- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 47(5); 2023 > Article
-
ReviewComplications Dyslipidemia in Patients with Chronic Kidney Disease: An Updated Overview
-
Sang Heon Suh
 , Soo Wan Kim
, Soo Wan Kim -
Diabetes & Metabolism Journal 2023;47(5):612-629.
DOI: https://doi.org/10.4093/dmj.2023.0067
Published online: July 24, 2023
Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
- Corresponding author: Soo Wan Kim Department of Internal Medicine, Chonnam National University Medical School, 42 Jebong-ro, Dong-gu, Gwangju 61469, Korea Email: skimw@chonnam.ac.kr
Copyright © 2023 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Dyslipidemia is a potentially modifiable cardiovascular risk factor. Whereas the recommendations for the treatment target of dyslipidemia in the general population are being more and more rigorous, the 2013 Kidney Disease: Improving Global Outcomes clinical practice guideline for lipid management in chronic kidney disease (CKD) presented a relatively conservative approach with respect to the indication of lipid lowering therapy and therapeutic monitoring among the patients with CKD. This may be largely attributed to the lack of high-quality evidence derived from CKD population, among whom the overall feature of dyslipidemia is considerably distinctive to that of general population. In this review article, we cover the characteristic features of dyslipidemia and impact of dyslipidemia on cardiovascular outcomes in patients with CKD. We also review the current evidence on lipid lowering therapy to modify the risk of cardiovascular events in this population. We finally discuss the association between dyslipidemia and CKD progression and the potential strategy to delay the progression of CKD in relation to lipid lowering therapy.
- Dyslipidemia is a potentially modifiable cardiovascular risk factor. As high low-density lipoprotein cholesterol (LDL-C) levels [1-4] as well as high triglycerides (TG) [5] and low high-density lipoprotein cholesterol (HDL-C) [6,7] levels are significantly associated with the risk of cardiovascular events in the general population, trials have aimed to correct lipid profiles in patients with dyslipidemia for the primary and secondary preventions of cardiovascular events. On the basis of currently available data, most clinical guidelines on dyslipidemia primarily target to lower LDL-C levels [8-10].
- Whereas the recommendations for the treatment target of dyslipidemia in the general population are being more and more rigorous, the 2013 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline for lipid management in chronic kidney disease (CKD) presented a relatively conservative approach with respect to the indication of lipid lowering therapy and therapeutic monitoring among the patients with CKD [11]. This may be largely attributed to the lack of high-quality evidence derived from CKD population, among whom the overall feature of dyslipidemia is considerably distinctive to that of general population. On top of the characteristic alterations in the lipid profile among the patients with CKD [2-4,12], the impact of dyslipidemia on cardiovascular outcomes seems to be substantially modified by deteriorating kidney function [13,14]. Most importantly, accumulating evidence strongly suggests the association between dyslipidemia and the risk of CKD progression [15-17].
- This review article covers the characteristic features of dyslipidemia and the impact of dyslipidemia on cardiovascular outcomes in patients with CKD. We also review the current evidence on lipid lowering therapy to modify the risk of cardiovascular events in this population. We finally discuss the association between dyslipidemia and CKD progression and the potential strategy to delay the progression of CKD in relation to lipid lowering therapy.
INTRODUCTION
- Dyslipidemia is a common complication of CKD [16,18,19], although the prevalence of dyslipidemia in Korean patients with CKD has not been precisely surveyed yet. As the Korean Society of Lipid and Atherosclerosis reported that, in 2018, the prevalence of dyslipidemia was 45.6% in men and 31.3% in women among the general population [20], the prevalence in CKD population is supposed to be higher than that. Uremic condition leads to various alterations in the quantity and quality of circulating lipoproteins. Typically, dyslipidemia in patients with CKD is featured with low HDL-C levels and high TG levels, as well as the other compositional changes in the lipoproteins [2-4,12]. In the overall, such changes are believed to promote atherosclerosis, contributing to high cardiovascular burden in patients with CKD [2-4].
- Structural changes in LDL-C
- Cholesterol derived from apolipoprotein B (ApoB), such as low-density lipoprotein (LDL), accumulates in the subintimal space of vascular beds, and is critical to initiate the subsequent atherosclerotic processes (Fig. 1) [21,22]. Therefore, lowering LDL-C levels has been a major strategy to reduce cardiovascular risk in the general population as well as in patients with CKD [1-4]. It is important to note that; however, LDL and total cholesterol levels are not dramatically increased among the patients with CKD [2,3,23,24]. Rather, a structural change is remarkable in LDL-C, with predominance of small dense LDL particles [25]. Due to their increased capacity to penetrate the arterial intima and increased susceptibility to oxidation, small dense LDL particles are known to be more atherogenic than the other LDL subfractions [22,26,27].
- Defective metabolism in HDL-C
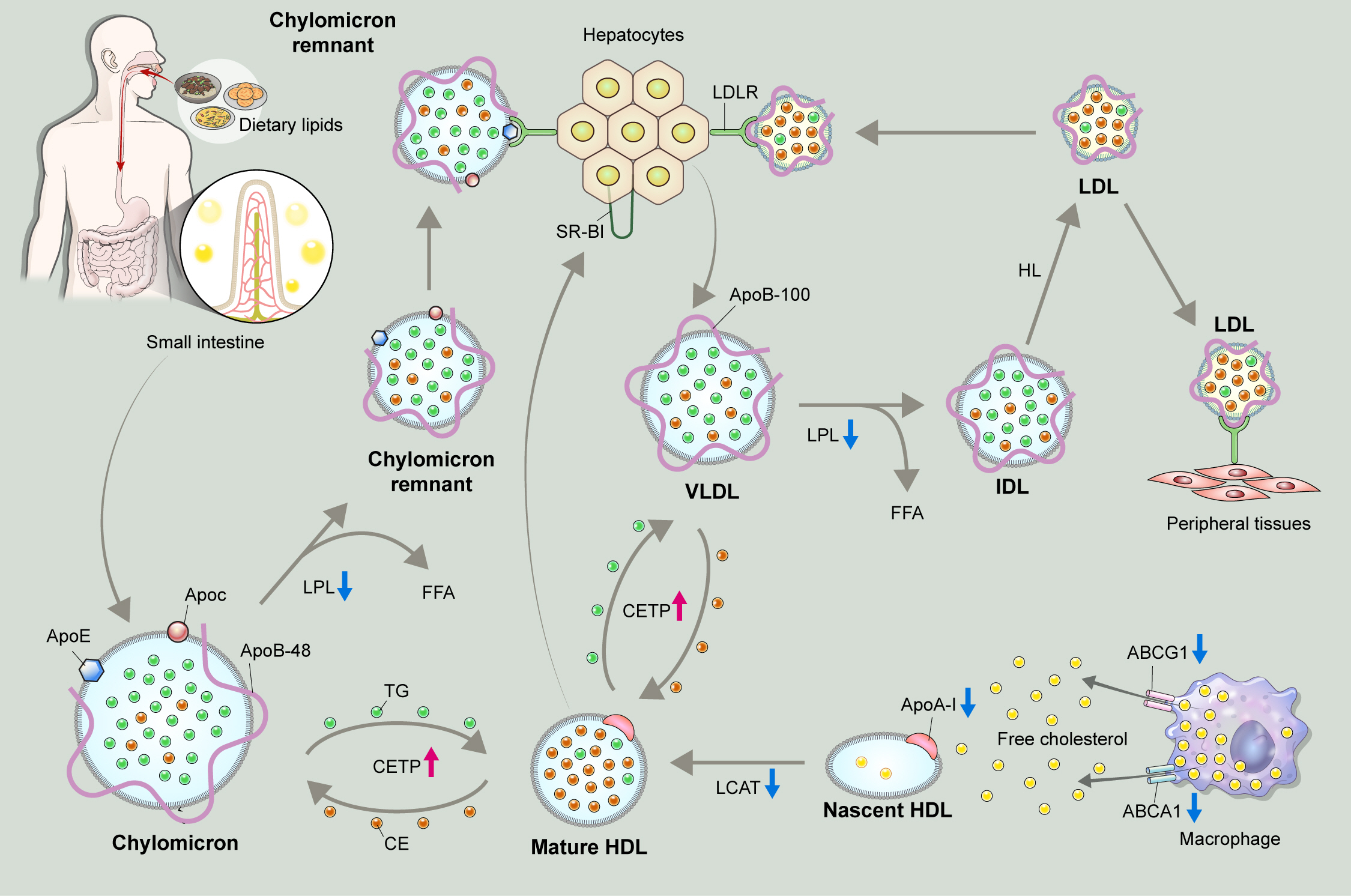
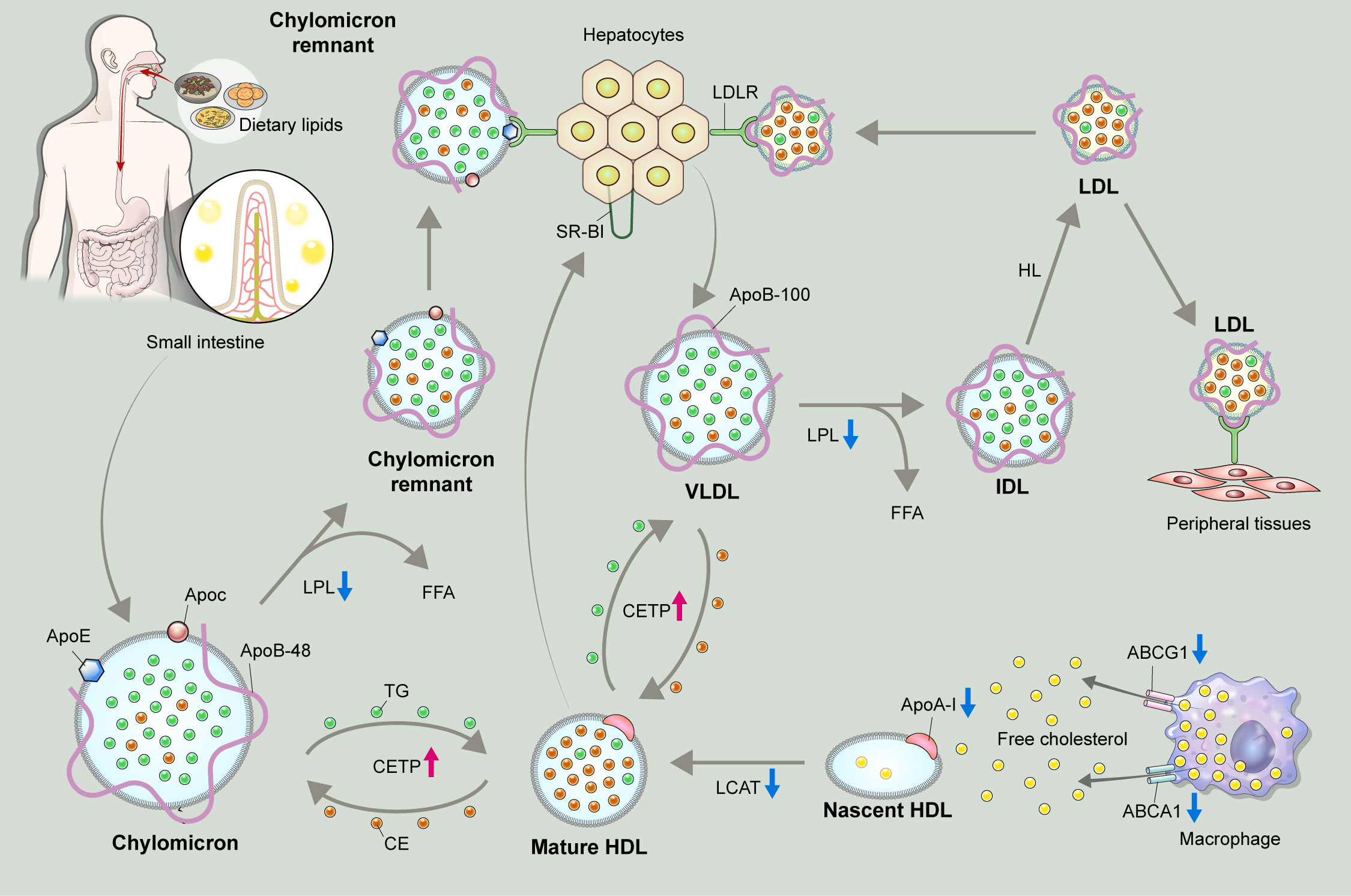
- HDL-C is involved in the process of reverse cholesterol transport to clear excess cholesterol particles from peripheral tissue, and has been known to be protective against atherosclerotic processes (Fig. 2) [23,28]. The synthesis and maturation of high-density lipoprotein (HDL) is deranged in multiple aspect under uremic conditions. First, the hepatic synthesis of apolipoprotein A-I (ApoA-I), a major apolipoprotein of HDL is significantly reduced [23,29]. Second, the efflux of free cholesterol particles from tissue macrophages via ATP-binding cassette (ABC) transporters, such as ABCA1 and ABCR1, is interrupted due to the downregulation of the transporters, resulting in the defective maturation of nascent HDL [23,30]. Third, both plasma levels and activity of lecithin-cholesterol acyltransferase (LCAT), which converts free cholesterol to cholesteryl ester (CE) to form mature HDL-C, is reduced [31,32]. Furthermore, the activity of cholesteryl ester transfer protein (CETP) is enhanced in patients with CKD [23,33]. As, CETP medicates exchange of TG and CE between HDL and ApoB lipoproteins, enhanced CETP activity leads to reduction in the HDL-C levels. As a net effect, the plasma levels and the maturation of HDL-C are significantly impaired in patients with CKD, contributing to the suboptimal anti-oxidative and anti-inflammatory function of HDL particles under uremic condition [34,35].
- Delayed catabolism of TG-rich lipoproteins
- As TG is a main component of TG-rich lipoproteins, such as very low-density lipoprotein (VLDL) and chylomicrons (CM), its plasma level reflects circulating quantity of TG-rich lipoproteins [36,37]. Circulating TG-rich lipoproteins bind to endothelial cells in vascular beds, triggering local inflammation characterized by upregulation of integrins, generation of reactive oxygen species, cytokine production, and complement activation [38,39]. Hypertriglyceridemia is an early finding of CKD, and is one of the most common features of dyslipidemia in patients with CKD [40]. Elevation in plasma TG levels is primarily attributed to the delayed catabolism of TG-rich lipoproteins. TG packed in VLDL or CM is hydrolyzed to free fatty acid by lipoprotein lipase (LPL) (Fig. 3) [41]. The expression of LPL is downregulated under uremic condition [42]. Moreover, the activity of LPL is also reduced in patients with CKD, because of parathyroid hormone-induced insulin resistance [43] and upregulation of its competitive inhibitor, such as apolipoprotein C-III (ApoC-III) [44]. Clearance of circulating VLDL particles is also defective under uremia due to the downregulation of VLDL receptors in adipocytes and myocytes [45]. Defective metabolism of major lipoproteins in CKD is summarized in Fig. 4.
- Elevated circulating level of lipoprotein(a)
- Lipoprotein(a) (Lp(a)) is a unique lipoprotein that has a LDL-like core with a single ApoB molecule linked by disulfide bonds to apolipoprotin(a) (Apo(a)) [46]. Lp(a) particles bind to extracellular matrix and are highly atherogenic [47], such that the rise in Lp(a) levels increased the risk of atherosclerotic cardiovascular disease (ASCVD) in the general population [48]. It is problematic that the use of statins is not effective to lower Lp(a) levels [49], and, rather increase its circulating levels [50], although the precise mechanisms should be further investigated. Elevated circulating level of Lp(a) (usually defined as serum level over 10 to 30 mg/dL) is independently associated with the risk of adverse cardiovascular events also in patients with CKD [1,51]. Moreover, the elevation in Lp(a) levels has been repeatedly reported even with mild reduction in estimated glomerular filtration rate (eGFR) [52,53]. The suggested mechanisms for the elevation in the circulating Lp(a) levels involve the decreased clearance via kidney, based on the finding of a drop in Lp(a) levels in the renal vein compared to the ascending aorta [54]. An animal study in rats demonstrated that injected Lp(a) accumulated in the renal tubules as well as urinary excretion of Apo(a) fragments [55]. On the other hand, some studies suggest that the liver is the major organ for the clearance of Lp(a) [56]. Further studies are warranted to reveal the precise reason for the elevation in the circulating Lp(a) levels.
FEATURES OF DYSLIPIDEMIA IN CKD
- The association between dyslipidemia and the risk of cardiovascular event is best illustrated in the elevation of LDL-C among the general population. In the general population, every 40 mg/dL increase in LDL-C increases the risk of cardiovascular events by 40% [57]. Among the patients on maintenance dialysis, however, this graded relation is largely blunted, or is inversed at below the average level, which is so called ‘reverse epidemiology’ [13,14]. A possible hypothesis for the inverse association between LDL-C levels and all-cause mortality among the patients with end-stage renal disease (ESRD) is that uremic milieu, independently of LDL-C levels, promotes the deaths due to nonatherosclerotic cardiovascular events, such as heart failure and sudden cardiac death, rather that ASCVD [58-60].
- Indeed, the patients with ESRD are usually exposed to pathological conditions including anemia, hypervolemia, hypertension and disturbances in bone and mineral metabolism [61-63]. All of these are likely to contribute to the development of uremic cardiomyopathy that is a specific pattern of myocardial fibrosis among the patients with CKD and ESRD [63-65]. A post hoc analysis of the Study of Heart and Renal Protection (SHARP) also supports the hypothesis [66]. The SHARP trial enrolled 9,270 patients with CKD, among which 3,015 patients were on dialysis, and reported a positive association of LDL-C with the risk of major vascular events (hazard ratio [HR], 1.14; 95% confidence interval [CI], 1.06 to 1.22 per 0.6 mmol/L increase in LDL-C), but a negative association with nonatherosclerotic events, including heart failure and arrhythmia (HR, 0.90; 95% CI, 0.83 to 0.97 per 0.6 mmol/L increase in LDL-C) [66].
- Albeit high HDL-C levels are protective against cardiovascular events in the general population [6,7], clinical trials failed to demonstrate that pharmacologic interventions, such as niacin, reduce the risk of cardiovascular events [67-70]. While low HDL-C levels are common in patients with CKD, the association between HDL-C and the risk of cardiovascular events is somewhat complicated. In the analyses of the patients with CKD, the association of HDL-C with the risk of cardiovascular events is not any more statistically significant after adjustment for the confounding factors [71,72]. Rather, some studies reported that all-cause mortality is increased with very low or very high levels of HDL-C among the patients with ESRD, probably due to the changes in the composition of lipoproteins related to uremia [73]. It seems like that inflammation modifies the association between HDL-C and cardiovascular risk in patients with nondialysis CKD, as HDL-C levels were inversely associated with the risk of cardiovascular events in the absence of inflammation, whereas HLD-C levels were positively associated with the risk in the presence of inflammation (i.e., high-sensitivity C-reactive protein level ≥1.0 mg/L) [74]. A study reported that non-HDL-C might be a better index for the predication of cardiovascular risk in patients with nondialysis CKD, as a simple, positive correlation was observed between non-HDL-C and the risk of cardiovascular events, even after adjustment for high-sensitivity C-reactive protein level [18].
- It has been elucidated that hyperglyceridemia also imposes a residual cardiovascular burden in the general population [5]. Hypertriglyceridemia is also a common phenotype of dyslipidemia in patients with CKD, especially in those with diabetes and those on peritoneal dialysis [75,76]. A recent cohort study of 2.9 million United States veterans including patients with CKD at stages 3a to 5 or ESRD reported a linear association between TG levels and the risk of hospitalization for ASCVD, although the association was attenuated with worsening CKD stages [77]. Interestingly, the study also reported an inverse relationship between TG levels and the risk of non-ASCVD, where elevated TG levels are associated with lower risk, regardless of CKD stages [77].
DYSLIPIDEMIA AND CARDIOVASCULAR OUTCOMES IN RELATION TO CKD
- Stains
- Statins are 3-hydroxy-3-methylglutaryl-coenzyem A reductase inhibitors that primarily target to lower LDL-C levels [78]. Their benefits for the primary [79,80] and secondary [81,82] prevention of cardiovascular events have been robustly established in the general population. Yet, the results from randomized controlled trials (RCTs) including the patients with CKD requires sophisticated precautions to interpret the efficacy of statins to reduce cardiovascular risk.
- The Die Deutsche Diabetes Dialyse Studie (4D) trial [83] enrolled 1,255 patients with diabetes who initiated hemodialysis within 2 years, who were randomly assigned to atorvastatin 20 mg daily or placebo. LDL-C levels in those treated with atorvastatin were reduced by 49 mg/dL in average from a median baseline level of 121 mg/dL at 4 weeks, and were persistently maintained for the duration of the study. Despite the significant reduction in LDL-C levels, the incidence of the primary composite outcome (death from cardiac causes, fatal stroke, nonfatal myocardial infarction, and nonfatal stroke) was not significantly different between the two groups during a median of 4 years of follow-up (HR, 0.92; 95% CI, 0.77 to 1.10).
- The A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Haemodialysis: An Assessment of Survival and Cardiovascular Events (AURORA) trial [84] enrolled 2,776 ESRD patients who had been on hemodialysis for at least 3 months and who were not treated with statins at the baseline. The participants were randomly assigned to rosuvastatin 10 mg daily or placebo. Treatment with rosuvastain decreased LDL-C levels by 43% from a mean baseline level of 100 mg/dL, and decreased C-reactive protein levels as well, although these improvements in the surrogate markers were not accompanied by the reduction in the incidence of primary composite outcome, which is defined as a nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes (HR, 0.96; 95% CI, 0.84 to 1.11).
- It should be noticed that the participants in 4D and AURORA trials were not selected by LDL-C levels [83,84]. A post hoc analysis of 4D trial demonstrated atorvastatin significantly reduces the risk of fatal and nonfatal cardiac events and death from any cause among the participants with pretreatment LDL-C level >145 mg/dL [85], although interpretation of secondary analyses from RCTs needs caution, because of reduced statistical power, increased variance, and the play of chance [86,87]. Moreover, cardiovascular events were less specifically defined in 4D and AURORA trials, which also included the deaths from nonatherosclerotic cardiac events [83,84].
- The SHARP trial [88] enrolled 9,270 patients with CKD or ESRD to evaluate the efficacy of simvastatin plus ezetimibe for the primary prevention of major atherosclerotic event, which was defined as nonfatal myocardial infarction or coronary death, nonhemorrhagic stroke, or arterial revascularization excluding dialysis access procedures. Contrary to the previous two RCTs, 6,247 patients were nondialysis-dependent, and the remaining 3,023 patients were on maintenance dialysis, where overall 75% of the study participants had CKD stages at 4 to 5 or ESRD. The patients were initially randomly assigned to simvastatin plus ezetimibe, simvastatin alone, and placebo groups. Those who were initially assigned to simvastatin alone group received simvastatin plus ezetimibe 1 year after the initiation of the study. Treatment with simvastatin plus ezetimibe yielded an average reduction of LDL-C level by 33 mg/dL. During a median follow-up of 4.9 years, simvastatin plus ezetimibe significantly reduced the risk of major atherosclerotic events (HR, 0.83; 95% CI, 0.74 to 0.94).
- Meta analyses report a clear risk reduction of cardiovascular event by statin therapy in the general population [89], while the effect is substantially modified in patients with CKD [60,90], indicating that the risk reduction of cardiovascular event per reduction in LDL-C levels is attenuated as CKD progresses [90], with no detectable benefits in patients with ESRD conferred by statin therapy [60]. This is also consistently well-demonstrated in the individual RCTs, such as 4D, AURORA, and SHARP trials [83,84,88]. The possible explanations have been suggested. First, a considerable portion of cardiovascular events in patients with ESRD may be due to nonatherosclerotic pathology, such as sudden cardiac death and heart failure [58,59], which could not be essentially aimed by statin therapy. Second, the number of the participants with ESRD might have been not sufficient to demonstrate the statistical significance, compared to the other studies with positive results, such as the Scandinavian Simvastatin Survival Study (n=4,444) [79] and the West of Scotland Coronary Prevention Study (n=6,595) [91]. Third, the effect of statins on the elevation of circulating Lp(a) levels may be maximized in patients with ESRD. It is known that statins tend to increase circulating Lp(a) levels to contribute to the residual cardiovascular burden in the general population [92]. As Lp(a) is cleared via kidney, its level is usually highest in patients with ESRD [48]. Therefore, we cannot exclude the possibility that the effect of statins on the elevation of circulating Lp(a) levels may be maximized in patients on dialysis to null the cardioprotective effect by LDL-C lowering, although the hypothesis remains to be further validated.
- Based on the observations from RCTs, the 2013 KDIGO clinical practice guideline for lipid management in CKD [11] and the others [8-10] commonly do not recommend the initiation of statin therapy in patient on dialysis who are not being treated with statins, while the continuation of statin therapy is acceptable for those who are already on statin therapy. In this context, a retrospective analysis of United States veterans initiating dialysis (n=14,298) reported that the continuation of statin therapy was associated with reduced all-cause mortality (HR, 0.72; 95% CI, 0.66 to 0.79) and cardiovascular mortality (HR, 0.82; 95% CI, 0.69 to 0.96) [93]. The administration of statins among the indicated patients with nondialysis CKD is a widely accepted concept throughout current guidelines, while varying targets for LDL-C levels are still on the controversy (Table 1) [8-11,94].
- Statin therapy in kidney transplant recipients to lower LDLC levels is also usually advocated by the current guidelines [9-11], although the class of recommendation is not strong. The Assessment of Lescol in Renal Transplantation (ALERT) study [95] enrolled 2,102 kidney transplant recipients receiving cyclosporine-based immunosuppression with stable graft function, and randomly assigned the participants to fluvastatin 40 mg daily or placebo. During a median follow-up of 5.1 years, LDL-C levels were decreased by 40 mg/dL in the intervention group, with a significant reduction in nonfatal myocardial infarction and cardiac deaths, although the incidence of the primary composite outcome of major cardiac events (defined as cardiac death, nonfatal myocardial infarction, or coronary intervention) was not significantly different between the two groups. The benefits of fluvastatin therapy in the initial study in terms of nonfatal myocardial infarction and cardiac death were sustained, even when all of the participants were offered open-label, long-term high dose of fluvastatin (80 mg) during a complex extension study period for a total of 6.7 years [96]. The results from the RCTs of statin therapy in patients with CKD are summarized in Table 2.
- Fibrates
- Fibrates stimulate peroxisome proliferator-activated receptor alpha (PPARα) to effectively reduce TG levels and elevate HDL levels. RCTs have demonstrated the efficacy of fibrates in the primary and secondary prevention of cardiovascular events in the general population. For instance, in Helsinki Heart Study, treatment of gemfibrozil in asymptomatic men with non-HDL-C ≥200 mg/dL significantly increased HDL-C and reduced total and LDL-C, and TG levels. Importantly, during the follow-up period of 5 years, the incidence of coronary heart disease was reduced by 34% in the gemfibrozil group compared to the placebo group. Considering the common feature of dyslipidemia in patients with CKD, fibrates should be an attractive therapeutic option. Currently, there are no RCTs available that directed included the patients with CKD to examine the cardioprotective effects of fibrate therapy. A meta-analysis, however, identified a total of 16,869 participants with CKD from RCTs that assess the effects of fibrate therapy compared with placebo in people with CKD, and reported that fibrates improve lipid profiles and prevent cardiovascular events in the subjects with eGFR <60 mL/min/1.73 m2 as well as in the subjects with eGFR <30 mL/min/1.73 m2 [97]. Whereas the use of fibrates is associated with increased serum creatinine levels especially among those with eGFR <30 mL/min/1.73 m2, a recent meta-analysis reported that initial increase in creatinine remains relatively constant afterwards, suggesting the use of fibrates does not significantly accelerate the progression of CKD [98]. Although 2013 KDIGO clinical practice guideline for lipid management in CKD recommends therapeutic lifestyle modification in the adults with CKD and hypertriglyceridemia, primarily due to lack of no published RCTs in CKD populations and too few participants with CKD included in previous trials to provide reliable information, it should be reminded that the recommendation do not entirely exclude the beneficial effect of fibrates in selected individuals with CKD.
- Omega-3 fatty acid
- Omega-3 fatty acid (eicosapenatnoic acid [EPA] and docosahexenoic acid) at pharmacologic dose (2 to 4 g/day) reduce TG levels by up to 45%, with little effect on LDL-C or HDL-C levels, in the general population as well as in patients with CKD, although the action mechanism is poorly understood. The effect of omega-3 fatty acid added on statin therapy for the reduction of residual cardiovascular burden is controversial. The Reduction of Cardiovascular Events with Icosapent Ethyl–Intervention Trial (REDUCE-IT) was designed to address the efficacy of icosapent ethyl (IPE), a highly purified EPA ethyl ester on the risk of cardiovascular events among patients with elevated TG levels despite the use of statins. The primary endpoint was the composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, coronary revascularization, or unstable angina requiring hospitalization. The participants were followed for a median of 4.9 years. The result demonstrated that the risk of cardiovascular event is significantly decreased with medication of IPE 2 g twice daily (HR, 0.71; 95% CI, 0.59 to 0.85) [99]. In a post hoc analysis of REDUCE-IT study, where the participants (n=8,179) were categorized by eGFR into eGFR ≥90 mL/min/1.73 m2, eGFR 60 to <90 mL/min/1.73 m2 and eGFR <60 mL/min/1.73 m2 (the median baseline eGFR 75 mL/min/1.73 m2 [range, 17 to 123]), the benefits of IPE on primary and key secondary composite endpoints were consistently observed across the eGFR categories, albeit the effect was less clear among the patients with eGFR <45 mL/min/1.73 m2 [100]. The Long-Term Outcomes Study to Assess Statin Residual Risk with Epanova in High Cardiovascular Risk Patients with Hypertriglyceridemia (STRENGTH) trial reported a contrary result [101]. The STRENGTH trial intended to test the efficacy of a carboxylic acid formulation of EPA (omega-3 CA) in patients with CKD in statin-treated participants (n=13,078) with high cardiovascular risk, hypertriglyceridemia, and low levels of HDL-C. The participants were randomly assigned to receive 4 g/day of omega-3 CA or corn oil, in addition to statins. The primary endpoint was the composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, coronary revascularization, or unstable angina requiring hospitalization. During the median follow-up duration of 42 months, the addition of omega-3 CA, compared with corn oil, resulted in no significant difference in a composite outcome of cardiovascular events (HR, 0.99; 95% CI, 0.90 to 1.09). Moreover, a high rate of new-onset atrial fibrillation was observed with the use of omega-3 CA than corn oil (2.2% vs. 1.3%, P<0.001). Currently there is no plausible explanation for the obviously discrepant results from the two RCTs. Although the Food and Drug Administration approved the use of IPE for the prevention of cardiovascular events based on the results from REDUCE-IT study, and the 2019 ESC/EAS guidelines for the management of dyslipidemias recommend to consider the use of IPE in high-risk patients with hypertriglyceridemia despite statin treatment [102], molecular targets of IPE have not been identified yet. Moreover, the cardiovascular risk reduction observed in REDUCE-IT study was not associated with the magnitude of the reduction in TG levels. The precise action mechanism of IPE should be further elucidated.
- Proprotein convertase subtilisin/kexin type 9 inhibitors
- Binding of proprotein convertase subtilisin/kexin type 9 (PCSK9), a secreted serine protease, to ectodomain of low-density lipoprotein receptor (LDLR) on the surface of hepatocytes promotes lysosomal degradation of LDLR, which in turn reduces the clearance of LDL particles from the circulation, resulting in increased LDL-C levels [103,104]. Monoclonal antibodies targeeting PCSK9, such as alirocumab [105-115] and evolocumab [116-120], are currently available as PCSK9 inhibitors, which effectively lower LDL-C levels even among those who were already on statin therapy, and reduced the risk of adverse cardiovascular events. Contrary to statins, the data on PCSK9 inhibitors in patients with CKD is very limited, because RCTs on PCSK9 inhibitors mostly excluded the patients with eGFR <20 to 30 mL/min/1.73 m2 [105-120]. An analysis of the pooled data from eight phase III the Effect of Alirocumab on the Occurrence of Cardiovascular Events in Patients Who Have Recently Experienced an Acute Coronary Syndrome (ODYSSEY) trials included a total of 4,629 patients with hypercholesterolemia, among whom 467 patients had CKD stage 3, which demonstrated that alirocumab consistently lowers LDL-C levels regardless of impaired renal function, although the patients with eGFR <30 mL/min/1.73 m2 were excluded from the analysis [121]. In a post hoc analysis of the Further cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER) trial, 8,077 patients with preserved kidney function (eGFR ≥90 mL/min/1.73 m2), 15,034 with CKD stage 2 (eGFR 60 to <90 mL/min/1.73 m2), and 4,443 with eGFR <60 mL/min/1.73 m2 were included to analyze the efficacy and safety of evolocumab in patients with CKD. Similar to the result from ODYSSEY trials, the efficacy of lowering LDL-C levels safety of evolocumab vs. placebo were consistent across subgroups defined by different eGFR range ([HR, 0.82; 95% CI, 0.71 to 0.94] in patients with preserved renal function; [HR, 0.85; 95% CI, 0.77 to 0.94] in patients with stage 2 CKD; [HR, 0.89; 95% CI, 0.76 to 1.05] in patients with stage 3 CKD; P for interaction=0.77) [122]. The patients with eGFR <30 mL/min/1.73 m2 were excluded from FOURIER trial. Whereas the potent lipid lowering effect of PCSK9 inhibitors should be attractive, it remains to be further evaluated whether PCSK9 inhibitors can be safely administered and ultimately reduce the risk of adverse cardiovascular events in patients with advanced CKD (eGFR <20 to 30 mL/min/1.73 m2).
CARDIOVASCULAR RISK MODIFICATION BY TARGETING DYSLIPIDEMIA IN CKD
- Although the management of dyslipidemia primarily targets the reduction of the risk for cardiovascular events, the parameters related to kidney function, such as eGFR decline, proteinuria, and initiation of dialysis, are also the clinical outcomes of particular importance in patients with CKD. Given that the kidney is a highly vascularized organ, and that the overall effect of dyslipidemia should be also deleterious in the vascular bed of the kidney, it is readily expectable that adverse renal outcomes might be associated with dyslipidemia in patients with CKD. In this regard, mounting evidence suggests the association between various abnormalities in the lipid profile and CKD progression, which are mostly derived from cohort studies.
- For instance, elevated LDL-C levels seem to be associated with the risk of CKD progression [15]. In the analysis of 1,886 patients with CKD stages 1 to pre-dialysis 5, the risk of composite kidney event (defined as a composite of 50% decline in eGFR during follow-up or onset of end-stage kidney disease including initiation of dialysis or kidney transplantation) was highest in those with LDL-C ≥130 mg/dL (HR, 2.05; 95% CI, 1.19 to 3.56) compared to those with LDL-C <70 mg/dL during the median follow-up of 5.2 years [15]. Hypertriglyceridemia is also associated with the progression of CKD [16]. In a prospective cohort study of the patients with nondialysis CKD at stage 1 to 5, a total of 2,158 participants were divided into the quartile by serum TG levels, where, compared to the 1st quartile (TG <92 mg/dL), the risk of CKD progression was significantly higher (HR, 1.43; 95% CI, 1.05 to 1.96) in the 4th quartile (TG ≥194 mg/dL) during the median follow-up of 6.9 years [16]. The association of low HDL-C levels with the risk of CKD progression is somewhat complicated. In a study that evaluated the association between serum HDL-C levels and the risk of CKD progression in 2,168 patients with nondialysis CKD, the risk of CKD progression was lowest in the reference group with with HDL-C levels of 50 to 59 mg/dL, whereas both low (<30 mg/dL: HR, 2.21; 95% CI, 1.30 to 3.77) or high (≥60 mg/dL: HR, 2.05; 95% CI, 1.30 to 3.77) HDL-C levels were associated with significantly increased risk of CKD progression during a median follow-up of 3.1 years, suggesting a U-shaped association between serum HDL-C levels and adverse renal outcomes [17]. A study from the same cohort that investigated the association between non-HDL-C levels and the risk of CKD progression also reported a U-shaped association [19].
- Accordingly, reports focused at improving the renal outcomes by correction of dyslipidemia followed, although the most were the results from the secondary analysis of RCTs or cohort studies. The effect of lowering LDL-C by statins on the delaying of CKD progression is disappointing. In the post hoc analysis of SHARP trial that included a total of 6,245 patients with nondialysis CKD, the incidence of ESRD was not significantly reduced in the simvastatin plus ezetimibe group compared to the placebo group (rate ratio, 0.97; 95% CI, 0.89 to 1.05) during a median follow-up of 4.8 years [123]. Even in a meta-analysis published in 2016, which included 143,888 participants from seven RCTs concluded that, despite the modest reduction in the proteinuria and the rate of eGFR decline, the risk kidney failure event, defined as a composite of more than 25% or 50% decrease in eGFR, doubling of serum creatinine level, or onset of ESRD, was not ultimately reduced by statin therapy (odds ratio, 0.98; 95% CI, 0.87 to 1.10) [124]. The protective effect of statins against CKD progression was denied even in a cohort study, which reported that intensity of statin therapy is not significantly relevant to the risk of CKD progression, suggesting that long-term kidney outcomes may not be modified by statin therapy [125].
- The effect of pharmacologic interventions other than statins on the CKD progression is largely negative or unknown due to lack of data. In a clinical trial to test the effect of omega-3 fatty acids on the development or progression of CKD in patients with type 2 diabetes mellitus, the rate of eGFR decline for 5 years was not significantly reduced in the omga-3 fatty acid group compared to the placebo group, regardless of vitamin D3 supplement [126]. The role of fibrates in the delaying of CKD progression, however, remains to be further tested. In a meta-analysis of the clinical trial that evaluated the clinical benefits and safety of fibrate therapy, the risk of albuminuria progression was significantly reduced by fibrate therapy (risk ratio, 0.86; 95% CI, 0.76 to 0.98), although the risk of eGFR reduction was also significantly increased with fibrate therapy (mean difference, –2.67 mL/min/1.73 m2; 95% CI, –4.81 to –0.54) [97]. Yet, as previously mentioned, the use of fibrates does not seem to significantly accelerate the progression of CKD, as the initial increase in creatinine remains relatively constant afterwards [98]. Moreover, a recent nation-wide cohort study conducted in Taiwan, which only included that the patients with advanced CKD, reported that monotherapy with fenofibrate was associated the lowest incidence of permanent dialysis (fenofibrate vs. nonuser: subdistribution hazard ratio [SHR], 0.78; 95% CI, 0.77 to 0.80; statins vs. fenofibrate: SHR, 1.27; 95% CI, 1.26 to 1.29; combination of statins and fenofibrate vs. fenofibrate: SHR, 1.15; 95% CI, 1.13 to 1.17) [127]. It is impressive that the index date of ‘advanced CKD’ in this study was operationally defined as the first prescription of an erythropoiesis-stimulating agent, which can be used in the case of eGFR <15 mL/min/1.73 m2 and a hematocrit level <28% in Taiwan, suggesting the potential efficacy of fenofibrate to delay the progression of CKD even in advanced stages. Currently, a clinical trial to address the effect of pemafibrate, a novel selective PPARα modulator, on the kidney protection in patients with CKD in on-going [128]. The key eligible criteria of the Pemafibrate, open-label, Randomized cOntrolled study to evaluate the renal protective eFfect In hypertriglyceridemia patients with Chronic Kidney Disease (PROFIT-CKD) study include spot urine protein-to-creatinine ration ≥0.15 g/gCr within 3 months before enrollment and fasting TG ≥150 mg/dL and <1,000 mg/dL at enrollment. It is expected that the study may present a conclusive result to determine the overall effect of fibrates on the kidney function in patients with CKD, as the estimation of eGFR at the baseline and 12-month follow-up is scheduled as a secondary endpoint, although those with serum creatinine ≥2.5 mg/dL or creatinine clearance <40 mL/min are excluded.
DYSLIPIDEMIA AND CKD PROGRESSION
- The management of dyslipidemia in CKD is obviously challenging. Besides the lack of high-quality evidence derived from CKD population, the impact of dyslipidemia on cardiovascular outcomes seems to be substantially modified as kidney function deteriorates. Further, it has been questionable whether the unique pattern of alterations in lipid profile of CKD population should be the target of therapy. Based on all of these contexts, it seems natural that the 2013 KDIGO guideline presented a relatively conservative approach with respect to the indication of lipid lowering therapy and therapeutic monitoring among the patients with CKD. However, the currently available data suggests that elevated LDL-C levels still increase the risk of atherosclerotic adverse events even in patients with ESRD, and that hypertriglyceridemia also impose residual cardiovascular burden in this population. A sophisticated analysis of updated evidence suggests that the use of statins, omega-3 fatty acid or fibrates might be beneficial on the basis of the individualized assessment of the risk for cardiovascular disease even among those who are not routinely indicated in the guidelines. The use of PCSK9 inhibitors should also be expanded in patients with CKD, provided that evidence for the patients with CKD will be accumulating. Moreover, there is compelling evidence that dyslipidemia is associated with CKD progression. Although the effect of statins to delay CKD progression by lowering LDL-Cs have been consistently failed, the role of pharmacologic interventions other than statins on the CKD progression is largely undetermined yet. In this regard, targeting hypertriglyceridemia by fibrates may be promising to prevent CKD progression, while conclusive results are being awaited from RCTs.
CONCLUSIONS
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
This work wassupported by the National Research Foundation of Korea (NRF) funded by the Korea government (MSIT) (RS2023-00217317, NRF -2020R1F1A1074001) and a grant (BCRI 22042 and BCRI22079) of Chonnam National University Hospital Biomedical Research Institute.
NOTES
-
Acknowledgements
- None




LDL-C, low-density lipoprotein cholesterol; CKD, chronic kidney disease; KDIGO, Kidney Disease: Improving Global Outcomes; ASCVD, atherosclerotic cardiovascular disease; KT, kidney transplantation; ESC, European Society of Cardiology; eGFR, estimated glomerular filtration rate; KSoLA, Korean Society of Lipid and Atherosclerosis.
4D, The Die Deutsche Diabetes Dialyse Studie; HD, hemodialysis; LDL, low-density lipoprotein; MI, myocardial infarction; HR, hazard ratio; CI, confidence interval; RR, relative risk; AURORA, A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Haemodialysis: An Assessment of Survival and Cardiovascular Events; ALERT, The Assessment of Lescol in Renal Transplantation; KT, kidney transplantation; SHARP, Study of Heart and Renal Protection; PD, peritoneal dialysis.
- 1. Hager MR, Narla AD, Tannock LR. Dyslipidemia in patients with chronic kidney disease. Rev Endocr Metab Disord 2017;18:29-40.ArticlePubMedPDF
- 2. Visconti L, Benvenga S, Lacquaniti A, Cernaro V, Bruzzese A, Conti G, et al. Lipid disorders in patients with renal failure: role in cardiovascular events and progression of chronic kidney disease. J Clin Transl Endocrinol 2016;6:8-14.ArticlePubMedPMC
- 3. Florens N, Calzada C, Lyasko E, Juillard L, Soulage CO. Modified lipids and lipoproteins in chronic kidney disease: a new class of uremic toxins. Toxins (Basel) 2016;8:376.ArticlePubMedPMC
- 4. Mesquita J, Varela A, Medina JL. Dyslipidemia in renal disease: causes, consequences and treatment. Endocrinol Nutr 2010;57:440-8.ArticlePubMed
- 5. Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, et al. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation 2007;115:450-8.ArticlePubMed
- 6. Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease: the Framingham Study. Am J Med 1977;62:707-14.ArticlePubMed
- 7. Arntzenius AC, Kromhout D, Barth JD, Reiber JH, Bruschke AV, Buis B, et al. Diet, lipoproteins, and the progression of coronary atherosclerosis: the Leiden Intervention Trial. N Engl J Med 1985;312:805-11.ArticlePubMed
- 8. Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139:e1046-81.PubMed
- 9. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J 2020;41:111-88.ArticlePubMedPDF
- 10. Anderson TJ, Gregoire J, Pearson GJ, Barry AR, Couture P, Dawes M, et al. 2016 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2016;32:1263-82.ArticlePubMed
- 11. Wanner C, Tonelli M; Kidney Disease: Improving Global Outcomes Lipid Guideline Development Work Group Members. KDIGO clinical practice guideline for lipid management in CKD: summary of recommendation statements and clinical approach to the patient. Kidney Int 2014;85:1303-9.ArticlePubMed
- 12. Vaziri ND, Sato T, Liang K. Molecular mechanisms of altered cholesterol metabolism in rats with spontaneous focal glomerulosclerosis. Kidney Int 2003;63:1756-63.ArticlePubMed
- 13. Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis 1990;15:458-82.ArticlePubMed
- 14. Baigent C, Landray MJ, Wheeler DC. Misleading associations between cholesterol and vascular outcomes in dialysis patients: the need for randomized trials. Semin Dial 2007;20:498-503.PubMed
- 15. Lee C, Park JT, Chang TI, Kang EW, Nam KH, Joo YS, et al. Low-density lipoprotein cholesterol levels and adverse clinical outcomes in chronic kidney disease: results from the KNOWCKD. Nutr Metab Cardiovasc Dis 2022;32:410-9.ArticlePubMed
- 16. Suh SH, Oh TR, Choi HS, Kim CS, Bae EH, Oh KH, et al. Serum triglycerides level is independently associated with renal outcomes in patients with non-dialysis chronic kidney disease: results from KNOW-CKD study. Front Nutr 2022;9:1037618.ArticlePubMedPMC
- 17. Nam KH, Chang TI, Joo YS, Kim J, Lee S, Lee C, et al. Association between serum high-density lipoprotein cholesterol levels and progression of chronic kidney disease: results from the KNOW-CKD. J Am Heart Assoc 2019;8:e011162.ArticlePubMedPMC
- 18. Suh SH, Oh TR, Choi HS, Kim CS, Bae EH, Ma SK, et al. Non-high-density lipoprotein cholesterol and cardiovascular outcomes in chronic kidney disease: results from KNOW-CKD Study. Nutrients 2022;14:3792.ArticlePubMedPMC
- 19. Suh SH, Oh TR, Choi HS, Kim CS, Bae EH, Ma SK, et al. Nonhigh-density lipoprotein cholesterol and progression of chronic kidney disease: results from the KNOW-CKD Study. Nutrients 2022;14:4704.ArticlePubMedPMC
- 20. Cho SMJ, Lee H, Lee HH, Baek J, Heo JE, Joo HJ, et al. Dyslipidemia fact sheets in Korea 2020: an analysis of nationwide population-based data. J Lipid Atheroscler 2021;10:202-9.ArticlePubMedPMCPDF
- 21. Boren J, Williams KJ. The central role of arterial retention of cholesterol-rich apolipoprotein-B-containing lipoproteins in the pathogenesis of atherosclerosis: a triumph of simplicity. Curr Opin Lipidol 2016;27:473-83.ArticlePubMed
- 22. Sniderman AD, Thanassoulis G, Glavinovic T, Navar AM, Pencina M, Catapano A, et al. Apolipoprotein B particles and cardiovascular disease: a narrative review. JAMA Cardiol 2019;4:1287-95.ArticlePubMedPMC
- 23. Reiss AB, Voloshyna I, De Leon J, Miyawaki N, Mattana J. Cholesterol metabolism in CKD. Am J Kidney Dis 2015;66:1071-82.ArticlePubMedPMC
- 24. Chen H, Chen L, Liu D, Chen DQ, Vaziri ND, Yu XY, et al. Combined clinical phenotype and lipidomic analysis reveals the impact of chronic kidney disease on lipid metabolism. J Proteome Res 2017;16:1566-78.ArticlePubMed
- 25. Chu M, Wang AY, Chan IH, Chui SH, Lam CW. Serum small-dense LDL abnormalities in chronic renal disease patients. Br J Biomed Sci 2012;69:99-102.ArticlePubMed
- 26. Gardner CD, Fortmann SP, Krauss RM. Association of small low-density lipoprotein particles with the incidence of coronary artery disease in men and women. JAMA 1996;276:875-81.ArticlePubMed
- 27. Qiao YN, Zou YL, Guo SD. Low-density lipoprotein particles in atherosclerosis. Front Physiol 2022;13:931931.ArticlePubMedPMC
- 28. Kronenberg F. HDL in CKD: the devil is in the detail. J Am Soc Nephrol 2018;29:1356-71.ArticlePubMedPMC
- 29. Batista MC, Welty FK, Diffenderfer MR, Sarnak MJ, Schaefer EJ, Lamon-Fava S, et al. Apolipoprotein A-I, B-100, and B-48 metabolism in subjects with chronic kidney disease, obesity, and the metabolic syndrome. Metabolism 2004;53:1255-61.ArticlePubMed
- 30. Cardinal H, Raymond MA, Hebert MJ, Madore F. Uraemic plasma decreases the expression of ABCA1, ABCG1 and cell-cycle genes in human coronary arterial endothelial cells. Nephrol Dial Transplant 2007;22:409-16.ArticlePubMed
- 31. Calabresi L, Simonelli S, Conca P, Busnach G, Cabibbe M, Gesualdo L, et al. Acquired lecithin:cholesterol acyltransferase deficiency as a major factor in lowering plasma HDL levels in chronic kidney disease. J Intern Med 2015;277:552-61.ArticlePubMedPDF
- 32. Vaziri ND, Liang K, Parks JS. Down-regulation of hepatic lecithin:cholesterol acyltransferase gene expression in chronic renal failure. Kidney Int 2001;59:2192-6.ArticlePubMed
- 33. Seiler S, Schlitt A, Jiang XC, Ulrich C, Blankenberg S, Lackner KJ, et al. Cholesteryl ester transfer protein activity and cardiovascular events in patients with chronic kidney disease stage V. Nephrol Dial Transplant 2008;23:3599-604.ArticlePubMed
- 34. Yamamoto S, Yancey PG, Ikizler TA, Jerome WG, Kaseda R, Cox B, et al. Dysfunctional high-density lipoprotein in patients on chronic hemodialysis. J Am Coll Cardiol 2012;60:2372-9.ArticlePubMedPMC
- 35. Shroff R, Speer T, Colin S, Charakida M, Zewinger S, Staels B, et al. HDL in children with CKD promotes endothelial dysfunction and an abnormal vascular phenotype. J Am Soc Nephrol 2014;25:2658-68.ArticlePubMedPMC
- 36. Castillo-Nunez Y, Morales-Villegas E, Aguilar-Salinas CA. Triglyceride-rich lipoproteins: their role in atherosclerosis. Rev Invest Clin 2022;74:61-70.
- 37. Duran EK, Pradhan AD. Triglyceride-rich lipoprotein remnants and cardiovascular disease. Clin Chem 2021;67:183-96.ArticlePubMedPDF
- 38. Zhang BH, Yin F, Qiao YN, Guo SD. Triglyceride and triglyceride-rich lipoproteins in atherosclerosis. Front Mol Biosci 2022;9:909151.ArticlePubMedPMC
- 39. de Vries MA, Klop B, Janssen HW, Njo TL, Westerman EM, Castro Cabezas M. Postprandial inflammation: targeting glucose and lipids. Adv Exp Med Biol 2014;824:161-70.PubMed
- 40. Kwan BC, Kronenberg F, Beddhu S, Cheung AK. Lipoprotein metabolism and lipid management in chronic kidney disease. J Am Soc Nephrol 2007;18:1246-61.ArticlePubMed
- 41. Moon JH, Kim K, Choi SH. Lipoprotein lipase: is it a magic target for the treatment of hypertriglyceridemia. Endocrinol Metab (Seoul) 2022;37:575-86.ArticlePubMedPMCPDF
- 42. Vaziri ND, Yuan J, Ni Z, Nicholas SB, Norris KC. Lipoprotein lipase deficiency in chronic kidney disease is accompanied by down-regulation of endothelial GPIHBP1 expression. Clin Exp Nephrol 2012;16:238-43.ArticlePubMedPMCPDF
- 43. Vaziri ND, Wang XQ, Liang K. Secondary hyperparathyroidism downregulates lipoprotein lipase expression in chronic renal failure. Am J Physiol 1997;273:F925-30.ArticlePubMed
- 44. Vaziri ND, Liang K. Down-regulation of tissue lipoprotein lipase expression in experimental chronic renal failure. Kidney Int 1996;50:1928-35.ArticlePubMed
- 45. Vaziri ND, Liang K. Down-regulation of VLDL receptor expression in chronic experimental renal failure. Kidney Int 1997;51:913-9.ArticlePubMed
- 46. van Capelleveen JC, van der Valk FM, Stroes ES. Current therapies for lowering lipoprotein (a). J Lipid Res 2016;57:1612-8.ArticlePubMedPMC
- 47. Klezovitch O, Edelstein C, Zhu L, Scanu AM. Apolipoprotein (a) binds via its C-terminal domain to the protein core of the proteoglycan decorin: implications for the retention of lipoprotein (a) in atherosclerotic lesions. J Biol Chem 1998;273:23856-65.PubMed
- 48. Hopewell JC, Haynes R, Baigent C. The role of lipoprotein (a) in chronic kidney disease. J Lipid Res 2018;59:577-85.ArticlePubMedPMC
- 49. Wang X, Li J, Ju J, Fan Y, Xu H. Effect of different types and dosages of statins on plasma lipoprotein(a) levels: a network meta-analysis. Pharmacol Res 2021;163:105275.ArticlePubMed
- 50. Tsimikas S, Gordts PL, Nora C, Yeang C, Witztum JL. Statin therapy increases lipoprotein(a) levels. Eur Heart J 2020;41:2275-84.ArticlePubMedPDF
- 51. Bajaj A, Damrauer SM, Anderson AH, Xie D, Budoff MJ, Go AS, et al. Lipoprotein(a) and risk of myocardial infarction and death in chronic kidney disease: findings from the CRIC Study (Chronic Renal Insufficiency Cohort). Arterioscler Thromb Vasc Biol 2017;37:1971-8.PubMedPMC
- 52. Milionis HJ, Elisaf MS, Tselepis A, Bairaktari E, Karabina SA, Siamopoulos KC. Apolipoprotein(a) phenotypes and lipoprotein (a) concentrations in patients with renal failure. Am J Kidney Dis 1999;33:1100-6.ArticlePubMed
- 53. Sechi LA, Zingaro L, De Carli S, Sechi G, Catena C, Falleti E, et al. Increased serum lipoprotein(a) levels in patients with early renal failure. Ann Intern Med 1998;129:457-61.ArticlePubMed
- 54. Kronenberg F, Trenkwalder E, Lingenhel A, Friedrich G, Lhotta K, Schober M, et al. Renovascular arteriovenous differences in Lp[a] plasma concentrations suggest removal of Lp[a] from the renal circulation. J Lipid Res 1997;38:1755-63.ArticlePubMed
- 55. Reblin T, Donarski N, Fineder L, Brasen JH, Dieplinger H, Thaiss F, et al. Renal handling of human apolipoprotein(a) and its fragments in the rat. Am J Kidney Dis 2001;38:619-30.ArticlePubMed
- 56. Cain WJ, Millar JS, Himebauch AS, Tietge UJ, Maugeais C, Usher D, et al. Lipoprotein [a] is cleared from the plasma primarily by the liver in a process mediated by apolipoprotein [a]. J Lipid Res 2005;46:2681-91.ArticlePubMed
- 57. Emerging Risk Factors Collaboration, Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009;302:1993-2000.ArticlePubMedPMC
- 58. Saran R, Robinson B, Abbott KC, Agodoa LY, Albertus P, Ayanian J, et al. US renal data system 2016 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis 2017;69(3 Suppl 1):A7-8.PubMedPMC
- 59. Methven S, Steenkamp R, Fraser S. UK Renal Registry 19th annual report: chapter 5 survival and causes of death in UK adult patients on renal replacement therapy in 2015: national and centre-specific analyses. Nephron 2017;137 Suppl 1:117-50.ArticlePubMed
- 60. Cholesterol Treatment Trialists’ (CTT) Collaboration, Herrington WG, Emberson J, Mihaylova B, Blackwell L, Reith C, et al. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens: a meta-analysis of individual participant data from 28 randomised trials. Lancet Diabetes Endocrinol 2016;4:829-39.ArticlePubMed
- 61. Chue CD, Townend JN, Steeds RP, Ferro CJ. Arterial stiffness in chronic kidney disease: causes and consequences. Heart 2010;96:817-23.ArticlePubMed
- 62. Zanoli L, Lentini P, Briet M, Castellino P, House AA, London GM, et al. Arterial stiffness in the heart disease of CKD. J Am Soc Nephrol 2019;30:918-28.ArticlePubMedPMC
- 63. Edwards NC, Moody WE, Chue CD, Ferro CJ, Townend JN, Steeds RP. Defining the natural history of uremic cardiomyopathy in chronic kidney disease: the role of cardiovascular magnetic resonance. JACC Cardiovasc Imaging 2014;7:703-14.PubMed
- 64. Mall G, Huther W, Schneider J, Lundin P, Ritz E. Diffuse intermyocardiocytic fibrosis in uraemic patients. Nephrol Dial Transplant 1990;5:39-44.ArticlePubMed
- 65. Aoki J, Ikari Y, Nakajima H, Mori M, Sugimoto T, Hatori M, et al. Clinical and pathologic characteristics of dilated cardiomyopathy in hemodialysis patients. Kidney Int 2005;67:333-40.ArticlePubMed
- 66. Storey BC, Staplin N, Haynes R, Reith C, Emberson J, Herrington WG, et al. Lowering LDL cholesterol reduces cardiovascular risk independently of presence of inflammation. Kidney Int 2018;93:1000-7.ArticlePubMedPMC
- 67. Barter PJ, Caulfield M, Eriksson M, Grundy SM, Kastelein JJ, Komajda M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med 2007;357:2109-22.ArticlePubMed
- 68. AIM-HIGH Investigators, Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011;365:2255-67.ArticlePubMed
- 69. Schwartz GG, Olsson AG, Abt M, Ballantyne CM, Barter PJ, Brumm J, et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med 2012;367:2089-99.ArticlePubMed
- 70. HPS2-THRIVE Collaborative Group, Landray MJ, Haynes R, Hopewell JC, Parish S, Aung T, et al. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med 2014;371:203-12.ArticlePubMed
- 71. Zewinger S, Speer T, Kleber ME, Scharnagl H, Woitas R, Lepper PM, et al. HDL cholesterol is not associated with lower mortality in patients with kidney dysfunction. J Am Soc Nephrol 2014;25:1073-82.ArticlePubMedPMC
- 72. Silbernagel G, Genser B, Drechsler C, Scharnagl H, Grammer TB, Stojakovic T, et al. HDL cholesterol, apolipoproteins, and cardiovascular risk in hemodialysis patients. J Am Soc Nephrol 2015;26:484-92.ArticlePubMedPMC
- 73. Moradi H, Streja E, Kashyap ML, Vaziri ND, Fonarow GC, Kalantar-Zadeh K. Elevated high-density lipoprotein cholesterol and cardiovascular mortality in maintenance hemodialysis patients. Nephrol Dial Transplant 2014;29:1554-62.ArticlePubMedPMC
- 74. Kim JY, Park JT, Kim HW, Chang TI, Kang EW, Ahn C, et al. Inflammation alters relationship between high-density lipoprotein cholesterol and cardiovascular risk in patients with chronic kidney disease: results from KNOW-CKD. J Am Heart Assoc 2021;10:e021731.ArticlePubMedPMC
- 75. Levy RI, Glueck CJ. Hypertriglyceridemia, diabetes mellitus, and coronary vessel disease. Arch Intern Med 1969;123:220-8.ArticlePubMed
- 76. Zammit AR, Katz MJ, Derby C, Bitzer M, Lipton RB. Chronic kidney disease in non-diabetic older adults: associated roles of the metabolic syndrome, inflammation, and insulin resistance. PLoS One 2015;10:e0139369.ArticlePubMedPMC
- 77. Soohoo M, Hashemi L, Hsiung JT, Moradi H, Budoff MJ, Kovesdy CP, et al. Risk of atherosclerotic cardiovascular disease and nonatherosclerotic cardiovascular disease hospitalizations for triglycerides across chronic kidney disease stages among 2.9 million US veterans. J Am Heart Assoc 2021;10:e022988.ArticlePubMedPMC
- 78. Liao JK. Effects of statins on 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibition beyond low-density lipoprotein cholesterol. Am J Cardiol 2005;96(5A):24F-33F.ArticlePubMedPMC
- 79. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9.PubMed
- 80. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med 1996;335:1001-9.ArticlePubMed
- 81. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685-96.ArticlePubMed
- 82. Collins R, Armitage J, Parish S, Sleigh P, Peto R; Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003;361:2005-16.ArticlePubMed
- 83. Wanner C, Krane V, Marz W, Olschewski M, Mann JF, Ruf G, et al. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med 2005;353:238-48.ArticlePubMed
- 84. Fellstrom BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med 2009;360:1395-407.ArticlePubMed
- 85. Marz W, Genser B, Drechsler C, Krane V, Grammer TB, Ritz E, et al. Atorvastatin and low-density lipoprotein cholesterol in type 2 diabetes mellitus patients on hemodialysis. Clin J Am Soc Nephrol 2011;6:1316-25.ArticlePubMedPMC
- 86. Peto R. Current misconception 3: that subgroup-specific trial mortality results often provide a good basis for individualising patient care. Br J Cancer 2011;104:1057-8.ArticlePubMedPMCPDF
- 87. Sleight P. Debate: subgroup analyses in clinical trials: fun to look at - but don’t believe them! Curr Control Trials Cardiovasc Med 2000;1:25-7.ArticlePubMedPMC
- 88. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet 2011;377:2181-92.PubMedPMC
- 89. Cholesterol Treatment Trialists’ (CTT) Collaboration, Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010;376:1670-81.ArticlePubMedPMC
- 90. Tonelli M, Muntner P, Lloyd A, Manns B, Klarenbach S, Pannu N, et al. Association between LDL-C and risk of myocardial infarction in CKD. J Am Soc Nephrol 2013;24:979-86.ArticlePubMedPMC
- 91. Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995;333:1301-7.ArticlePubMed
- 92. Tsimikas S. A test in context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Am Coll Cardiol 2017;69:692-711.PubMed
- 93. Streja E, Gosmanova EO, Molnar MZ, Soohoo M, Moradi H, Potukuchi PK, et al. Association of continuation of statin therapy initiated before transition to chronic dialysis therapy with mortality after dialysis initiation. JAMA Netw Open 2018;1:e182311.ArticlePubMedPMC
- 94. Rhee EJ, Kim HC, Kim JH, Lee EY, Kim BJ, Kim EM, et al. 2018 Guidelines for the management of dyslipidemia in Korea. J Lipid Atheroscler 2019;8:78-131.ArticlePubMedPMCPDF
- 95. Holdaas H, Fellstrom B, Jardine AG, Holme I, Nyberg G, Fauchald P, et al. Effect of fluvastatin on cardiac outcomes in renal transplant recipients: a multicentre, randomised, placebo-controlled trial. Lancet 2003;361:2024-31.ArticlePubMed
- 96. Holdaas H, Fellstrom B, Cole E, Nyberg G, Olsson AG, Pedersen TR, et al. Long-term cardiac outcomes in renal transplant recipients receiving fluvastatin: the ALERT extension study. Am J Transplant 2005;5:2929-36.ArticlePubMed
- 97. Jun M, Zhu B, Tonelli M, Jardine MJ, Patel A, Neal B, et al. Effects of fibrates in kidney disease: a systematic review and meta-analysis. J Am Coll Cardiol 2012;60:2061-71.PubMed
- 98. Hadjivasilis A, Kouis P, Kousios A, Panayiotou A. The effect of fibrates on kidney function and chronic kidney disease progression: a systematic review and meta-analysis of randomised studies. J Clin Med 2022;11:768.ArticlePubMedPMC
- 99. Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11-22.ArticlePubMed
- 100. Majithia A, Bhatt DL, Friedman AN, Miller M, Steg PG, Brinton EA, et al. Benefits of icosapent ethyl across the range of kidney function in patients with established cardiovascular disease or diabetes: REDUCE-IT RENAL. Circulation 2021;144:1750-9.ArticlePubMedPMC
- 101. Nicholls SJ, Lincoff AM, Garcia M, Bash D, Ballantyne CM, Barter PJ, et al. Effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events in patients at high cardiovascular risk: the STRENGTH Randomized Clinical Trial. JAMA 2020;324:2268-80.ArticlePubMedPMC
- 102. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2020;41:111-88.PubMed
- 103. Marais DA, Blom DJ, Petrides F, Goueffic Y, Lambert G. Proprotein convertase subtilisin/kexin type 9 inhibition. Curr Opin Lipidol 2012;23:511-7.ArticlePubMed
- 104. Lambert G, Sjouke B, Choque B, Kastelein JJ, Hovingh GK. The PCSK9 decade. J Lipid Res 2012;53:2515-24.ArticlePubMedPMC
- 105. Colhoun HM, Robinson JG, Farnier M, Cariou B, Blom D, Kereiakes DJ, et al. Efficacy and safety of alirocumab, a fully human PCSK9 monoclonal antibody, in high cardiovascular risk patients with poorly controlled hypercholesterolemia on maximally tolerated doses of statins: rationale and design of the ODYSSEY COMBO I and II trials. BMC Cardiovasc Disord 2014;14:121.ArticlePubMedPMCPDF
- 106. Kastelein JJ, Robinson JG, Farnier M, Krempf M, Langslet G, Lorenzato C, et al. Efficacy and safety of alirocumab in patients with heterozygous familial hypercholesterolemia not adequately controlled with current lipid-lowering therapy: design and rationale of the ODYSSEY FH studies. Cardiovasc Drugs Ther 2014;28:281-9.ArticlePubMedPMCPDF
- 107. Moriarty PM, Jacobson TA, Bruckert E, Thompson PD, Guyton JR, Baccara-Dinet MT, et al. Efficacy and safety of alirocumab, a monoclonal antibody to PCSK9, in statin-intolerant patients: design and rationale of ODYSSEY ALTERNATIVE, a randomized phase 3 trial. J Clin Lipidol 2014;8:554-61.ArticlePubMed
- 108. Robinson JG, Colhoun HM, Bays HE, Jones PH, Du Y, Hanotin C, et al. Efficacy and safety of alirocumab as add-on therapy in high-cardiovascular-risk patients with hypercholesterolemia not adequately controlled with atorvastatin (20 or 40 mg) or rosuvastatin (10 or 20 mg): design and rationale of the ODYSSEY OPTIONS Studies. Clin Cardiol 2014;37:597-604.ArticlePubMedPMCPDF
- 109. Schwartz GG, Bessac L, Berdan LG, Bhatt DL, Bittner V, Diaz R, et al. Effect of alirocumab, a monoclonal antibody to PCSK9, on long-term cardiovascular outcomes following acute coronary syndromes: rationale and design of the ODYSSEY outcomes trial. Am Heart J 2014;168:682-9.ArticlePubMed
- 110. Cannon CP, Cariou B, Blom D, McKenney JM, Lorenzato C, Pordy R, et al. Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated doses of statins: the ODYSSEY COMBO II randomized controlled trial. Eur Heart J 2015;36:1186-94.ArticlePubMedPMC
- 111. Bays H, Gaudet D, Weiss R, Ruiz JL, Watts GF, Gouni-Berthold I, et al. Alirocumab as add-on to atorvastatin versus other lipid treatment strategies: ODYSSEY OPTIONS I randomized trial. J Clin Endocrinol Metab 2015;100:3140-8.ArticlePubMedPMC
- 112. Kastelein JJ, Ginsberg HN, Langslet G, Hovingh GK, Ceska R, Dufour R, et al. ODYSSEY FH I and FH II: 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur Heart J 2015;36:2996-3003.ArticlePubMedPMC
- 113. Kereiakes DJ, Robinson JG, Cannon CP, Lorenzato C, Pordy R, Chaudhari U, et al. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: the ODYSSEY COMBO I study. Am Heart J 2015;169:906-15.ArticlePubMed
- 114. Roth EM, McKenney JM. ODYSSEY MONO: effect of alirocumab 75 mg subcutaneously every 2 weeks as monotherapy versus ezetimibe over 24 weeks. Future Cardiol 2015;11:27-37.ArticlePubMed
- 115. Farnier M, Jones P, Severance R, Averna M, Steinhagen-Thiessen E, Colhoun HM, et al. Efficacy and safety of adding alirocumab to rosuvastatin versus adding ezetimibe or doubling the rosuvastatin dose in high cardiovascular-risk patients: the ODYSSEY OPTIONS II randomized trial. Atherosclerosis 2016;244:138-46.ArticlePubMed
- 116. Robinson JG, Nedergaard BS, Rogers WJ, Fialkow J, Neutel JM, Ramstad D, et al. Effect of evolocumab or ezetimibe added to moderate- or high-intensity statin therapy on LDL-C lowering in patients with hypercholesterolemia: the LAPLACE-2 randomized clinical trial. JAMA 2014;311:1870-82.ArticlePubMed
- 117. Stroes E, Colquhoun D, Sullivan D, Civeira F, Rosenson RS, Watts GF, et al. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: the GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. J Am Coll Cardiol 2014;63:2541-8.PubMed
- 118. Koren MJ, Lundqvist P, Bolognese M, Neutel JM, Monsalvo ML, Yang J, et al. Anti-PCSK9 monotherapy for hypercholesterolemia: the MENDEL-2 randomized, controlled phase III clinical trial of evolocumab. J Am Coll Cardiol 2014;63:2531-40.PubMed
- 119. Blom DJ, Hala T, Bolognese M, Lillestol MJ, Toth PD, Burgess L, et al. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N Engl J Med 2014;370:1809-19.ArticlePubMed
- 120. Raal FJ, Stein EA, Dufour R, Turner T, Civeira F, Burgess L, et al. PCSK9 inhibition with evolocumab (AMG 145) in heterozygous familial hypercholesterolaemia (RUTHERFORD-2): a randomised, double-blind, placebo-controlled trial. Lancet 2015;385:331-40.ArticlePubMed
- 121. Toth PP, Dwyer JP, Cannon CP, Colhoun HM, Rader DJ, Upadhyay A, et al. Efficacy and safety of lipid lowering by alirocumab in chronic kidney disease. Kidney Int 2018;93:1397-408.ArticlePubMed
- 122. Charytan DM, Sabatine MS, Pedersen TR, Im K, Park JG, Pineda AL, et al. Efficacy and safety of evolocumab in chronic kidney disease in the FOURIER Trial. J Am Coll Cardiol 2019;73:2961-70.ArticlePubMed
- 123. Haynes R, Lewis D, Emberson J, Reith C, Agodoa L, Cass A, et al. Effects of lowering LDL cholesterol on progression of kidney disease. J Am Soc Nephrol 2014;25:1825-33.ArticlePubMedPMC
- 124. Su X, Zhang L, Lv J, Wang J, Hou W, Xie X, et al. Effect of statins on kidney disease outcomes: a systematic review and meta-analysis. Am J Kidney Dis 2016;67:881-92.ArticlePubMed
- 125. Jhee JH, Joo YS, Park JT, Yoo TH, Park SK, Jung JY, et al. Intensity of statin therapy and renal outcome in chronic kidney disease: results from the Korean cohort study for outcome in patients with chronic kidney disease. Kidney Res Clin Pract 2020;39:93-102.ArticlePubMedPMC
- 126. de Boer IH, Zelnick LR, Ruzinski J, Friedenberg G, Duszlak J, Bubes VY, et al. Effect of vitamin D and omega-3 fatty acid supplementation on kidney function in patients with type 2 diabetes: a randomized clinical trial. JAMA 2019;322:1899-909.ArticlePubMedPMC
- 127. Yen CL, Fan PC, Lin MS, Lee CC, Tu KH, Chen CY, et al. Fenofibrate delays the need for dialysis and reduces cardiovascular risk among patients with advanced CKD. J Clin Endocrinol Metab 2021;106:1594-605.ArticlePubMedPDF
- 128. Seki M, Nakano T, Tanaka S, Matsukuma Y, Funakoshi K, Ohkuma T, et al. Design and methods of an open-label, randomized controlled trial to evaluate the effect of pemafibrate on proteinuria in CKD patients (PROFIT-CKD). Clin Exp Nephrol 2023;27:358-64.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
- Statin Therapy and Lipid Indices in Chronic Kidney Disease: A Systematic
Review and Meta-analysis of Randomized Control Trials
Jafar Karami, Bahman Razi, Danyal Imani, Saeed Aslani, Mahdi Pakjoo, Mahdieh Fasihi, Keyhan Mohammadi, Amirhossein Sahebkar
Current Pharmaceutical Design.2024; 30(5): 362. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite