
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Ahead-of print > Article
-
Original ArticleMetabolic Risk/Epidemiology Harnessing Metabolic Indices as a Predictive Tool for Cardiovascular Disease in a Korean Population without Known Major Cardiovascular Event
-
Hyun-Jin Kim1*
 , Byung Sik Kim1*, Yonggu Lee1, Sang Bong Ahn2, Dong Wook Kim3, Jeong-Hun Shin1
, Byung Sik Kim1*, Yonggu Lee1, Sang Bong Ahn2, Dong Wook Kim3, Jeong-Hun Shin1 -
DOI: https://doi.org/10.4093/dmj.2023.0197
Published online: February 1, 2024
- 992 Views
- 25 Download
1Division of Cardiology, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea
2Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Korea
3Division of Endocrinology, Diabetes and Hypertension, Center for Weight Management and Wellness, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
- Corresponding author: Jeong-Hun Shin Division of Cardiology, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, 153 Gyeongchun-ro, Guri 11923, Korea E-mail: cardio.hyapex@gmail.com
- *Hyun-Jin Kim and Byung Sik Kim contributed equally to this study as first authors.
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study evaluated the usefulness of indices for metabolic syndrome, non-alcoholic fatty liver disease (NAFLD), and insulin resistance (IR), as predictive tools for cardiovascular disease in middle-aged Korean adults.
-
Methods
- The prospective data obtained from the Ansan-Ansung cohort database, excluding patients with major adverse cardiac and cerebrovascular events (MACCE). The primary outcome was the incidence of MACCE during the follow-up period.
-
Results
- A total of 9,337 patients were included in the analysis, of whom 1,130 (12.1%) experienced MACCE during a median follow-up period of 15.5 years. The metabolic syndrome severity Z-score, metabolic syndrome severity score, hepatic steatosis index, and NAFLD liver fat score were found to significantly predict MACCE at values above the cut-off point and in the second and third tertiles. Among these indices, the hazard ratios of the metabolic syndrome severity score and metabolic syndrome severity Z-score were the highest after adjusting for confounding factors. The area under the receiver operating characteristic curve (AUC) of the 10-year atherosclerotic cardiovascular disease (ASCVD) score for predicting MACCE was 0.716, and the metabolic syndrome severity Z-score had an AUC of 0.619.
-
Conclusion
- The metabolic syndrome severity score is a highly reliable indicator and was closely associated with the 10-year ASCVD risk score in predicting MACCE in the general population. Given the specific characteristics and limitations of metabolic syndrome severity scores as well as the indices of NAFLD and IR, a more practical scoring system that considers these factors is essential to achieve greater accuracy in forecasting cardiovascular outcomes.
Highlights
- Cardiovascular disease (CVD) is a significant global health issue that warrants widespread attention from clinicians, researchers, and public health officials [1]. Post initial cardiovascular (CV) events, clinical emphasis is commonly placed on intensive therapeutic interventions and secondary prevention strategies, which are aimed at minimizing the risk of event recurrence and mitigating the associated complications [2]. Nevertheless, primary prevention has gained increasing attention, particularly among adults devoid of prior CVD events, and studies have been conducted on the primary prevention and prediction of future CVD [3,4]. Numerous predictors have been validated for their ability to predict long-term CV outcomes in healthy adults, and several scoring systems have been developed accordingly [5-8]. However, a persistent requirement remains for predictive scores that can be readily applied in clinical settings. Important risk factors for predicting the development of CVD include metabolic syndrome, non-alcoholic fatty liver disease (NAFLD), and insulin resistance (IR), each of which has corresponding indices [8-10].
- Metabolic syndrome is strongly associated with an increased risk of CVDs [11,12]. Central obesity, hyperglycemia, hypertension, and dyslipidemia are important metabolic syndrome components that contribute directly to the pathophysiology of CVD [13,14]. These components are included in the criteria for diagnosing metabolic syndrome presented by the Adult Therapy Program III (ATP-III) [13]; however, this definition is limited as it is dichotomous and does not include the concept of severity. To address this limitation, metabolic syndrome severity scores have been proposed for sex and racial/ethnic groups [15,16]. In addition, IR, an important mechanism of metabolic syndrome, increases the risk of CVD by promoting the development of atherosclerosis and endothelial dysfunction [10,17]. NAFLD is also associated with metabolic syndrome and has an important pathophysiological association with IR [18,19]. NAFLD and IR have a significant impact on CV outcomes, and indices reflecting NAFLD and IR have shown to predict CV risks in previous studies [20-28].
- In the present study, we evaluated the usefulness of the indices for metabolic syndrome, NAFLD, and IR as predictive tools for the overall CV risk in middle-aged Korean adults using large-scale cohort data.
INTRODUCTION
- Study population
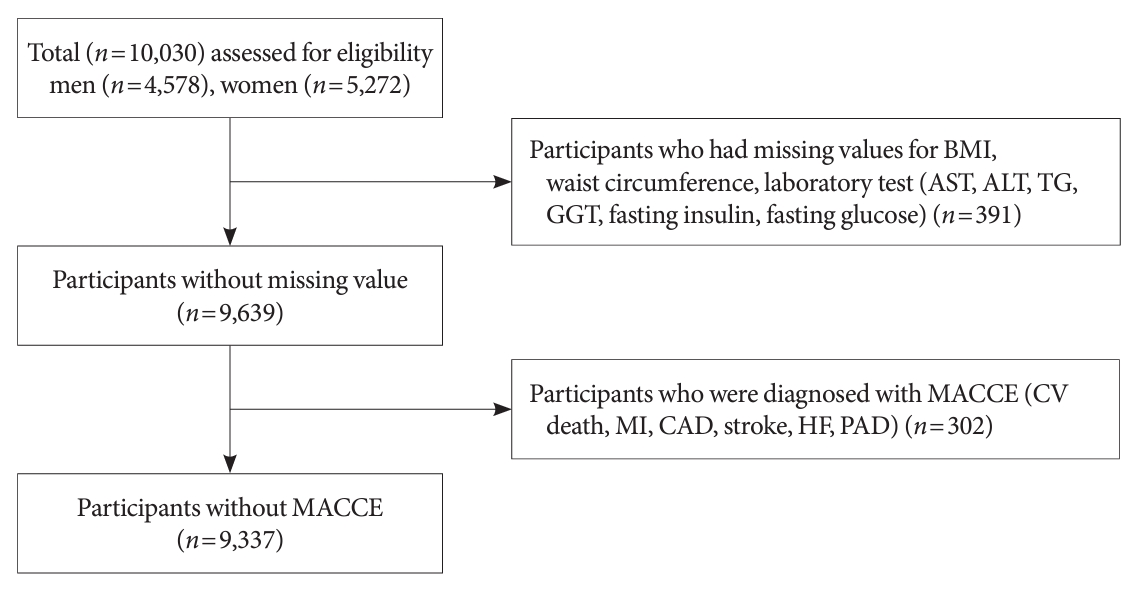
- Study data were obtained from the Ansan-Ansung cohort, a prospective cohort of 10,030 patients. These patients were enrolled between June 2001 and January 2003, aged 40 to 69 years, residing in two cities in Korea, with follow-up data of up to 18 years. This cohort was part of the Korean Genome Epidemiology Study, which aimed to investigate the genetic and environmental etiology of prevalent metabolic and CVD. This study was funded by the Korean National Research Institute of Health, Korean Centers for Disease Control and Prevention, and Ministry of Health and Welfare. Detailed information on the study methods has been reported in a previous publication [29]. In summary, comprehensive health examinations, on-site interviews, and laboratory tests were conducted during each visit to the survey sites. Nine successive assessments adhering to the entire cohort protocol were performed following the baseline assessment with scheduled biennial revisits until 2018.
- Of the 10,030 patients initially enrolled, 9,639 had baseline data available for baseline body mass index (BMI), waist circumference, and laboratory test results (aspartate transaminase [AST], alanine aminotransferase [ALT], triglyceride [TG], gamma-glutamyl transferase [GGT], fasting insulin, and fasting glucose levels). Additionally, among the patients without missing values, 9,337 were not diagnosed with major adverse cardiac and cerebrovascular events (MACCE), including CV death, myocardial infarction (MI), coronary artery disease (CAD), stroke, heart failure (HF), and peripheral artery disease (PAD) (Fig. 1).
- The study protocol adhered to the principals of the Declaration of Helsinki and was reviewed and approved by the Korean National Research Institute of Health and Institutional Review Board of Hanyang University Guri Hospital (IRB No. GURI-2023-06-020). Written informed consent by the patients was waived due to a retrospective nature of our study.
- Data collection
- Patient demographic and clinical characteristics that were extracted included age, sex, BMI, waist circumference, systolic blood pressure (SBP), diastolic blood pressure (DBP), income level, education level, smoking status, alcohol consumption status, physical activity, and medical history of traditional CV risk. In addition, key laboratory findings related to metabolic syndrome, including the estimated glomerular filtration rate and fasting glucose, glycosylated hemoglobin, total cholesterol, TG, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol levels. In order to compute the 10-year risk score for atherosclerotic cardiovascular disease (ASCVD), we also gathered data on the use of antihypertensive therapy [30].
- Study outcomes
- The primary outcome was the incidence of MACCE identified during the follow-up (median, 15.5 years; interquartile range [IQR], 8.3 to 15.8). MACCE were defined as the composite outcome consisting of CV death, MI, CAD, stroke, HF, and PAD. Information on CV related death, MI, CAD, stroke, HF, and PAD during follow-up was obtained. CV related death was defined according to the International Classification of Diseases 10th Revision (ICD-10) codes I20–I82 (including ischemic heart disease, HF, ventricular arrhythmia, pulmonary thromboembolism, and ischemic and hemorrhagic stroke) using the Korean national database for the causes of death registered in the Korean National Statistics Office. Additionally, data were collected using an on-site interview questionnaire to ascertain the incidence of recent MI, CAD, stroke, HF, and PAD during biennial visits. MI was defined as a clinical emergency where the patient recalled experiencing a heart attack episode that necessitated hospitalization or revascularization [31]. CAD was defined as requiring hospitalization or revascularization, excluding any incidents of MI recalled by the patient. Stroke was defined as a clinical emergency where the patient remembered experiencing sudden paralysis, language impairment, or stroke that required hospitalization. HF was defined as any clinical event that the patient recalled requiring hospitalization. PAD was defined as a clinical event that the patient recalled requiring revascularization.
- Metabolic index calculation
- We calculated the indices for metabolic syndrome, including the metabolic syndrome component (0–5), metabolic syndrome severity score, and metabolic syndrome severity Z-score. For NAFLD, we calculated indices including the hepatic steatosis index, fatty liver index, NAFLD liver fat score, and fibrosis-4 index. For IR, we calculated the indices including the TG index, homeostatic model assessment of insulin resistance (HOMA-IR), and metabolic score for IR (METS-IR).
- Components of metabolic syndrome were investigated according to the modified National Cholesterol Education Program, Adult Treatment Panel III (NCEP ATP-III) criteria [13], including the following: (1) abdominal obesity (waist circumference >90 cm for men and >85 cm for women according to the Korean Society of Obesity) [32]; (2) hypertriglyceridemia (serum TG concentration of ≥150 mg/dL); (3) low HDL-C (serum HDL-C <40 mg/dL for men or <50 mg/dL for women); (4) hypertension (SBP >130 mm Hg, DBP >85 mm Hg or treatment with antihypertensive drugs); and (5) high fasting blood glucose (fasting serum glucose >100 mg/dL or previous diagnosis of type 2 diabetes mellitus). The metabolic syndrome severity score considers the weighted contribution of each of the five traditional metabolic syndrome components based on sex- and age-specific criteria; this formulation method has been previously reported in a study [15]. In this study, a formula validated for the Koreans was used [7,33] and the metabolic syndrome severity score was expressed as a Z-score.
- The formula for the hepatic steatosis index, which is a validated index for detecting NAFLD, included 8×ALT/AST ratio+ BMI. Additional points (+2) were given if the patient had diabetes mellitus or was female [34]. The fatty liver index, which consists of BMI, waist circumference, TG, and GGT, is a validated index used in clinical practice for identifying hepatic steatosis [35]. The equation for this index is as follows:
- The NAFLD liver fat score, which is also a validated index for identifying NAFLD was calculated as follows: –2.89+1.18×metabolic syndrome (yes=1/no=0)+0.45×type 2 diabetes mellitus (yes=2/no=0)+0.15×insulin (mU/L)+0.04×AST (U/L)–0.94×AST/ALT. The fibrosis-4 index is a validated index for predicting hepatic fibrosis was calculated by multiplying age with AST level (U/L) [36]. The triglyceride-glucose index (TyG) was calculated as ln (fasting TG×fasting glucose/2) [37]. The HOMA-IR was calculated using the following formula: (fasting insulin [U/L]×fasting glucose [mg/dL])/405 [33]. The METS-IR is a metabolic index that quantifies IR [38] and was calculated using the following formula:
- Statistical analyses
- All categorical data were expressed as frequencies and percentages, and continuous variables were presented as means, standard deviations, medians, and IQR. Univariate analysis followed by multivariate Cox proportional hazards regression analyses was performed to evaluate the MACCE predictability for each metabolic index during follow-up, after adjusting for individual risk factors. Model 1 was adjusted for age (per 1 year) and sex, and model 2 was adjusted for the variables in model 1 as well as BMI, smoking status, alcohol consumption status, physical activity (per 1 METs-hr/wk), income level, and education level. In addition to the adjustments for the variables in model 2, model 3 was further adjusted for medical history, including hypertension, diabetes mellitus, dyslipidemia, and chronic kidney disease. The analysis was conducted by classifying the cutoff values and tertiles 1, 2, and 3 for each index. To determine the optimal cutoff value for each metabolic index in predicting MACCE, we conducted time-dependent receiver operating characteristic (ROC) curve analyses. Additionally, we measured the area under the receiver operating characteristic curve (AUC) to evaluate the predictability of MACCE for metabolic, NAFLD, and IR index, and the DeLong test was used to compare the performance between each index. Furthermore, we evaluated the predictability of MACCE using the established cut-off values for detecting liver fibrosis and hepatic steatosis as suggested in the NAFLD guidelines (hepatic steatosis index, fatty liver index, NAFLD liver fat score, and fibrosis-4 index) [34,39-41]. To evaluate the additional value of combining the metabolic syndrome severity Z-score and other metabolic indices, we analyzed the changes in the additive predictive value when adding other NAFLD or IR indices to the metabolic syndrome severity score with the highest AUC. Statistical significance was set at P<0.05. All analyses were performed using the open-source statistical software R version 4.2.2 (www.R-project.org, accessed on 31 October 2022) and R-studio version 2022.12.0+353 (www.rstudio.com, accessed on 03 December 2022). Various statistical packages, including tableone, timeROC, ggplot2, and rms were used for the analyses.
METHODS
- Baseline characteristics
- A total of 9,337 patients with an average age of 52 years were analyzed, among whom, 4,407 (47.2%) were male patients, and 50% had an income level above the median. The prevalence of previously diagnosed CV risk factors was low; specifically, 955 patients (10.2%) had hypertension, 200 patients (2.1%) had diabetes mellitus, and 33 patients (0.4%) had hyperlipidemia. Table 1 presents the various metabolic indices, including the metabolic syndrome severity Z-score, metabolic syndrome severity score, hepatic steatosis index, fatty liver index, NAFLD liver fat score, fibrosis-4 index, TyG index, HOMA-IR, and METS-IR. The mean metabolic syndrome severity score was 0.575±1.007, and the mean metabolic syndrome severity Z-score was –0.000 00003030413±0.9999465. Additionally, 2,448 (26.2%) patients had three or more components of the metabolic syndrome, with 744 (8.0%) having four components and 181 (1.9%) having five components.
- MACCE predictability for each metabolic index
- The median follow-up period was 15.5 years (IQR, 8.3 to 15.8). Of the 9,337 patients, 1,130 (12.1%) experienced MACCE during the follow-up period, with 623 (6.7%) experiencing MACCE specifically during the 10-year follow-up period. Table 2 presents the quantitative evaluation of the 10-year MACCE risk by categorizing each metabolic index into cutoff and tertile values. All indices revealed significant hazard ratios (HRs) for predicting MACCE at values greater than the cutoff point. However, the results of the HRs varied after adjusting for each variable in models 1, 2, and 3. The metabolic syndrome severity Z-score, metabolic syndrome severity score, hepatic steatosis index, and NAFLD liver fat score significantly predicted MACCE at values greater than the cutoff point and in the second and third tertiles. Among them, the metabolic syndrome severity score and metabolic syndrome severity Z-score had the highest HRs (HR, 1.794; 95% confidence interval [CI], 1.507 to 2.135 [model 3]; HR, 1.730; 95% CI, 1.463 to 2.044 [model 3]). In addition, the HRs significantly increased in predicting MACCE as the number of metabolic syndrome components increased. In particular, even with one metabolic component, MACCE showed a 37% increase after 10 years (HR, 1.563; 95% CI, 1.108 to 1.705). Moreover, when the metabolic components increased to four and five, the HRs for model 3 were 1.981 (95% CI, 11.536 to 2.554) and 2.546 (95% CI, 1.771 to 3.661) respectively, indicating an association with the number of components. However, the fibrosis-4 index did not significantly predict MACCE, even when the index value exceeded the tertile after adjusting for multiple variables. Furthermore, the fatty liver index, TyG index, HOMA-IR, and METS-IR scores were only able to significantly predict MACCE when the score increased above the tertile after adjusting for multiple variables. Building on the analysis, further evaluation of MACCE predictability was conducted using the established cut-off values for detecting liver fibrosis and hepatic steatosis, as suggested in the NAFLD guidelines. This additional analysis, presented in Supplementary Table 1, includes the hepatic steatosis index, fatty liver index, NAFLD liver fat score, and fibrosis-4 index. While the results varied across the indices and models, a general trend emerged where higher index values were associated with increased HRs for MACCE. However, as the result of analysis using the cut-off value derived from the timeROC curve and tertile value, the fibrosis-4 index did not significantly predict MACCE even if it exceeded the cut-off value presented in the guidelines for fibrosis detection.
- Fig. 2 presents the time-dependent ROC curve for MACCE and the MACCE predictive power of each index. The 10-year ASCVD score was observed to be the most effective index for predicting MACCE over 10 years in a general population, with an AUC value of 0.716 and a sensitivity and specificity of 0.768 and 0.546, respectively. The metabolic syndrome severity Z-score had an AUC value of 0.619, a cut-off value of –0.046, and a sensitivity and specificity of 0.661 and 0.522, respectively, for predicting MACCE over 10 years. The metabolic syndrome severity Z-score revealed an AUC value close to that of the 10-year ASCVD score for predicting MACCE. Other scores or indices related to NAFLD, in the order of fibrosis-4 index (AUC, 0.594), NAFLD liver fat score (AUC, 0.588), fatty liver index (AUC, 0.585), and hepatic steatosis index (AUC, 0.528), also exhibited AUC levels <0.6 for MACCE prediction (Fig. 2). Additionally, indices related to IR, in the order of TyG index, METS-IR, and HOMA-IR, revealed an AUC of <0.6. The 10-year ASCVD score and metabolic syndrome severity Z-score were significantly different from all other indices, except for the fibrosis-4 index, when comparing the AUC values of each index. A comparison of the indices is presented in Supplementary Table 2. Similarly, the predictive power of MACCE for each metabolic index demonstrated a consistent pattern in time-dependent ROC curves throughout 14 and 16 years of follow-up period (Supplementary Fig. 1).
- Additional value of combining the metabolic syndrome severity Z-score and other metabolic indices
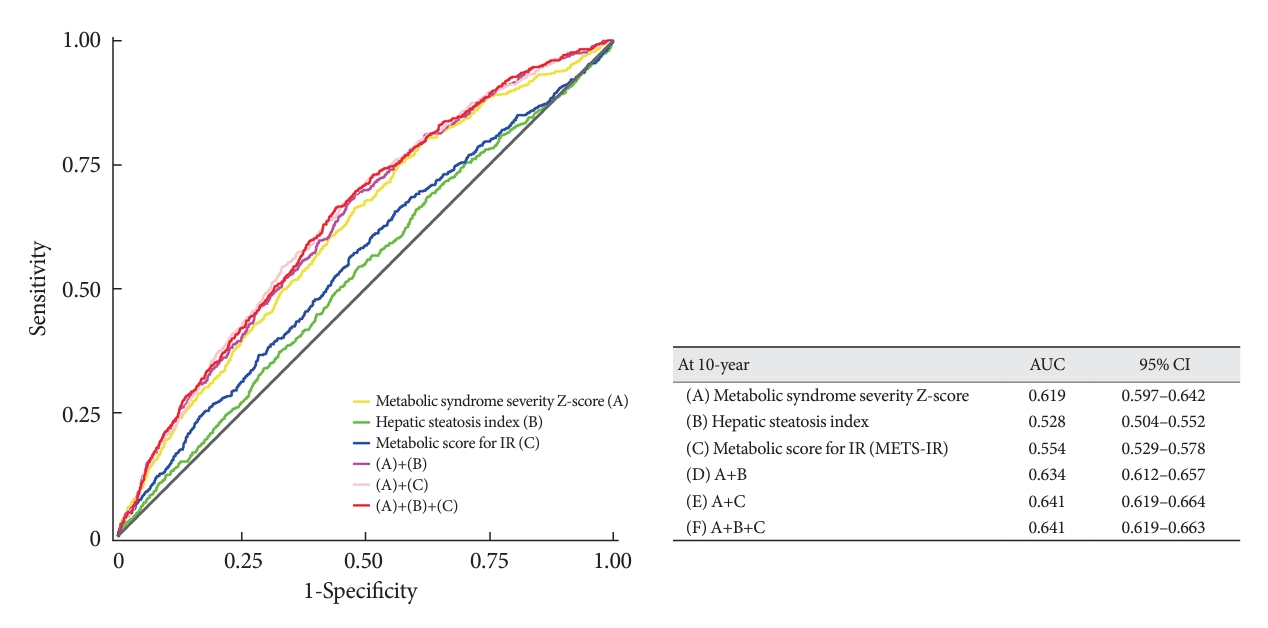
- Among the metabolic indices, both the hepatic steatosis index and METS-IR revealed a significant increase in AUC for predicting MACCE when added to the metabolic syndrome severity Z-score, indicating an additive value (Fig. 3). Combining the metabolic syndrome severity Z-score and hepatic steatosis index resulted in an AUC of 0.634, which was significantly higher than the AUC of metabolic syndrome severity Z-score alone (P<0.001). Combining the metabolic syndrome severity Z-score and METS-IR resulted in an AUC value of 0.641 (P<0.001). Combining the metabolic syndrome severity Zscore, hepatic steatosis index, and METS-IR resulted in an AUC of 0.641, which revealed significantly better MACCE predictability than that obtained from all other combinations, except for the combination of the metabolic syndrome severity Z-score and METS-IR (P values are presented in Supplementary Table 3).
RESULTS
- Among the Korean population aged 40 to 69 years, with unknown MACCE, 2,448 (26.2%) experienced metabolic syndrome according to the modified NCEP ATP-III criteria, of which 1,130 (12.1%) experienced MACCE during the follow-up period and 623 (6.7%) experienced MACCE specifically during the 10-year follow-up period. Metabolic syndrome severity score and Z-score were strongly associated with risk of MACCE occurrence. The hepatic steatosis index and NAFLD liver fat score also demonstrated an independent association with the risk of MACCE occurrence; however, other NAFLD and IR indices varied depending on whether they were in the second or third tertile range, after adjusting for confounding factors. Additionally, when comparing the predictive value of the 10-year ASCVD risk score and the indices for metabolic syndrome, NAFLD, and IR indices for MACCE over 10 years, the 10-year ASCVD risk score demonstrated superior predictive power compared to those of the other indices. The metabolic severity Z-score, with an AUC of 0.619, was observed to have the closest predictive power to the 10-year ASCVD risk score compared to that of the other predictors. Among the NAFLD indices, fibrosis-4 index, demonstrated the highest predictive power for MACCE, followed by the IR index. Additionally, the TyG index demonstrated the highest predictive power among the IR indices, although its AUC was <0.6. Moreover, the combination of the hepatic steatosis index and METS-IR with the metabolic syndrome severity Z-score demonstrated an additional value in predicting MACCE. This combination demonstrated significantly improved predictability for MACCE compared to that of the other combinations.
- Metabolic syndrome is an important health concern in the general population, and its prevalence is increasing worldwide [1,11,42]. The 2021 Metabolic Syndrome Fact Sheet in Korea highlights a dramatic increase in the prevalence of metabolic syndrome since 2015, with approximately 23% of adults aged ≥19 years and approximately 50% of adults aged ≥65 years reported to have developed metabolic syndrome [43]. The diagnostic criteria for metabolic syndrome have traditionally been based on the ATP-III criteria, and metabolic syndrome is identified only when abnormalities beyond the cut-offs for the three yes-or-no components are present [13]. To provide personalized treatment for individuals with metabolic syndrome, continuous variables are needed to evaluate CV outcomes in patients with metabolic syndrome. Moreover, considering the challenge of applying uniform criteria across different races, metabolic syndrome severity score formulas have been proposed to classify patients based on their sex and race [15,44]. Recently, a metabolic syndrome severity score has been developed in Korea using data from the Korean National Health and Nutrition Examination Survey, which incorporates severity scores developed in the Western population [7,33]. These metabolic syndrome severity scores can be an independent predictors of CVD in Korean middle-aged adults [7]. In our study, we determined that metabolic syndrome indices, including the metabolic syndrome severity score and metabolic syndrome components, were useful in predicting the 10-year MACCE. As the metabolic syndrome diagnostic criteria used in our study were based on the Asian criteria (modified NCEP ATP-III criteria) [13], our findings aligned with those of previous studies demonstrating a strong association between metabolic syndrome severity score and the risk of developing coronary heart disease, MI, and stroke [7,45]. According to the results of our study, which categorized metabolic syndrome indices into cut-off values and tertiles to predict MACCE using HRs, we observed significant association between the metabolic syndrome severity Z-score, metabolic syndrome severity score, and metabolic syndrome components with an increased risk of MACCE, as their values exceeded the cut-off or upper tertile even after adjusting for prognostic variables. These results highlight the predictive power of these metabolic syndrome-related indices for MACCE over a 10-year period. Notably, even with the presence of one metabolic syndrome component, the risk of MACCE increased by 37% over a 10-year period. Moreover, the risk of MACCE increases with an increase in the number of metabolic syndrome components. Interestingly, the predictive power of the dichotomous criterion for metabolic syndrome component was not inferior to that of the metabolic syndrome severity Z-score, with an AUC of 0.613 and a sensitivity and specificity of 0.655 and 0.515, respectively, suggesting the need to investigate and manage individual risk factors for metabolic syndrome.
- The 10-year ASCVD score is a well-known predictor of adverse CV events. In our study, it was the most useful indicator for predicting MACCE events (AUC, 0.716) in the general population, with a sensitivity and specificity of 0.768 and 0.546, respectively. Nonetheless, the metabolic syndrome severity score exhibited the closest predictive power to the 10-year ASCVD score, and no previous research has conducted a comparative study of these two scores for adverse CV outcomes. Due to the complexity of the 10-year ASCVD risk score calculation, which includes variables such as sex, age, total cholesterol, HDL-C, SBP, use of antihypertensive therapy, diabetes mellitus, and smoking history, its application is challenging in busy clinical settings. In contrast, the metabolic syndrome severity score and number of metabolic syndrome components may provide a straightforward screening tool for predicting long-term CV outcomes in patients with relatively low-risk conditions. These findings underscore the significance of the metabolic syndrome severity score as a valuable tool for assessing and evaluating metabolic syndrome.
- NAFLD and IR are involved in the pathophysiology of metabolic syndrome. They share common underlying process and are important factors in the development of adverse CV outcomes [9,46]. Several indices for assessing NAFLD and IR include the hepatic steatosis index, fatty liver index, NAFLD liver fat score, fibrosis-4 index, TyG index, HOMA-IR, and METS-IR. Previous studies have demonstrated that these indices, reflecting NAFLD and IR, can predict CV risk [18-27]. However, our study revealed that all these indices had lower power than metabolic syndrome indices in predicting 10-year MACCE, with some indices demonstrating significant predictive ability only when the values exceeded the upper tertile for predicted the 10-year MACCE. The hepatic steatosis index and NAFLD liver fat score also demonstrated statistically significant HRs; however, these values were lower than those of the metabolic severity score. The fatty liver index, TyG index, HOMA-IR, and METS-IR demonstrated independent predictive significance only in the upper tertile group, and their HR values were smaller than those of the metabolic severity score. Additionally, when evaluating the additional value of the combination of the metabolic syndrome severity Z-score and other metabolic indices, the predictive power for MACCE significantly increased by incorporating the hepatic steatosis index and METS-IR to the metabolic syndrome severity Z-score. Combining NAFLD, IR indices and metabolic syndrome severity Z-score could serve as a screening tool for predicting CV outcomes in the general population. Furthermore, evaluation of their additive value could offer substantial background information for the development of a more precise risk-scoring system, thereby contributing to the advancement in clinical practice.
- Each index for metabolic syndrome, NAFLD, and IR has its own characteristics and limitations. In specific patient populations including those with hypertension, diabetes mellitus, dyslipidemia, obesity, and conditions like NAFLD and IR, the metabolic syndrome severity score may exhibit superior predictive ability compared to those of other metabolic syndrome indicators. Nevertheless, the predictive accuracy is lower when compared to validated scoring systems, such as the ASCVD score. This result suggested that despite the growing interest in NAFLD and IR as emerging indices, their application as standalone predictors in the actual clinical setting for predicting CVD could have limitations. However, these indices hold significance in stratifying high-risk groups for primary prevention. Therefore, further research is necessary to develop a more realistic scoring system and predictive tools using these indices, as well as to explore the role of these metabolic indices in stratifying high-risk groups for CVD in populations with hypertension, diabetes mellitus, dyslipidemia, and obesity.
- This study has several limitations. First, our analysis focused on the predictive power of various metabolic, NAFLD, and IR indices for a 10-year MACCE, even though the Ansan-Ansung cohort data encompasses a median follow-up period of 15.5 years (IQR, 8.3 to 15.8). This was done because it allows a direct comparison with the 10-year ASCVD risk score. Moreover, previous studies did not conduct a comparative analysis between different indices of metabolic syndromes, IR, and fatty liver for predicting CVD; thus justifying the adjustment of the time period for analysis. Additionally, we presented a time-dependent ROC curve for MACCE of each index at 14- and 16-year follow-ups in the Supplementary Fig. 1, except for the 10-year ASCVD risk score. Second, this study had certain limitations due to the inadequate consideration of potential confounding factors, which could have affected the relationship between metabolic indices and MACCE. Furthermore, the observed associations may have been influenced by factors, such as genetic predisposition, socioeconomic status, dietary habits, and medication use, which were not sufficiently accounted for in the present study. Third, although the NAFLD indices—hepatic steatosis index, fatty liver index, NAFLD liver fat score, and fibrosis-4 index—have validated cut-off values in the guidelines for detecting liver fibrosis and hepatic steatosis, our study employed a different approach for predicting MACCE. We utilized the cut-off value and the tertile value derived from the timeROC curve analysis. This approach acknowledges that the optimal cut-off values of the same index may vary depending on the predicted outcomes. Finally, the number of CV outcomes, except CV mortality, may have been underestimated due to exclusion from subsequent assessments, which is a limitation of the cohort data. However, the utilization of the Korean national database to determine the cardiac-related cause of death ensured that the number of patient who died was accurately reflected in this study.
- In conclusion, the metabolic syndrome severity score and its components, along with certain indices for NAFLD and IR, demonstrated predictive value for long-term CV events in a middle-aged Korean population. Although the 10-year ASCVD risk score demonstrated the highest predictive power, the metabolic syndrome severity score exhibited the closest predictive ability among the metabolic indices assessed. Moreover, incorporating the representative indices of NAFLD and IR into the metabolic syndrome severity score may create a more realistic scoring system that considers the distinct characteristics and limitations of each index.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 2.
Supplementary Table 3.
Supplementary Fig. 1.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: H.J.K., B.S.K., J.H.S.
Acquisition, analysis, or interpretation of data: H.J.K., B.S.K., Y.L.
Drafting the work or revising: H.J.K., B.S.K., S.B.A., D.W.K., J.H.S.
Final approval of the manuscript: H.J.K., B.S.K., Y.L., S.B.A., D.W.K., J.H.S.
-
FUNDING
None
NOTES
-
Acknowledgements
- None


Values are presented as mean±standard deviation or number (%).
IQR, interquartile range; METS, metabolic score; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NAFLD, nonalcoholic fatty liver disease; TyG, triglyceride glucose index; HOMA-IR, homeostatic model assessment for insulin resistance; METS-IR, metabolic score for insulin resistance.
| Variable |
Hazard ratios (95% confidence interval) |
|||
|---|---|---|---|---|
| Unadjusted | Model 1a | Model 2b | Model 3c | |
| Metabolic syndrome component | ||||
| ≥3 | 1.938 (1.720–2.183) | 1.624 (1.438–1.834) | 1.463 (1.274–1.679) | 1.309 (1.135–1.510) |
| Metabolic syndrome component | ||||
| 0 | Reference | Reference | Reference | Reference |
| 1 | 1.662 (1.349–2.047) | 1.436 (1.165–1.770) | 1.397 (1.125–1.735) | 1.374 (1.108–1.705) |
| 2 | 2.088 (1.697–2.569) | 1.654 (1.342–2.038) | 1.610 (1.289–2.011) | 1.563 (1.259–1.940) |
| 3 | 2.733 (2.212–3.376) | 2.093 (1.690–2.591) | 1.935 (1.531–2.446) | 1.819 (1.453–2.276) |
| 4 | 3.520 (2.783–4.451) | 2.441 (1.923–3.098) | 2.236 (1.710–2.924) | 1.981 (1.536–2.554) |
| 5 | 4.617 (3.282–6.496) | 3.319 (2.351–4.686) | 3.090 (2.132–4.479) | 2.546 (1.771–3.660) |
| Metabolic syndrome severity Z-score | ||||
| Cut-off value of score | ||||
| >–0.046 | 1.974 (1.748–2.230) | 1.645 (1.455–1.861) | 1.539 (1.330–1.781) | 1.489 (1.306–1.698) |
| Tertiles of score | ||||
| Tertile 1 (–2.612 to –0.473) | Reference | Reference | Reference | Reference |
| Tertile 2 (–0.473 to 0.363) | 1.577 (1.338–1.859) | 1.363 (1.156–1.608) | 1.376 (1.160–1.633) | 1.321 (1.113–1.569) |
| Tertile 3 (0.363 to 9.359) | 2.451 (2.102–2.858) | 1.931 (1.653–2.256) | 2.000 (1.703–2.348) | 1.730 (1.463–2.044) |
| Metabolic syndrome severity score | ||||
| Cut-off value of score | ||||
| >0.997 | 1.990 (1.770–2.237) | 1.816 (1.599–2.063) | 1.695 (1.461–1.967) | 1.513 (1.298–1.764) |
| Tertiles of score | ||||
| Tertile 1 (–2.306 to 0.116) | Reference | Reference | Reference | Reference |
| Tertile 2 (0.116 to 0.922) | 1.234 (1.049–1.451) | 1.261 (1.068–1.487) | 1.343 (1.131–1.593) | 1.298 (1.093–1.541) |
| Tertile 3 (0.922 to 10.309) | 2.166 (1.870–2.510) | 2.008 (1.708–2.359) | 2.083 (1.762–2.463) | 1.794 (1.507–2.135) |
| Hepatic steatosis index | ||||
| Cut-off value of score | ||||
| >31.295 | 1.217 (1.075–1.377) | 1.416 (1.247–1.607) | 1.292 (1.087–1.537) | 1.204 (1.011–1.434) |
| Tertiles of score | ||||
| Tertile 1 (17.185 to 30.778) | Reference | Reference | Reference | Reference |
| Tertile 2 (30.778 to 34.700) | 1.078 (0.929–1.251) | 1.248 (1.074–1.451) | 1.296 (1.109–1.514) | 1.199 (1.025–1.403) |
| Tertile 3 (34.700 to 55.771) | 1.294 (1.121–1.494) | 1.603 (1.383–1.857) | 1.702 (1.461–1.983) | 1.464 (1.250–1.715) |
| Fatty liver index | ||||
| Cut-off value of score | ||||
| >30.421 | 1.647 (1.465–1.852) | 1.531 (1.360–1.723) | 1.454 (1.245–1.698) | 1.421 (1.253–1.611) |
| Tertiles of score | ||||
| Tertile 1 (0.600 to 15.390) | Reference | Reference | Reference | Reference |
| Tertile 2 (15.390 to 40.114) | 1.405 (1.202–1.643) | 1.235 (1.056–1.445) | 1.240 (1.054–1.458) | 1.167 (0.991–1.374) |
| Tertile 3 (40.114 to 99.117) | 1.878 (1.619–2.179) | 1.681 (1.447–1.953) | 1.752 (1.500–2.045) | 1.523 (1.298–1.787) |
| NAFLD liver fat score | ||||
| Cut-off value of score | ||||
| >1.576 | 1.657 (1.472–1.864) | 1.531 (1.360–1.725) | 1.443 (1.240–1.681) | 1.393 (1.227–1.582) |
| Tertiles of score | ||||
| Tertile 1 (–5.032 to –0.806) | Reference | Reference | Reference | Reference |
| Tertile 2 (–0.806 to 3.585) | 1.424 (1.217–1.667) | 1.265 (1.080–1.482) | 1.246 (1.058–1.468) | 1.183 (1.003–1.395) |
| Tertile 3 (3.585 to 38.000) | 1.982 (1.707–2.300) | 1.780 (1.531–2.069) | 1.835 (1.572–2.143) | 1.588 (1.352–1.865) |
| Fibrosis-4 index | ||||
| Cut-off value of score | ||||
| >1.164 | 1.765 (1.571–1.984) | 0.980 (0.860–1.117) | 1.047 (0.915–1.198) | 1.073 (0.938–1.228) |
| Tertiles of score | ||||
| Tertile 1 (0.281 to 0.856) | Reference | Reference | Reference | Reference |
| Tertile 2 (0.856 to 1.193) | 1.257 (1.073–1.472) | 0.850 (0.721–1.002) | 0.869 (0.733–1.030) | 0.872 (0.735–1.033) |
| Tertile 3 (1.193 to 50.836) | 2.022 (1.747–2.341) | 0.888 (0.748–1.053) | 0.968 (0.811–1.154) | 0.996 (0.835–1.187) |
| TyG index | ||||
| Cut-off value of score | ||||
| >8.716 | 1.499 (1.334–1.685) | 1.384 (1.231–1.556) | 1.292 (1.139–1.465) | 1.212 (1.067–1.376) |
| Tertiles of score | ||||
| Tertile 1 (7.148 to 8.370) | Reference | Reference | Reference | Reference |
| Tertile 2 (8.370 to 8.878) | 1.418 (1.215–1.655) | 1.211 (1.037–1.414) | 1.121 (0.954–1.319) | 1.099 (0.935–1.293) |
| Tertile 3 (8.878 to 11.716) | 1.781 (1.535–2.065) | 1.545 (1.330–1.793) | 1.399 (1.192–1.641) | 1.288 (1.095–1.514) |
| HOMA-IR | ||||
| Cut-off value of score | ||||
| >1.566 | 1.370 (1.218–1.540) | 1.462 (1.299–1.645) | 1.377 (1.213–1.563) | 1.306 (1.150–1.484) |
| Tertiles of score | ||||
| Tertile 1 (0.018 to 1.235) | Reference | Reference | Reference | Reference |
| Tertile 2 (1.235 to 1.923) | 0.981 (0.844–1.139) | 1.071 (0.921–1.244) | 1.085 (0.929–1.268) | 1.079 (0.924–1.261) |
| Tertile 3 (1.923 to 59.107) | 1.331 (1.156–1.532) | 1.445 (1.253–1.666) | 1.365 (1.170–1.593) | 1.273 (1.089–1.487) |
| METS-IR | ||||
| Cut-off value of score | ||||
| >35.311 | 1.440 (1.275–1.627) | 1.462 (1.294–1.652) | 1.425 (1.198–1.695) | 1.404 (1.232–1.600) |
| Tertiles of score | ||||
| Tertile 1 (19.605 to 33.507) | Reference | Reference | Reference | Reference |
| Tertile 2 (33.507 to 39.308) | 1.126 (0.967–1.311) | 1.176 (1.009–1.370) | 1.243 (1.060–1.456) | 1.173 (0.999–1.376) |
| Tertile 3 (39.308 to 71.416) | 1.520 (1.317–1.755) | 1.595 (1.381–1.841) | 1.707 (1.470–1.983) | 1.487 (1.274–1.736) |
MACCE, major adverse cardiovascular and cerebrovascular events; NAFLD, nonalcoholic fatty liver disease; TyG, triglyceride-glucose index; HOMA-IR, homeostatic model assessment of insulin resistance; METS-IR, metabolic score for insulin resistance.
a Adjusted for age and sex,
b Adjusted for age, sex, body mass index, smoking status, alcohol consumption status, physical activity (per 1METs-hour/week), income level, and education level,
c Adjusted for age, sex, smoking status, alcohol consumption status, physical activity (per 1METs-hour/week), income level, education level, hypertension, diabetes mellitus, dyslipidemia, and chronic kidney disease.
- 1. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 Study. J Am Coll Cardiol 2020;76:2982-3021.PubMedPMC
- 2. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016;37:2315-81.PubMedPMC
- 3. Takahara M, Katakami N, Hayashino Y, Nishimura R, Suzuki H, Shimano H, et al. Different impacts of metabolic profiles on future risk of cardiovascular disease between diabetes with and without established cardiovascular disease: the Japan diabetes complication and its prevention prospective study 7 (JDCP study 7). Acta Diabetol 2022;59:57-65.ArticlePubMedPDF
- 4. SCORE2 working group and ESC cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J 2021;42:2439-54.PubMedPMC
- 5. D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 2008;117:743-53.ArticlePubMed
- 6. Conroy RM, Pyorala K, Fitzgerald AP, Sans S, Menotti A, De Backer G, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 2003;24:987-1003.ArticlePubMed
- 7. Jang YN, Lee JH, Moon JS, Kang DR, Park SY, Cho J, et al. Metabolic syndrome severity score for predicting cardiovascular events: a nationwide population-based study from Korea. Diabetes Metab J 2021;45:569-77.ArticlePubMedPMCPDF
- 8. Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019;140:e596-646.PubMedPMC
- 9. Kasper P, Martin A, Lang S, Kutting F, Goeser T, Demir M, et al. NAFLD and cardiovascular diseases: a clinical review. Clin Res Cardiol 2021;110:921-37.ArticlePubMedPDF
- 10. Lee SH, Park SY, Choi CS. Insulin resistance: from mechanisms to therapeutic strategies. Diabetes Metab J 2022;46:15-37.ArticlePubMedPDF
- 11. Chae J, Seo MY, Kim SH, Park MJ. Trends and risk factors of metabolic syndrome among Korean adolescents, 2007 to 2018. Diabetes Metab J 2021;45:880-9.ArticlePubMedPMCPDF
- 12. Grundy SM, Hansen B, Smith SC Jr, Cleeman JI, Kahn RA; American Heart Association, et al. Clinical management of metabolic syndrome: report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Circulation 2004;109:551-6.ArticlePubMed
- 13. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005;112:2735-52.ArticlePubMed
- 14. Shin D, Choi J, Lee HY. Suboptimal control status of young hypertensive population. Clin Hypertens 2023;29:13.ArticlePubMedPMCPDF
- 15. Gurka MJ, Lilly CL, Oliver MN, DeBoer MD. An examination of sex and racial/ethnic differences in the metabolic syndrome among adults: a confirmatory factor analysis and a resulting continuous severity score. Metabolism 2014;63:218-25.ArticlePubMed
- 16. DeBoer MD, Gurka MJ. Clinical utility of metabolic syndrome severity scores: considerations for practitioners. Diabetes Metab Syndr Obes 2017;10:65-72.ArticlePubMedPMCPDF
- 17. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep 2018;20:12.ArticlePubMedPMCPDF
- 18. Bugianesi E, McCullough AJ, Marchesini G. Insulin resistance: a metabolic pathway to chronic liver disease. Hepatology 2005;42:987-1000.ArticlePubMed
- 19. Fujii H, Kawada N; Japan Study Group of Nafld Jsg-Nafld. The role of insulin resistance and diabetes in nonalcoholic fatty liver disease. Int J Mol Sci 2020;21:3863.ArticlePubMedPMC
- 20. Kim JH, Moon JS, Byun SJ, Lee JH, Kang DR, Sung KC, et al. Fatty liver index and development of cardiovascular disease in Koreans without pre-existing myocardial infarction and ischemic stroke: a large population-based study. Cardiovasc Diabetol 2020;19:51.ArticlePubMedPMCPDF
- 21. Duell PB, Welty FK, Miller M, Chait A, Hammond G, Ahmad Z, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol 2022;42:e168-85.ArticlePubMed
- 22. Lee CO, Li HL, Tsoi MF, Cheung CL, Cheung BM. Association between the liver fat score (LFS) and cardiovascular diseases in the national health and nutrition examination survey 1999-2016. Ann Med 2021;53:1065-73.ArticlePubMed
- 23. Vieira Barbosa J, Milligan S, Frick A, Broestl J, Younossi Z, Afdhal N, et al. Fibrosis-4 index can independently predict major adverse cardiovascular events in nonalcoholic fatty liver disease. Am J Gastroenterol 2022;117:453-61.ArticlePubMed
- 24. Han E, Lee YH, Lee JS, Lee HW, Kim BK, Park JY, et al. Fibrotic burden determines cardiovascular risk among subjects with metabolic dysfunction-associated fatty liver disease. Gut Liver 2022;16:786-97.ArticlePubMedPMC
- 25. Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol 2022;21:68.ArticlePubMedPMCPDF
- 26. Gast KB, Tjeerdema N, Stijnen T, Smit JW, Dekkers OM. Insulin resistance and risk of incident cardiovascular events in adults without diabetes: meta-analysis. PLoS One 2012;7:e52036.ArticlePubMedPMC
- 27. Yoon J, Jung D, Lee Y, Park B. The metabolic score for insulin resistance (METS-IR) as a predictor of incident ischemic heart disease: a longitudinal study among Korean without diabetes. J Pers Med 2021;11:742.ArticlePubMedPMC
- 28. Shim SY, Jung SJ, Kim SU, Kim HC. Ideal cardiovascular health metrics and the risk of nonalcoholic fatty liver disease in Korean adults. Clin Hypertens 2023;29:3.ArticlePubMedPMCPDF
- 29. Kim Y, Han BG; KoGES group. Cohort profile: the Korean Genome and Epidemiology Study (KoGES) Consortium. Int J Epidemiol 2017;46:e20.ArticlePubMed
- 30. Andrus B, Lacaille D. 2013 ACC/AHA guideline on the assessment of cardiovascular risk. J Am Coll Cardiol 2014;63(25 Pt A):2886.Article
- 31. Kim BS, Lee Y, Park JK, Lim YH, Shin JH. Association of the estimated pulse wave velocity with cardio-vascular disease outcomes among men and women aged 40-69 years in the Korean population: an 18-year follow-up report on the Ansung-Ansan Cohort in the Korean Genome Environment Study. J Pers Med 2022;12:1611.ArticlePubMedPMC
- 32. Kim BY, Kang SM, Kang JH, Kang SY, Kim KK, Kim KB, et al. 2020 Korean Society for the Study of Obesity guidelines for the management of obesity in Korea. J Obes Metab Syndr 2021;30:81-92.ArticlePubMedPMC
- 33. Huh JH, Lee JH, Moon JS, Sung KC, Kim JY, Kang DR. Metabolic syndrome severity score in Korean adults: analysis of the 2010-2015 Korea National Health and Nutrition Examination Survey. J Korean Med Sci 2019;34:e48.ArticlePubMedPMCPDF
- 34. Lee JH, Kim D, Kim HJ, Lee CH, Yang JI, Kim W, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis 2010;42:503-8.ArticlePubMed
- 35. Bedogni G, Bellentani S, Miglioli L, Masutti F, Passalacqua M, Castiglione A, et al. The fatty liver index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol 2006;6:33.ArticlePubMedPMCPDF
- 36. Sterling RK, Lissen E, Clumeck N, Sola R, Correa MC, Montaner J, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006;43:1317-25.ArticlePubMed
- 37. Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, Martinez-Abundis E, Ramos-Zavala MG, Hernandez-Gonzalez SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab 2010;95:3347-51.ArticlePubMed
- 38. Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D, Viveros-Ruiz T, Cruz-Bautista I, Romo-Romo A, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol 2018;178:533-44.ArticlePubMed
- 39. Kang SH, Lee HW, Yoo JJ, Cho Y, Kim SU, Lee TH, et al. KASL clinical practice guidelines: management of nonalcoholic fatty liver disease. Clin Mol Hepatol 2021;27:363-401.ArticlePubMedPMCPDF
- 40. Shah AG, Lydecker A, Murray K, Tetri BN, Contos MJ, Sanyal AJ, et al. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2009;7:1104-12.ArticlePubMedPMC
- 41. Kotronen A, Peltonen M, Hakkarainen A, Sevastianova K, Bergholm R, Johansson LM, et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009;137:865-72.ArticlePubMed
- 42. Shi TH, Wang B, Natarajan S. The influence of metabolic syndrome in predicting mortality risk among US adults: importance of metabolic syndrome even in adults with normal weight. Prev Chronic Dis 2020;17:E36.ArticlePubMedPMC
- 43. Huh JH, Kang DR, Kim JY, Koh KK; on behalf of the Taskforce Team of the Metabolic Syndrome Fact Sheet of the Korean Society of Cardiometabolic Syndrome. Metabolic syndrome fact sheet 2021: executive report. Cardiometab Syndr J 2021;1:125-34.ArticlePDF
- 44. Gurka MJ, Ice CL, Sun SS, Deboer MD. A confirmatory factor analysis of the metabolic syndrome in adolescents: an examination of sex and racial/ethnic differences. Cardiovasc Diabetol 2012;11:128.ArticlePubMedPMC
- 45. Guo Y, Musani SK, Sims M, Pearson TA, DeBoer MD, Gurka MJ. Assessing the added predictive ability of a metabolic syndrome severity score in predicting incident cardiovascular disease and type 2 diabetes: the Atherosclerosis Risk in Communities Study and Jackson Heart Study. Diabetol Metab Syndr 2018;10:42.ArticlePubMedPMCPDF
- 46. Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuniga FA. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol 2018;17:122.ArticlePubMedPMCPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite






