kim H, Kim KY, Jung J. Insulin resistance and the risk of diabetes and dysglycemia in Korean general adult population. Diabetes Metab J 2018;42:296-307.ArticlePubMedPMCPDF
- 13. Kim SK, Choi YJ, Huh BW, Park SW, Lee EJ, Cho YW, et al. Nonalcoholic fatty liver disease is associated with increased carotid intima-media thickness only in type 2 diabetic subjects with insulin resistance. J Clin Endocrinol Metab 2014;99:1879-84.ArticlePubMed
- 14. Choe EY, Lee YH, Choi YJ, Huh BW, Lee BW, Kim SK, et al. Waist-to-calf circumstance ratio is an independent predictor of hepatic steatosis and fibrosis in patients with type 2 diabetes. J Gastroenterol Hepatol 2018;33:1082-91.ArticlePubMedPDF
- 15. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care 2021;44(Suppl 1):S15-33.ArticlePubMedPDF
- 16. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med 2009;150:604-12.ArticlePubMedPMC
- 17. Sharma R, Vikram NK, Misra A. Comparison of short insulin tolerance test with HOMA method for assessment of insulin sensitivity in Asian Indians in north India. Diabetes Res Clin Pract 2008;82:e9. -12.
- 18. World Health Organization. The Asia-Pacific perspective: redefining obesity and its treatment. Sydney: Health Communications Australia; 2000.
- 19. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract 2007;75:72-80.ArticlePubMed
- 20. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc 2002;50:889-96.ArticlePubMed
- 21. Kim KM, Lim S, Choi SH, Kim JH, Shin CS, Park KS, et al. Cardiometabolic implication of sarcopenia: the Korea National Health and Nutrition Examination Study (KNHANES) 2008-2010. IJC Metab Endocr 2014;4:63-9.Article
- 22. Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014;15:95-101.ArticlePubMed
- 23. Qi Y, Fan J, Liu J, Wang W, Wang M, Sun J, et al. Cholesteroloverloaded HDL particles are independently associated with progression of carotid atherosclerosis in a cardiovascular disease-free population: a community-based cohort study. J Am Coll Cardiol 2015;65:355-63.PubMed
- 24. Wijarnpreecha K, Panjawatanan P, Thongprayoon C, Jaruvongvanich V, Ungprasert P. Sarcopenia and risk of nonalcoholic fatty liver disease: a meta-analysis. Saudi J Gastroenterol 2018;24:12-7.ArticlePubMedPMC
- 25. Pan X, Han Y, Zou T, Zhu G, Xu K, Zheng J, et al. Sarcopenia contributes to the progression of nonalcoholic fatty liver disease- related fibrosis: a meta-analysis. Dig Dis 2018;36:427-36.ArticlePubMedPDF
- 26. Yu R, Shi Q, Liu L, Chen L. Relationship of sarcopenia with steatohepatitis and advanced liver fibrosis in non-alcoholic fatty liver disease: a meta-analysis. BMC Gastroenterol 2018;18:51.ArticlePubMedPMCPDF
- 27. Chen Z, Yu R, Xiong Y, Du F, Zhu S. A vicious circle between insulin resistance and inflammation in nonalcoholic fatty liver disease. Lipids Health Dis 2017;16:203.ArticlePubMedPMCPDF
- 28. Sibal L, Agarwal SC, Home PD. Carotid intima-media thickness as a surrogate marker of cardiovascular disease in diabetes. Diabetes Metab Syndr Obes 2011;4:23-34.ArticlePubMedPMC
- 29. Bots ML, Dijk JM, Oren A, Grobbee DE. Carotid intima-media thickness, arterial stiffness and risk of cardiovascular disease: current evidence. J Hypertens 2002;20:2317-25.PubMed
- 30. Wannarong T, Parraga G, Buchanan D, Fenster A, House AA, Hackam DG, et al. Progression of carotid plaque volume predicts cardiovascular events. Stroke 2013;44:1859-65.ArticlePubMed
- 31. Landry A, Spence JD, Fenster A. Measurement of carotid plaque volume by 3-dimensional ultrasound. Stroke 2004;35:864-9.ArticlePubMed
- 32. Ainsworth CD, Blake CC, Tamayo A, Beletsky V, Fenster A, Spence JD. 3D ultrasound measurement of change in carotid plaque volume: a tool for rapid evaluation of new therapies. Stroke 2005;36:1904-9.ArticlePubMed
- 33. Koo BK, Kim D, Joo SK, Kim JH, Chang MS, Kim BG, et al. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J Hepatol 2017;66:123-31.ArticlePubMed
- 34. Beyer I, Mets T, Bautmans I. Chronic low-grade inflammation and age-related sarcopenia. Curr Opin Clin Nutr Metab Care 2012;15:12-22.ArticlePubMed
- 35. Singh U, Jialal I. Oxidative stress and atherosclerosis. Pathophysiology 2006;13:129-42.ArticlePubMed
- 36. Gaggini M, Morelli M, Buzzigoli E, DeFronzo RA, Bugianesi E, Gastaldelli A. Non-alcoholic fatty liver disease (NAFLD) and its connection with insulin resistance, dyslipidemia, atherosclerosis and coronary heart disease. Nutrients 2013;5:1544-60.ArticlePubMedPMC
- 37. Lee YH, Kim SU, Song K, Park JY, Kim DY, Ahn SH, et al. Sarcopenia is associated with significant liver fibrosis independently of obesity and insulin resistance in nonalcoholic fatty liver disease: nationwide surveys (KNHANES 2008-2011). Hepatology 2016;63:776-86.ArticlePubMedPDF
- 38. Petta S, Ciminnisi S, Di Marco V, Cabibi D, Camma C, Licata A, et al. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2017;45:510-8.ArticlePubMedPDF
- 39. Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Nonalcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol 2016;65:589-600.ArticlePubMed
- 40. Lakka TA, Lakka HM, Salonen R, Kaplan GA, Salonen JT. Abdominal obesity is associated with accelerated progression of carotid atherosclerosis in men. Atherosclerosis 2001;154:497-504.ArticlePubMed
- 41. Rexrode KM, Carey VJ, Hennekens CH, Walters EE, Colditz GA, Stampfer MJ, et al. Abdominal adiposity and coronary heart disease in women. JAMA 1998;280:1843-8.ArticlePubMed
- 42. Kojima S, Watanabe N, Numata M, Ogawa T, Matsuzaki S. Increase in the prevalence of fatty liver in Japan over the past 12 years: analysis of clinical background. J Gastroenterol 2003;38:954-61.ArticlePubMedPDF
- 43. Fracanzani AL, Valenti L, Bugianesi E, Vanni E, Grieco A, Miele L, et al. Risk of nonalcoholic steatohepatitis and fibrosis in patients with nonalcoholic fatty liver disease and low visceral adiposity. J Hepatol 2011;54:1244-9.ArticlePubMed
- 44. Zou B, Yeo YH, Nguyen VH, Cheung R, Ingelsson E, Nguyen MH. Prevalence, characteristics and mortality outcomes of obese, nonobese and lean NAFLD in the United States, 1999-2016. J Intern Med 2020;288:139-51.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
- Metabolic-associated fatty liver disease and sarcopenia: A double whammy
Aditya Viswanath, Sherouk Fouda, Cornelius James Fernandez, Joseph M Pappachan
World Journal of Hepatology.2024; 16(2): 152. CrossRef - Association of nonalcoholic fatty liver disease and carotid media‐intima thickness: A systematic review and a meta‐analysis
Manouchehr Khoshbaten, Sepideh H. Maleki, Sara Hadad, Amrit Baral, Ana V. Rocha, Laxmi Poudel, Alireza Abdshah
Health Science Reports.2023;[Epub] CrossRef - Cardiometabolic risk factors in patients with type 2 diabetes and sarcopenia
Yu. G. Samoilova, M. V. Matveeva, E. A. Khoroshunova, D. V. Podchinenova, L. L. Maksimova, G. G. Gorbach, A. B. Trivozhenko, V. A. Avkhimenko
Cardiovascular Therapy and Prevention.2023; 23(1): 3655. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- Related articles
-
- Clinical and Lifestyle Determinants of Continuous Glucose Monitoring Metrics in Insulin-Treated Patients with Type 2 Diabetes Mellitus
- Low Household Income Status and Death from Pneumonia in People with Type 2 Diabetes Mellitus: A Nationwide Study
- Optimal Low-Density Lipoprotein Cholesterol Level for Primary Prevention in Koreans with Type 2 Diabetes Mellitus
- Higher Muscle Mass Protects Women with Gestational Diabetes Mellitus from Progression to Type 2 Diabetes Mellitus
- A Real-World Study of Long-Term Safety and Efficacy of Lobeglitazone in Korean Patients with Type 2 Diabetes Mellitus



