
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 36(5); 2012 > Article
-
Original ArticleComplications Correlations between Glucagon Stimulated C-peptide Levels and Microvascular Complications in Type 2 Diabetes Patients
- Hye-Jin Yoon1, Youn-Zoo Cho1, Ji-young Kim1, Byung-Joon Kim1, Keun-Young Park1, Gwan-Pyo Koh2, Dae-Ho Lee2, Dong-Mee Lim1
-
Diabetes & Metabolism Journal 2012;36(5):379-387.
DOI: https://doi.org/10.4093/dmj.2012.36.5.379
Published online: October 18, 2012
1Division of Endocrinology and Metabolism, Konyang University Hospital, Konyang University College of Medicine, Daejeon, Korea.
2Division of Endocrinology and Metabolism, Jeju National University Hospital, Jeju National University College of Medicine, Jeju, Korea.
- Corresponding author: Dong-Mee Lim. Division of Endocrinology and Metabolism, Konyang University Hospital, Konyang University College of Medicine, 158 Gwanjeodong-ro, Seo-gu, Daejeon 302-718, Korea. mdldm@hanmail.net
• Received: September 9, 2011 • Accepted: May 23, 2012
Copyright © 2012 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
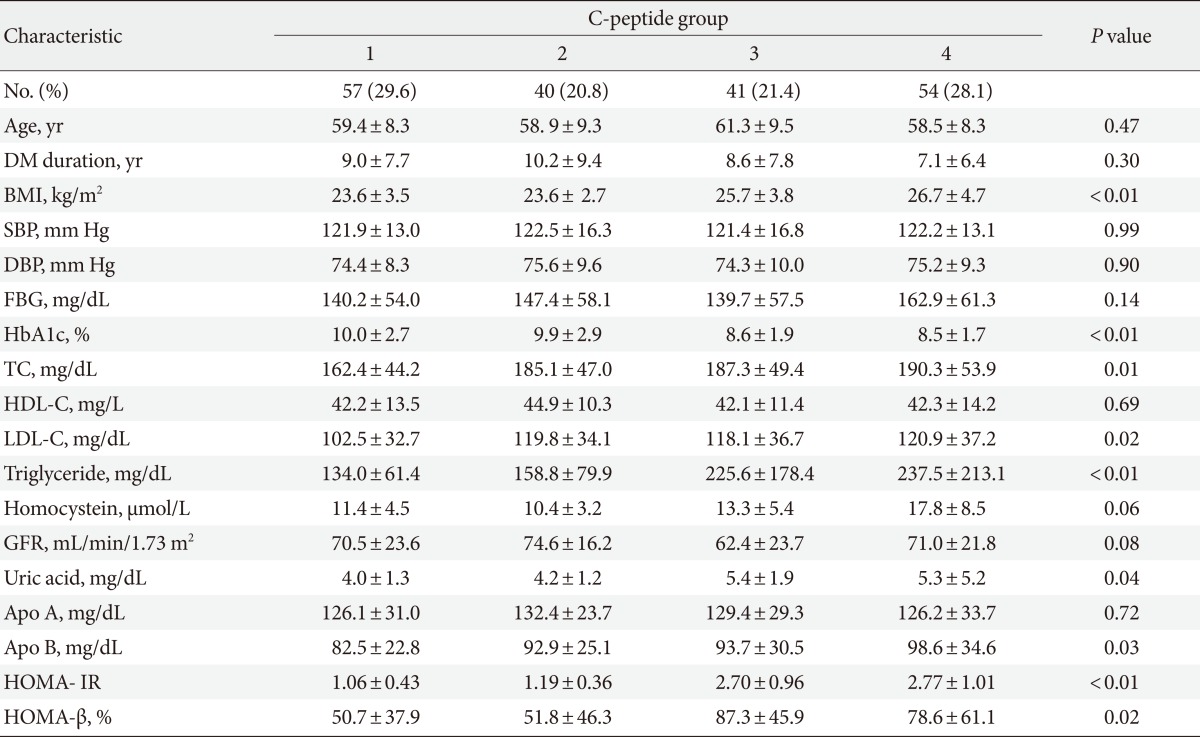
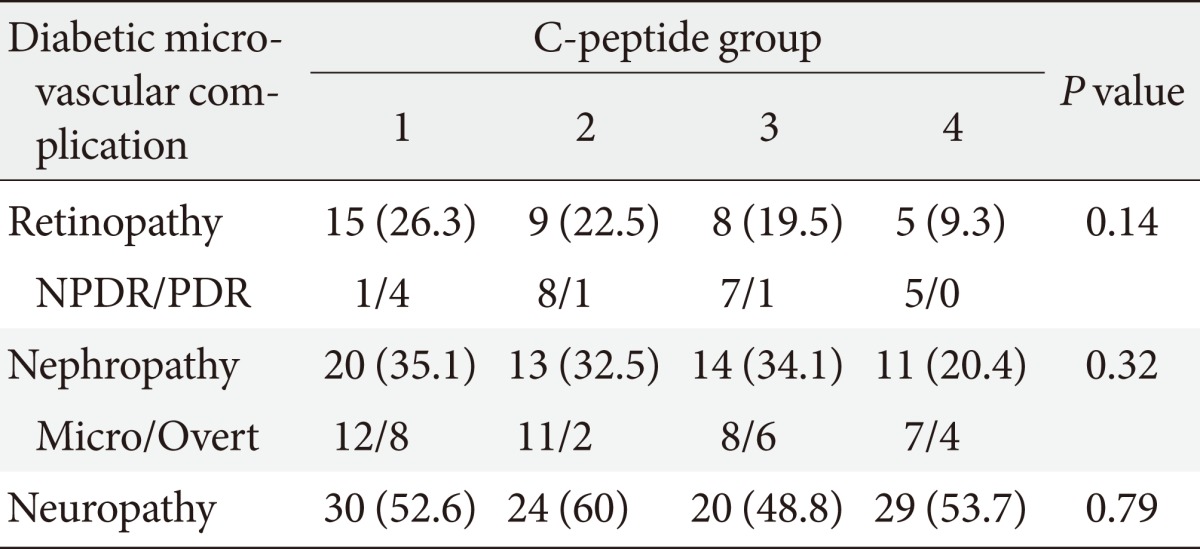

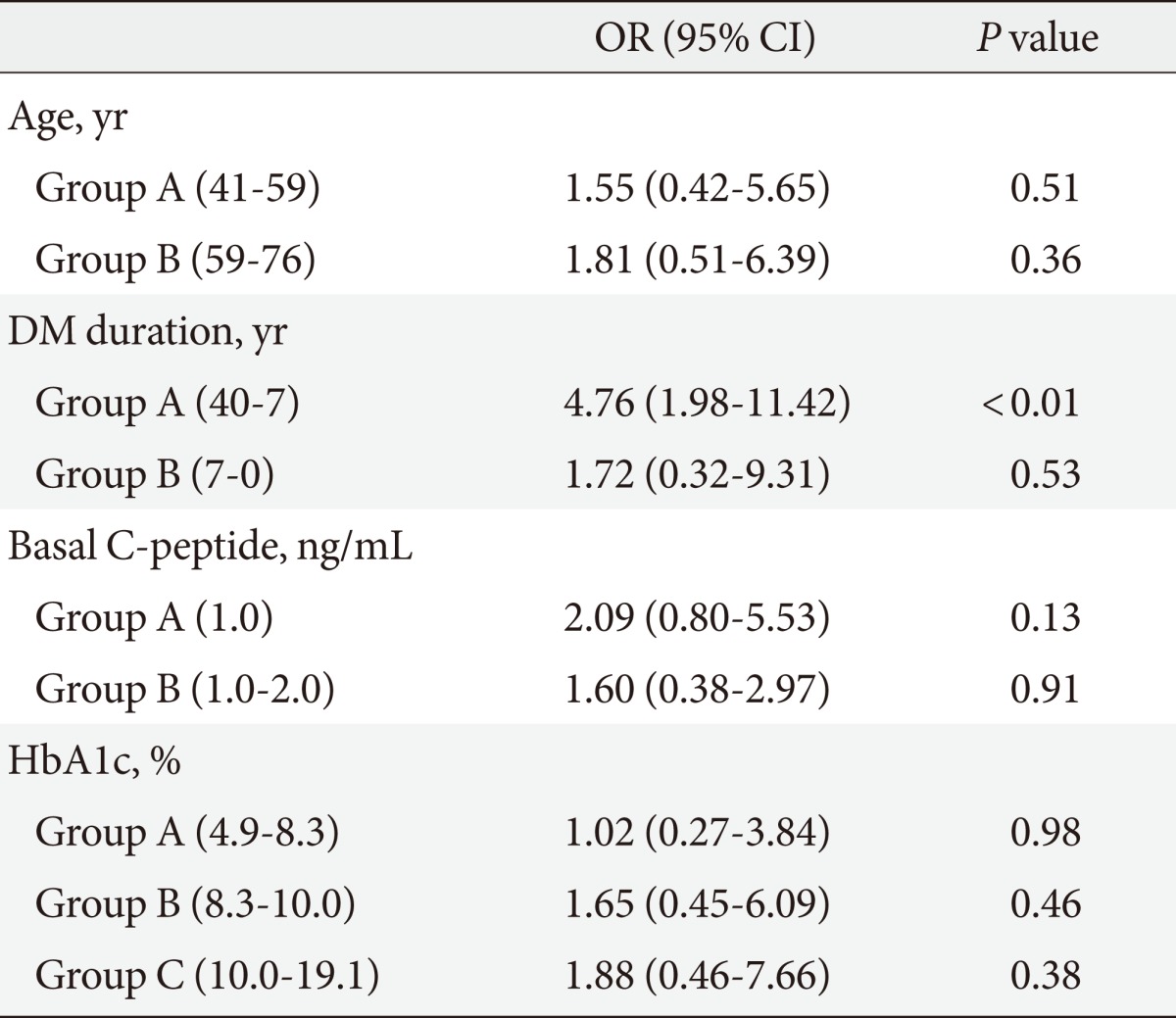
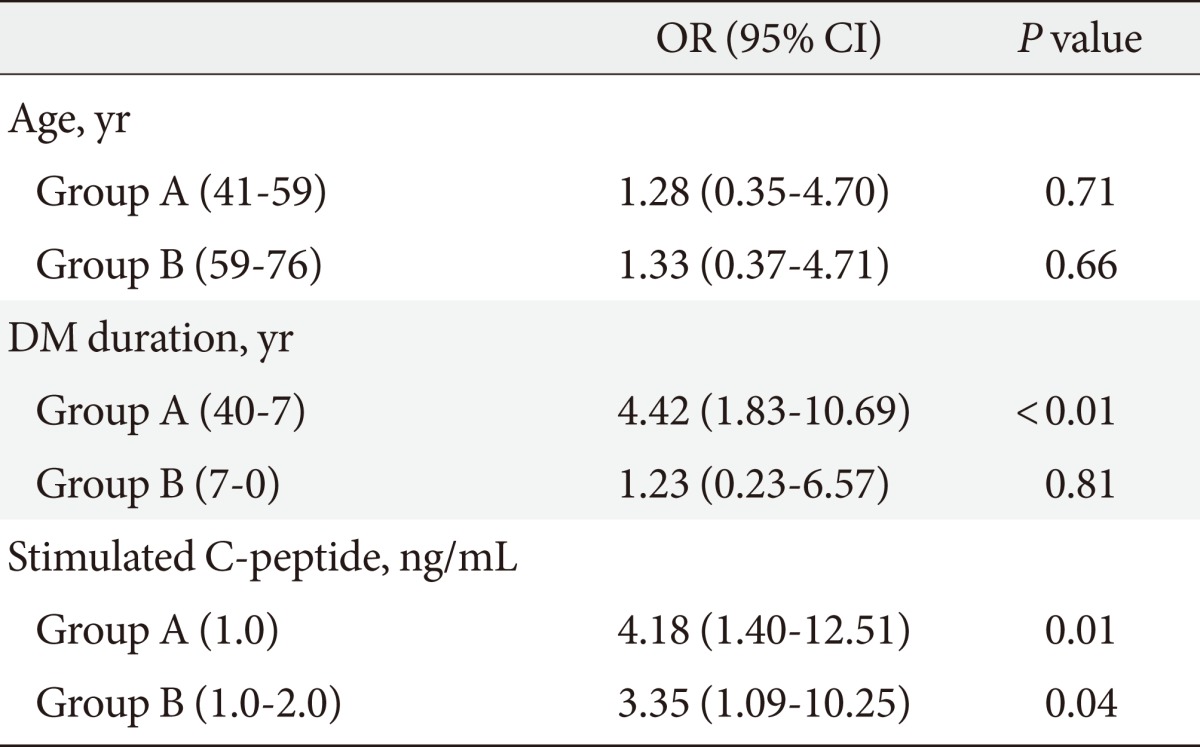
Figure & Data
References
Citations
Citations to this article as recorded by 
- A Nomogram for Predicting Vision-Threatening Diabetic Retinopathy Among Mild Diabetic Retinopathy Patients: A Case–Control and Prospective Study of Type 2 Diabetes
Jing Ke, Kun Li, Bin Cao
Diabetes, Metabolic Syndrome and Obesity.2023; Volume 16: 275. CrossRef - The average 30-minute post-prandial C-peptide predicted diabetic retinopathy progress: a retro-prospective study
Ting Pan, Jie Gao, Xinghua Cai, Huihui Zhang, Jun Lu, Tao Lei
BMC Endocrine Disorders.2023;[Epub] CrossRef - Dysregulation of miR-374a is involved in the progression of diabetic retinopathy and regulates the proliferation and migration of retinal microvascular endothelial cells
Zhanhong Wang, Xiao Zhang, Yanjun Wang, Dailing Xiao
Clinical and Experimental Optometry.2022; 105(3): 287. CrossRef - The Relationship between the Lipid Accumulation Product and Beta-cell Function in Korean Adults with or without Type 2 Diabetes Mellitus: The 2015 Korea National Health and Nutrition Examination Survey
Hye Eun Cho, Seung Bum Yang, Mi Young Gi, Ju Ae Cha, so Young Park, Hyun Yoon
Endocrine Research.2022; 47(2): 80. CrossRef - Effects of Serum C-Peptide Level on Blood Lipid and Cardiovascular and Cerebrovascular Injury in Patients with Type 2 Diabetes Mellitus: A Meta-Analysis
Juan Qin, Rongli Sun, Ding Ding, Yuvaraja Teekaraman
Contrast Media & Molecular Imaging.2022; 2022: 1. CrossRef - Investigation of Diabetes Complication Risk Perception and Diabetes Self-Management Skills in Individuals with Diabetes
Mehmet AYTEMUR, Bahar İNKAYA
Turkish Journal of Diabetes and Obesity.2022; 6(2): 121. CrossRef - Diabetic Retinopathy and Insulin Insufficiency: Beta Cell Replacement as a Strategy to Prevent Blindness
Eli Ipp
Frontiers in Endocrinology.2021;[Epub] CrossRef - Association of C-peptide with diabetic vascular complications in type 2 diabetes
Y. Wang, H. Wan, Y. Chen, F. Xia, W. Zhang, C. Wang, S. Fang, K. Zhang, Q. Li, N. Wang, Y. Lu
Diabetes & Metabolism.2020; 46(1): 33. CrossRef - Variations in glucose/C-peptide ratio in patients with type 2 diabetes associated with renal function
John A. D'Elia, Christopher Mulla, Jiankang Liu, Larry A. Weinrauch
Diabetes Research and Clinical Practice.2019; 150: 1. CrossRef - The pharmacokinetics of porcine C‐peptide after intraperitoneal injection
Naho Iizuka, Masuhiro Nishimura, Yasutaka Fujita, Osamu Sawamoto, Shinichi Matsumoto
Xenotransplantation.2019;[Epub] CrossRef - Association of KCNJ11(RS5219) gene polymorphism with biochemical markers of glycemic status and insulin resistance in gestational diabetes mellitus
Lenin M, Ramesh Ramasamy, Sweta Kulkarani, Seetesh Ghose, Srinivasan A.R.S., Sathish Babu M
Meta Gene.2018; 16: 134. CrossRef - Glucagon secretion is increased in patients with Type 2 diabetic nephropathy
Xiaoyu Wang, Juhong Yang, Baocheng Chang, Chunyan Shan, Yanguang Xu, Miaoyan Zheng, Ying Wang, Huizhu Ren, Liming Chen
Journal of Diabetes and its Complications.2016; 30(3): 488. CrossRef - Relationship between serum C-peptide level and diabetic retinopathy according to estimated glomerular filtration rate in patients with type 2 diabetes
Jin Ook Chung, Dong Hyeok Cho, Dong Jin Chung, Min Young Chung
Journal of Diabetes and its Complications.2015; 29(3): 350. CrossRef - Independent association between serum C‐peptide levels and fat mass‐to‐lean mass ratio in the aging process
Ying Li, Lian Shun Zheng, Yue Li, Duo Duo Zhao, Lu Meng
Geriatrics & Gerontology International.2015; 15(7): 918. CrossRef - Relationship Between β-Cell Function, Metabolic Control, and Microvascular Complications in Type 2 Diabetes Mellitus
Lihua Zhao, Jing Ma, Shaoxin Wang, Yun Xie
Diabetes Technology & Therapeutics.2015; 17(1): 29. CrossRef - Association of fasting insulin and C peptide with diabetic retinopathy in Latinos with type 2 diabetes
Jane Z Kuo, Xiuqing Guo, Ronald Klein, Barbara E Klein, Robert N Weinreb, Pauline Genter, Fone-Ching Hsiao, Mark O Goodarzi, Jerome I Rotter, Yii-Der Ida Chen, Eli Ipp
BMJ Open Diabetes Research & Care.2014; 2(1): e000027. CrossRef - Association between physical activity and serum C‐peptide levels among the elderly
Ying Li, Lu Meng, QianQian Miao, Yasuto Sato
Geriatrics & Gerontology International.2014; 14(3): 647. CrossRef - Age at Diagnosis and C-Peptide Level Are Associated with Diabetic Retinopathy in Chinese
Xiaoling Cai, Xueyao Han, Simin Zhang, Yingying Luo, Yingli Chen, Linong Ji, Alfred S. Lewin
PLoS ONE.2014; 9(3): e91174. CrossRef - Prevalence and risk factors for diabetic retinopathy in Asian Indians with young onset Type 1 and Type 2 Diabetes
Ramachandran Rajalakshmi, Anandakumar Amutha, Harish Ranjani, Mohammed K. Ali, Ranjit Unnikrishnan, Ranjit Mohan Anjana, K.M. Venkat Narayan, Viswanathan Mohan
Journal of Diabetes and its Complications.2014; 28(3): 291. CrossRef - Prediction of response to GLP-1 receptor agonist therapy in Japanese patients with type 2 diabetes
Kenjiro Imai, Tetsuro Tsujimoto, Atsushi Goto, Maki Goto, Miyako Kishimoto, Ritsuko Yamamoto-Honda, Hiroshi Noto, Hiroshi Kajio, Mitsuhiko Noda
Diabetology & Metabolic Syndrome.2014;[Epub] CrossRef - The Association between the Serum C-Peptide Level and Bone Mineral Density
Ying Li, Hua Liu, Yasuto Sato, Bin He
PLoS ONE.2013; 8(12): e83107. CrossRef - C-Peptide and Its Career from Innocent Bystander to Active Player in Diabetic Atherogenesis
Corinna Lebherz, Nikolaus Marx
Current Atherosclerosis Reports.2013;[Epub] CrossRef - C-Peptide and Vascular Complications in Type 2 Diabetic Subjects
Seok Man Son
Diabetes & Metabolism Journal.2012; 36(5): 345. CrossRef
 PubReader
PubReader Cite
Cite- Related articles
-
- Association between Metabolic Syndrome and Microvascular Complications in Chinese Adults with Type 1 Diabetes Mellitus (Diabetes Metab J 2022;46:93-103)
- Association between Metabolic Syndrome and Microvascular Complications in Chinese Adults with Type 1 Diabetes Mellitus (Diabetes Metab J 2022;46:93-103)
- Association between Metabolic Syndrome and Microvascular Complications in Chinese Adults with Type 1 Diabetes Mellitus



