The Effects of Small Sized Rice Bowl on Carbohydrate Intake and Dietary Patterns in Women with Type 2 Diabetes
Article information
Abstract
Background
The main source of carbohydrate in the Korean diet is rice, which is usually served in a rice bowl. This study investigated the impact of a meal plan using smaller rice bowls on dietary energy intake and macronutrient composition in overweight or obese patients with type 2 diabetes mellitus.
Methods
A total of 67 women with type 2 diabetes were enrolled in our study. We divided these participants into three groups: a normal-weight group (NW; body mass index [BMI] < 23 kg/m2; n = 17), an overweight group (OW; 23 ≤ BMI < 25 kg/m2; n = 24) and an obese group (OB; BMI ≥ 25 kg/m2; n = 26). Three-day dietary records were analyzed for total energy intake (TEI) and macronutrient composition both before enrollment and two weeks after patients received instruction in a dietary plan based on using a small (200 mL) rice bowl.
Results
After the intervention, TEI decreased in the OW and OB groups. Decreased carbohydrate (NW, -4 ± 5%; OW, -4 ± 5%; OB, -3 ± 6%) and increased fat intakes were found in all three groups, which complies with Korean Diabetes Association recommendations. The protein proportion of TEI significantly increased only in the OW group. Body weight decreased both in the OW and OB groups.
Conclusion
A short-term, small-rice-bowl-based meal plan was effective for body weight control and macronutrient balance in overweight or obese women in Korea with type 2 diabetes.
INTRODUCTION
The carbohydrate proportion of total energy intake of Korean and Americans are 64.5%, 51.7%, respectively (National Health and Nutrition Examination Survey) [1]. Usually Koreans consume high intake of carbohydrate than Americans. According to the Korea Health and Nutrition Examination Survey (KHANES), carbohydrate proportion of total energy intake in Korean with type 2 diabetes was 68% which is above the carbohydrate recommendations of Korean Diabetes Association (KDA); 55 to 60% [2,3]. Yang and Kim [4] reported that diabetes patients consume more carbohydrates than individuals without diabetes, and Jung et al. [5] also pointed out that reducing carbohydrate intake may decrease risk factors of cardiovascular disease in the adults.
Another study reported that carbohydrate intake affects blood glucose; excessive intake leads to obesity by promoting appetitite and the secretion of insulin, which increase body fat [6,7]. Hollenbeck et al. [8] revealed that when type 2 diabetes patients increase carbohydrate proportion of total energy intake from 50% to 60%, both triglyceride and postprandial blood glucose levels rise, and the higher blood glucose was difficult to control even after administration of more insulin in Koreans.
The traditional Korean rice-based diet includes numerous side dishes, because rice itself is bland. Korean side dishes tend to have strong tastes, such that they are difficult to eat without rice [9]. Therefore, the total energy intake for Koreans who eat a rice-based diet is dependent on the absolute amount of rice consumed [10]; decreasing rice intake by recommending the use of smaller rice bowls can influence total energy intake.
Ahn et al. [11] found that type 2 diabetes patients ate rice-based meals an average of 19.9 ± 2.3 times per week; the amount of rice intake was related to the sizes of the rice bowl used by patients. A 380-mL rice-bowl-based meal plan, which is most frequently used for type 2 diabetes patients in Korea, has already been reported to be as effective in controlling carbohydrate, protein and fat intake as food exchange system-based meal plans [12]. However, it is still unknown how dietary intake patterns affect obesity when patients with type 2 diabetes use smaller rice bowls.
This was a preliminary study to investigate the clinical effects of a small-rice-bowl-based meal plan in Korean type 2 diabetes patients. We examined the effects of short-term changes in carbohydrate and total energy intake through meals and snacks according to obesity by decreasing only rice bowl size.
METHODS
Participants
We recruited women with type 2 diabetes who visited the Diabetes Center of Eulji Hospital located in the Seoul from July 2009 to August 2009. The study participants included a total of 67 women aged 20 to 69 years with glycosylated hemoglobin (HbA1c) levels between 7% and 11%. Patients who had any special dietary habit (i.e., a vegetarian diet), gestational diabetes, malignant tumors, been treated with renal replacement therapy, secondary diabetes, or were difficult to follow-up, refused examination, ate meals at restaurants more the two times per week, and had dyspepsia or anorexia were excluded from our sample.
The participants were divided by body mass index (BMI) score into a normal weight (NW) group (BMI < 23 kg/m2, n = 17), an overweight (OW) group (23 kg/m2 ≤ BMI < 25 kg/m2, n = 24) and an obese (OB) group (BMI ≥ 25 kg/m2, n = 26), and their data were analyzed and compared.
Education
Rice bowls (Seonsu Chinaware, Seoul, Korea) of 200 mL that hold about 200 kcal of rice were given to all participants, and each received five minutes of individualized education on tips for putting rice in the bowl and for utilizing the bowl. The participants were informed that the rice bowl should be used for every meal and that no more rice should be eaten than would fit in the bowl. An informational leaflet was provided to inform participants that other sources of carbohydrate, such as bread, rice cake, potato and sweet potato should also be limited. Education regarding daily fruit intake was also provided through a leaflet.
Survey of bowl size
The participants were asked to bring the rice bowl they usually used to their meals. Because the sizes and shapes of bowls differed among participants, the sizes were determined by measuring the volume of water contained in the bowl with 100 mL and 500 mL measuring cylinders.
Dietary nutrient intake and patterns
To compare and analyze changes of energy intake during the study that resulted from meals and snacks, any foods that could be classified as fruit or dairy in the food exchange system (Korean Diabetes Association, Korean Dietetic Association, Korean Nutrition Society, 1994) and also those taken between meals were defined as snacks. The intake of meals and snacks was gauged using a three-day dietary record (two weekdays and one weekend day). A simple preliminary education on how to record meals and snacks was provided to help participants understand how to record food intake. Types and amount of all foods eaten each day were recorded; participants divided their intake into meals or supplementary foods and snacks. To increase the accuracy of these three-day food records, nutritionists reviewed examples using life-sized food models, measuring cups, measuring spoons, and data on eye measurement of foods (Korean Dietetic Association, 1999) with participants when the record sheet was returned. The contents of the records were analyzed with CAN-Pro version 2.0 (Computer-Aided Nutritional Analysis Program; Korean Nutrition Society, Seoul, Korea) and then translated into nutrient intake data.
As dietary energy intake differed according to obesity, the ratio of dietary energy intake to recommended energy intake was calculated and assessed for each patient. The recommended energy intake was obtained by multiplying the ideal body weight by 30 kcal/kg [13]. To observe dietary patterns and places for meals eaten on weekdays and weekends, the total number of meals, the number of meals consisting of rice and side dishes, and places where the participants ate the meals were investigated [14,15], and patients showing unusual dietary energy patterns (e.g., birthday party) were excluded from this study.
Physical measurements and biochemical tests
Heights and body weights of all participants were measured at the beginning of the study and again following the 2-week. Height and body weight measurements were take in light clothing (no outerwear), and BMI was calculated by dividing the body weight (kg) with the square of the height (m2). HbA1c was measured with high-performance liquid chromatography (HPLC) using cation exchange resin.
Statistical analyses
All data were analyzed with the SPSS version 15.0 (SPSS Inc., Chicago, IL, USA), and the means and standard deviations of all items were calculated. To investigate changes in physical characteristics for the two weeks of the study and to compare nutritient intake before and after the use of the smaller rice bowl, a paired sample t-test was used. One-way ANOVA and Duncan's post hoc tests were used to compare the three patient groups. A P value of less than 0.05 was considered to be statistically significant.
RESULTS
Participant characteristics
Our study initially included 78 patients (NW, n = 26; OW, n = 26; OB, n = 26), but after excluding those who had unusual dietary patterns (n = 3), those who refused to participate (n = 5), and those who had two or more meals a week at restaurants (n = 3), 67 patients were finally included as participants. There were no significant differences in the drop-out rates among the three groups. The mean age, duration of diabetes and HbA1c of the participants were 61.9 ± 6.4 years, 15.4 ± 6.8 years and 8.3 ± 0.9%, respectively, and they were not significantly different among the groups. Among our participants, 10.4% had not received formal education; educational status was not significantly different among the three groups. For diabetes treatments, the rates of using insulin, oral hypoglycemic agents and diet therapy were 58.1%, 32.8%, and 9%, respectively, and there were no significant differences among the groups for any of these variables. Ninety-four percent of our sample had received some type of diabetes education, but significant differences resulting from this education were not observed among the three groups (Table 1).
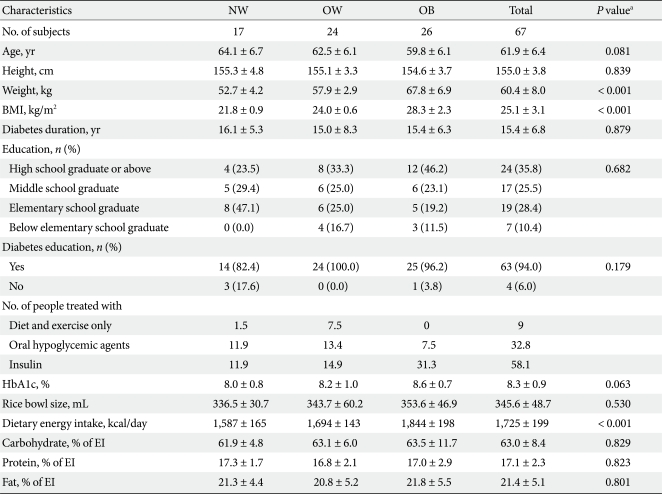
Baseline clinical characteristics of study subjects
Dietary total energy intake and nutrient intake by BMI before rice bowl based meal plan
The dietary total energy intake of the participants before education was 1,725 ± 199 kcal/day, and the OW and OB groups took in significantly more dietary energy than the NW group (P < 0.001, P < 0.001, respectively). The ratio of dietary energy intake to recommended energy intake were 104 ± 10%, 111 ± 8%, and 122 ± 13% in the NW, the OW, and the OB groups, respectively; those of the OW and the OB groups were higher than that of the NW group (Table 2).
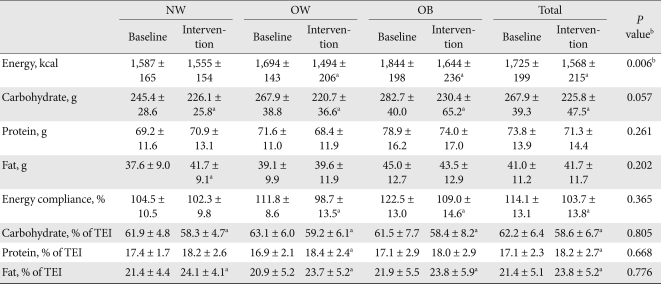
Dietary energy intake and amount and proportion of macronutrients in study subjects
The carbohydrate, protein and fat proportion of total energy intake were 62.2%, 17.1%, and 21.4%, respectively, and the carbohydrate proportion of total energy intake was higher than the 55 to 60% recommended by the KDA. There were no significant differences among the three groups for macronutrient intake (Table 2) [2].
Dietary energy intake and nutrient intake by BMI after rice bowl based meal plan
After education on the benefits of using a 200 mL rice bowl, total energy intake for participants remained the same in the NW group, but was significantly reduced by 200 ± 181 kcal/day and 199 ± 224 kcal/day in the OW and the OB groups, respectively (P < 0.001, P < 0.001, respectively). The ratio of dietary energy intake to recommended energy intake also did not change in the NW group, but it reached the recommended levels at 98 ± 13% and 109 ± 14% in the OW and the OB groups, respectively (P < 0.001, P < 0.001, respectively) (Table 2).
After education, the carbohydrate proportion of total energy intake decreased by 3.7 ± 4.5%, 3.9 ± 4.7%, and 3.1 ± 6.0% in the NW, the OW, and the OB groups, respectively, and their proportions became closer to those recommended by the KDA (P = 0.004, P < 0.001, and P = 0.015, respectively) [2]. Although the protein proportion of total energy intake increased by 1.4 ± 1.7% only in the OW group, it did not exceed the recommended daily level (P < 0.001). Changes of the protein proportion of total energy intake were not significantly different among the three groups. The fat proportion of total energy intake grew significantly by 2.7 ± 4.3%, 2.8 ± 5.1%, and 1.9 ± 4.6%, respectively (P = 0.019, P = 0.014, and P = 0.043, respectively), but it was still within the recommended KDA range [2]. There were no significant differences in fat proportion of total energy intake among the three groups (Table 2).
Changes of energy intake through meals and snacks
When measuring total energy intake, we classified milk and fruit as snacks and considered all other foods to be meals. Total energy intake from meals declined significantly by 142 ± 185 kcal/day and 189 ± 207 kcal/day in the OW and the OB groups, respectively (P = 0.001, P < 0.001, respectively), but total energy intake did not change in the NW group. Total energy intake from snacks decreased significantly by 59.1 ± 106.5 kcal/day only in the OW group (P = 0.005) but did not significantly change in the NW or the OB groups (Fig. 1).
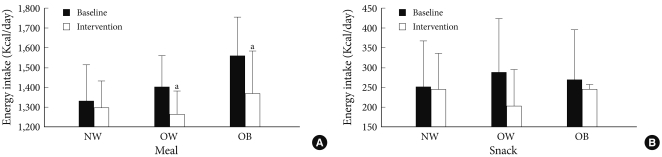
Patterns of meal and snack intake according to the body mass index. Values are energy intakes as meals and snacks. (A) Differences by energy intake as meal. (B) Differences by energy intake as snack. The energy intake as meal was decreased both in OW and OB (P = 0.001, P < 0.001), but not with in NW. The energy intake as snack was decreased in OW (P = 0.005). NW, normal weight; OW, overweight; OB, obese. aP values <0.05 for comparison between baseline and intervention.
Changes of body weight
After the education, body weight was reduced significantly by 0.4 ± 0.6 kg (-0.7%) and 0.5 ± 0.8 kg (-0.7%) in the OW and the OB groups, respectively (P = 0.003, P = 0.007, respectively), and no significant change was observed in the NW group. When considered as a percentage of ideal body weight, body weight was reduced from 115 ± 3.1% to 114 ± 3.0% and from 135 ± 11.4% to 134 ± 11.3% in the OW and the OB groups after the education, respectively (P = 0.003, P = 0.007, respectively) (Fig. 2).

Change of weight according to the body mass index. The weight was decreased both in OW and OB (P = 0.003, P = 0.007), but not with in NW. NW, normal weight; OW, overweight; OB, obese. aP values <0.05 for comparison between baseline and intervention.
DISCUSSION
In 2005, the KNHANES reported that the carbohydrate proportion of total energy intake in Korean women with diabetes was 70.3% [3]. Therefore, Korean women with diabetes consume a relatively high carbohydrate diet [16]. In addition, the KNHANES revealed that main source of carbohydrates are obtained from white rice, and mixed grains and white rice ranked first in frequently consumed food; these findings confirm that Koreans typically consume a rice-centered diet [3].
Among our participants, the carbohydrate proportion of total energy intake was 61.9%, 63.1%, and 63.5% in the NW, the OW, and the OB groups, respectively. These figures were lower than the proportion of 70.3% found by the KNHANES in 2005 [3] and also that of a study of Song and Lee [17] that reported proportions of 66.1%, 66.8%, and 67.4%, in normal, overweight, and obese type 2 diabetes patients, respectively. These variations were considered to result from differences in dietary patterns according to survey period and age [18], region [19], economic status [20,21] and level of diabetes education. In our study, 94% of the participants received education on diabetes, and our participants were observed to better control carbohydrate intake as a result. Nevertheless, we found that the carbohydrate proportion of total energy intake (62.2%) was higher than the recommended KDA range (55 to 60%), which suggests that more dietary education is needed to reduce carbohydrate consumption [2].
In this study, education using a smaller rice bowl effectively decreased carbohydrate intake in Korean women with diabetes regardless of BMI. Food-exchange-system-based education, which is commonly used for diabetes patients, teaches participants to regulate energy intake and marcronutrient composition [22]. Lee and Chang [22] reported that the carbohydrate proportion of type 2 diabetes patients decreased significantly from 62.3% to 59.6% following food-exchange-system-based education, and Ahn et al. [12] also revealed that carbohydrate proportion could decrease significantly from 61% to 57.3% with this type of education method. However, conventional education methods using a food exchange system require a great deal of time and intensive education or additional management education because patients cannot understand them easily; the shortage of available nutritionists also prevents adequate education [23]. To address the problem of food-exchange-system-based education, Ahn et al. [12] instead educated type 2 diabetes patients using an ordinary-sized rice bowl (380 mL) and found that portion control alone could decrease the carbohydrate proportion from 60.7% to 58.1%, or to the levels recommended by the KDA.
Education based on using a smaller rice bowl has been found to significantly increase the protein proportion from 17.1% to 18.2% while not exceeding the range of 15% to 20% recommended by the KDA; there was no significant difference among the groups [2]. This is similar to the findings of a study by Lee and Chang [22] showing that in type 2 diabetes patients, the protein proportion to total energy intake increased from 16.7% before education based on the food exchange system to 18.1% after it; and in this study, education based on a smaller rice bowl also regulated the protein proportion to total energy intake within the recommended range [2].
Although the fat proportion of total energy intake also increased significantly from 21.4% before the education to 23.8% after it, it still fell within the recommended range (P < 0.001), and no significant difference among the groups was observed. According to a study of Lee and Chang [22] education based on the food exchange system significantly increased the fat proportion of total energy intake by following the decrease of total energy intake in obese middle-aged woman, Ahn et al. [12] found that after a 12-week education program using a food exchange system for obese females with type 2 diabetes, the fat proportion to total energy intake increased, although the change was not statistically significant. In this study, the fat proportion of total energy intake became significantly higher in all three groups, and this change was thought to be caused by the decrease of the carbohydrate proportion of total energy intake. However, since the fat proportion of total energy intake increased significantly but was still within the recommended range, further studies on its long-term and clinical effects are necessary.
Smaller rice bowl based diets reduced engery intake by 200 ± 181 kcal/day and 199 ± 224 kcal/day in the OW and OB groups of our study, respectively. In the OW group, energy intake from meals and snacks was reduced; in the OB, energy intake from meals also declined. This finding was similar to that of Lee [24], who reported that education based on a food exchange system for middle-aged women decreased total dietary energy intake but did not reduce snack intake. Therefore, other active methods were needed to control snack intake, although our education method of using a small sized rice bowl was effective in lowering dietary energy intake from meals in the OW and the OB groups.
We used a rice bowl that could hold enough rice to provide 200 kcal of energy. Athough a rice bowl of that could hold 200 kcal to 300 kcal per meal was recommended, we chose the 200-kcal size because patients could potentially heap or push more rice in their bowl and exceed its 200-kcal capacity. Because our study only lasted for two weeks, we could not conclude that the education and the smaller rice bowl led to effective energy intake control or clinical outcomes in our participants. In addition, the method, frequency and period of education in this study were different than those other studies that based their education on an ordinary-sized rice bowl, so it was also difficult to determine that using a smaller rice bowl was more effective than using an ordinary-sized rice bowl. Nevertheless, the education plan that we prescribed decreased the carbohydrate proportion of total energy intake regardless of obesity and particularly in the OW and the OB groups. These findings suggest our method's potential effectiveness for overweight and obese patients, and long-term studies will be needed to determine the effect of our education on intake control.
Unlike a previous study that controlled the amount of foods, our education program used a method based on bowl size, and its effect as a plate method had been proven in foreign countries. Pedersen et al. [25] reported that using a smaller plate for meals helped effectively reduce the body weight of women with diabetes, and Diliberti et al. [26] also showed that a small-sized plate decreased total energy intake at restaurants. Athough our short-term study could not observe major changes in body weight after the education program using the smaller bowl, the body weight of the OW and the OB groups was reduced significantly. Further long-term studies on decreased body weight following the use of a smaller rice bowl are necessary.
In conclusion, our education program reduced total energy intake in overweight and obese patients. Our meal education program reduced rice intake effectively so participants could more closely reach the recommended carbohydrate intake. However, because this study was conducted only in a single hospital and its sample size was small, the effects and changes of dietary patterns (such as gender and age) could not be examined. In addition, this study included a three-day dietary record to observe macronutrient intake changes, but it was difficult to evaluate the daily intake of diabetes patients using this record. Dietary records are more effective than recall methods, which have been widely used to survey food intake. Patients using recall methods tend to report a lower intake than was actually consumed due to factors such as decreased memory in elderly patients; however, since the food frequency method is not suitable for investigations on short-term changes, our study used the three-day dietary record [27].
Our study used a two-week study period to examine changes of carbohydrate intake after using a smaller rice bowl, but this short period made it difficult to determine the effect of the rice-bowl-based meal plan. Therefore, additional studies investigating long-term changes using a similar education method are necessary.