- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 36(2); 2012 > Article
-
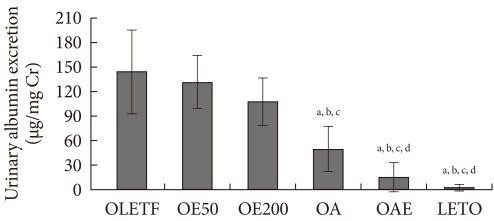
Original ArticleEffect of Eplerenone, a Selective Aldosterone Blocker, on the Development of Diabetic Nephropathy in Type 2 Diabetic Rats
- Jae Hee Ahn, Ho Cheol Hong, Myong Jin Cho, Yoon Jung Kim, Hae Yoon Choi, Chai Ryoung Eun, Sae Jeong Yang, Hye Jin Yoo, Hee Young Kim, Ji A Seo, Sin Gon Kim, Kyung Mook Choi, Sei Hyun Baik, Dong Seop Choi, Nan Hee Kim
-
Diabetes & Metabolism Journal 2012;36(2):128-135.
DOI: https://doi.org/10.4093/dmj.2012.36.2.128
Published online: April 17, 2012
Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- Corresponding author: Nan Hee Kim. Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, 123 Jeokgeum-ro, Danwon-gu, Ansan 425-707, Korea. nhkendo@gmail.com
• Received: July 20, 2011 • Accepted: October 10, 2011
Copyright © 2012 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
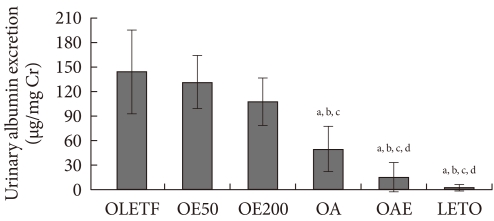
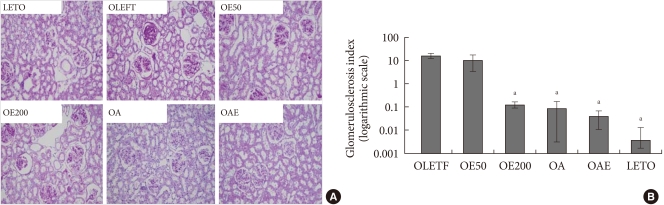
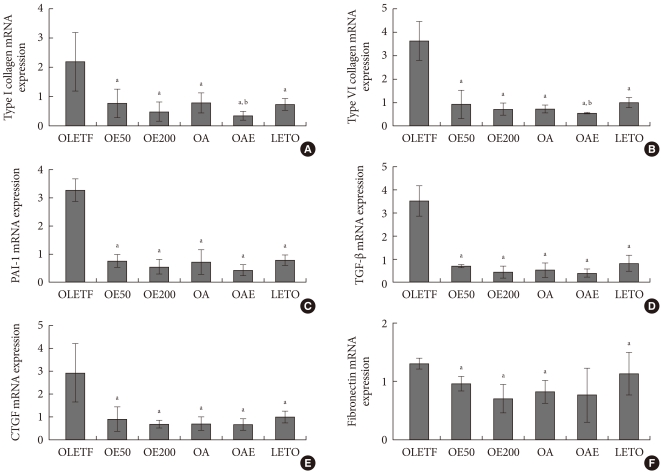
Figure & Data
References
Citations
Citations to this article as recorded by 
- Up-Date on Diabetic Nephropathy
Maria Chiara Pelle, Michele Provenzano, Marco Busutti, Clara Valentina Porcu, Isabella Zaffina, Lucia Stanga, Franco Arturi
Life.2022; 12(8): 1202. CrossRef - The role of free radical oxidation in the kidneys in the nephroprotective action of eplerenone, a mineralocorticoid receptor antagonist, in experimental diabetes mellitus
A. Yu. Zharikov, S. O. Filinova, O. N. Mazko, O. G. Makarova, I. P. Bobrov, V. M. Bryukhanov
Bulletin of Siberian Medicine.2021; 20(2): 29. CrossRef - Effect of Mineralocorticoid Receptor Antagonism and ACE Inhibition on Angiotensin Profiles in Diabetic Kidney Disease: An Exploratory Study
Johannes J. Kovarik, Christopher C. Kaltenecker, Oliver Domenig, Marlies Antlanger, Marko Poglitsch, Chantal Kopecky, Marcus D. Säemann
Diabetes Therapy.2021; 12(9): 2485. CrossRef - Diabetic nephropathy: An update on pathogenesis and drug development
Vikram Rao A/L B Vasanth Rao, Sean Hong Tan, Mayuren Candasamy, Subrat Kumar Bhattamisra
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2019; 13(1): 754. CrossRef - Effects of mineralocorticoid receptor antagonists on the progression of diabetic nephropathy
Li‐Jing Sun, Yan‐Ni Sun, Jian‐Ping Shan, Geng‐Ru Jiang
Journal of Diabetes Investigation.2017; 8(4): 609. CrossRef - New agents modulating the renin-angiotensin-aldosterone system—Will there be a new therapeutic option?
Anna Gromotowicz-Poplawska, Piotr Szoka, Patrycjusz Kolodziejczyk, Karol Kramkowski, Marzena Wojewodzka-Zelezniakowicz, Ewa Chabielska
Experimental Biology and Medicine.2016; 241(17): 1888. CrossRef - Crosstalk between peroxisome proliferator-activated receptor-γ and mineralcorticoid receptor in TNF-α activated renal tubular cell
Jing Xiao, Weijun Chen, Yijun Lu, Xiaoli Zhang, Chensheng Fu, Zhenwen Yan, Zhenxing Zhang, Zhibin Ye
Inflammation Research.2015; 64(8): 603. CrossRef - Eplerenone reduces arterial thrombosis in diabetic rats
Agnieszka Zakrzeska, Anna Gromotowicz-Popławska, Janusz Szemraj, Piotr Szoka, Wioleta Kisiel, Tomasz Purta, Irena Kasacka, Ewa Chabielska
Journal of the Renin-Angiotensin-Aldosterone System.2015; 16(4): 1085. CrossRef - Pharmacological modulation of fibrinolytic response – In vivo and in vitro studies
Karol Kramkowski, Agnieszka Leszczynska, Wlodzimierz Buczko
Pharmacological Reports.2015; 67(4): 695. CrossRef
 PubReader
PubReader Cite
Cite