- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 38(2); 2014 > Article
-
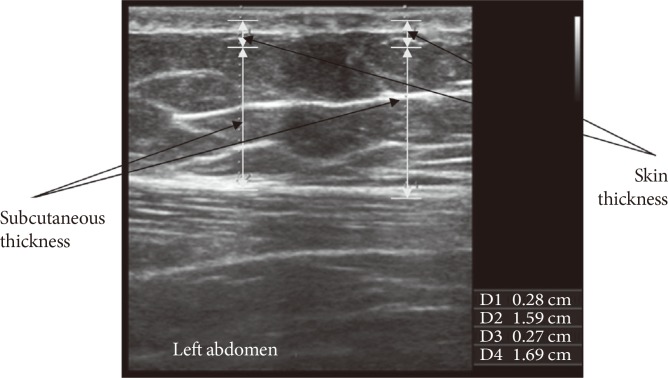
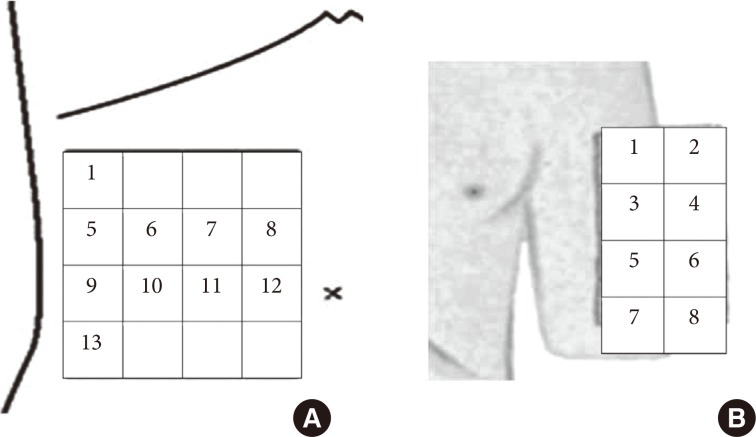
Original ArticleClinical Care/Education The Appropriateness of the Length of Insulin Needles Based on Determination of Skin and Subcutaneous Fat Thickness in the Abdomen and Upper Arm in Patients with Type 2 Diabetes
- Kang Hee Sim1, Moon Sook Hwang2, Sun Young Kim1, Hye Mi Lee1, Ji Yeun Chang3, Moon Kyu Lee4
-
Diabetes & Metabolism Journal 2014;38(2):120-133.
DOI: https://doi.org/10.4093/dmj.2014.38.2.120
Published online: April 18, 2014
1Department of Nursing, Samsung Medical Center, Seoul, Korea.
2Department of Nursing Science, Woo Suk University, Wanju, Korea.
3Department of Internal Medicine, Seoul St. Mary's Hospital, Seoul, Korea.
4Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding author: Moon Sook Hwang. Department of Nursing Science, WooSuk University, 443 Samnye-ro, Wanju-gun 565-701, Korea. msyellow45@hanmail.net
• Received: May 28, 2013 • Accepted: August 26, 2013
Copyright © 2014 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
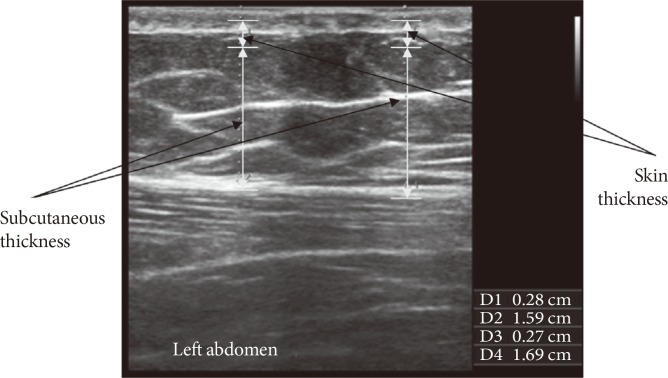
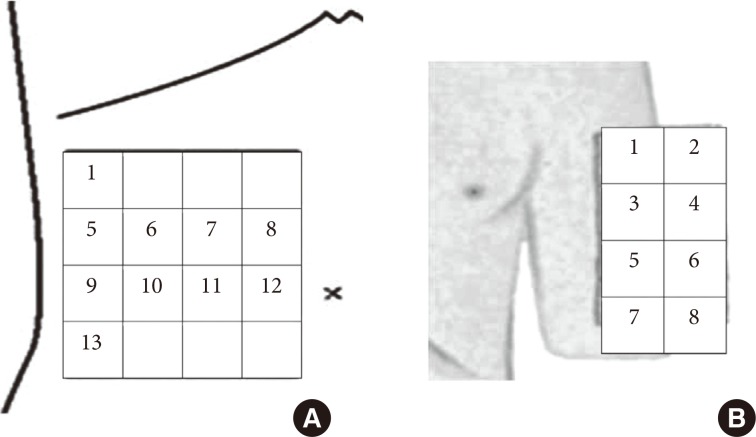

Figure & Data
References
Citations
Citations to this article as recorded by 
- Inadvertent intramuscular injection risk with subcutaneous insulin injections and risk predictors in adults: a cross-sectional sonographic study
U. A. Liyanage, Y. Mathangasinghe, C. K. Liyanage, E. S. Wijewickrama, D. Mahathanthila, A. J. Dharmawansa, S. Jeyerajesingham, D. S. Warapitiya, M. D. M. S. Wijayabandara, B. C. T. A. N. W. M. R. C. S. Kempitiya, A. Aravinthan, L. M. D. T. Jayasekara, N.
International Journal of Diabetes in Developing Countries.2023; 43(5): 731. CrossRef - COVID-19 vaccination and the skin to deltoid muscle distance in adults with diabetes
Marjan Doppen, Ali Mirjalili, Matire Harwood, Allie Eathorne, Irene Braithwaite, Jonathan Bong, Louis Kirton, Ruth Semprini, Mark Weatherall, Alex Semprini, Ciléin Kearns, Melissa Black, Stacey Kung, Michaela Walton, Richard Beasley, Thomas Hills
Vaccine: X.2023; 13: 100248. CrossRef - Integration of capillaric strain sensors toward recognition of human movements
Hudson Gasvoda, Nick Cmager, Rana Altay, Ju Young Lee, I. Emre Araci
Sensors & Diagnostics.2023; 2(1): 212. CrossRef - What variables should inform needle length choice for deltoid intramuscular injection? A systematic review
Ciléin Kearns, Claire Houghton, Emily Dickinson, Lee Hatter, Pepa Bruce, Srinidhi Krishnamoorthy, Mark Weatherall, Thomas Hills, Marjan Doppen, Seyed Ali Mirjalili, Richard Beasley
BMJ Open.2023; 13(1): e063530. CrossRef - Investigation of appropriate needle length considering skin thickness with the real injection posture for insulin injections in diabetic patients
Aya Torii-Goto, Kana Hirai, Yuri Inukai, Yoshimi Hoshina, Kazumi Shiomi, Junko Ito, Masae Yoshikawa
Journal of Pharmaceutical Health Care and Sciences.2023;[Epub] CrossRef - Machine Learning-Based Prediction of Abdominal Subcutaneous Fat Thickness During Pregnancy
Moon Sook Hwang, Eunjeong Song, Jeonghee Ahn, Seungmi Park
Metabolic Syndrome and Related Disorders.2023; 21(9): 479. CrossRef - Human continuous glucose monitors for measurement of glucose in dairy cows
M.K.H. Byrd, A.G. Arneson, D.R. Soffa, J.W. Stewart, M.L. Rhoads
JDS Communications.2022; 3(1): 78. CrossRef - A finite element model of abdominal human tissue for improving the accuracy in insulin absorption assessment: A feasibility study
Pasquale Arpaia, Davide Cuneo, Sabrina Grassini, Francesca Mancino, Simone Minucci, Nicola Moccaldi, Isabella Sannino
Measurement: Sensors.2021; 18: 100218. CrossRef - Abdominal skin subcutaneous fat thickness over the gestational period in Korean pregnant women: a descriptive observational study
Moon Sook Hwang
Korean Journal of Women Health Nursing.2021; 27(4): 318. CrossRef - User experience for manual injection of 2 mL viscous solutions is enhanced by a new prefillable syringe with a staked 8 mm ultra-thin wall needle
Aurélie Pager, Anne Combedazou, Karen Guerrero, Tzvetelina Tzvetkova-Chevolleau, Didier Morel, Cécile Frolet, Stanislav Glezer
Expert Opinion on Drug Delivery.2020; 17(10): 1485. CrossRef - Evaluating the Impact of Human Factors and Pen Needle Design on Insulin Pen Injection
Christopher Rini, Bruce C. Roberts, Didier Morel, Rick Klug, Benjamin Selvage, Ronald J. Pettis
Journal of Diabetes Science and Technology.2019; 13(3): 533. CrossRef - Subcutaneous Injection of Drugs: Literature Review of Factors Influencing Pain Sensation at the Injection Site
Iris Usach, Rafael Martinez, Teodora Festini, José-Esteban Peris
Advances in Therapy.2019; 36(11): 2986. CrossRef - The Injection Technique Factor: What You Don’t Know or Teach Can Make a Difference
Laurence J. Hirsch, Kenneth W. Strauss
Clinical Diabetes.2019; 37(3): 227. CrossRef - Factors associated with removal difficulties of etonogestrel-containing contraceptive implants (Nexplanon ® )
Julien Chevreau, David Krief, Osama Abou Arab, Mickaël Zitoun, Arthur Foulon, Fabrice Sergent, Jean Gondry
European Journal of Obstetrics & Gynecology and Reproductive Biology.2018; 224: 81. CrossRef - Insulin Injection Technique in China Compared with the Rest of the World
Zhenqiang Song, Xiaohui Guo, Linong Ji, Xiao Huang, Laurence J. Hirsch, Kenneth W. Strauss
Diabetes Therapy.2018; 9(6): 2357. CrossRef - Ultrasound-guided measurement of skin and subcutaneous tissue thickness in children with diabetes and recommendations for giving insulin injections
Soo Ting Joyce Lim, Yuen Ching Angela Hui, Pei Kwee Lim, Chin Choo Evelyn Lim, Yen Yen Chia, Rashida Farhad Vasanwala
Journal of Clinical & Translational Endocrinology.2018; 12: 26. CrossRef - Comment on the New Indian Injection Technique Recommendations: Critical Appraisal of the Real-World Implementation of the Current Guidelines
Felice Strollo, Sandro Gentile
Diabetes Therapy.2017; 8(3): 507. CrossRef - Worldwide Injection Technique Questionnaire Study
Anders H. Frid, Laurence J. Hirsch, Astrid R. Menchior, Didier R. Morel, Kenneth W. Strauss
Mayo Clinic Proceedings.2016; 91(9): 1212. CrossRef - Skin and subcutaneous tissue thickness at insulin injection sites in Chinese diabetes patients: Clinical implications
W. Wang, X. Guo, G. Shen, G. Bai, Z. Wei, J. Liu, L. Hirsch, K. Strauss
Diabetes & Metabolism.2016; 42(5): 374. CrossRef - New Insulin Delivery Recommendations
Anders H. Frid, Gillian Kreugel, Giorgio Grassi, Serge Halimi, Debbie Hicks, Laurence J. Hirsch, Mike J. Smith, Regine Wellhoener, Bruce W. Bode, Irl B. Hirsch, Sanjay Kalra, Linong Ji, Kenneth W. Strauss
Mayo Clinic Proceedings.2016; 91(9): 1231. CrossRef - Le tissu sous-cutané et l’insuline : Une cohabitation délicate Revue de la littérature
K. Strauss, S. Halimi
Médecine des Maladies Métaboliques.2015; 9(5): 504. CrossRef - Subcutaneous Injection Depth Does Not Affect the Pharmacokinetics or Glucodynamics of Insulin Lispro in Normal Weight or Healthy Obese Subjects
Amparo de la Peña, Kwee P. Yeo, Helle Linnebjerg, Edward Catton, Shobha Reddy, Patricia Brown-Augsburger, Linda Morrow, Debra A. Ignaut
Journal of Diabetes Science and Technology.2015; 9(4): 824. CrossRef
 PubReader
PubReader Cite
Cite