
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Search
- Page Path
- HOME > Search
- Drug/Regimen
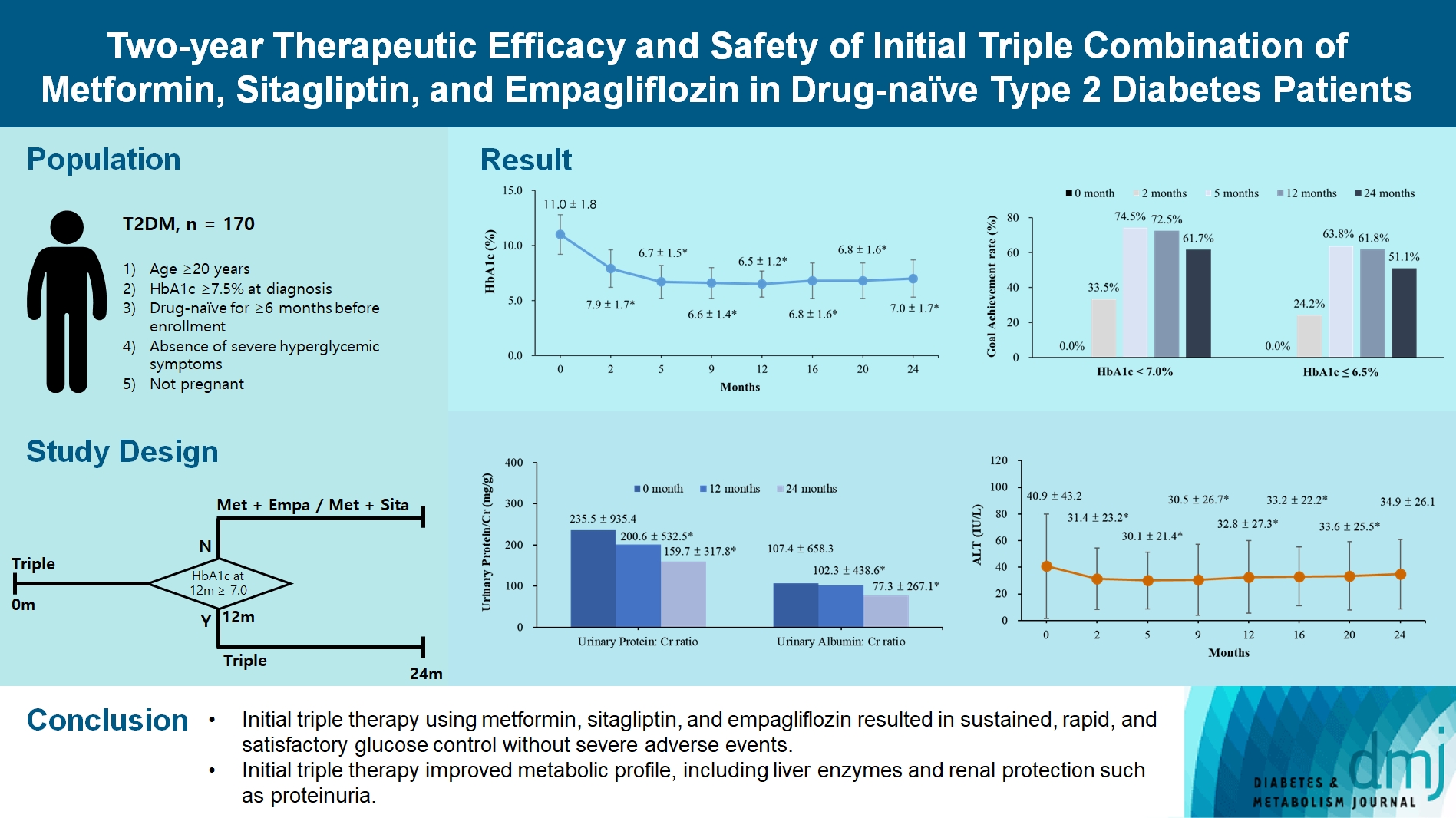
- Two-Year Therapeutic Efficacy and Safety of Initial Triple Combination of Metformin, Sitagliptin, and Empagliflozin in Drug-Naïve Type 2 Diabetes Mellitus Patients
- Young-Hwan Park, Minji Sohn, So Yeon Lee, Soo Lim
- Diabetes Metab J. 2024;48(2):253-264. Published online January 26, 2024
- DOI: https://doi.org/10.4093/dmj.2023.0128
- 1,722 View
- 275 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
We investigated the long-term efficacy and safety of initial triple therapy using metformin, a dipeptidyl peptidase-4 inhibitor, and a sodium-glucose cotransporter-2 inhibitor, in patients with type 2 diabetes mellitus.
Methods
We enrolled 170 drug-naïve patients with glycosylated hemoglobin (HbA1c) level >7.5% who had started triple therapy (metformin, sitagliptin, and empagliflozin). Glycemic, metabolic, and urinary parameters were measured for 24 months.
Results
After 24 months, HbA1c level decreased significantly from 11.0%±1.8% to 7.0%±1.7%. At 12 and 24 months, the rates of achievement of the glycemic target goal (HbA1c <7.0%) were 72.5% and 61.7%, respectively, and homeostasis model assessment of β-cell function and insulin resistance indices improved. Whole-body fat percentage decreased by 1.08%, and whole-body muscle percentage increased by 0.97% after 24 months. Fatty liver indices and albuminuria improved significantly. The concentration of ketone bodies was elevated at the baseline but decreased after 24 months. There were no serious adverse events, including ketoacidosis.
Conclusion
Initial triple combination therapy with metformin, sitagliptin, and empagliflozin led to achievement of the glycemic target goal, which was maintained for 24 months without severe hypoglycemia but with improved metabolic function and albuminuria. This combination therapy may be a good strategy for drug-naïve patients with type 2 diabetes mellitus.
- Drug Regimen
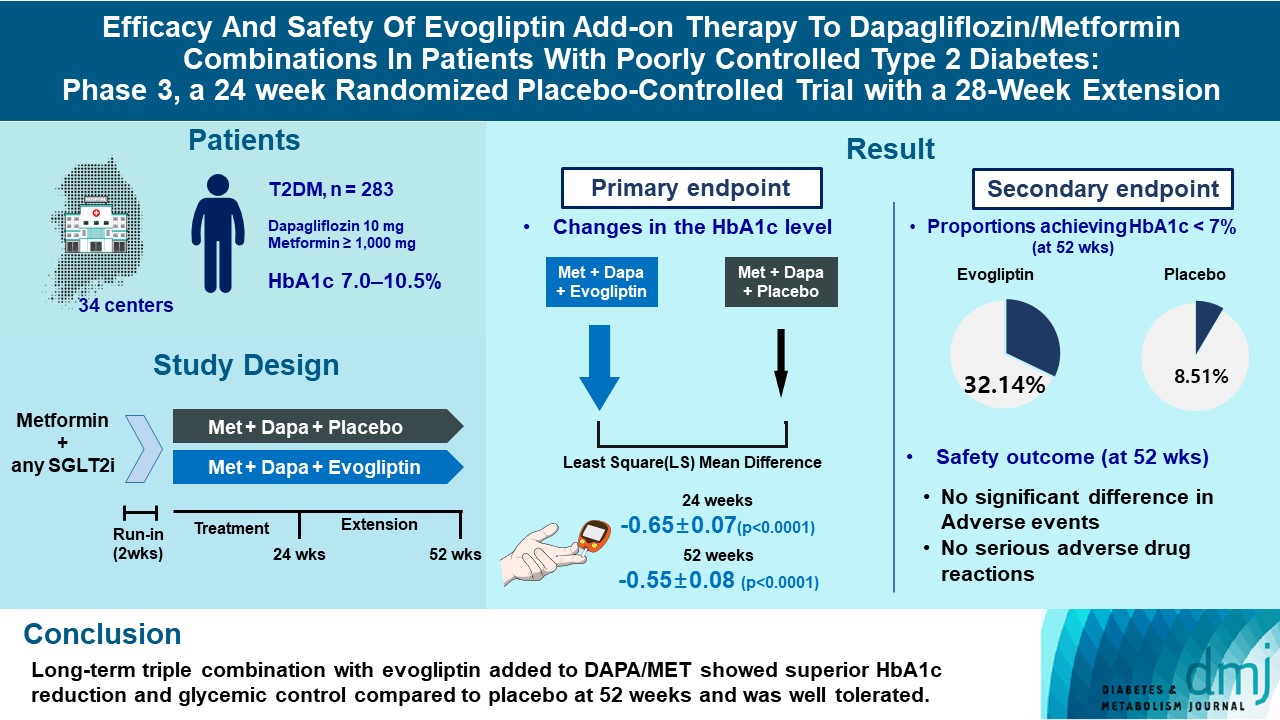
- Efficacy and Safety of Evogliptin Add-on Therapy to Dapagliflozin/Metformin Combinations in Patients with Poorly Controlled Type 2 Diabetes Mellitus: A 24-Week Multicenter Randomized Placebo-Controlled Parallel-Design Phase-3 Trial with a 28-Week Extension
- Jun Sung Moon, Il Rae Park, Hae Jin Kim, Choon Hee Chung, Kyu Chang Won, Kyung Ah Han, Cheol-Young Park, Jong Chul Won, Dong Jun Kim, Gwan Pyo Koh, Eun Sook Kim, Jae Myung Yu, Eun-Gyoung Hong, Chang Beom Lee, Kun-Ho Yoon
- Diabetes Metab J. 2023;47(6):808-817. Published online September 26, 2023
- DOI: https://doi.org/10.4093/dmj.2022.0387
- 2,577 View
- 281 Download
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
This study investigates the long-term efficacy and safety of evogliptin add-on therapy in patients with inadequately controlled type 2 diabetes mellitus (T2DM) previously received dapagliflozin and metformin (DAPA/MET) combination.
Methods
In this multicenter randomized placebo-controlled phase 3 trial, patients with glycosylated hemoglobin (HbA1c) levels 7.0% to 10.5% (n=283) previously used DAPA 10 mg plus MET (≥1,000 mg) were randomly assigned to the evogliptin 5 mg once daily or placebo group (1:1). The primary endpoint was the difference in the HbA1c level from baseline at week 24, and exploratory endpoints included the efficacy and safety of evogliptin over 52 weeks (trial registration: ClinicalTrials.gov NCT04170998).
Results
Evogliptin add-on to DAPA/MET therapy was superior in HbA1c reduction compared to placebo at weeks 24 and 52 (least square [LS] mean difference, –0.65% and –0.55%; 95% confidence interval [CI], –0.79 to –0.51 and –0.71 to –0.39; P<0.0001). The proportion of patients achieving HbA1c <7% was higher in the triple combination group at week 52 (32.14% vs. 8.51% in placebo; odds ratio, 5.62; P<0.0001). Evogliptin significantly reduced the fasting glucose levels and mean daily glucose levels with improvement in homeostatic model assessment of β-cell function (LS mean difference, 9.04; 95% CI, 1.86 to 16.21; P=0.0138). Adverse events were similar between the groups, and no serious adverse drug reactions were reported in the evogliptin group.
Conclusion
Long-term triple combination with evogliptin added to DAPA/MET showed superior HbA1c reduction and glycemic control compared to placebo at 52 weeks and was well tolerated.
- Drug/Regimen
- Increasing Age Associated with Higher Dipeptidyl Peptidase-4 Inhibition Rate Is a Predictive Factor for Efficacy of Dipeptidyl Peptidase-4 Inhibitors
- Sangmo Hong, Chang Hee Jung, Song Han, Cheol-Young Park
- Diabetes Metab J. 2022;46(1):63-70. Published online April 19, 2021
- DOI: https://doi.org/10.4093/dmj.2020.0253

- 65,535 View
- 287 Download
-
 Graphical Abstract
Abstract
PDFSupplementary MaterialPubReader ePub
Graphical Abstract
Abstract
PDFSupplementary MaterialPubReader ePub - Background
It is not known which type 2 diabetes mellitus (T2DM) patients would most benefit from dipeptidyl peptidase-4 (DPP-4) inhibitor treatment. We aimed to investigate the predictors of response to DPP-4 inhibitors considering degree of DPP-4 inhibition.
Methods
This study is a post hoc analysis of a 24-week, randomized, double-blind, phase III trial that compared the efficacy and safety of a DPP-4 inhibitor (gemigliptin vs. sitagliptin) in patients with T2DM. Subjects were classified into tertiles of T1 <65.26%, T2=65.26%–76.35%, and T3 ≥76.35% by DPP-4 inhibition. We analyzed the change from baseline in glycosylated hemoglobin (HbA1c) according to DPP-4 inhibition with multiple linear regression adjusting for age, ethnicity, body mass index, baseline HbA1c, and DPP-4 activity at baseline.
Results
The mean age was greater in the high tertile group compared with the low tertile group (T1: 49.8±8.3 vs. T2: 53.1±10.5 vs. T3: 55.3±9.5, P<0.001) of DPP-4 inhibition. Although HbA1c at baseline was not different among tertiles of DPP-4 inhibition (P=0.398), HbA1c after 24-week treatment was lower in the higher tertile compares to the lower tertile (T1: 7.30%±0.88% vs. T2: 7.12%±0.78% vs. T3: 7.00%±0.78%, P=0.021). In multiple regression analysis, DPP-4 enzyme inhibition rate was not a significant determent for HbA1c reduction due to age. In subgroup analysis by tertile of DPP-4 inhibition, age was the only significant predictor and only in the highest tertile (R2=0.281, B=–0.014, P=0.024).
Conclusion
This study showed that HbA1c reduction by DPP-4 inhibitor was associated with increasing age, and this association was linked with higher DPP-4 inhibition.
- Drug/Regimen
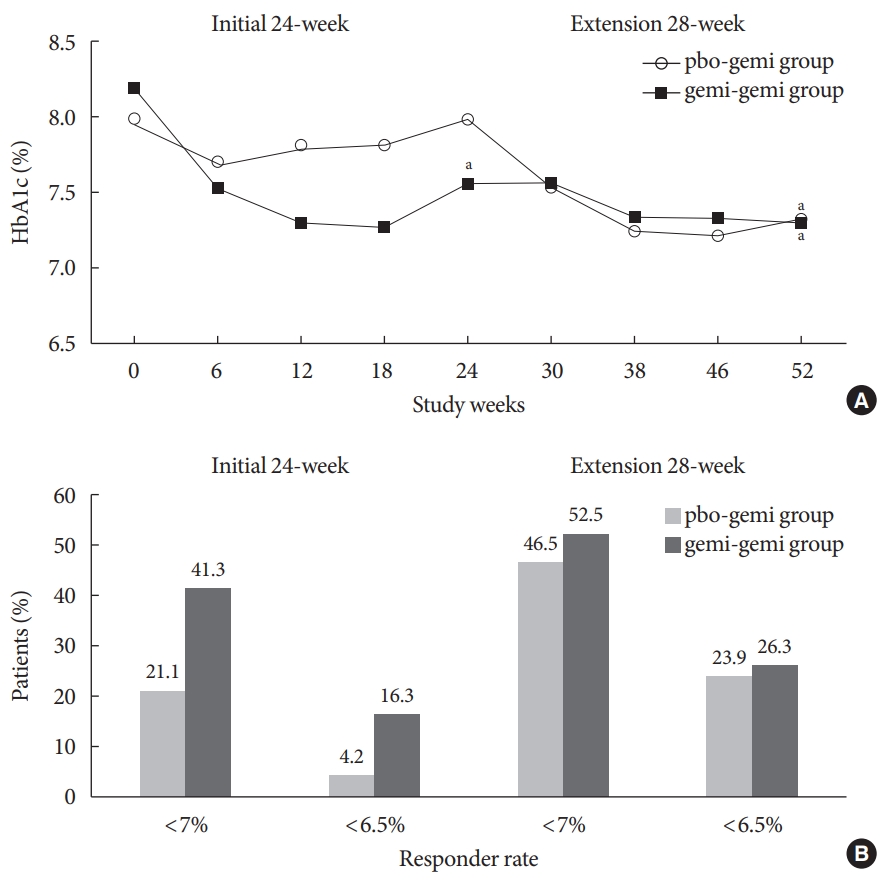
- A Multicentre, Multinational, Open-Label, 52-Week Extension Study of Gemigliptin (LC15-0444) Monotherapy in Patients with Type 2 Diabetes Mellitus
- Sae Jeong Yang, Kyung Wan Min, Sandeep Kumar Gupta, Joong Yeol Park, Vyankatesh K.Shivane, Pankaj Kumar Agarwal, Doo Man Kim, Yong Seung Kim, Sei Hyun Baik
- Diabetes Metab J. 2021;45(4):606-612. Published online September 9, 2020
- DOI: https://doi.org/10.4093/dmj.2020.0047
- 5,034 View
- 139 Download
- 1 Crossref
-
Abstract
PDFPubReader ePub
- The purpose of this extension study was to assess the long-term efficacy and safety of gemigliptin 50 mg in patients with type 2 diabetes mellitus (T2DM). Patients with T2DM who had completed the initial 24-week study comparing gemigliptin monotherapy with placebo were eligible to enrol. In the open-label, 28-week extension study, all enrolled patients received gemigliptin, regardless of the treatment received during the initial 24-week study period. The mean reduction±standard deviation (SD) in glycosylated hemoglobin (HbA1c) observed after 24 weeks of treatment (–0.6%±1.1%) was further decreased for the gemi-gemi group and the mean change in HbA1c at week 52 from baseline was –0.9%±1.2% (P<0.0001). For the pbo-gemi group, HbA1c decreased after they were switched to gemigliptin, and the mean change in HbA1c at week 52 from baseline was –0.7%±1.2% (P<0.0001). Furthermore, the overall incidence of adverse events demonstrated that gemigliptin was safe and well tolerated up to 52 weeks.
-
Citations
Citations to this article as recorded by
- Efficacy and safety of enavogliflozin versus dapagliflozin added to metformin plus gemigliptin treatment in patients with type 2 diabetes: A double-blind, randomized, comparator-active study: ENHANCE-D study
Kyung-Soo Kim, Kyung Ah Han, Tae Nyun Kim, Cheol-Young Park, Jung Hwan Park, Sang Yong Kim, Yong Hyun Kim, Kee Ho Song, Eun Seok Kang, Chul Sik Kim, Gwanpyo Koh, Jun Goo Kang, Mi Kyung Kim, Ji Min Han, Nan Hee Kim, Ji Oh Mok, Jae Hyuk Lee, Soo Lim, Sang S
Diabetes & Metabolism.2023; 49(4): 101440. CrossRef
- Efficacy and safety of enavogliflozin versus dapagliflozin added to metformin plus gemigliptin treatment in patients with type 2 diabetes: A double-blind, randomized, comparator-active study: ENHANCE-D study
- Drug/Regimen
- Evogliptin, a Dipeptidyl Peptidase-4 Inhibitor, Attenuates Renal Fibrosis Caused by Unilateral Ureteral Obstruction in Mice
- Mi-Jin Kim, Na-young Kim, Yun-A Jung, Seunghyeong Lee, Gwon-Soo Jung, Jung-Guk Kim, In-Kyu Lee, Sungwoo Lee, Yeon-Kyung Choi, Keun-Gyu Park
- Diabetes Metab J. 2020;44(1):186-192. Published online October 31, 2019
- DOI: https://doi.org/10.4093/dmj.2018.0271
- 5,662 View
- 97 Download
- 10 Web of Science
- 10 Crossref
-
Abstract
PDFSupplementary MaterialPubReader
Renal fibrosis is considered to be the final common outcome of chronic kidney disease. Dipeptidyl peptidase-4 (DPP-4) inhibitors have demonstrated protective effects against diabetic kidney disease. However, the anti-fibrotic effect of evogliptin, a DPP-4 inhibitor, has not been studied. Here, we report the beneficial effects of evogliptin on unilateral ureteral obstruction (UUO)-induced renal fibrosis in mice. Evogliptin attenuated UUO-induced renal atrophy and tubulointerstitial fibrosis. Immunohistochemistry and Western blotting demonstrated that evogliptin treatment inhibits pro-fibrotic gene expressions and extracellular matrix production.
In vitro findings showed that the beneficial effects of evogliptin on renal fibrosis are mediated by inhibition of the transforming growth factor-β/Smad3 signaling pathway. The present study demonstrates that evogliptin is protective against UUO-induced renal fibrosis, suggesting that its clinical applications could extend to the treatment of kidney disease of non-diabetic origin.-
Citations
Citations to this article as recorded by- Targeting cluster of differentiation 26 / dipeptidyl peptidase 4 (CD26/DPP4) in organ fibrosis
Birte Ohm, Isabelle Moneke, Wolfgang Jungraithmayr
British Journal of Pharmacology.2023; 180(22): 2846. CrossRef - Linagliptin ameliorates pulmonary fibrosis in systemic sclerosis mouse model via inhibition of endothelial-to-mesenchymal transition
Biwei Pei, Na Zhang, Tingting Pang, Gengyun Sun
Molecular and Cellular Biochemistry.2022; 477(4): 995. CrossRef - Association Between DPP4 Inhibitor Use and the Incidence of Cirrhosis, ESRD, and Some Cancers in Patients With Diabetes
Yewon Na, Soo Wan Kim, Ie Byung Park, Soo Jung Choi, Seungyoon Nam, Jaehun Jung, Dae Ho Lee
The Journal of Clinical Endocrinology & Metabolism.2022; 107(11): 3022. CrossRef - Evogliptin Directly Inhibits Inflammatory and Fibrotic Signaling in Isolated Liver Cells
Hye-Young Seo, So-Hee Lee, Eugene Han, Jae Seok Hwang, Sol Han, Mi Kyung Kim, Byoung Kuk Jang
International Journal of Molecular Sciences.2022; 23(19): 11636. CrossRef - Optimization and validation of a fluorogenic dipeptidyl peptidase 4 enzymatic assay in human plasma
Hyunyee Yoon, Su Hee Cho, Yu Rim Seo, Kyung-Sang Yu, Sung Sup Park, Moon Jung Song
Analytical Biochemistry.2021; 612: 113952. CrossRef - Use of Anti-Diabetic Agents in Non-Diabetic Kidney Disease: From Bench to Bedside
Sungjin Chung, Gheun-Ho Kim
Life.2021; 11(5): 389. CrossRef - Targeting Dermal Fibroblast Subtypes in Antifibrotic Therapy: Surface Marker as a Cellular Identity or a Functional Entity?
Xin Huang, Yimin Khoong, Chengyao Han, Dai Su, Hao Ma, Shuchen Gu, Qingfeng Li, Tao Zan
Frontiers in Physiology.2021;[Epub] CrossRef - Efficacy and safety of evogliptin treatment in patients with type 2 diabetes: A multicentre, active‐controlled, randomized, double‐blind study with open‐label extension (the EVERGREEN study)
Gyuri Kim, Soo Lim, Hyuk‐Sang Kwon, Ie B. Park, Kyu J. Ahn, Cheol‐Young Park, Su K. Kwon, Hye S. Kim, Seok W. Park, Sin G. Kim, Min K. Moon, Eun S. Kim, Choon H. Chung, Kang S. Park, Mikyung Kim, Dong J. Chung, Chang B. Lee, Tae H. Kim, Moon‐Kyu Lee
Diabetes, Obesity and Metabolism.2020; 22(9): 1527. CrossRef Effect of Switching from Linagliptin to Teneligliptin Dipeptidyl Peptidase-4 Inhibitors in Older Patients with Type 2 Diabetes Mellitus
Eugene Han, Minyoung Lee, Yong-ho Lee, Hye Soon Kim, Byung-wan Lee, Bong-Soo Cha, Eun Seok Kang
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2020; Volume 13: 4113. CrossRef- Efficacy and safety of novel dipeptidyl-peptidase-4 inhibitor evogliptin in the management of type 2 diabetes mellitus: A meta-analysis
Deep Dutta, Saptarshi Bhattacharya, Aishwarya Krishnamurthy, LokeshKumar Sharma, Meha Sharma
Indian Journal of Endocrinology and Metabolism.2020; 24(5): 434. CrossRef
- Targeting cluster of differentiation 26 / dipeptidyl peptidase 4 (CD26/DPP4) in organ fibrosis
- Drug/Regimen
- Efficacy and Safety of Pioglitazone versus Glimepiride after Metformin and Alogliptin Combination Therapy: A Randomized, Open-Label, Multicenter, Parallel-Controlled Study
- Jeong Mi Kim, Sang Soo Kim, Jong Ho Kim, Mi Kyung Kim, Tae Nyun Kim, Soon Hee Lee, Chang Won Lee, Ja Young Park, Eun Sook Kim, Kwang Jae Lee, Young Sik Choi, Duk Kyu Kim, In Joo Kim
- Diabetes Metab J. 2020;44(1):67-77. Published online July 11, 2019
- DOI: https://doi.org/10.4093/dmj.2018.0274
- 7,516 View
- 156 Download
- 5 Web of Science
- 7 Crossref
-
Abstract
PDFPubReader
Background There is limited information regarding the optimal third-line therapy for managing type 2 diabetes mellitus (T2DM) that is inadequately controlled using dual combination therapy. This study assessed the efficacy and safety of pioglitazone or glimepiride when added to metformin plus alogliptin treatment for T2DM.
Methods This multicenter, randomized, active-controlled trial (
ClinicalTrials.gov :NCT02426294 ) recruited 135 Korean patients with T2DM that was inadequately controlled using metformin plus alogliptin. The patients were then randomized to also receive pioglitazone (15 mg/day) or glimepiride (2 mg/day) for a 26-week period, with dose titration was permitted based on the investigator's judgement.Results Glycosylated hemoglobin levels exhibited similar significant decreases in both groups during the treatment period (pioglitazone: −0.81%,
P <0.001; glimepiride: −1.05%,P <0.001). However, the pioglitazone-treated group exhibited significantly higher high density lipoprotein cholesterol levels (P <0.001) and significantly lower homeostatic model assessment of insulin resistance values (P <0.001). Relative to pioglitazone, adding glimepiride to metformin plus alogliptin markedly increased the risk of hypoglycemia (pioglitazone: 1/69 cases [1.45%], glimepiride: 14/66 cases [21.21%];P <0.001).Conclusion Among patients with T2DM inadequately controlled using metformin plus alogliptin, the addition of pioglitazone provided comparable glycemic control and various benefits (improvements in lipid profiles, insulin resistance, and hypoglycemia risk) relative to the addition of glimepiride.
-
Citations
Citations to this article as recorded by- Cost-effectiveness and budget impact analysis of fixed combination of alogliptin and pioglitazone in the treatment of type 2 diabetes mellitus
Yu.V. Strunina, N.A. Petunina
Medical Technologies. Assessment and Choice.2023; (3): 70. CrossRef - Pioglitazone-Enhanced Brown Fat Whitening Contributes to Weight Gain
in Diet-Induced Obese Mice
Piaojian Yu, Wei Wang, Wanrong Guo, Lidan Cheng, Zhiping Wan, Yanglei Cheng, Yunfeng Shen, Fen Xu
Experimental and Clinical Endocrinology & Diabetes.2023; 131(11): 595. CrossRef - Compliance with Cardiovascular Prevention Guidelines in Type 2 Diabetes Individuals in a Middle-Income Region: A Cross-Sectional Analysis
Joaquim Barreto, Beatriz Luchiari, Vaneza L. W. Wolf, Isabella Bonilha, Ticiane G. Bovi, Barbara S. Assato, Ikaro Breder, Sheila T. Kimura-Medorima, Daniel B. Munhoz, Thiago Quinaglia, Otavio R. Coelho-Filho, Luiz Sergio F. Carvalho, Wilson Nadruz, Andrei
Diagnostics.2022; 12(4): 814. CrossRef - Effects of Glimepiride Combined with Recombinant Human Insulin Injection on Serum IGF-1, VEGF and TRACP-5b Oxidative Stress Levels in Patients with Type 2 Diabetes Mellitus
Xue Chen, Sheng Kang, Zeqing Bao, Ciara Hughes
Evidence-Based Complementary and Alternative Medicine.2022; 2022: 1. CrossRef - Glycaemic control with add‐on thiazolidinedione or a sodium‐glucose co‐transporter‐2 inhibitor in patients with type 2 diabetes after the failure of an oral triple antidiabetic regimen: A 24‐week, randomized controlled trial
Jaehyun Bae, Ji Hye Huh, Minyoung Lee, Yong‐Ho Lee, Byung‐Wan Lee
Diabetes, Obesity and Metabolism.2021; 23(2): 609. CrossRef - Development and validation of a sensitive LC-MS/MS method for pioglitazone: application towards pharmacokinetic and tissue distribution study in rats
Kusuma Kumari G., Praveen Thaggikuppe Krishnamurthy, Ravi Kiran Ammu V. V. V., Kurawattimath Vishwanath, S. T. Narenderan, B. Babu, Nagappan Krishnaveni
RSC Advances.2021; 11(19): 11437. CrossRef - Compliance with Cardiovascular Prevention Guidelines in Individuals with Type 2 Diabetes in a Middle-Income Region: Cross-Sectional Analysis
Joaquim Barreto, Beatriz Luchiari, Vaneza Lira W. Wolf, Isabella Bonilha, Ticiane G. Bovi, Barbara S. Assato, Ikaro Breder, Sheila T. Kimura-Medorima, Daniel B. Munhoz, Thiago Quinaglia, Otavio R. Coelho-Filho, Luiz Sérgio Fernandes de Carvalho, Wilson Na
SSRN Electronic Journal .2021;[Epub] CrossRef
- Cost-effectiveness and budget impact analysis of fixed combination of alogliptin and pioglitazone in the treatment of type 2 diabetes mellitus
- Complications
- Gemigliptin Attenuates Renal Fibrosis Through Down-Regulation of the NLRP3 Inflammasome
- Jung Beom Seo, Yeon-Kyung Choi, Hye-In Woo, Yun-A Jung, Sungwoo Lee, Seunghyeong Lee, Mihyang Park, In-Kyu Lee, Gwon-Soo Jung, Keun-Gyu Park
- Diabetes Metab J. 2019;43(6):830-839. Published online March 5, 2019
- DOI: https://doi.org/10.4093/dmj.2018.0181
- 5,417 View
- 128 Download
- 23 Web of Science
- 24 Crossref
-
Abstract
PDFPubReader
Background The hypoglycemic drugs dipeptidyl peptidase-4 (DPP-4) inhibitors have proven protective effects on diabetic kidney disease, including renal fibrosis. Although NOD-like receptor protein 3 (NLRP3) inflammasome activation is known to play an important role in the progression of renal fibrosis, the impact of DPP-4 inhibition on NLRP3-mediated inflammation while ameliorating renal fibrosis has not been fully elucidated. Here, we report that the renoprotective effect of gemigliptin is associated with a reduction in NLRP3-mediated inflammation in a murine model of renal fibrosis.
Methods We examined the effects of gemigliptin on renal tubulointerstitial fibrosis induced in mice by unilateral ureteral obstruction (UUO). Using immunohistochemical and Western blot analysis, we quantitated components of the NLRP3 inflammasome in kidneys with and without gemigliptin treatment, and
in vitro in human kidney tubular epithelial human renal proximal tubule cells (HK-2) cells, we further analyzed the effect of gemigliptin on transforming growth factor-β (TGF-β)-stimulated production of profibrotic proteins.Results Immunohistological examination revealed that gemigliptin ameliorated UUO-induced tubular atrophy and renal fibrosis. Gemigliptin-treated kidneys showed a reduction in levels of NLRP3, apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC), caspase-1, and interleukin-1β, which had all been markedly increased by UUO. In line with the
in vivo Conclusion The present study shows that activation of the NLRP3 inflammasome contributes to UUO-induced renal fibrosis and the renoprotective effect of gemigliptin is associated with attenuation of NLRP3 inflammasome activation.
-
Citations
Citations to this article as recorded by- Novel pharmacological interventions for diabetic kidney disease
Seng Kiong Tan, Jairo A. Pinzon-Cortes, Mark E. Cooper
Current Opinion in Nephrology & Hypertension.2024; 33(1): 13. CrossRef - Integrated analysis reveals crosstalk between pyroptosis and immune regulation in renal fibrosis
Fengxia Bai, Longchao Han, Jifeng Yang, Yuxiu Liu, Xiangmeng Li, Yaqin Wang, Ruijian Jiang, Zhaomu Zeng, Yan Gao, Haisong Zhang
Frontiers in Immunology.2024;[Epub] CrossRef - Di (2-ethylhexyl) phthalate and polystyrene microplastics co-exposure caused oxidative stress to activate NF-κB/NLRP3 pathway aggravated pyroptosis and inflammation in mouse kidney
Shanshan Li, Xuedie Gu, Muyue Zhang, Qihang Jiang, Tong Xu
Science of The Total Environment.2024; 926: 171817. CrossRef - Fluorofenidone attenuates renal fibrosis by inhibiting lysosomal cathepsin‑mediated NLRP3 inflammasome activation
Linfeng Zheng, Wenjuan Mei, Jing Zhou, Xin Wei, Zhijuan Huang, Xiaozhen Lin, Li Zhang, Wei Liu, Qian Wu, Jinhong Li, Yan Yan
Experimental and Therapeutic Medicine.2024;[Epub] CrossRef - HIF1α-BNIP3-mediated mitophagy protects against renal fibrosis by decreasing ROS and inhibiting activation of the NLRP3 inflammasome
Jialin Li, Qisheng Lin, Xinghua Shao, Shu Li, Xuying Zhu, Jingkui Wu, Shan Mou, Leyi Gu, Qin Wang, Minfang Zhang, Kaiqi Zhang, Jiayue Lu, Zhaohui Ni
Cell Death & Disease.2023;[Epub] CrossRef - Pyroptosis in renal inflammation and fibrosis: current knowledge and clinical significance
Ya Liu, Haibo Lei, Wenyou Zhang, Qichang Xing, Renzhu Liu, Shiwei Wu, Zheng Liu, Qingzi Yan, Wencan Li, Xiang Liu, Yixiang Hu
Cell Death & Disease.2023;[Epub] CrossRef - Tubular injury in diabetic kidney disease: molecular mechanisms and potential therapeutic perspectives
Yu Wang, Mingyue Jin, Chak Kwong Cheng, Qiang Li
Frontiers in Endocrinology.2023;[Epub] CrossRef - Hederagenin inhibits high glucose‐induced fibrosis in human renal cells by suppression of NLRP3 inflammasome activation through reducing cathepsin B expression
Guohua Yang, Wang Yang, Hairong Jiang, Qing Yi, Wei Ma
Chemical Biology & Drug Design.2023; 102(6): 1409. CrossRef - Obstructive nephropathy and molecular pathophysiology of renal interstitial fibrosis
Rikke Nørregaard, Henricus A. M. Mutsaers, Jørgen Frøkiær, Tae-Hwan Kwon
Physiological Reviews.2023; 103(4): 2847. CrossRef - Adenine model of chronic renal failure in rats to determine whether MCC950, an NLRP3 inflammasome inhibitor, is a renopreventive
Mahmoud S. Sabra, Fahmy K. Hemida, Essmat A. H. Allam
BMC Nephrology.2023;[Epub] CrossRef - Gut microbiota dysbiosis promotes age-related atrial fibrillation by lipopolysaccharide and glucose-induced activation of NLRP3-inflammasome
Yun Zhang, Song Zhang, Bolin Li, Yingchun Luo, Yongtai Gong, Xuexin Jin, Jiawei Zhang, Yun Zhou, Xiaozhen Zhuo, Zixi Wang, Xinbo Zhao, Xuejie Han, Yunlong Gao, Hui Yu, Desen Liang, Shiqi Zhao, Danghui Sun, Dingyu Wang, Wei Xu, Guangjin Qu, Wanlan Bo, Dan
Cardiovascular Research.2022; 118(3): 785. CrossRef - The NLRP3 inflammasome in fibrosis and aging: The known unknowns
Yanqing Liu, Xuezeng Xu, Wangrui Lei, Yuxuan Hou, Yan Zhang, Ran Tang, Zhi Yang, Ye Tian, Yanli Zhu, Changyu Wang, Chao Deng, Shaofei Zhang, Yang Yang
Ageing Research Reviews.2022; 79: 101638. CrossRef - Research progress of endothelial‐mesenchymal transition in diabetic kidney disease
Ying Chen, Hang Zou, Hongwei Lu, Hong Xiang, Shuhua Chen
Journal of Cellular and Molecular Medicine.2022; 26(12): 3313. CrossRef - Exploring the mechanism of Shendi Bushen capsule in anti-renal fibrosis using metabolomics theory and network analysis
Tianwei Meng, Hong Chang, Hongyu Meng
Molecular Omics.2022; 18(9): 873. CrossRef - Gemigliptin suppresses salivary dysfunction in streptozotocin-induced diabetic rats
Wan Seok Kang, Woo Kwon Jung, Su-Bin Park, Hyung Rae Kim, Junghyun Kim
Biomedicine & Pharmacotherapy.2021; 137: 111297. CrossRef - Long‐Term Dipeptidyl Peptidase 4 Inhibition Worsens Hypertension and Renal and Cardiac Abnormalities in Obese Spontaneously Hypertensive Heart Failure Rats
Edwin K. Jackson, Zaichuan Mi, Delbert G. Gillespie, Dongmei Cheng, Stevan P. Tofovic
Journal of the American Heart Association.2021;[Epub] CrossRef - Disulfiram inhibits inflammation and fibrosis in a rat unilateral ureteral obstruction model by inhibiting gasdermin D cleavage and pyroptosis
Yu Zhang, Ruicheng Zhang, Xiaohu Han
Inflammation Research.2021; 70(5): 543. CrossRef - Inflammasome as an Effective Platform for Fibrosis Therapy
Ting-Ting Chen, Feng Xiao, Nan Li, Shan Shan, Meng Qi, Zi-Ying Wang, Sheng-Nan Zhang, Wei Wei, Wu-Yi Sun
Journal of Inflammation Research.2021; Volume 14: 1575. CrossRef - Targeting Dermal Fibroblast Subtypes in Antifibrotic Therapy: Surface Marker as a Cellular Identity or a Functional Entity?
Xin Huang, Yimin Khoong, Chengyao Han, Dai Su, Hao Ma, Shuchen Gu, Qingfeng Li, Tao Zan
Frontiers in Physiology.2021;[Epub] CrossRef - Linagliptin Protects against Endotoxin-Induced Acute Kidney Injury in Rats by Decreasing Inflammatory Cytokines and Reactive Oxygen Species
Tsung-Jui Wu, Yi-Jen Hsieh, Chia-Wen Lu, Chung-Jen Lee, Bang-Gee Hsu
International Journal of Molecular Sciences.2021; 22(20): 11190. CrossRef - Psidium guajava Flavonoids Prevent NLRP3 Inflammasome Activation and Alleviate the Pancreatic Fibrosis in a Chronic Pancreatitis Mouse Model
Guixian Zhang, Liming Tang, Hongbin Liu, Dawei Liu, Manxue Wang, Jun Cai, Weijun Liu, Wei Nie, Yi Zhang, Xiaomeng Yu
The American Journal of Chinese Medicine.2021; 49(08): 2001. CrossRef - Effect and Regulation of the NLRP3 Inflammasome During Renal Fibrosis
Hong Zhang, Zhengchao Wang
Frontiers in Cell and Developmental Biology.2020;[Epub] CrossRef - Zhen-Wu-Tang Protects IgA Nephropathy in Rats by Regulating Exosomes to Inhibit NF-κB/NLRP3 Pathway
Honglian Li, Ruirui Lu, Yu Pang, Jicheng Li, Yiwen Cao, Hongxin Fu, Guoxing Fang, Qiuhe Chen, Bihao Liu, Junbiao Wu, Yuan Zhou, Jiuyao Zhou
Frontiers in Pharmacology.2020;[Epub] CrossRef - Protective effect of exogenous hydrogen sulfide on diaphragm muscle fibrosis in streptozotocin-induced diabetic rats
Rui Yang, Qiang Jia, Yan Li, Shomaila Mehmood
Experimental Biology and Medicine.2020; 245(14): 1280. CrossRef
- Novel pharmacological interventions for diabetic kidney disease
- Complications
- Dipeptidyl Peptidase-4 Inhibitors versus Other Antidiabetic Drugs Added to Metformin Monotherapy in Diabetic Retinopathy Progression: A Real World-Based Cohort Study
- Yoo-Ri Chung, Kyoung Hwa Ha, Hyeon Chang Kim, Sang Jun Park, Kihwang Lee, Dae Jung Kim
- Diabetes Metab J. 2019;43(5):640-648. Published online February 20, 2019
- DOI: https://doi.org/10.4093/dmj.2018.0137
- 5,011 View
- 66 Download
- 15 Web of Science
- 16 Crossref
-
Abstract
PDFSupplementary MaterialPubReader
Background To investigate the effects of dipeptidyl peptidase-4 inhibitor (DPP4i) as add-on medications to metformin on progression of diabetic retinopathy (DR) in patients with type 2 diabetes mellitus, compared with sulfonylurea (SU) or thiazolidinedione (TZD).
Methods We identified 4,447 patients with DPP4i, 6,136 with SU, and 617 with TZD in addition to metformin therapy from the database of Korean National Health Insurance Service between January 2013 and December 2015. Cox proportional hazards regression models were used to calculate hazard ratios (HRs) for DR progression. The progression of DR was defined by the procedure code of panretinal photocoagulation, intravitreal injection or vitrectomy; or the addition of diagnostic code of vitreous hemorrhage, retinal detachment, or neovascular glaucoma.
Results The age and sex-adjusted HR of DR progression was 0.74 for DPP4i add-on group compared with SU add-on group (95% confidence interval [CI], 0.62 to 0.89). This lower risk of DR progression remained significant after additional adjustments for comorbidities, duration of metformin therapy, intravitreal injections and calendar index year (HR, 0.80; 95% CI, 0.66 to 0.97).
Conclusion This population-based cohort study showed that the use of DPP4i as add-on therapy to metformin did not increase the risk of DR progression compared to SU.
-
Citations
Citations to this article as recorded by- Effects of newer-generation anti-diabetics on diabetic retinopathy: a critical review
Dimitrios P. Ntentakis, Victor San Martin Carvalho Correa, Anastasia Maria Ntentaki, Eleni Delavogia, Toshio Narimatsu, Nikolaos E. Efstathiou, Demetrios G. Vavvas
Graefe's Archive for Clinical and Experimental Ophthalmology.2024; 262(3): 717. CrossRef - Incretin‐based drugs and the risk of diabetic retinopathy among individuals with type 2 diabetes: A systematic review and meta‐analysis of observational studies
Samuel Igweokpala, Naheemot Olaoluwa Sule, Antonios Douros, Oriana H. Y. Yu, Kristian B. Filion
Diabetes, Obesity and Metabolism.2024; 26(2): 721. CrossRef - Weight loss, bariatric surgery, and novel antidiabetic drugs effects on diabetic retinopathy: a review
Alejandro M. Perez, Emily Neag, Jayanth Sridhar, Basil K. Williams
Current Opinion in Ophthalmology.2024; 35(3): 192. CrossRef - Role of Systemic Factors in Improving the Prognosis of Diabetic Retinal Disease and Predicting Response to Diabetic Retinopathy Treatment
Joe Mellor, Anita Jeyam, Joline W.J. Beulens, Sanjeeb Bhandari, Geoffrey Broadhead, Emily Chew, Ward Fickweiler, Amber van der Heijden, Daniel Gordin, Rafael Simó, Janet Snell-Bergeon, Anniina Tynjälä, Helen Colhoun
Ophthalmology Science.2024; 4(4): 100494. CrossRef - Novel Antidiabetic Drugs and the Risk of Diabetic Retinopathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Artur Małyszczak, Joanna Przeździecka-Dołyk, Urszula Szydełko-Paśko, Marta Misiuk-Hojło
Journal of Clinical Medicine.2024; 13(6): 1797. CrossRef - Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy
Jennifer Perais, Ridhi Agarwal, Jennifer R Evans, Emma Loveman, Jill L Colquitt, David Owens, Ruth E Hogg, John G Lawrenson, Yemisi Takwoingi, Noemi Lois
Cochrane Database of Systematic Reviews.2023;[Epub] CrossRef - Rapid Reduction of HbA1c and Early Worsening of Diabetic Retinopathy: A Real-world Population-Based Study in Subjects With Type 2 Diabetes
Rafael Simó, Josep Franch-Nadal, Bogdan Vlacho, Jordi Real, Ester Amado, Juana Flores, Manel Mata-Cases, Emilio Ortega, Mercedes Rigla, Joan-Anton Vallés, Cristina Hernández, Didac Mauricio
Diabetes Care.2023; 46(9): 1633. CrossRef - Minimum Effective Dose of DPP-4 Inhibitors for Treating Early Stages of Diabetic Retinopathy in an Experimental Model
Patricia Bogdanov, Hugo Ramos, Marta Valeri, Anna Deàs-Just, Jordi Huerta, Rafael Simó, Cristina Hernández
Biomedicines.2022; 10(2): 465. CrossRef - Glucagon-Like Peptide 1 Receptor Agonists – Potential Game Changers in the Treatment of Glaucoma?
Zaynab Ahmad Mouhammad, Rupali Vohra, Anna Horwitz, Anna-Sophie Thein, Jens Rovelt, Barbara Cvenkel, Pete A. Williams, Augusto Azuara-Blanco, Miriam Kolko
Frontiers in Neuroscience.2022;[Epub] CrossRef - Transcriptomic Analysis Reveals That Retinal Neuromodulation Is a Relevant Mechanism in the Neuroprotective Effect of Sitagliptin in an Experimental Model of Diabetic Retinopathy
Hugo Ramos, Patricia Bogdanov, Rafael Simó, Anna Deàs-Just, Cristina Hernández
International Journal of Molecular Sciences.2022; 24(1): 571. CrossRef - The Safety of Pharmacological and Surgical Treatment of Diabetes in Patients with Diabetic Retinopathy—A Review
Wojciech Matuszewski, Angelika Baranowska-Jurkun, Magdalena Maria Stefanowicz-Rutkowska, Katarzyna Gontarz-Nowak, Ewa Gątarska, Elżbieta Bandurska-Stankiewicz
Journal of Clinical Medicine.2021; 10(4): 705. CrossRef - Effects of Fibrates on Risk of Development of Diabetic Retinopathy in Japanese Working Age Patients with Type 2 Diabetes and Dyslipidemia: a Retrospective Cohort Study
Hayato Akimoto, Yasuo Takahashi, Satoshi Asai
YAKUGAKU ZASSHI.2021; 141(5): 761. CrossRef - Association between Add-On Dipeptidyl Peptidase-4 Inhibitor Therapy and Diabetic Retinopathy Progression
Eugene Yu-Chuan Kang, Chunya Kang, Wei-Chi Wu, Chi-Chin Sun, Kuan-Jen Chen, Chi-Chun Lai, Tien-Hsing Chen, Yih-Shiou Hwang
Journal of Clinical Medicine.2021; 10(13): 2871. CrossRef - Understanding molecular upsets in diabetic nephropathy to identify novel targets and treatment opportunities
Nidhi Raval, Akshant Kumawat, Dnyaneshwar Kalyane, Kiran Kalia, Rakesh K. Tekade
Drug Discovery Today.2020; 25(5): 862. CrossRef - Letter: Dipeptidyl Peptidase-4 Inhibitors versus Other Antidiabetic Drugs Added to Metformin Monotherapy in Diabetic Retinopathy Progression: A Real World-Based Cohort Study (Diabetes Metab J 2019;43:640–8)
Jun Sung Moon
Diabetes & Metabolism Journal.2019; 43(6): 911. CrossRef - Response: Dipeptidyl Peptidase-4 Inhibitors versus Other Antidiabetic Drugs Added to Metformin Monotherapy in Diabetic Retinopathy Progression: A Real World-Based Cohort Study (Diabetes Metab J 2019;43:640–8)
Yoo-Ri Chung, Kyoung Hwa Ha, Kihwang Lee, Dae Jung Kim
Diabetes & Metabolism Journal.2019; 43(6): 917. CrossRef
- Effects of newer-generation anti-diabetics on diabetic retinopathy: a critical review
- Clinical Care/Education
- Gemigliptin: An Update of Its Clinical Use in the Management of Type 2 Diabetes Mellitus
- Sung-Ho Kim, Jung-Hwa Yoo, Woo Je Lee, Cheol-Young Park
- Diabetes Metab J. 2016;40(5):339-353. Published online September 12, 2016
- DOI: https://doi.org/10.4093/dmj.2016.40.5.339
- 6,400 View
- 163 Download
- 42 Web of Science
- 40 Crossref
-
Abstract
PDFPubReader
Dipeptidyl peptidase-4 (DPP-4) inhibitors are a new class of oral antidiabetic agent for the treatment of type 2 diabetes mellitus. They increase endogenous levels of incretin hormones, which stimulate glucose-dependent insulin secretion, decrease glucagon secretion, and contribute to reducing postprandial hyperglycemia. Although DPP-4 inhibitors have similar benefits, they can be differentiated in terms of their chemical structure, pharmacology, efficacy and safety profiles, and clinical considerations. Gemigliptin (brand name: Zemiglo), developed by LG Life Sciences, is a potent, selective, competitive, and long acting DPP-4 inhibitor. Various studies have shown that gemigliptin is an optimized DPP-4 inhibitor in terms of efficacy, safety, and patient compliance for treatment of type 2 diabetes mellitus. In this review, we summarize the characteristics of gemigliptin and discuss its potential benefits in clinical practice.
-
Citations
Citations to this article as recorded by- A Multicenter, Randomized, Open-Label Study to Compare the Effects of Gemigliptin Add-on or Escalation of Metformin Dose on Glycemic Control and Safety in Patients with Inadequately Controlled Type 2 Diabetes Mellitus Treated with Metformin and SGLT-2 Inh
Hae Jin Kim, Jung Hyun Noh, Min Kyong Moon, Sung Hee Choi, Seung-Hyun Ko, Eun-Jung Rhee, Kyu Yeon Hur, In-Kyung Jeong, Mark Yorek
Journal of Diabetes Research.2024; 2024: 1. CrossRef - Gemigliptin, a potent selective dipeptidyl peptidase 4 inhibitor, protects endothelial progenitor cells by oxidative stress via caspase-3 dependent pathway
Mijung Lee, Amna Rashid Tariq, Manho Kim
Biochemistry and Biophysics Reports.2024; 38: 101673. CrossRef - Selective targeting of dipeptidyl‐peptidase 4 (DPP‐4) positive senescent chondrocyte ameliorates osteoarthritis progression
Du Hyun Ro, Gun Hee Cho, Ji Yoon Kim, Seong Ki Min, Ha Ru Yang, Hee Jung Park, Sun Young Wang, You Jung Kim, Myung Chul Lee, Hyun Cheol Bae, Hyuk‐Soo Han
Aging Cell.2024;[Epub] CrossRef - Opportunities and challenges of incretin-based hypoglycemic agents treating type 2 diabetes mellitus from the perspective of physiological disposition
Yaochen Xie, Qian Zhou, Qiaojun He, Xiaoyi Wang, Jincheng Wang
Acta Pharmaceutica Sinica B.2023; 13(6): 2383. CrossRef - Therapeutic Effects of Switching to Anagliptin from Other DPP-4 Inhibitors in T2DM Patients with Inadequate Glycemic Control: A Non-interventional, Single-Arm, Open-Label, Multicenter Observational Study
Sang-Yong Kim, Sungrae Kim
Diabetes Therapy.2023; 14(1): 109. CrossRef - Pharmacokinetic and pharmacodynamic interaction of DWP16001, a sodium–glucose cotransporter 2 inhibitor, with gemigliptin and metformin in healthy adults
Sae Im Jeong, Yun Kim, Jae Jin Nah, Wan Huh, In‐Jin Jang, Jun Gi Hwang, SeungHwan Lee
British Journal of Clinical Pharmacology.2023; 89(6): 1780. CrossRef - 1,2,3‐Triazole analogs with bulky and conformationally rigid substructures: Synthesis and in vitro evaluation as DPP‐4 inhibitors
Duy‐Viet Vo, Jongkook Lee, Haeil Park
Bulletin of the Korean Chemical Society.2023; 44(5): 425. CrossRef - DPP-4 inhibitors for treating T2DM - hype or hope? an analysis based on the current literature
Kunika Saini, Smriti Sharma, Yousuf Khan
Frontiers in Molecular Biosciences.2023;[Epub] CrossRef - The effect of gemigliptin treatment on immune parameters including regulatory T cells in patients with type 2 diabetes and moderate to very severe chronic renal impairment
Yanghyeon Kim, Nagyeom Lee, Sujung Heo, Ye Na Kim, Ho Sik Shin, Yeonsoon Jung, Hark Rim
Medicine.2023; 102(49): e36455. CrossRef - Increasing Age Associated with Higher Dipeptidyl Peptidase-4 Inhibition Rate Is a Predictive Factor for Efficacy of Dipeptidyl Peptidase-4 Inhibitors
Sangmo Hong, Chang Hee Jung, Song Han, Cheol-Young Park
Diabetes & Metabolism Journal.2022; 46(1): 63. CrossRef - Does DPP-IV Inhibition Offer New Avenues for Therapeutic Intervention in Malignant Disease?
Petr Busek, Jonathan S. Duke-Cohan, Aleksi Sedo
Cancers.2022; 14(9): 2072. CrossRef - Divergent Reaction of Activated Pyridines with α,α-Difluorinated gem-Diols: Regioselective Synthesis of gem-Difluorinated Dihydropyridines and Dihydropyridones
Koushik Patra, Mallu Kesava Reddy, Sumitava Mallik, Mahiuddin Baidya
Organic Letters.2022; 24(22): 4014. CrossRef - Gemigliptin exerts protective effects against doxorubicin-induced hepatotoxicity by inhibiting apoptosis via the regulation of fibroblast growth factor 21 expression
Kyeong-Min Lee, Yeo Jin Hwang, Gwon-Soo Jung
Biochemical and Biophysical Research Communications.2022; 626: 135. CrossRef - FDA-Approved Trifluoromethyl Group-Containing Drugs: A Review of 20 Years
Aathira Sujathan Nair, Ashutosh Kumar Singh, Astik Kumar, Sunil Kumar, Sunitha Sukumaran, Vishal Payyalot Koyiparambath, Leena K. Pappachen, T. M. Rangarajan, Hoon Kim, Bijo Mathew
Processes.2022; 10(10): 2054. CrossRef - Glucagon-like peptide-1 (GLP-1) receptor agonists and neuroinflammation: Implications for neurodegenerative disease treatment
Katherine O. Kopp, Elliot J. Glotfelty, Yazhou Li, Nigel H. Greig
Pharmacological Research.2022; 186: 106550. CrossRef - An evaluation of drug lag for new drugs approved by the Indian regulator relative to the United States, European Union, and Japanese regulatory agencies: A 15-year analysis (2004–2018)
Mahanjit Konwar, MiteshR Maurya, TusharB Nishandar, UrmilaM Thatte, NithyaJ Gogtay
Perspectives in Clinical Research.2021; 12(3): 159. CrossRef - Pharmacokinetic and Pharmacodynamic Comparison of Two Formulations of a Fixed-Dose Combination of Gemigliptin/Rosuvastatin 50/20 mg: A Randomized, Open-Label, Single-Dose, Two-Way Crossover Study
Eunsol Yang, Hyounggyoon Yoo, In-Jin Jang, Kyung-Sang Yu, SeungHwan Lee
Drug Design, Development and Therapy.2021; Volume 15: 651. CrossRef - Efficacy and Safety of the Novel Dipeptidyl Peptidase-4 Inhibitor Gemigliptin in the Management of Type 2 Diabetes: A Meta-Analysis
Deep Dutta, Anshita Agarwal, Indira Maisnam, Rajiv Singla, Deepak Khandelwal, Meha Sharma
Endocrinology and Metabolism.2021; 36(2): 374. CrossRef - Structure–Activity Relationship Analysis of Cocrystallized Gliptin-like Pyrrolidine, Trifluorophenyl, and Pyrimidine-2,4-Dione Dipeptidyl Peptidase-4 Inhibitors
Katarina Tomovic, Budimir S. Ilic, Andrija Smelcerovic
Journal of Medicinal Chemistry.2021; 64(14): 9639. CrossRef - A review upon medicinal perspective and designing rationale of DPP-4 inhibitors
Shubham Kumar, Anu Mittal, Amit Mittal
Bioorganic & Medicinal Chemistry.2021; 46: 116354. CrossRef - Effect of Dipeptidyl Peptidase-4 (DPP-4) Inhibition on Biomarkers of Kidney Injury and Vascular Calcification in Diabetic Kidney Disease: A Randomized Controlled Trial
Thananda Trakarnvanich, Bancha Satirapoj, Swangjit Suraamornkul, Thanit Chirananthavat, Anoma Sanpatchayapong, Torpong Claimon, Eusebio Chiefari
Journal of Diabetes Research.2021; 2021: 1. CrossRef - Antidiabetic effect of gemigliptin: a systematic review and meta-analysis of randomized controlled trials with Bayesian inference through a quality management system
Hojin Oh, Hai Duc Nguyen, In Mo Yoon, Byung-Ryong Ahn, Min-Sun Kim
Scientific Reports.2021;[Epub] CrossRef - Pleiotropic Benefits of DPP-4 Inhibitors Beyond Glycemic Control
Seon Mee Kang, Jeong Hyun Park
Clinical Medicine Insights: Endocrinology and Diabetes.2021; 14: 117955142110516. CrossRef - The vasodilatory effect of gemigliptin via activation of voltage-dependent K+ channels and SERCA pumps in aortic smooth muscle
Hee Seok Jung, Mi Seon Seo, Jin Ryeol An, Minji Kang, Ryeon Heo, Hongliang Li, Won-Kyo Jung, Il-Whan Choi, Eun-Hee Cho, Hongzoo Park, Young Min Bae, Won Sun Park
European Journal of Pharmacology.2020; 882: 173243. CrossRef - Development and Validation of a Rapid and Sensitive Method for the Simultaneous Estimation of Gemigliptin and Teneligliptin in Bulk and Dosage Forms by Using Liquid Chromatography-tandem Mass Spectrometry
Amrish Chandra, Ramji Rathod, Faraat Ali, Anuj Prakash, Robin Kumar, Gyanendra Nath Singh
Current Pharmaceutical Analysis.2020; 16(8): 1104. CrossRef - Incretin Mimetics as Rational Candidates for the Treatment of Traumatic Brain Injury
Elliot J. Glotfelty, Thomas E. Delgado, Luis B. Tovar-y-Romo, Yu Luo, Barry J. Hoffer, Lars Olson, Tobias E. Karlsson, Mark P. Mattson, Brandon K. Harvey, David Tweedie, Yazhou Li, Nigel H. Greig
ACS Pharmacology & Translational Science.2019; 2(2): 66. CrossRef - Mechanisms and pathways of anti‐inflammatory activity of DPP‐4 inhibitors in cardiovascular and renal protection
Katarina Tomovic, Jelena Lazarevic, Gordana Kocic, Marina Deljanin‐Ilic, Marko Anderluh, Andrija Smelcerovic
Medicinal Research Reviews.2019; 39(1): 404. CrossRef - Dipeptidyl Peptidase-4 Inhibitors versus Other Antidiabetic Drugs Added to Metformin Monotherapy in Diabetic Retinopathy Progression: A Real World-Based Cohort Study
Yoo-Ri Chung, Kyoung Hwa Ha, Hyeon Chang Kim, Sang Jun Park, Kihwang Lee, Dae Jung Kim
Diabetes & Metabolism Journal.2019; 43(5): 640. CrossRef - Effect of gemigliptin on cardiac ischemia/reperfusion and spontaneous hypertensive rat models
Dae-Hwan Nam, Jinsook Park, Sun-Hyun Park, Ki-Suk Kim, Eun Bok Baek
The Korean Journal of Physiology & Pharmacology.2019; 23(5): 329. CrossRef - Clinical Use of DPP-4 Inhibitors
Baptist Gallwitz
Frontiers in Endocrinology.2019;[Epub] CrossRef - Efficacy and Safety of Switching to Teneligliptin in Patients with Type 2 Diabetes Inadequately Controlled with Dipeptidyl Peptidase-4 Inhibitors: A 12-Week Interim Report
Hae Jin Kim, Young Sik Kim, Chang Beom Lee, Moon-Gi Choi, Hyuk-Jae Chang, Soo Kyoung Kim, Jae Myung Yu, Tae Ho Kim, Ji Hyun Lee, Kyu Jeung Ahn, Kyoungmin Kim, Kwan Woo Lee
Diabetes Therapy.2019; 10(4): 1271. CrossRef - Efficacy and Safety of Gemigliptin in Post-Transplant Patients With Type 2 Diabetes Mellitus
Jaehyun Bae, Youjin Kim, Yongin Cho, Minyoung Lee, Ji-Yeon Lee, Yong-ho Lee, Byung-Wan Lee, Bong-Soo Cha, Dong Jin Joo, Kyu Ha Huh, Myoung Soo Kim, Yu Seun Kim, Eun Seok Kang
Transplantation Proceedings.2019; 51(10): 3444. CrossRef - Protective effects of gemigliptin against type II collagen degradation in human chondrocytes
Momin Mohetaer, Guoqing Li, Yang Wang, Li Cao
Biomedicine & Pharmacotherapy.2018; 104: 590. CrossRef - Pharmacokinetic Interactions Between Gemigliptin and Metformin, and Potential Differences in the Pharmacokinetic Profile of Gemigliptin Between the Mexican and Korean Populations: A Randomized, Open-label Study in Healthy Mexican Volunteers
Ignacio Conde-Carmona, Sandra García-Medina, Juan M. Jiménez-Vargas, Alberto Martínez-Muñoz, Sung-Hack Lee
Clinical Therapeutics.2018; 40(10): 1729. CrossRef - Comparative efficacy and safety of gemigliptin versus linagliptin in type 2 diabetes patients with renal impairment: A 40‐week extension of the GUARD randomized study
Sang Youb Han, Sun Ae Yoon, Byoung Geun Han, Sung Gyun Kim, Young‐Il Jo, Kyung Hwan Jeong, Kook‐Hwan Oh, Hyeong Cheon Park, Sun‐Hee Park, Shin‐Wook Kang, Ki‐Ryang Na, Sun Woo Kang, Nam‐Ho Kim, Younghwan Jang, Bogyeong Kim, Seonghye Shin, Dae Ryong Cha
Diabetes, Obesity and Metabolism.2018; 20(2): 292. CrossRef - Comparative Cardiovascular Risks of Dipeptidyl Peptidase-4 Inhibitors: Analyses of Real-world Data in Korea
Kyoung Hwa Ha, Bongseong Kim, Hae Sol Shin, Jinhee Lee, Hansol Choi, Hyeon Chang Kim, Dae Jung Kim
Korean Circulation Journal.2018; 48(5): 395. CrossRef - Gemigliptin: Newer promising gliptin for type 2 diabetes mellitus
Manish Gutch, Abhay Joshi, Sukriti Kumar, Avinash Agarwal, RajendraKumar Pahan, SyedMohd Razi
Indian Journal of Endocrinology and Metabolism.2017; 21(6): 898. CrossRef - Protective Effects of Gemigliptin, a Dipeptidyl Peptidase-4 Inhibitor, against Cisplatin-Induced Nephrotoxicity in Mice
Seung Hee Choi, Jaechan Leem, In-Kyu Lee
Mediators of Inflammation.2017; 2017: 1. CrossRef - Effects of gemigliptin, a dipeptidyl peptidase‐4 inhibitor, on lipid metabolism and endotoxemia after a high‐fat meal in patients with type 2 diabetes
Chang Ho Ahn, Eun Ky Kim, Se Hee Min, Tae Jung Oh, Young Min Cho
Diabetes, Obesity and Metabolism.2017; 19(3): 457. CrossRef - Efficacy and safety of gemigliptin, a dipeptidyl peptidase‐4 inhibitor, in patients with type 2 diabetes mellitus inadequately controlled with combination treatment of metformin and sulphonylurea: a 24‐week, multicentre, randomized, double‐blind, placebo‐
Chang Ho Ahn, Kyung Ah Han, Jae Myung Yu, Joo Young Nam, Kyu Jeung Ahn, Tae Keun Oh, Hyoung Woo Lee, Dae Ho Lee, Jaetaek Kim, Choon Hee Chung, Tae Sun Park, Byung Joon Kim, Seok Won Park, Hyeong Kyu Park, Kwang Jae Lee, Sang‐Wook Kim, Jeong Hyun Park, Kwa
Diabetes, Obesity and Metabolism.2017; 19(5): 635. CrossRef
- A Multicenter, Randomized, Open-Label Study to Compare the Effects of Gemigliptin Add-on or Escalation of Metformin Dose on Glycemic Control and Safety in Patients with Inadequately Controlled Type 2 Diabetes Mellitus Treated with Metformin and SGLT-2 Inh
- Clinical Care/Education
- Clinical Characteristics and Metabolic Predictors of Rapid Responders to Dipeptidyl Peptidase-4 Inhibitor as an Add-on Therapy to Sulfonylurea and Metformin
- Ye An Kim, Won Sang Yoo, Eun Shil Hong, Eu Jeong Ku, Kyeong Seon Park, Soo Lim, Young Min Cho, Kyong Soo Park, Hak Chul Jang, Sung Hee Choi
- Diabetes Metab J. 2015;39(6):489-497. Published online November 27, 2015
- DOI: https://doi.org/10.4093/dmj.2015.39.6.489
- 3,502 View
- 39 Download
- 1 Web of Science
- 1 Crossref
-
Abstract
PDFPubReader
Background Dipeptidyl peptidase-4 (DPP-4) inhibitor add-on therapy is a new option for patients with inadequately controlled type 2 diabetes who are taking combined metformin and sulfonylurea (SU). We evaluated the efficacy and safety of this triple therapy and the characteristics of rapid responders and hypoglycemia-prone patients.
Methods We included 807 patients with type 2 diabetes who were prescribed a newly added DPP-4 inhibitor to ongoing metformin and SU in 2009 to 2011. Glycemia and other metabolic parameters at baseline, 12, 24, and 52 weeks, as well as episodes of hypoglycemia were analyzed. Rapid responders were defined as patients with ≥25% reduction in glycosylated hemoglobin (HbA1c) within 12 weeks.
Results At baseline, while on the submaximal metformin and SU combination, the mean HbA1c level was 8.4%. Twelve weeks after initiation of DPP-4 inhibitor add-on, 269 patients (34.4%) achieved an HbA1c level ≤7%. Sixty-six patients (8.2%, 47 men) were rapid responders. The duration of diabetes was shorter in rapid responders, and their baseline fasting plasma glucose (FPG), HbA1c, C-peptide, and homeostasis model assessment of insulin resistance were significantly higher. Patients who experienced hypoglycemia after taking DPP-4 inhibitor add-on were more likely to be female, to have a lower body weight and lower triglyceride and FPG levels, and to have higher homeostasis model assessment of β-cells.
Conclusion An oral hypoglycemic triple agent combination including a DPP-4 inhibitor was effective in patients with uncontrolled diabetes. Proactive dose reduction of SU should be considered when a DPP-4 inhibitor is added for rapid responders and hypoglycemia-prone patients.
-
Citations
Citations to this article as recorded by- A genetic variant in GLP1R is associated with response to DPP-4 inhibitors in patients with type 2 diabetes
Eugene Han, Hye Sun Park, Obin Kwon, Eun Yeong Choe, Hye Jin Wang, Yong-ho Lee, Sang-Hak Lee, Chul Hoon Kim, Lee-Kyung Kim, Soo Heon Kwak, Kyong Soo Park, Chul Sik Kim, Eun Seok Kang
Medicine.2016; 95(44): e5155. CrossRef
- A genetic variant in GLP1R is associated with response to DPP-4 inhibitors in patients with type 2 diabetes
- Predictive Factors for Efficacy of Dipeptidyl Peptidase-4 Inhibitors in Patients with Type 2 Diabetes Mellitus
- Shusuke Yagi, Ken-ichi Aihara, Masashi Akaike, Daiju Fukuda, Hotimah Masdan Salim, Masayoshi Ishida, Tomomi Matsuura, Takayuki Ise, Koji Yamaguchi, Takashi Iwase, Hirotsugu Yamada, Takeshi Soeki, Tetsuzo Wakatsuki, Michio Shimabukuro, Toshio Matsumoto, Masataka Sata
- Diabetes Metab J. 2015;39(4):342-347. Published online July 21, 2015
- DOI: https://doi.org/10.4093/dmj.2015.39.4.342
- 3,993 View
- 54 Download
- 18 Web of Science
- 15 Crossref
-
Abstract
PDFPubReader
Background Predictive factors for the efficacy of dipeptidyl peptidase-4 (DPP-4) inhibitors for lowering glycosylated hemoglobin (HbA1c) remain unclear in patients with type 2 diabetes mellitus. The aim of this study is therefore to clarify predictive factors of the efficacy of DPP-4 inhibitors for lowering HbA1c after 12 months of treatment.
Methods A total of 191 consecutive type 2 diabetic patients (male sex 55%, mean age, 68.3±35.8 years), who had been treated with DPP-4 inhibitors for 12 months, were enrolled in this study and evaluated retrospectively.
Results After 12 months of DPP-4 inhibitor treatment, random blood glucose level, and HbA1c level, decreased from 167±63 to 151±49 mg/dL (
P <0.01), and from 7.5%±1.3% to 6.9%±0.9% (P <0.01) respectively, without severe side effects. Multiple regression analysis showed that predictors of DPP-4 inhibitor treatment efficacy in lowering HbA1c level after 12 months were a decrease in HbA1c level after 3 months of treatment, a high baseline HbA1c level, a low baseline body mass index, and the absence of coronary artery disease.Conclusion Most suitable candidates for treatment with DPP-4 inhibitors are diabetics who are not obese and do not have coronary artery disease. In addition, long-term efficacy of DPP-4 inhibitors can be predicted by decrement of HbA1c after 3 months of treatment.
-
Citations
Citations to this article as recorded by- Endogenous GLP-1 levels play an important role in determining the efficacy of DPP-IV Inhibitors in both prediabetes and type 2 diabetes
Shiau Chin Chong, Norlela Sukor, Sarah Anne Robert, Kim Fong Ng, Nor Azmi Kamaruddin
Frontiers in Endocrinology.2022;[Epub] CrossRef - Dipeptidyl peptidase‐4 inhibitor, anagliptin, alters hepatic insulin clearance in relation to the glycemic status in Japanese individuals with type 2 diabetes
Takahiro Abe, Yasuhiro Matsubayashi, Sayaka Muragishi, Akihiro Yoshida, Hideki Suganami, Kenichi Furusawa, Kazuya Fujihara, Shiro Tanaka, Kohei Kaku, Hirohito Sone
Journal of Diabetes Investigation.2021; 12(10): 1805. CrossRef - Effects of omarigliptin on glucose variability and oxidative stress in type 2 diabetes patients: A prospective study
Makoto Ohara, Hiroe Nagaike, Tomoki Fujikawa, Yo Kohata, Maiho Ogawa, Takemasa Omachi, Risa Sasajima, Hirotoshi Chiba, Toshimasa Ara, Ayuka Sugawara, Munenori Hiromura, Michishige Terasaki, Yusaku Mori, Tomoyasu Fukui, Tsutomu Hirano, Hiroki Yokoyama, Sho
Diabetes Research and Clinical Practice.2021; 179: 108999. CrossRef - Factors associated with the glucose‐lowering efficacy of sitagliptin in Japanese patients with type 2 diabetes mellitus: Pooled analysis of Japanese clinical trials
Naoko Tajima, Jun‐ichi Eiki, Taro Okamoto, Kotoba Okuyama, Masaru Kawashima, Samuel S Engel
Journal of Diabetes Investigation.2020; 11(3): 640. CrossRef - Efficacy and safety of evogliptin versus sitagliptin as add on to metformin alone in a combined russian-korean population. Evo-combi trial
Alina Y. Babenko, Anna A. Mosikian, Igor E. Makarenko, Victoriya V. Leusheva, Evgeny V. Shlyakhto
Diabetes mellitus.2018; 21(4): 241. CrossRef - Predictors for the Treatment Effect of Sodium Glucose Co-transporter 2 Inhibitors in Patients with Type 2 Diabetes Mellitus
Shusuke Yagi, Ken-ichi Aihara, Takeshi Kondo, Kiyoe Kurahashi, Sumiko Yoshida, Itsuro Endo, Daiju Fukuda, Yutaka Nakaya, Kin-ichiro Suwaki, Takashi Takeji, Toshihiro Wada, Hotimah Masdan Salim, Saori Hama, Tomomi Matsuura, Takayuki Ise, Kenya Kusunose, Ko
Advances in Therapy.2018; 35(1): 124. CrossRef - Ethnic Differences in Efficacy and Safety of Alogliptin: A Systematic Review and Meta-Analysis
Yuli Cai, Tianshu Zeng, Zhongyuan Wen, Lulu Chen
Diabetes Therapy.2018; 9(1): 177. CrossRef - Effectiveness prediction of Evogliptin treatment in type 2 diabetes mellitus in russian-korean population
Anna A. Mosikian, Alina Y. Babenko, Yulia A. Sevastyanova, Roman V. Drai, Evgenij V. Shlyakhto
Diabetes mellitus.2018; 21(5): 333. CrossRef - Efficacy and Safety of Linagliptin in 2681 Asian Patients Stratified by Age, Obesity, and Renal Function: A Pooled Analysis of Randomized Clinical Trials
Guang Ning, Tushar Bandgar, Uwe Hehnke, Jisoo Lee, Juliana C. N. Chan
Advances in Therapy.2017; 34(9): 2150. CrossRef - Potential regulatory mechanisms of lncRNA in diabetes and its complications
Shui-Dong Feng, Ji-Hua Yang, Chao Hua Yao, Si-Si Yang, Ze-Mei Zhu, Di Wu, Hong-Yan Ling, Liang Zhang
Biochemistry and Cell Biology.2017; 95(3): 361. CrossRef - Baseline Body Mass Index and the Efficacy of Hypoglycemic Treatment in Type 2 Diabetes: A Meta-Analysis
Xiaoling Cai, Wenjia Yang, Xueying Gao, Lingli Zhou, Xueyao Han, Linong Ji, Francesco Giorgino
PLOS ONE.2016; 11(12): e0166625. CrossRef - Efficacy of hypoglycemic treatment in type 2 diabetes stratified by age or diagnosed age: a meta-analysis
Xiaoling Cai, Wenjia Yang, Yifei Chen, Xueying Gao, Lingli Zhou, Simin Zhang, Xueyao Han, Linong Ji
Expert Opinion on Pharmacotherapy.2016; 17(12): 1591. CrossRef - Pharmacokinetic, pharmacodynamic and clinical evaluation of saxagliptin in type 2 diabetes
Rose Anderson, Jennifer Hayes, Jeffrey W. Stephens
Expert Opinion on Drug Metabolism & Toxicology.2016; 12(4): 467. CrossRef - Letter: Predictive Factors for Efficacy of Dipeptidyl Peptidase-4 Inhibitors in Patients with Type 2 Diabetes Mellitus (Diabetes Metab J2015;39:342-7)
Ye An Kim
Diabetes & Metabolism Journal.2015; 39(5): 444. CrossRef - Response: Predictive Factors for Efficacy of Dipeptidyl Peptidase-4 Inhibitors in Patients with Type 2 Diabetes Mellitus (Diabetes Metab J2015;39:342-7)
Shusuke Yagi, Ken-ichi Aihara, Masataka Sata
Diabetes & Metabolism Journal.2015; 39(5): 446. CrossRef
- Endogenous GLP-1 levels play an important role in determining the efficacy of DPP-IV Inhibitors in both prediabetes and type 2 diabetes
- Increased Risk of Hospitalization for Heart Failure with Newly Prescribed Dipeptidyl Peptidase-4 Inhibitors and Pioglitazone Using the Korean Health Insurance Claims Database
- Sunghwan Suh, Gi Hyeon Seo, Chang Hee Jung, Mee-Kyoung Kim, Sang-Man Jin, You-Cheol Hwang, Byung-Wan Lee, Jae Hyeon Kim
- Diabetes Metab J. 2015;39(3):247-252. Published online April 22, 2015
- DOI: https://doi.org/10.4093/dmj.2015.39.3.247
- 3,996 View
- 35 Download
- 21 Web of Science
- 18 Crossref
-
Abstract
PDFPubReader
Background We assessed the association of dipeptidyl peptidase 4 inhibitors (DPP4i) with hospitalization for heart failure (HF) using the Korean Health Insurance claims database.
Methods We collected data on newly prescribed sitagliptin, vildagliptin, and pioglitazone between January 1, 2009 and December 31, 2012 (mean follow-up of 336.8 days) to 935,519 patients with diabetes (518,614 males and 416,905 females) aged 40 to 79 years (mean age of 59.4 years).
Results During the study, 998 patients were hospitalized for primary HF (115.7 per 100,000 patient-years). The incidence rate of hospitalization for HF was 117.7 per 100,000 per patient-years among patients on pioglitazone, 105.7 for sitagliptin, and 135.8 for vildagliptin. The hospitalization rate for HF was greatest in the first 30 days after starting the medication, which corresponded to a significantly higher incidence at days 0 to 30 compared with days 31 to 360 for all three drugs. The hazard ratios were 1.85 (pioglitazone), 2.00 (sitagliptin), and 1.79 (vildagliptin). The incidence of hospitalization for HF did not differ between the drugs for any time period.
Conclusion This study showed an increase in hospitalization for HF in the initial 30 days of the DPP4i and pioglitazone compared with the subsequent follow-up period. However, the differences between the drugs were not significant.
-
Citations
Citations to this article as recorded by- Cardioprotective effects of dipeptidyl peptidase-4 inhibitors versus sulfonylureas in addition to metformin: A nationwide cohort study of patients with type 2 diabetes
Jui Wang, Hon-Yen Wu, Kuo-Liong Chien
Diabetes & Metabolism.2022; 48(3): 101299. CrossRef - Changing Fields-Diabetes Medications Invading the Cardiovascular Space
Lauren D. Breite, Mackenzie Steck, Brandon Tate Cutshall, Samarth P. Shah, Brandon E. Cave
Current Problems in Cardiology.2021; 46(3): 100736. CrossRef - Cardiovascular Safety and Benefits of Noninsulin Antihyperglycemic Drugs for the Treatment of Type 2 Diabetes Mellitus: Part 2
Srikanth Yandrapalli, Aaqib Malik, Adam Horblitt, Gayatri Pemmasani, Wilbert S. Aronow, William H. Frishman
Cardiology in Review.2020; 28(5): 219. CrossRef - Effects of antidiabetic drugs on left ventricular function/dysfunction: a systematic review and network meta-analysis
Da-Peng Zhang, Li Xu, Le-Feng Wang, Hong-Jiang Wang, Feng Jiang
Cardiovascular Diabetology.2020;[Epub] CrossRef - Dipeptidyl peptidase-4 inhibitor compared with sulfonylurea in combination with metformin: cardiovascular and renal outcomes in a propensity-matched cohort study
Kyoung Jin Kim, Jimi Choi, Juneyoung Lee, Jae Hyun Bae, Jee Hyun An, Hee Young Kim, Hye Jin Yoo, Ji A. Seo, Nan Hee Kim, Kyung Mook Choi, Sei Hyun Baik, Sin Gon Kim, Nam Hoon Kim
Cardiovascular Diabetology.2019;[Epub] CrossRef - Comparative Cardiovascular Risks of Dipeptidyl Peptidase-4 Inhibitors: Analyses of Real-world Data in Korea
Kyoung Hwa Ha, Bongseong Kim, Hae Sol Shin, Jinhee Lee, Hansol Choi, Hyeon Chang Kim, Dae Jung Kim
Korean Circulation Journal.2018; 48(5): 395. CrossRef - Worsening Heart Failure During the Use of DPP-4 Inhibitors
Milton Packer
JACC: Heart Failure.2018; 6(6): 445. CrossRef - Resistance exercise improves cardiac function and mitochondrial efficiency in diabetic rat hearts
Tae Hee Ko, Jubert C. Marquez, Hyoung Kyu Kim, Seung Hun Jeong, SungRyul Lee, Jae Boum Youm, In Sung Song, Dae Yun Seo, Hye Jin Kim, Du Nam Won, Kyoung Im Cho, Mun Gi Choi, Byoung Doo Rhee, Kyung Soo Ko, Nari Kim, Jong Chul Won, Jin Han
Pflügers Archiv - European Journal of Physiology.2018; 470(2): 263. CrossRef - Do DPP-4 Inhibitors Cause Heart Failure Events by Promoting Adrenergically Mediated Cardiotoxicity?
Milton Packer
Circulation Research.2018; 122(7): 928. CrossRef - Comparative safety for cardiovascular outcomes of DPP-4 inhibitors versus glimepiride in patients with type 2 diabetes
Hyouk-Jun Chin, Jin Hyun Nam, Eui-Kyung Lee, Ju-Young Shin
Medicine.2017; 96(25): e7213. CrossRef - Effects of dipeptidyl peptidase-4 inhibitor in insulin-resistant rats with myocardial infarction
Nattayaporn Apaijai, Tharnwimol Inthachai, Suree Lekawanvijit, Siriporn C Chattipakorn, Nipon Chattipakorn
Journal of Endocrinology.2016; 229(3): 245. CrossRef - The current role of thiazolidinediones in diabetes management
Christos V. Rizos, Anastazia Kei, Moses S. Elisaf
Archives of Toxicology.2016; 90(8): 1861. CrossRef - Alternative Interventions to Prevent Oxidative Damage following Ischemia/Reperfusion
Simón Quetzalcoatl Rodríguez-Lara, Ernesto German Cardona-Muñoz, Ernesto Javier Ramírez-Lizardo, Sylvia Elena Totsuka-Sutto, Araceli Castillo-Romero, Teresa Arcelia García-Cobián, Leonel García-Benavides
Oxidative Medicine and Cellular Longevity.2016; 2016: 1. CrossRef - Lessons learned from cardiovascular outcome clinical trials with dipeptidyl peptidase 4 (DPP-4) inhibitors
Teresa Vanessa Fiorentino, Giorgio Sesti
Endocrine.2016; 53(2): 373. CrossRef - Letter: Increased Risk of Hospitalization for Heart Failure with Newly Prescribed Dipeptidyl Peptidase-4 Inhibitors and Pioglitazone Using the Korean Health Insurance Claims Database (Diabetes Metab J2015;39:247-52)
Dae Ho Lee
Diabetes & Metabolism Journal.2015; 39(4): 348. CrossRef - Response: Increased Risk of Hospitalization for Heart Failure with Newly Prescribed Dipeptidyl Peptidase-4 Inhibitors and Pioglitazone Using the Korean Health Insurance Claims Database (Diabetes Metab J2015;39:247-52)
Sunghwan Suh, Gi Hyeon Seo, Chang Hee Jung, Mee-Kyoung Kim, Sang-Man Jin, You-Cheol Hwang, Byung-Wan Lee, Jae Hyeon Kim
Diabetes & Metabolism Journal.2015; 39(4): 350. CrossRef - Cardiovascular, renal and gastrointestinal effects of incretin-based therapies: an acute and 12-week randomised, double-blind, placebo-controlled, mechanistic intervention trial in type 2 diabetes
Mark M Smits, Lennart Tonneijck, Marcel H A Muskiet, Trynke Hoekstra, Mark H H Kramer, Indra C Pieters, Djuna L Cahen, Michaela Diamant, Daniël H van Raalte
BMJ Open.2015; 5(11): e009579. CrossRef - Dipeptidyl Peptidase-4 Inhibitor Alarms: Is Heart Failure Caused by a Class Effect?
Yong-ho Lee
Diabetes & Metabolism Journal.2015; 39(3): 204. CrossRef
- Cardioprotective effects of dipeptidyl peptidase-4 inhibitors versus sulfonylureas in addition to metformin: A nationwide cohort study of patients with type 2 diabetes
 First
First Prev
Prev




