ABSTRACT
-
Background
- Using real-world data, cardiovascular safety was investigated in metformin users newly starting sodium glucose cotransporter 2 (SGLT2) inhibitors compared with other glucose-lowering drugs in Korea.
-
Methods
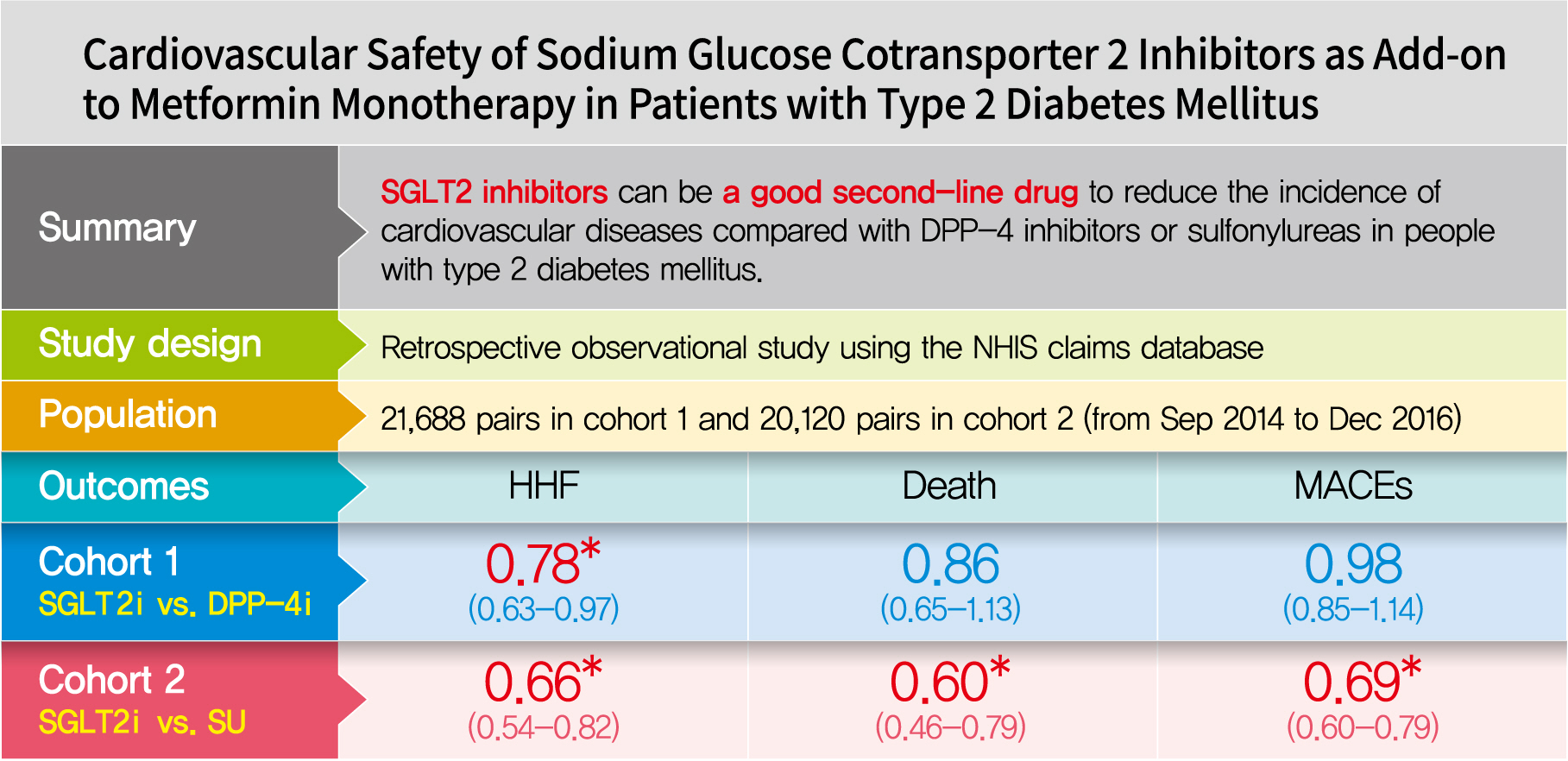
- This was a retrospective observational study using the National Health Insurance Service claims database in Korea. The study period was from September 2014 to December 2016. The study included subjects who were newly prescribed SGLT2 inhibitors or other glucose-lowering drugs while on metformin monotherapy; cohort 1 was composed of new users of SGLT2 inhibitors versus dipeptidyl peptidase-4 (DPP-4) inhibitors and cohort 2 included new users of SGLT2 inhibitors versus sulfonylureas. To balance the patient characteristics, propensity score matching was performed at a 1:1 ratio. Cardiovascular outcomes included hospitalization for heart failure (HHF), all-cause mortality, HHF plus all-cause mortality, myocardial infarction (MI), stroke, and modified major adverse cardiovascular events (MACEs).
-
Results
- After propensity score matching, each cohort group was well balanced at baseline (21,688 pairs in cohort 1 and 20,120 pairs in cohort 2). As the second-line treatment, use of SGLT2 inhibitors was associated with a lower risk of HHF and HHF plus all-cause mortality compared with DPP-4 inhibitors. In addition, use of SGLT2 inhibitors versus sulfonylurea as add-on therapy to metformin was associated with decreased risks of HHF, all-cause mortality, HHF plus all-cause mortality, MI, stroke, and modified MACEs.
-
Conclusion
- SGLT2 inhibitors can be a good second-line drug to reduce the incidence of cardiovascular diseases compared with DPP-4 inhibitors or sulfonylureas in people with type 2 diabetes mellitus.
-
Keywords: Death; Diabetes mellitus; type 2; Heart failure; Myocardial infarction; Retrospective studies; Sodium-glucose transporter 2 inhibitors; Stroke
Graphical abstract
INTRODUCTION
- People with diabetes are at high risk of cardiovascular disease and heart failure [1–3]. Cardiovascular disease is the main cause of death in people with diabetes [4]. The management for preventing or reducing cardiovascular disease has been emphasized in subjects with diabetes [5]. When patients with diabetes received comprehensive management of multiple cardiovascular risk factors, the benefit of lowering glucose to reduce the risk of cardiovascular disease was not clearly proven [6,7]. The issues associated with the use of thiazolidinediones or saxagliptin, including the increased risk of heart failure, have been raised regarding glucose-lowering drug treatment [8,9].
- Sodium glucose cotransporter 2 (SGLT2) inhibitors were recently introduced as a new class of glucose-lowering drugs that reduce glycemia by increasing renal glucose excretion [10]. The cardiovascular outcomes of patients treated with SGLT2 inhibitors (empagliflozin, canagliflozin, and dapagliflozin) have been reported [11–13]. Concordant results regarding cardiovascular death and three major adverse cardiovascular events (MACEs) were not shown in those previous studies. Discrepancies among the three trials were explained by differences in the study populations with established atherosclerotic cardiovascular disease (ASCVD) which was supported by meta-analysis results in subgroups from the three trials [14]. The American Diabetes Association-European Association for the Study of Diabetes consensus report in October 2018 reflected these results and modified the recommendations regarding diabetes medication therapy [15]. SGLT2 inhibitors are preferred for type 2 diabetes mellitus (T2DM) patients with ASCVD if additional medications while on metformin are needed [15]. Even if patients with T2DM have no proven ASCVD, SGLT2 inhibitors are primarily selected for their low hypoglycemic risk and weight loss effects [15]. Although these studies provide useful information regarding the effects of SGLT2 inhibitors on cardiovascular outcomes, several issues require clarification such as the effect on each composite outcome or the results compared with specific drug classes.
- In the present study, cardiovascular outcomes including all-cause mortality in users on metformin monotherapy newly started on SGLT2 inhibitors compared with other glucose-lowering drugs were compared using real-world data in Korea.
METHODS
- Data source
- This observational cohort study was based on the National Health Insurance Service (NHIS; NHIS-2018–1–349) claims database. In Korea, the NHIS is a mandatory national healthcare system that covers the entire population. The NHIS database contains inpatient and outpatient information, demographics, diagnoses (using International Classification of Disease, tenth revision [ICD-10] codes), prescriptions, and procedures. To complement laboratory measurements and health behavior data, the NHIS claims database was merged with nationwide health examinations provided by the NHIS [16]. Subgroup analysis was performed using health examination results.
- The study protocol was approved by the Institutional Review Board of Ajou University Hospital (AJIRB-MED-MDB-15-363) and conformed to the ethical guidelines of the Declaration of Helsinki.
- Study cohort
- The study was conducted from September 2014 (the time when a SGLT2 inhibitor was introduced in Korea) to December 2016. Patients with T2DM ≥18 years of age who were on metformin monotherapy and newly started on a SGLT2 inhibitor (dapagliflozin, empagliflozin, or ipragliflozin), a dipeptidyl peptidase-4 (DPP-4) inhibitor (alogliptin, anagliptin, evogliptin, gemigliptin, linagliptin, saxagliptin, sitagliptin, teneligliptin, or vildagliptin), or a sulfonylurea (glibenclamide, gliclazide, glimepiride, or glipizide) were identified. The individual exposure times are shown in Supplementary Table 1. The index date was defined as the date the patient first started on a SGLT2 inhibitor, DPP-4 inhibitor, or sulfonylurea, with no prescription of the same drug class during the preceding year. When multiple new-user dates were found, the first dispensed drug was chosen. On the index date, patients treated with other glucose-lowering drugs or insulin, excluding metformin and each comparative drug, were excluded. Among those, patients who received metformin monotherapy within 1 year before the index date were further selected. Next, we divided the patients into two cohorts. Cohort 1 consisted of patients on metformin monotherapy who were also started on a SGLT2 inhibitor or DPP-4 inhibitor but did not take a SGLT2 inhibitor or DPP-4 inhibitor during the preceding year. Cohort 2 consisted of patients on metformin monotherapy who were started on a SGLT2 inhibitor or sulfonylurea but did not take a SGLT2 inhibitor or sulfonylurea during the preceding year. Follow-up for the intention-to-treatment analysis was continued until December 2016 or the occurrence of an outcome regardless of whether the indicated drug (cohort 1, SGLT2 inhibitor or DPP-4 inhibitor; cohort 2 SGLT2 inhibitor or sulfonylurea) was continued or not. That for the on-treatment analysis was stopped if the indicated drug was stopped or a comparator drug was started. Metformin could be switched to another glucose-lowering drug or another glucose-lowering drug could be added.
- In Korea, nationwide health examinations are performed biannually for citizens ≥40 years of age. In our study population, health examination data were available for 42% of cohort 1 and 38% of cohort 2 patients within 1 year before the index date. In addition, analysis of the subjects in the two subgroups was performed.
- Baseline variables
- Baseline characteristics including age, sex, index date, comorbidities, frailty, and medication were collected. Frailty was defined as at least one hospital admission ≥3 consecutive days during the preceding year before the index date. Comorbidities were searched based on ICD-10 diagnosis codes from 1 year before the index date to the index date (Supplementary Table 2). Percutaneous coronary intervention was searched using Healthcare Common Procedure Coding System codes provided by the Health Insurance Review and Assessment service regarding the procedure or surgery. Peripheral arterial disease was identified based on the ICD-10 code, procedure, and surgery code. Drug prescriptions were identified based on the Anatomical Therapeutic Chemical code (Supplementary Table 2).
- Study outcomes
- Study outcomes included hospitalization for heart failure (HHF), all-cause mortality, HHF plus all-cause mortality, myocardial infarction (MI), stroke, and modified MACEs. HHF was defined as admission to the hospital with a main diagnosis of heart failure, and modified MACEs were defined as all-cause mortality, MI, and stroke.
- Statistical analyses
- Continuous variables are presented as mean±standard deviation (SD). Categorical variables are presented as numbers and percentages. To balance the baseline characteristics between the groups, propensity score matching with a 1:1 ratio and a nearest neighbor caliper width of 0.25 SD of the propensity score distribution were used for each cohort. Covariates were balanced using standardized differences; a standardized difference >10% was used to indicate a significant group imbalance between baseline variables. The main analysis was performed according to the intention-to-treat (ITT) principle. The results of on-treatment analyses are included as supplementary data. A Cox proportional hazard regression analysis was performed to calculate hazard ratios (HR) and 95% confidence interval (CI) for the occurrence of cardiovascular events and mortality. The cumulative incidences of cardiovascular events and mortality were plotted using the Kaplan-Meier method, and the resulting curves were compared using the log-rank test based on treatment group in each cohort. Subgroup analyses were performed based on the presence of risk factors for the cardiovascular events HHF or HHF plus all-cause mortality. A two-sided P<0.05 was considered significant. All data were analyzed using the SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) and R software packages version 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
- Study cohort and patient characteristics
- During the study period from September 2014 to December 2016, cohort 1 included patients who newly added a SGLT2 inhibitor (n=21,713) or DPP-4 inhibitor (n=104,224) to their metformin monotherapy, and cohort 2 included patients who newly added a SGLT2 inhibitor (n=21,837) or sulfonylurea (n=66,463) to metformin monotherapy (Supplementary Table 3). Before propensity score matching, patients in the SGLT2 inhibitor group were generally younger, predominantly female, and had less frailty. In addition, patients in the SGLT2 inhibitor group received statins or angiotensin receptor blockers more frequently and dihydropyridines less frequently compared with the patients in the DPP-4 inhibitor group or sulfonylurea group. After 1:1 propensity score matching, the baseline characteristics were well balanced between the groups from each cohort with a standardized difference <10% for most of the variables evaluated (Table 1). Two well-matched cohorts of patients who newly added a SGLT2 inhibitor versus DPP-4 inhibitor (21,688 pairs) and a SGLT2 inhibitor versus sulfonylurea (20,120 pairs) to metformin monotherapy were compared. The median follow-up times were 333 and 341 days in the SGLT2 inhibitor and DPP-4 inhibitor groups of cohort 1 after matching, respectively, and 348 and 354 days in the SGLT2 inhibitor and sulfonylurea groups of cohort 2, respectively.
- Risks of cardiovascular outcomes in the SGLT2 inhibitor compared with DPP-4 inhibitor or sulfonylurea groups
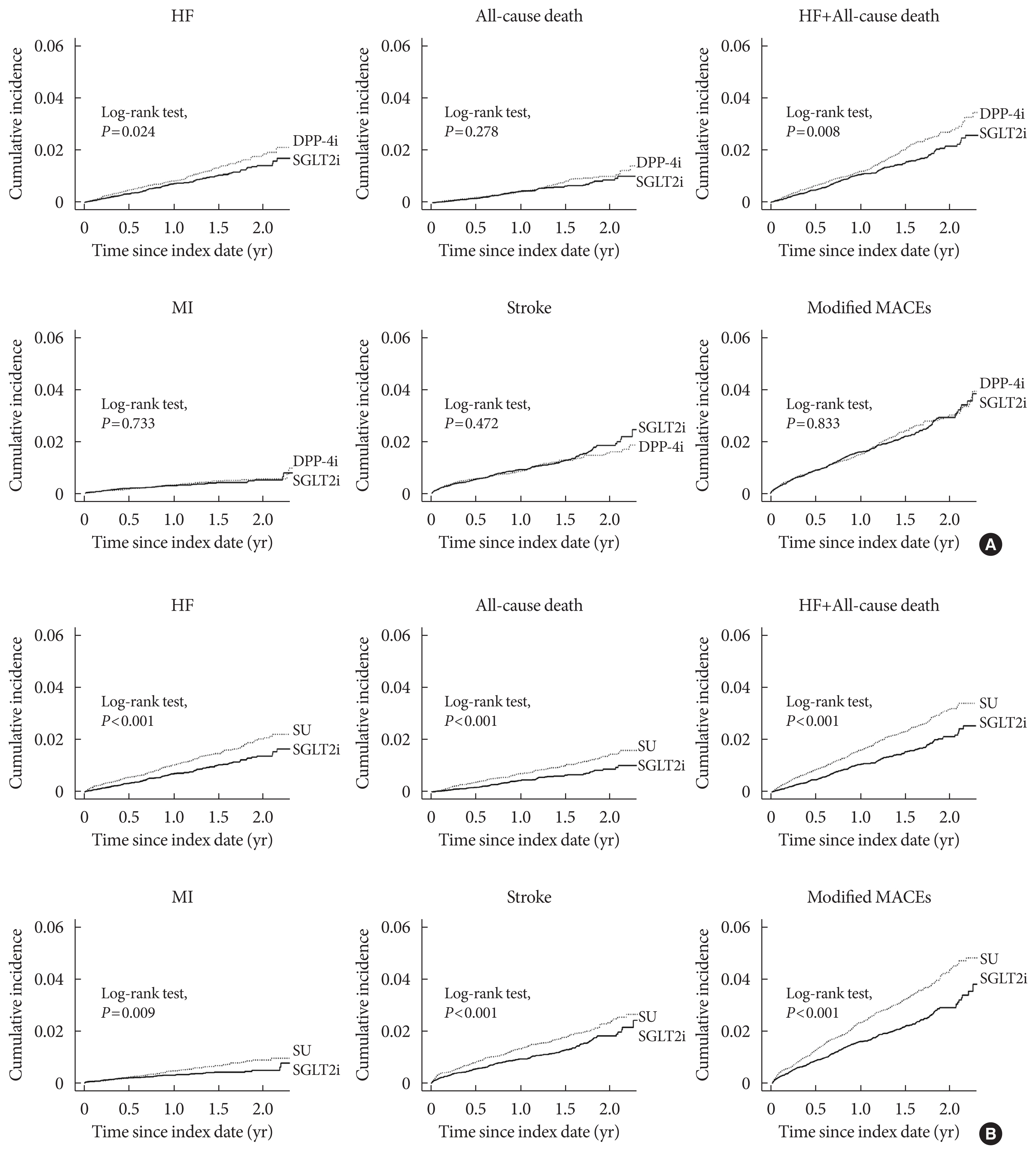
- ITT analysis of the results was performed. On-treatment analyses were generally similar to the ITT analyses (Supplementary Table 4). Patients in the SGLT2 inhibitor group showed lower risks of HHF and HHF plus all-cause mortality compared with patients in the DPP-4 inhibitor group (HR, 0.78; 95% CI, 0.63 to 0.97 and HR, 0.79; 95% CI, 0.66 to 0.94, respectively) (Table 2). Treatment with a SGLT2 inhibitor was associated with lower risks of HHF (HR, 0.66; 95% CI, 0.54 to 0.82), all-cause mortality (HR, 0.60; 95% CI, 0.46 to 0.79), MI (HR, 0.65; 95% CI, 0.55 to 0.77), stroke (HR, 0.74; 95% CI, 0.61 to 0.89), and modified MACEs (HR, 0.69; 95% CI, 0.60 to 0.79) compared with sulfonylurea. Kaplan-Meier curves consistently showed differences in the cumulative incidence of cardiovascular events between the SGLT2 inhibitor group and comparator group from either cohort 1 or 2 (Fig. 1). The cumulative incidences of HHF and HHF plus all-cause mortality were significantly lower in the SGLT2 inhibitor group than in those treated with the DPP-4 inhibitor (log-rank test, P=0.024 and P=0.008, respectively) (Fig. 1A). In addition, the rates of HHF, all-cause mortality, MI, stroke, and modified MACE were significantly lower in the SGLT2 inhibitor group than in those treated with the sulfonylurea (log-rank test, P<0.001, P<0.001, P=0.009, P<0.001, and P<0.001, respectively) (Fig. 1B).
- Sensitivity analysis
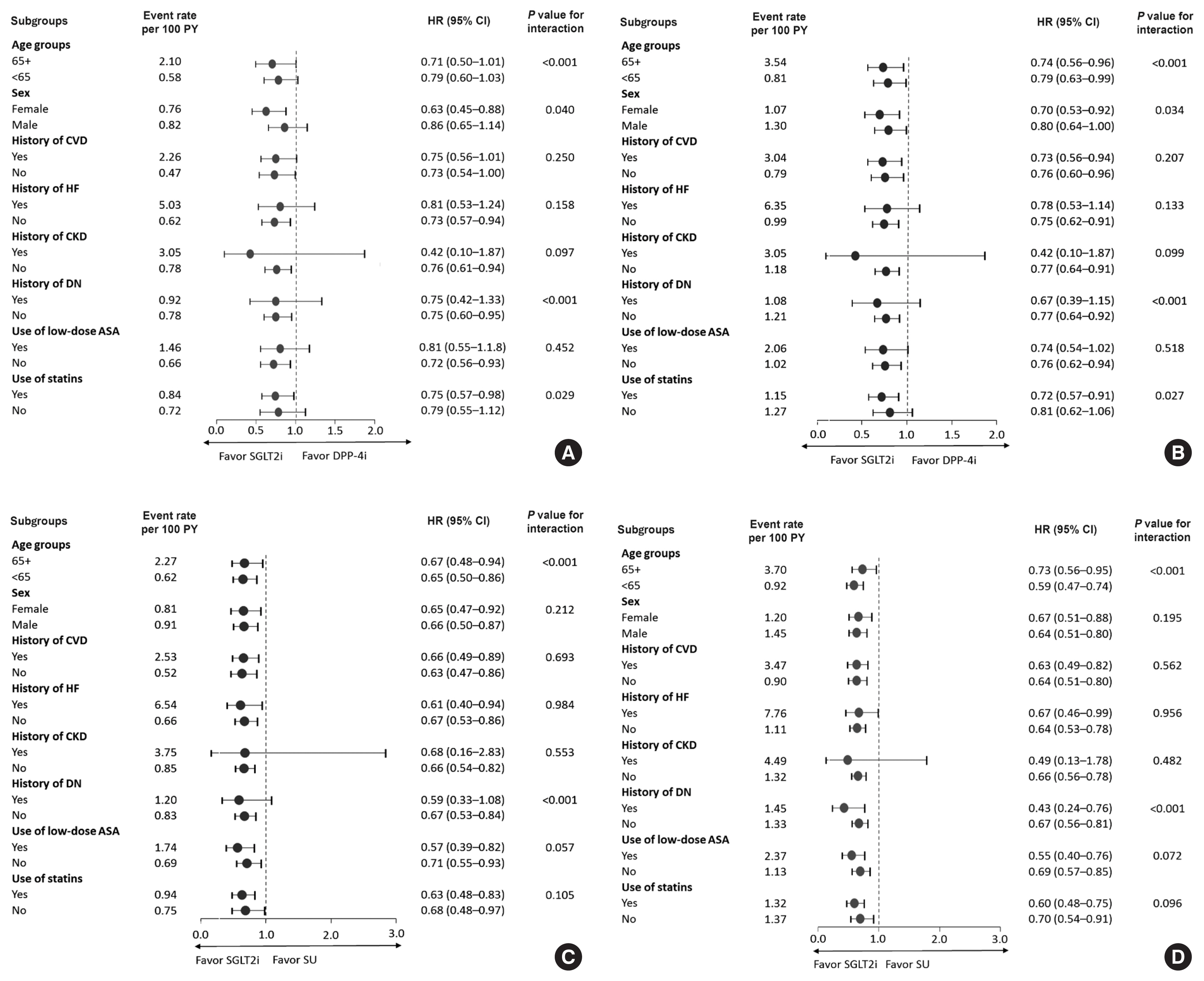
- Subgroup analyses of HHF and HHF plus all-cause mortality were performed based on risk group (Fig. 2). In most subgroups, SGLT2 inhibitors showed more favorable effects on HHF and HHF plus all-cause mortality than did DPP-4 inhibitors or sulfonylureas. In the subgroup with available health screening data (Supplementary Table 5), SGLT2 inhibitors showed significantly lower rates of HHF, HHF plus all-cause mortality, and MI compared with sulfonylureas but not DPP-4 inhibitors (Supplementary Tables 5 and 6).
DISCUSSION
- This was a large observational study in which more than 40,000 drug pairs were analyzed from nationwide data in Korea. SGLT2 inhibitors as a second-line treatment were associated with lower rates of HHF (22% and 34% reduction) and HHF plus all-cause mortality (21% and 35% reduction) compared with DPP-4 inhibitors or sulfonylureas. SGLT2 inhibitors were also associated with beneficial effects on all-cause mortality, MI, stroke, and modified MACEs compared with sulfonylureas only. The favorable effects of SGLT2 inhibitors on HHF were identified when compared 1:1 with each comparator (DPP-4 inhibitor and sulfonylurea) in the present study. This result was supported by the natriuretic effect, a unique action of SGLT2 inhibitors compared with other antidiabetic medications. The beneficial effects of the SGLT2 inhibitors on HHF plus all-cause mortality were from the results obtained for reducing HHF. The preventive effects of SGLT2 inhibitors on HHF appear evident regardless of the comparator medication, type of SGLT2 inhibitor, or patient characteristics [11–13].
- In cardiovascular outcome trials (CVOTs) of SGLT2 inhibitors, different results regarding cardiovascular death and all-cause mortality were observed depending on SGLT2 inhibitors [11–13]. The clinical benefit of reducing the risks of cardiovascular death and all-cause mortality was limited in the empagliflozin trial [11]. A recent meta-analysis of three CVOTs showed that SGLT2 inhibitors reduced the risks of cardiovascular death and all-cause mortality specifically in subjects with established ASCVD [14]. In large observational real-world studies similar to the present study, SGLT2 inhibitors were associated with beneficial effects on all-cause mortality [17–20]. These observational studies were not direct comparisons with specific drug classes and were conducted using a broader and unselected population compared with the present study. In addition, differences in study populations may have existed. The present study population may be at a lower risk of developing cardiovascular events because they were young and might have a relatively shorter duration of diabetes based on the requirement for a second agent while on metformin monotherapy. In the present study, SGLT2 inhibitors were associated with a lower risk of all-cause mortality compared to sulfonylureas but not DPP-4 inhibitors. The current study suggested that SGLT2 inhibitors were associated with reduced all-cause mortality compared to sulfonylurea, even in groups at lower risk for cardiovascular events. In a previous study on a real-world population with fewer subjects with established ASCVD unlike the abovementioned CVOTs, all-cause mortality between individual drug classes was not clarified [21]. Hypoglycemia and weight gain are associated with sulfonylureas and are related to increased mortality. In particular, severe hypoglycemia is strongly associated with higher mortality and cardiovascular disease [22,23]. Moreover, the hemodynamic effects plus the effects of less hypoglycemia and weight reduction by SGLT2 inhibitors may contribute to the low risk of all-cause mortality compared to sulfonylureas [24]. Unfortunately, our study did not explain the pathogenesis linking all-cause mortality and SGLT2 inhibitors compared to sulfonylureas.
- Compared with sulfonylureas (mainly glimepiride), SGLT2 inhibitors were associated with reduced risks of HHF and all-cause mortality as well as other composite cardiovascular outcomes (MI, stroke, and modified MACEs). Some data directly comparing the risks of cardiovascular events between sulfonylureas and other specific drug classes were reported. Sulfonylureas (chlorpropamide and glibenclamide) showed unfavorable effects on all-cause mortality compared with metformin [25]. In the Cardiovascular Outcome Study of Linagliptin vs Glimepiride in Type 2 Diabetes (CAROLINA) study, glimepiride compared with the DPP-4 inhibitor linagliptin was not inferior in terms of MACE occurrence [26].
- In the present study, the subgroup analysis was performed using available health screening data. When comparing the SGLT2 inhibitor with the DPP-4 inhibitor or sulfonylurea, differences in the occurrence of several cardiovascular composite outcomes were not significant. This disparity may be explained by the analysis including <50% of the whole population, and the subjects in this subgroup appeared to be relatively healthy, were at lower risk, and could receive a health screening examination.
- Cardiovascular outcomes and the safety of SGLT2 inhibitors were confirmed in recent CVOTs [11–13]. In several large-scale observational studies, the results of SGLT2 inhibitors were generalized to a broad population of patients with diabetes and increased use regarding clinical applicability [17–20]. The present study complemented the findings of the above studies and provided useful information when choosing a second agent for patients on metformin monotherapy. SGLT2 inhibitors as a second-line treatment were safe and beneficial drugs for the development of most cardiovascular events (HHF, all-cause mortality, and modified MACEs) compared with sulfonylureas and were also safe and preventive drugs in terms of HHF and HHF plus all-cause mortality compared with DPP-4 inhibitors. Considering the progressive course of T2DM [27], treatments requiring a larger number of oral hypoglycemic agents or more insulin serve as a marker for poor glycemic control, diabetic complications, or a high risk for cardiovascular disease [28]. Our study population started treatment with dual combination therapy and may be a lower-risk group for cardiovascular events. Therefore, beneficial effects on cardiovascular composite outcomes of SGLT2 inhibitors might be expected in the general population of patients with diabetes based on the results of the present study and a previous study [18].
- The present study had several limitations. First, due to the observational research design, undetected and residual confounding by indication could have existed despite performing propensity score matching. Second, the claim database used in this study does not include information regarding the duration of diabetes, laboratory findings, or health behavior. Adding a second agent to a metformin monotherapy may have reduced wide variations in the diabetes duration between comparison groups. Health insurance data and available health screening information were merged for subgroup analysis. Due to a decrease in the number of subjects analyzed and lack of incidence rate, several composite outcomes did not show significant differences when comparing sulfonylureas. Third, individual drugs within the same class may show different results, although the focus was on drug class effects and comparisons among medication classes; glimepiride and dapagliflozin in the SGLT2 inhibitor group and the sulfonylurea group mainly contributed to exposure time. Lastly, longer time effects could not be assessed because SGLT2 inhibitors were recently introduced in clinical practice.
- In a direct 1:1 comparison cohort study of drug classes using large real-world data, SGLT2 inhibitors were associated with reduced risks of HHF and HHF plus all-cause mortality compared with DPP-4 inhibitors as a second agent. When added to metformin, SGLT2 inhibitors were also associated with lower risks of HHF and all-cause mortality as well as MI, stroke, and modified MACEs compared to sulfonylureas. SGLT2 inhibitors could be a safe and beneficial medication compared with DPP-4 inhibitors or sulfonylureas as evidenced by recently revised international practice guidelines.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2020.0057.
Supplementary Table 2.
Definitions of drug prescriptions and comorbidities based on ICD-10 codes, procedures, and surgery codes
dmj-2020-0057-suppl2.pdf
Supplementary Table 3.
Demographic data and baseline characteristics before propensity score matching
dmj-2020-0057-suppl3.pdf
Supplementary Table 4.
Hazard ratios for cardiovascular events in the propensity score-matched population
dmj-2020-0057-suppl4.pdf
Supplementary Table 5.
Demographic data and baseline characteristics after propensity score matching in the patient subgroup with available health examination data
dmj-2020-0057-suppl5.pdf
Supplementary Table 6.
Hazard ratios for cardiovascular events in the subgroup with available health examination data after propensity score matching
dmj-2020-0057-suppl6.pdf
NOTES
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: J.Y.J., K.H.H., D.J.K.
Acquisition, analysis, or interpretation of data: J.Y.J., K.H.H., D.J.K.
Drafting the work or revising: J.Y.J., K.H.H., D.J.K.
Final approval of the manuscript: J.Y.J., K.H.H., D.J.K.
-
FUNDING
This work was supported by a grant (Ja Young Jeon, 2016S-5) from the Korean Diabetes Association, a National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (NRF-2020M3A9E8024904), and AstraZenca.
Acknowledgements- This study used NHIS data (NHIS-2018-1-349).
Fig. 1Kaplan-Meier curves for cumulative incidence of cardiovascular outcomes. (A) Sodium glucose cotransporter 2 inhibitor (SGLT2i) versus dipeptidyl peptidase-4 inhibitor (DPP-4i). (B) SGLT2i versus sulfonylurea (SU). HF, heart failure; MACE, major adverse cardiovascular event; MI, myocardial infarction.
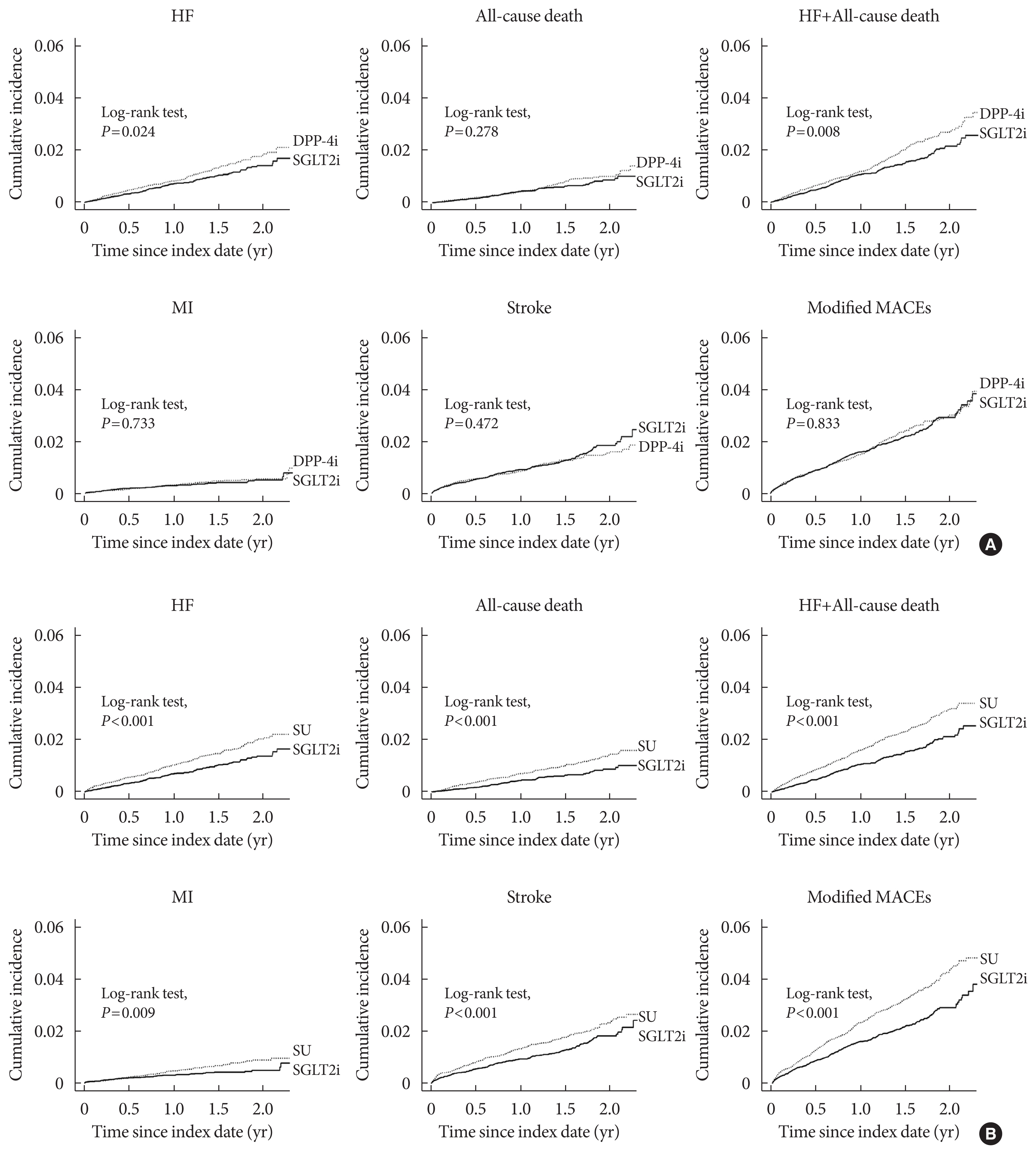
Fig. 2Subgroup analyses for hospitalization for heart failure (HHF) and HHF plus all-cause death. HHF (A) and HHF and all-cause death (B) in comparison of sodium glucose cotransporter 2 inhibitor (SGLT2i) versus dipeptidyl peptidase-4 inhibitor (DPP-4i) and HHF (C) and HHF and all-cause mortality (D) compared between SGLT2i and sulfonylurea (SU). Hazard ratios (HRs) and 95% confidence intervals (CIs) for occurrence of cardiovascular events are presented for SGLT2i vs. DPP-4i or SU. CVD, cardiovascular disease; HF, heart failure; CKD, chronic kidney disease; DN, diabetic nephropathy; ASA, acetyl-salicylic acid.
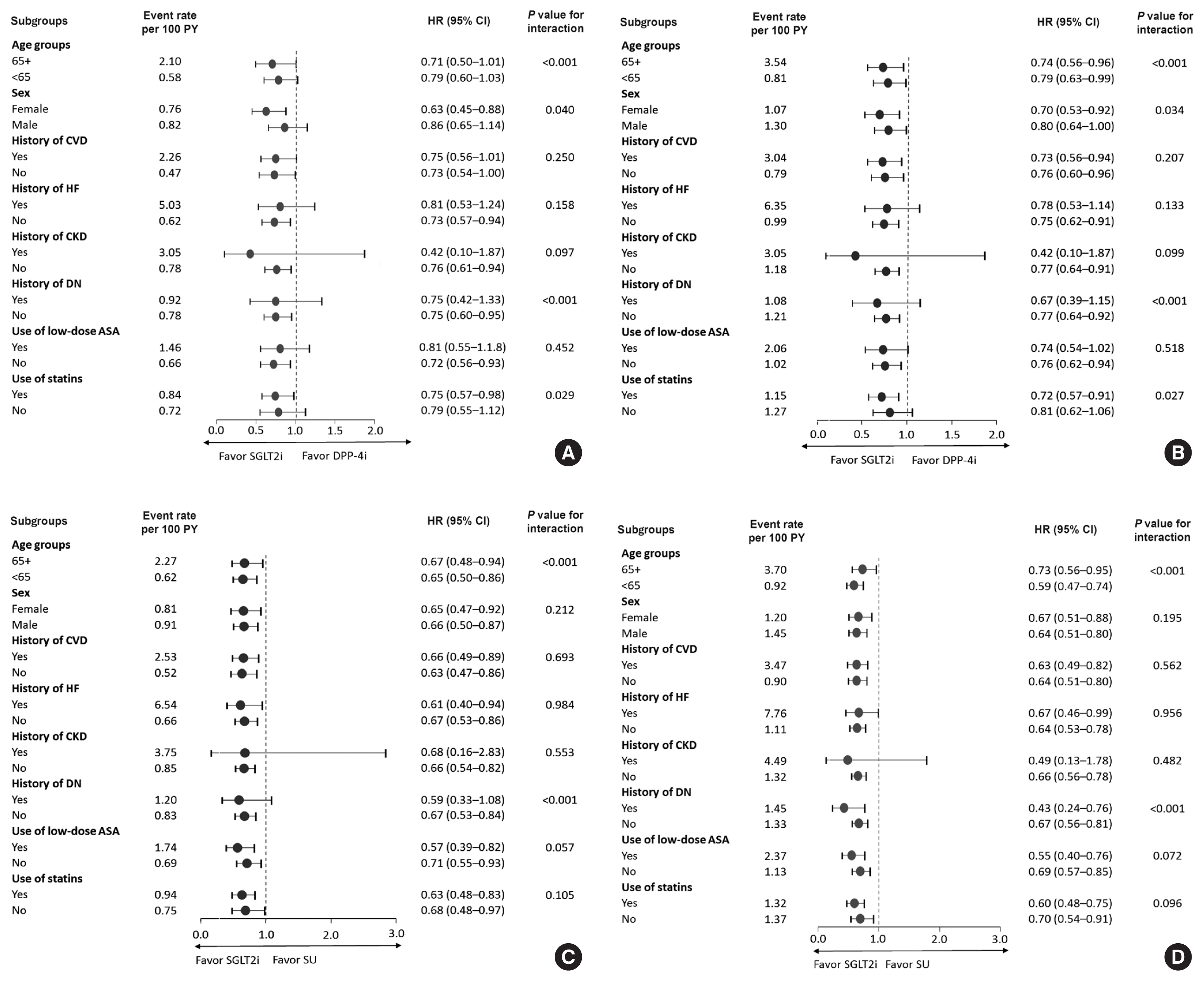
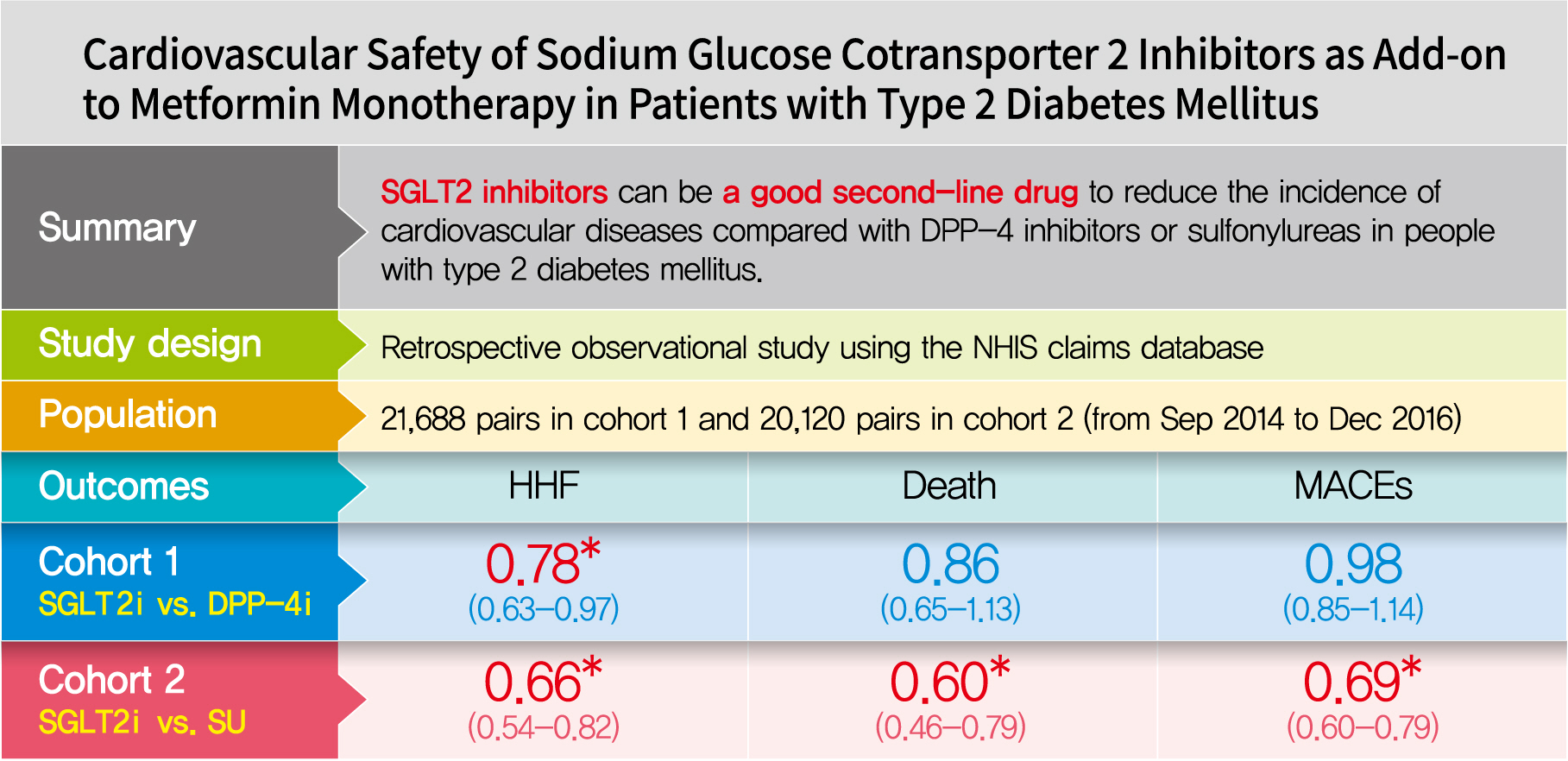
Table 1Demographic data and baseline characteristics after propensity score matching
|
Characteristic |
Cohort 1 |
Cohort 2 |
|
|
|
SGLT2i (n=21,688) |
DPP-4i (n=21,688) |
Standardized difference |
SGLT2i (n=20,120) |
SU (n=20,120) |
Standardized difference |
|
Age, yr |
51.9±11.9 |
51.6±12.2 |
2.1 |
52.6±11.7 |
52.4±12.4 |
1.4 |
|
|
Women |
9,629 (44.4) |
9,684 (44.7) |
0.5 |
8,764 (43.6) |
8,815 (43.8) |
0.5 |
|
|
Index year |
|
2014 |
1,975 (9.1) |
2,054 (9.5) |
1.3 |
1,955 (9.7) |
2,082 (10.3) |
2.1 |
|
2015 |
7,899 (36.4) |
7,888 (36.4) |
0.1 |
7,665 (38.1) |
7,610 (37.8) |
0.6 |
|
2016 |
11,814 (54.5) |
11,746 (54.2) |
0.6 |
10,500 (52.2) |
10,428 (51.8) |
0.7 |
|
|
Comorbidities |
|
Cardiovascular disease |
4,440 (20.5) |
3,991 (18.4) |
5.2 |
3,979 (19.8) |
3,554 (17.7) |
5.4 |
|
Myocardial infarction |
432 (2.0) |
392 (1.8) |
1.4 |
361 (1.8) |
336 (1.7) |
1.0 |
|
PCI with stent |
276 (1.3) |
237 (1.1) |
1.7 |
200 (1.0) |
192 (1.0) |
0.4 |
|
Unstable angina |
658 (3.0) |
576 (2.7) |
2.3 |
574 (2.9) |
547 (2.7) |
0.8 |
|
Angina pectoris |
2,508 (11.6) |
2,350 (10.8) |
2.3 |
2,201 (10.9) |
2,012 (10.0) |
3.1 |
|
Heart failure |
1,032 (4.8) |
929 (4.3) |
2.3 |
864 (4.3) |
817 (4.1) |
1.2 |
|
Atrial fibrillation |
389 (1.8) |
347 (1.6) |
1.5 |
330 (1.6) |
317 (1.6) |
0.5 |
|
Stroke |
1,452 (6.7) |
1,322 (6.1) |
2.5 |
1,355 (6.7) |
1,247 (6.2) |
2.2 |
|
Peripheral artery disease |
13 (0.1) |
17 (0.1) |
0.7 |
12 (0.1) |
15 (0.1) |
0.6 |
|
Chronic kidney disease |
165 (0.8) |
136 (0.6) |
1.6 |
142 (0.7) |
130 (0.6) |
0.7 |
|
Diabetic neuropathy |
1,973 (9.1) |
1,798 (8.3) |
2.9 |
1,801 (9.0) |
1,747 (8.7) |
0.9 |
|
Diabetic retinopahty |
2,884 (13.3) |
2,757 (12.7) |
1.7 |
2,536 (12.6) |
2,443 (12.1) |
1.4 |
|
Diabetic nephropathy |
2,732 (12.6) |
2,622 (12.1) |
1.5 |
2,098 (10.4) |
1,975 (9.8) |
2.0 |
|
Severe hypoglycemia |
241 (1.1) |
213 (1.0) |
1.3 |
228 (1.1) |
217 (1.1) |
0.5 |
|
Keto-/lactate acidosis |
77 (0.4) |
81 (0.4) |
0.3 |
71 (0.4) |
58 (0.3) |
1.1 |
|
Cancer |
1,747 (8.1) |
1,634 (7.5) |
1.9 |
1,587 (7.9) |
1,550 (7.7) |
0.7 |
|
Frailty (yes) |
364 (1.7) |
313 (1.4) |
1.9 |
358 (1.8) |
327 (1.6) |
1.2 |
|
|
Drugs |
|
Low dose acetylic salicylic acid |
3,764 (17.4) |
3,547 (16.4) |
2.7 |
3,495 (17.4) |
3,302 (16.4) |
2.6 |
|
Statin therapy |
13,287 (61.3) |
13,156 (60.7) |
1.2 |
11,822 (58.8) |
11,872 (59.0) |
0.5 |
|
ACE inhibitors |
460 (2.1) |
400 (1.8) |
2.0 |
402 (2.0) |
366 (1.8) |
1.3 |
|
ARB |
9,240 (42.6) |
9,082 (41.9) |
1.5 |
8,349 (41.5) |
8,291 (41.2) |
0.6 |
|
Dihydropyridines |
3,346 (15.4) |
3,134 (14.5) |
2.7 |
3,197 (15.9) |
3,093 (15.4) |
1.4 |
|
Low ceiling diuretics |
1,402 (6.5) |
1,277 (5.9) |
2.4 |
1,316 (6.5) |
1,269 (6.3) |
1.0 |
|
Beta blockers |
3,205 (14.8) |
2,982 (13.7) |
2.9 |
2,834 (14.1) |
2,673 (13.3) |
2.3 |
|
Non-hydropyridines |
477 (2.2) |
433 (2.0) |
1.4 |
404 (2.0) |
390 (1.9) |
0.5 |
|
High ceiling diuretics |
678 (3.1) |
603 (2.8) |
2.0 |
606 (3.0) |
578 (2.9) |
0.8 |
|
Aldosterone antagonists |
328 (1.5) |
274 (1.3) |
2.1 |
282 (1.4) |
260 (1.3) |
0.9 |
|
Warfarin |
126 (0.6) |
114 (0.5) |
0.7 |
115 (0.6) |
109 (0.5) |
0.4 |
|
Receptor P2Y12 antagonists |
1,223 (5.6) |
1,093 (5.0) |
2.7 |
1,075 (5.3) |
1,044 (5.2) |
0.7 |
Table 2Hazard ratios for cardiovascular events in propensity score matched population
|
Variable |
Cohort 1 (n=21,688 pairs) |
Cohort 2 (n=20,120 pairs) |
|
|
|
Event rate |
HR (95% CI) |
Event rate |
HR (95% CI) |
|
|
|
SGLT2i |
DPP-4i |
SGLT2i |
SU |
|
HHF |
0.69 |
0.89 |
0.78 (0.63–0.97) |
0.69 |
1.03 |
0.66 (0.54–0.82) |
|
|
All-cause death |
0.41 |
0.48 |
0.86 (0.65–1.13) |
0.42 |
0.70 |
0.60 (0.46–0.79) |
|
|
HHF+All-cause death |
1.05 |
1.33 |
0.79 (0.66–0.94) |
1.05 |
1.61 |
0.65 (0.55–0.77) |
|
|
Myocardial infarction |
0.29 |
0.31 |
0.94 (0.67–1.33) |
0.29 |
0.44 |
0.65 (0.47–0.90) |
|
|
Stroke |
0.94 |
0.86 |
1.08 (0.88–1.31) |
0.96 |
1.29 |
0.74 (0.61–0.89) |
|
|
Modified MACEs |
1.54 |
1.56 |
0.98 (0.85–1.14) |
1.58 |
2.27 |
0.69 (0.60–0.79) |
REFERENCES
- 1. Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation 1999;100:1134-46.ArticlePubMed
- 2. Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1974;34:29-34.ArticlePubMed
- 3. Ko SH, Han K, Lee YH, Noh J, Park CY, Kim DJ, et al. Past and current status of adult type 2 diabetes mellitus management in Korea: a National Health Insurance Service database analysis. Diabetes Metab J 2018;42:93-100.ArticlePubMedPMCPDF
- 4. International Diabetes Federation. Diabetes and cardiovascular disease report. Brussels: IDF; 2016.
- 5. American Diabetes Association. 10. Cardiovascular disease and risk management: standards of medical care in diabetes. 2019. Diabetes Care 2019;42(Suppl 1):S103-23.ArticlePubMedPDF
- 6. ADVANCE Collaborative Group. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560-72.ArticlePubMed
- 7. Gerstein HC, Riddle MC, Kendall DM, Cohen RM, Goland R, Feinglos MN, et al. Glycemia treatment strategies in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Am J Cardiol 2007;99:34i-43i.ArticlePubMed
- 8. Scirica BM, Braunwald E, Raz I, Cavender MA, Morrow DA, Jarolim P, et al. Heart failure, saxagliptin, and diabetes mellitus: observations from the SAVOR-TIMI 53 randomized trial. Circulation 2014;130:1579-88.ArticlePubMed
- 9. Nassif M, Kosiborod M. Effect of glucose-lowering therapies on heart failure. Nat Rev Cardiol 2018;15:282-91.ArticlePubMedPDF
- 10. Jung CH, Jang JE, Park JY. A novel therapeutic agent for type 2 diabetes mellitus: SGLT2 inhibitor. Diabetes Metab J 2014;38:261-73.ArticlePubMedPMC
- 11. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 12. Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644-57.ArticlePubMed
- 13. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347-57.ArticlePubMed
- 14. Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019;393:31-9.ArticlePubMed
- 15. Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018;41:2669-701.ArticlePubMedPMCPDF
- 16. Lee J, Lee JS, Park SH, Shin SA, Kim K. Cohort profile: the National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int J Epidemiol 2017;46:e15.ArticlePubMed
- 17. Kosiborod M, Lam CSP, Kohsaka S, Kim DJ, Karasik A, Shaw J, et al. Cardiovascular events associated with SGLT-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL 2 study. J Am Coll Cardiol 2018;71:2628-39.PubMed
- 18. Persson F, Nystrom T, Jorgensen ME, Carstensen B, Gulseth HL, Thuresson M, et al. Dapagliflozin is associated with lower risk of cardiovascular events and all-cause mortality in people with type 2 diabetes (CVD-REAL Nordic) when compared with dipeptidyl peptidase-4 inhibitor therapy: a multinational observational study. Diabetes Obes Metab 2018;20:344-51.PubMed
- 19. Birkeland KI, Jorgensen ME, Carstensen B, Persson F, Gulseth HL, Thuresson M, et al. Cardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): a multinational observational analysis. Lancet Diabetes Endocrinol 2017;5:709-17.ArticlePubMed
- 20. Kosiborod M, Cavender MA, Fu AZ, Wilding JP, Khunti K, Holl RW, et al. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL Study (comparative effectiveness of cardiovascular outcomes in new users of sodium-glucose cotransporter-2 inhibitors). Circulation 2017;136:249-59.ArticlePubMedPMC
- 21. Jensen MH, Kjolby M, Hejlesen O, Jakobsen PE, Vestergaard P. Risk of major adverse cardiovascular events, severe hypoglycemia, and all-cause mortality for widely used antihyperglycemic dual and triple therapies for type 2 diabetes management: a cohort study of all Danish users. Diabetes Care 2020;43:1209-18.ArticlePubMedPDF
- 22. Goto A, Arah OA, Goto M, Terauchi Y, Noda M. Severe hypoglycaemia and cardiovascular disease: systematic review and meta-analysis with bias analysis. BMJ 2013;347:f4533.ArticlePubMed
- 23. McCoy RG, Van Houten HK, Ziegenfuss JY, Shah ND, Wermers RA, Smith SA. Increased mortality of patients with diabetes reporting severe hypoglycemia. Diabetes Care 2012;35:1897-901.ArticlePubMedPMCPDF
- 24. Kashiwagi A, Maegawa H. Metabolic and hemodynamic effects of sodium-dependent glucose cotransporter 2 inhibitors on cardio-renal protection in the treatment of patients with type 2 diabetes mellitus. J Diabetes Investig 2017;8:416-27.ArticlePubMedPMCPDF
- 25. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352:854-65.ArticlePubMed
- 26. Rosenstock J, Kahn SE, Johansen OE, Zinman B, Espeland MA, Woerle HJ, et al. Effect of linagliptin vs glimepiride on major adverse cardiovascular outcomes in patients with type 2 diabetes: the CAROLINA randomized clinical trial. JAMA 2019;322:1155-66.ArticlePubMedPMC
- 27. Fonseca VA. Defining and characterizing the progression of type 2 diabetes. Diabetes Care 2009;32(Suppl 2):S151-6.ArticlePubMedPMCPDF
- 28. Gamble JM, Simpson SH, Eurich DT, Majumdar SR, Johnson JA. Insulin use and increased risk of mortality in type 2 diabetes: a cohort study. Diabetes Obes Metab 2010;12:47-53.ArticlePubMed
Citations
Citations to this article as recorded by

- Evaluation and Management of Patients With Diabetes and Heart Failure: A Korean Diabetes Association and Korean Society of Heart Failure Consensus Statement
Kyu-Sun Lee, Junghyun Noh, Seong-Mi Park, Kyung Mook Choi, Seok-Min Kang, Kyu-Chang Won, Hyun-Jai Cho, Min Kyong Moon
International Journal of Heart Failure.2023; 5(1): 1. CrossRef - Evaluation and Management of Patients with Diabetes and Heart Failure: A Korean Diabetes Association and Korean Society of Heart Failure Consensus Statement
Kyu-Sun Lee, Junghyun Noh, Seong-Mi Park, Kyung Mook Choi, Seok-Min Kang, Kyu-Chang Won, Hyun-Jai Cho, Min Kyong Moon
Diabetes & Metabolism Journal.2023; 47(1): 10. CrossRef - Advances in Research on Type 2 Diabetes Mellitus Targets and Therapeutic Agents
Jingqian Su, Yingsheng Luo, Shan Hu, Lu Tang, Songying Ouyang
International Journal of Molecular Sciences.2023; 24(17): 13381. CrossRef - Cardioprotective effects of dipeptidyl peptidase-4 inhibitors versus sulfonylureas in addition to metformin: A nationwide cohort study of patients with type 2 diabetes
Jui Wang, Hon-Yen Wu, Kuo-Liong Chien
Diabetes & Metabolism.2022; 48(3): 101299. CrossRef - Cardiovascular disease in patients with type 2 diabetes
Ja Young Jeon, Dae Jung Kim
Journal of Diabetes Investigation.2022; 13(4): 614. CrossRef - The Impact of Novel Anti-Diabetic Medications on CV Outcomes: A New Therapeutic Horizon for Diabetic and Non-Diabetic Cardiac Patients
Israel Mazin, Fernando Chernomordik, Paul Fefer, Shlomi Matetzky, Roy Beigel
Journal of Clinical Medicine.2022; 11(7): 1904. CrossRef - Effect of Sodium-Glucose Cotransporter Inhibitors on Major Adverse Cardiovascular Events and Hospitalization for Heart Failure in Patients With Type 2 Diabetes Mellitus and Atrial Fibrillation
Chang Hee Kwon, Ye-Jee Kim, Min-Ju Kim, Myung-Jin Cha, Min Soo Cho, Gi-Byoung Nam, Kee-Joon Choi, Jun Kim
The American Journal of Cardiology.2022; 178: 35. CrossRef - Using real-world data for supporting regulatory decision making: Comparison of cardiovascular and safety outcomes of an empagliflozin randomized clinical trial versus real-world data
Ha Young Jang, In-Wha Kim, Jung Mi Oh
Frontiers in Pharmacology.2022;[Epub] CrossRef - Cardiovascular Safety of SGLT2 Inhibitors Compared to DPP4 Inhibitors and Sulfonylureas as the Second-Line of Therapy in T2DM Using Large, Real-World Clinical Data in Korea
Kyuho Kim, Sung Hee Choi
Diabetes & Metabolism Journal.2021; 45(4): 502. CrossRef - The effect of sodium‐glucose transport protein 2 inhibitors on mortality and heart failure in randomized trials versus observational studies
Jesper Krogh, Carsten Hjorthøj, Søren L. Kristensen, Christian Selmer, Steen B. Haugaard
Diabetic Medicine.2021;[Epub] CrossRef - Outcomes of patients with type 2 diabetes treated with SGLT-2 inhibitors versus DPP-4 inhibitors. An Italian real-world study in the context of other observational studies
Enrico Longato, Benedetta Maria Bonora, Barbara Di Camillo, Giovanni Sparacino, Lara Tramontan, Angelo Avogaro, Gian Paolo Fadini
Diabetes Research and Clinical Practice.2021; 179: 109024. CrossRef

 , Kyoung Hwa Ha, Dae Jung Kim
, Kyoung Hwa Ha, Dae Jung Kim
 PubReader
PubReader ePub Link
ePub Link Cite
Cite