Diabetes and Cancer: Cancer Should Be Screened in Routine Diabetes Assessment
Article information

Abstract
Cancer incidence appears to be increased in both type 1 and type 2 diabetes mellitus (DM). DM represents a risk factor for cancer, particularly hepatocellular, hepatobiliary, pancreas, breast, ovarian, endometrial, and gastrointestinal cancers. In addition, there is evidence showing that DM is associated with increased cancer mortality. Common risk factors such as age, obesity, physical inactivity and smoking may contribute to increased cancer risk in patients with DM. Although the mechanistic process that may link diabetes to cancer is not completely understood yet, biological mechanisms linking DM and cancer are hyperglycemia, hyperinsulinemia, increased bioactivity of insulin-like growth factor 1, oxidative stress, dysregulations of sex hormones, and chronic inflammation. However, cancer screening rate is significantly lower in people with DM than that in people without diabetes. Evidence from previous studies suggests that some medications used to treat DM are associated with either increased or reduced risk of cancer. However, there is no strong evidence supporting the association between the use of anti-hyperglycemic medication and specific cancer. In conclusion, all patients with DM should be undergo recommended age- and sex appropriate cancer screenings to promote primary prevention and early detection. Furthermore, cancer should be screened in routine diabetes assessment.
INTRODUCTION
People with diabetes mellitus (DM) have an increased risk of developing a number of serious life-threatening health problems resulting in higher medical care costs, reduced quality of life and increased mortality [1]. The global prevalence of diabetes and impaired glucose tolerance in adults has been increasing over recent decades [2]. This trend has been accompanied by increasing rates of some cancers, leading to a hypothesis that there might be a potential direct relationship between DM and cancer [3]. Cancer is a major life-threatening disease worldwide. The global burden of cancer is expected to grow rapidly due to aging population [4]. In Korea, cancer has been the leading causes of death [5]. It is expected to become more common due to aging and westernized lifestyles [6]. Moreover, malignant neoplasm is the most common cause of death in patients with type 2 diabetes mellitus (T2DM) in Korea [7]. This increased risk of cancer deaths in people with diabetes is also shown in other countries [8]. A link between DM and cancer has been noted for at least 100 years [9]. If causal, these associations might be of great importance for public health given the substantial global burden of these diseases [2]. However, some claimed associations could also be caused by biases in the literature, particularly selective reporting biases that favor the publication of significant associations and cause either false positives or inflated estimates of association [10]. In addition, epidemiologic evidence linking antidiabetic drugs with cancer risk has been suspected during the last several years [1112].
We have previously published a review article about the causal relation between diabetes and cancer in 2011 [13]. In the present review, we updated with the most recent evidences regarding this issue and reinforced the issue of pharmacologic therapy of DM and cancer risk with suggestions.
INCREASED CANCER INCIDENCE IN PATIENTS WITH DIABETES
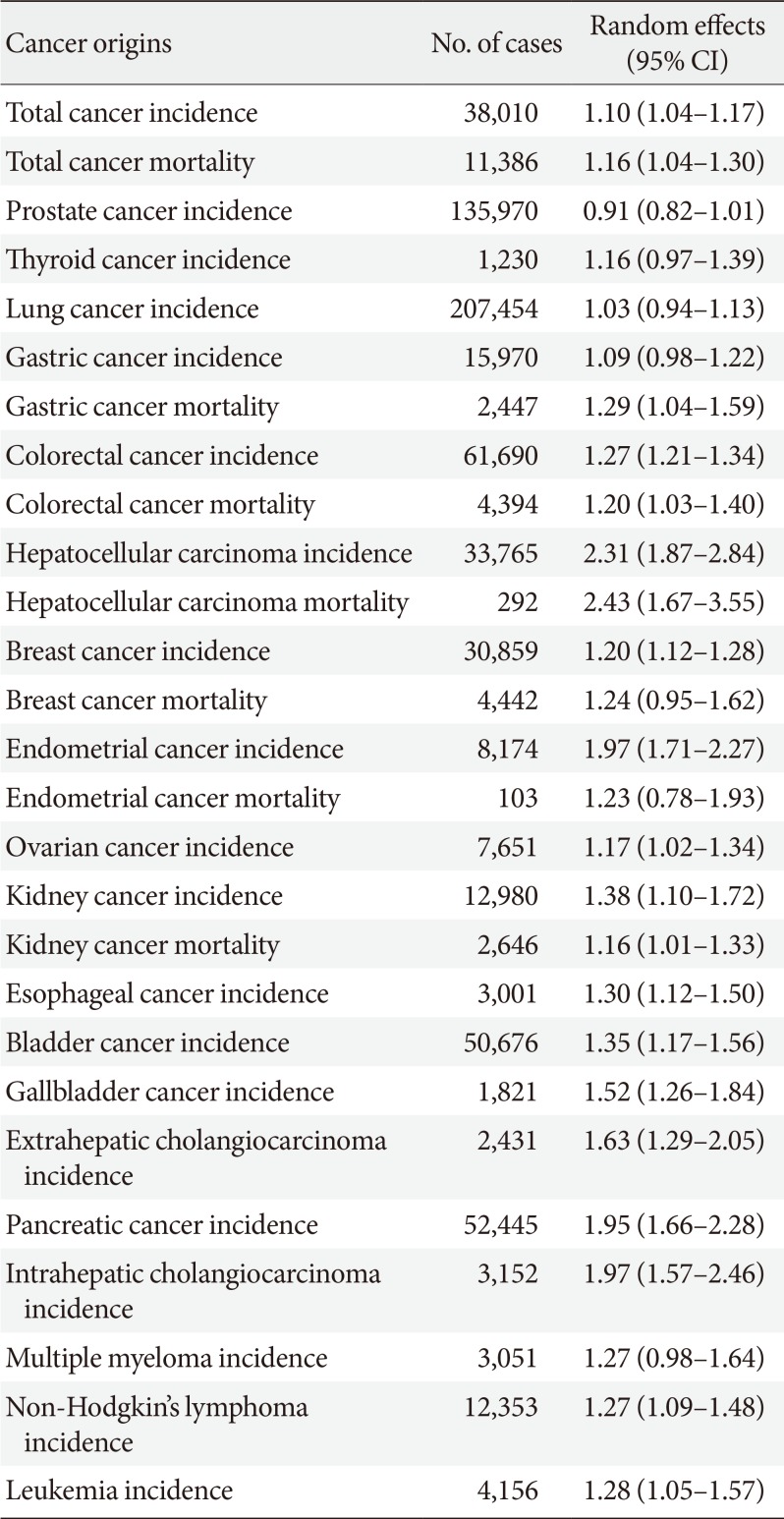
Cancer incidence appears to be increased in both type 1 diabetes mellitus (T1DM) and T2DM [14]. A comprehensive meta-analysis regarding T2DM and risk of developing cancer and mortality has shown that the presence of diabetes is associated with a 10% increase of the relative risk (RR) to develop cancer (RR, 1.10; 95% confidence interval [CI], 1.04 to 1.17) as shown in Table 1 [10]. In that analysis, evidence was substantiated for associations between T2DM and risk of developing hepatocellular, hepatobiliary, pancreas, breast, ovarian, endometrial and gastrointestinal cancers as shown in Table 1. The RR of incidence of all cancer types for Asian men was significantly higher than that for non-Asian men [15]. Since more than 90% of patients with diabetes who are affected by T2DM generally belong to an age group particularly affected by cancer, the association between T2DM and cancer is stronger compared to that between T1DM and cancer [14]. However, significant higher incidence of cancer has also been demonstrated in subjects with T1DM, particularly evident in liver, pancreas, kidney, endometrium, and ovary cancers [16]. Moreover, prediabetes is also associated with an increased risk of cancer, especially liver, endometrial, stomach and colorectal cancers [17].

Random effects estimates with 95% confidence and prediction intervals from 27 meta-analyses of type 2 diabetes mellitus and incidence of cancer or mortality
INCREASED CANCER MORTALITY IN PATIENTS WITH DIABETES
Interestingly, DM could represent an independent risk factor for higher cancer-related mortality, particularly evident for colon, pancreas, and breast cancers in women and for liver and intestine cancers in men [18]. However, since DM is associated with higher mortality than the general population [1920], it is not completely understood whether the higher mortality of patients with diabetes associated with cancer is independent of this factor. Although the relationship between diabetes and cancer-specific mortality is inconsistent [2122], there is emerging evidence that T2DM is associated with an increased risk of death from cancer. A previous meta-analysis has estimated that diabetes is associated with 41% increased risk of death from any cancer [23]. More recent meta-analysis has also found the risk of cancer mortality in patients with T2DM is increased 16% [10] as shown in Table 1. However, most studies on the association between diabetes and cancer risk have been conducted in Western populations [10]. In a recent analysis of 19 Asian cohorts including more than 771,000 participants followed for up to 21 years, diabetes was associated with a 26% increase in the risk of death from any cancer [24] in line with Western studies. T1DM is also associated with an increased risk of overall and site specific cancer incidence and mortality [25]. Specifically, DM is related to an increased risk of death from colorectal cancer, liver cancer, bile duct cancer, gallbladder cancer, pancreatic cancer, breast cancer, endometrial cancer, ovarian cancer, prostate cancer, kidney cancer, thyroid cancer and lymphoma [24]. Another study has also found that cancer patients with DM are frequently treated less aggressively and have a worse prognosis compared to those without diabetes [26]. The association of DM with specific cancers suggests a need for better control (prevention, detection, and management) of the growing epidemic of DM in order to reduce cancer mortality. These findings indicate a potential need for appropriate cancer screening among individuals with DM. However, further research is needed to determine if more stringent management of insulin resistance and hyperglycemia in patients with cancer can improve their response to oncology treatments and overall survival [11].
COMMON RISK FACTORS FOR BOTH DIABETES MELLITUS AND CANCER
DM and cancer represent common health concerns. They often coexist in the same individual. Overall, 8% to 18% of individuals suffering from cancer also have diabetes. The prevalence of cancer in patients with DM varies according to tumor site [27]. The association may result from shared risk factors between T2DM and cancer (older age, obesity, physical inactivity, and smoking) as shown in Table 2. It may also be due to diabetes-related factors, such as underlying disease physiology and diabetes treatments [2829], although evidence for these links is scarce. A recent study using a large database suggested that increases in DM and body mass index (BMI) worldwide could lead to a substantial increase in cancer burden in future decades [29]. Therefore, population-based strategies to prevent DM and high BMI have great potential impact because these two diseases have overlapping risk factors, comorbidities, and shared sequelae, such as cancer [30]. Future efforts should focus on identifying the most effective clinical interventions to prevent the development of DM and obesity in at-risk groups to halt and reverse the rise in DM. In addition, global efforts and clinical guidance should reflect the importance of cancer as a sequela of both DM and obesity. Control measures should also be integrated into clinical guidelines to identify opportunities to reduce morbidity in this group of patients [29].

Common risk factors and biological mechanisms linking diabetes and cancer
POSSIBLE MECHANISMS UNDERLYING DIABETES MELLITUS AND CANCER
Although the mechanistic process that may link diabetes to cancer is not completely understood yet, several experimental observations have suggested how multiple risk factors involving proliferation and apoptosis pathways may be in common between T2DM and cancer [11]. The major risk factors were hyperglycemia [3132], hyperinsulinemia [31], increased bioactivity of insulin-like growth factor 1 (IGF-1) [33], oxidative stress [34], dysregulations of sex hormones, and chronic inflammation [2835] as shown in Table 3. Supraphysiological concentrations of insulin and glycemia to which body tissues are exposed represent a potent growth factor and energy source, respectively. They are essential for neoplastic transformation and cancer progression [34]. Insulin resistance, subsequent hyperinsulinemia (i.e., insulin can promote mitogenic effect on pancreatic cells in vitro), and hyperglycemia have been hypothesized as the biological mechanism that link T2DM to pancreatic cancer incidence [31]. Hyperinsulinemia also has an indirect effect on endometrial, breast and ovarian tissues by increasing endogenous estrogen and androgen levels as well as decreasing plasma levels of sex hormones binding globulin [36]. Moreover, hyperglycemia is responsible for induction of oxidative stress and DNA damage, which may trigger the first phases of tumorigenesis [3738]. Epidemiologic evidence supports the role of insulin and the IGF pathway in cancer incidence. Some cohort studies have described an association between increased levels of IGF-1 and risk of cancer [33]. Furthermore, patients affected by acromegaly, a disorder characterized by excess of growth hormone and IGF-1, have been shown to have increased risks of several types of cancer [39].

Potential risks of anti-hyperglycemic medications and cancer
Interestingly, a recent review showed that adiposity and obesity were associated with several cancers [40]. The excess of weight was associated with increased cancer risk probably by biological pathways that involve hormonal control, cellular proliferation, and inflammation [41]. Similar mechanisms have been hypothesized for the association of T2DM and cancer. In the relationship between T2DM and cancer, obesity can act as an important confounder or as an effect modifier. A previous study estimated that about 3.6% of all cancer cases in 2012 were attributable to obesity [42]. In a recent population study, a substantial number of cancer cases were attributable to diabetes and obesity [29].
The most convincing pathophysiological mechanisms implicated in the association between T2DM with cancer have been proposed for colorectal cancers [3]. In particular, the T2DM microenvironment, represented by advanced glycation end-products, chronic local inflammation, hyperlipidemia, extracellular matrix disorders and altered microbiota could predispose the development of colorectal cancer [3]. The plausibility of these mechanisms was strengthened by a meta-analysis [43] that showed a strong association of markers of glucose metabolism (including fasting glucose, fasting insulin, homeostasis model of risk assessment-insulin resistance, glycated hemoglobin, and C-peptide) with colorectal cancer. Furthermore, a meta-analysis by Yu et al. [44] has suggested that T2DM plays a role also in developing colorectal adenomas, a well-known precursor lesions lesion of colon cancer, demonstrating a role in all the natural history of disease in line with our previous report [45].
Further studies are needed to fully identify mechanisms involved in the reciprocal interaction between diabetes and cancer to prevent additional burden and promote targeted clinical and social prevention strategies. Researchers across diabetes and cancer communities must continue to collaborate, design trials, and explore new and existing databases, especially when outcomes are rare. In addition, editors and readers of the journal must be aware of methodological pitfalls of each study before interpreting its results.
ANTI-HYPERGLYCEMIC MEDICATION AND CANCER
Evidence from both observational and experimental studies suggests that some medications used to treat DM are associated with either increased or reduced risk of cancer [14]. As a result, several anti-hyperglycemic drugs introduced over the last decade have been under surveillance by regulatory agencies for possible increase in tumor incidence. In general, anti-diabetes therapies such as sulfonylureas (SUs) and exogenous insulin associated with hyperinsulinemia have been shown to increase cancer risk while treatments associated with amelioration of insulin resistance such as metformin may reduce this risk [1112]. However, awareness of methodological shortcomings such as prevalent-user bias, detection bias, reverse causality, time-related bias, and residual confounding afflicting most of these previous studies is increasing [14]. As a result, there is currently no definitive evidence for a carcinogenic effect of any anti-diabetic therapeutics. However, given the novelty and benefit of some of these agents and conflicting study results, future well-designed prospective trials are needed to further elucidate their neoplastic or anti-neoplastic effects. Even if the evidence for specific drugs affecting cancer risk is still incomplete, anti-diabetes therapy should not be recognized as a contributing risk factor. Therefore, cancer risk should not be a major factor when choosing between available diabetes therapies for an average patient. Yet, for a selected sub-group of patients exhibiting a history or risk of specific types of cancer, the choice of antidiabetic drug may require more meticulous evaluation.
Sodium glucose cotransporter 2 inhibitors
Sodium glucose cotransporter 2 (SGLT2) inhibitors can lower blood glucose by impairing its renal resorption, thus increasing its urinary excretion. While this strategy results in reduction of hyperglycemia, epithelial cells in nephron segments downstream the renal proximal tubule are exposed to constant glycosuria whose effect remains to be elucidated. A meta-analysis of 46 randomized controlled studies indicated that SGLT2 inhibitors did not significant increase the risk of overall cancer [46]. Accordingly, a post hoc pooled analysis of clinical trials with dapagliflozin showed no significant difference in risk of any type of cancer, including bladder cancer, between treatment and placebo groups [47]. As SGLT2 inhibitors are relatively new in clinical practice, their effects on cancer incidence or mortality cannot be easily assessed in short-term trials or in those with follow-up for a few years. These issues should be further delineated in large-scale, controlled studies with longer duration of follow-up.
Incretin-based drugs
Incretin-based therapy is broadly and increasingly used in T2DM, although some concerns about its effects on carcinogenesis of the pancreas and thyroid have been raised by both preclinical and observational studies [4849]. These new class of drugs went through large-scale clinical trials. There is no evidence that glucagon-like peptide-1 (GLP-1) receptor agonist [50] or dipeptidyl peptidase-4 inhibitors [51] can increase the risk of pancreatic cancer. A meta-analysis of six cardiovascular outcomes trials (CVOTs) has found that the risk of pancreatic cancer in patients on incretin-based is similar to that in patients on other therapies [52]. Concerns about medullary thyroid cancer are due to the observation that GLP-1 receptors are expressed in all thyroid tissues, especially in settings of C-cell hyperplasia and medullary thyroid cancer. Incretin therapy resulted in increased calcitonin levels in rodents but not in primates and humans, who have fewer C-cells and GLP-1 receptor levels [53]. In recent CVOTs, cancer rates did not differ between incretin users and controls. Specifically no thyroid cancers were reported [1449]. As these incretin-based agents are increasingly used in the treatment of T2DM, their potential antineoplastic and procarcinogenic effects must be further addressed in future clinical studies.
Thiazolidinediones
Thiazolidinediones (TZDs) are commonly used as insulin-sensitizers and glucose and lipid-lowering agents in T2DM [54]. In a meta-analysis of randomized trials, TZD was associated with a significantly lower risk of colon cancer and a significant reduction in breast cancer [1255]. However, other clinical studies have failed to corroborate their antineoplastic effect in colorectal [56] and breast cancer [5758]. Until now, the role of TZDs in cancer treatment and prevention is uncertain [11].
On the contrary, there are concerns regarding increased incidence of bladder cancer associated with pioglitazone use. The prospective pioglitazone clinical trial in macrovascular events (PROactive Study) was the first to draw attention to the association of bladder cancer with pioglitazone use in humans [59]. Some observational studies have suggested a possible link between the two. However, there is no association between bladder cancer and pioglitazone in randomized controlled trials (RCTs) [60]. Jin et al. [61] could not find an association between ever use of pioglitazone and bladder cancer in a prevalent case-control analysis nested within a Korean cohort. A prospective study from Kaiser Permanente database has found that pioglitazone use is not associated with increased risk of bladder cancer [62]. Although there is a possible association between bladder cancer and pioglitazone, the causality is not definitely proven considering results from the most recent meta-analysis [63]. These new studies suggest that the association of bladder cancer with pioglitazone might be due to ascertainment bias [64]. Further confirmatory studies are required to answer this question. To be safe, European Medicines Agency advises that risk factors for bladder cancer should be assessed and that pioglitazone should be avoided in patients with a history of bladder cancer, affected by this disease, or with uninvestigated macrohematuria before prescription. Despite concerns regarding bladder cancer, we should remember that TZD has an undoubtable cardiovascular benefit [60].
Sulfonylureas
SUs are among the oldest drug classes available for the treatment of T2DM. SUs act as insulin secretagogues. They are still extensively used in T2DM treatment [54]. A primary data meta-analysis has analyzed 24 metformin studies and 18 SU studies investigating the correlation between antidiabetic drugs and cancer incidence [65]. In this analysis, increased cancer risk emerged only in cohort studies regarding SUs, whereas case-control and RCTs failed to confirm this finding [65]. Accordingly, a retrospective cohort study using data from the registry of the surveillance, epidemiology, and end results (SEER) program of the National Cancer Institute showed that patients on SUs were at higher risk of breast cancer death (hazard ratio, 1.49; 95% CI, 1.00 to 2.23) [66]. However, most of these previous studies bore the burden of time-related biases. When these biases were eliminated, no increased risk of malignancies was detected [14]. Moreover, no evidence of any effect of glipizide or glimepiride, so-called 2nd generation SUs, on tumor growth has been reported [67]. Although SUs have been in clinical use for many years, their associations with cancer remains uncertain [11]. Further and more statistically accurate epidemiological studies are thus required for a better understanding of the link between SUs and cancer.
Metformin
Metformin is the first-line T2DM treatment and reduces hyperglycemia by primarily reducing hepatic gluconeogenesis with subsequent lowering of insulin requirements [54]. A large meta-analysis has shown that metformin may reduce cancer risk and improve the prognosis and survival of cancer patients [68]. These results are complemented by studies in cancer cell lines in vitro and in animal models, in which metformin appears to reduce proliferation of cancer cells [69]. The mechanism underlying protective effects of metformin against cancer initiation has been linked to AMP-activated protein kinase (AMPK) activation, mammalian target of rapamycin (mTOR) inhibition, and concomitant reduction of insulin levels [70]. To date, most in vitro studies and animal models that demonstrate antineoplastic effects of metformin involve doses that are substantially higher than those indicated for treatment of T2DM [71]. Therefore, it is unclear if metformin can exert direct effects on tumors in patients. The possible role of metformin as an antineoplastic agent is being extensively studied and several novel anti-cancer mechanisms have been demonstrated [64]. Although repurposing drugs with excellent safety profiles is an appealing strategy for cancer prevention and treatment in an adjuvant setting, there is no substitute for well-executed, large RCTs to define efficacy and determine populations that are most likely to benefit from metformin prescription [69].
Insulin analogue
Several insulin analogues have been developed aiming at restoring the physiological insulin kinetics and control blood glucose excursions [54]. Studies in cell models comparing the activity of insulin analogues to that of native insulin and exploring insulin receptor and IGF-1 receptor signaling have indicated that minor differences may exist between insulin and short-acting analogues. However, there has been claim that long-acting analogues may activate mitogenic pathways more than insulin, thus increasing cell proliferation [72]. Potential mechanisms by which administration of insulin or insulin analogues might affect neoplastic disease include several aspects [33]: (1) insulin glargine has much higher affinity to the IGF-1 receptor and higher mitogenic potency, than human insulin or other analogues; (2) long-acting analogues have a slower dissociation rate than native insulin (about 1.5 to 3 times longer); and (3) the growth-promoting effect of insulin analogues on malignant cells due to its mitogenic effects. Indeed, despite these therapies are associated with metabolic benefit, some retrospective studies have highlighted an increased risk of cancer within the first years after starting insulin treatment, particularly breast cancer after insulin glargine administration [11, 12]. However, these observational studies had design limitations, making it impossible to draw firm conclusions [73]. In addition, both the outcome reduction with initial glargine intervention (ORIGIN) trial [74] and the ORIGIN and legacy effects (ORIGINALE) study [75] reported neutral effects of insulin glargine on cancers. These large long-term data seemed definitive, leading some commentators to suggest closure on this topic [64]. In addition, a recent multi-country cancer risk and insulin analogues (CARING) project which included 250,000 patients noted no increased risk for development of any cancers with insulin glargine or insulin detemir compared to human insulin with a follow-up exceeding 5 years [76]. Furthermore, it has been more recently clarified that, following in vivo administration in humans, insulin glargine is rapidly and almost completely transformed into active metabolites that have the same mitogenic properties as human insulin [77]. In summary, although in vitro studies have raised concerns regarding mitogenic effects of insulin analogues, particularly glargine, the relevance of these in vitro studies to humans is questionable. To date, there is no strong evidence supporting the association between the use of insulin analogues and cancer [11].
CANCER SCREENING IN PEOPLE WITH DIABETES
We are now aware that patients with DM are at increased risk of several common cancer types compared to the general population. However, this does not translate into a need for more intensive cancer screening in patients with DM. The American diabetes association guidelines recommends that patients with diabetes should be encouraged to undergo recommended age- and sex appropriate cancer screenings and reduce their modifiable cancer risk factors (obesity, physical inactivity, and smoking) [78]. Special attention is needed for those with new onset of atypical diabetes (elderly, having lower premorbid BMI, weight loss and no family history of diabetes) who need screening of pancreatic cancer as we have previously recommended [79]. In Korea, the national cancer screening program was implemented in 1999 by the Korean government as an organized cancer screening program. Opportunistic screenings are also provided depending on individuals' needs [80]. However, in a Korean study using nationwide survey and health examination data, cancer screening rate (both lifetime screening rate and recommended screening rate for gastric, breast, and cervical cancers) was significantly lower in people with DM than that in people without diabetes [81]. Moreover, lower cancer screening rates in older people with DM than in people without diabetes in the same age group, especially regarding recommended screenings for gastric and breast cancer, were observed in that study [81]. Previous studies conducted in Western countries have consistently shown lower cancer screening rates in people with DM [8283], similar to the Korean study. Therefore, advising patients with DM to get these health examinations is of upmost importance. In the future, continuous public health efforts should emphasize the importance of long-term preventive care, including cancer screening, for high-risk populations such as individuals with DM. In addition, future research should focus on cancer screening rate by type and duration of DM and medication used.
CONCLUSIONS
With escalating prevalence of DM, risks of cancer and cancer-related mortality are significantly increased, causing great concern internationally. Diabetes represents a risk factor for cancancer, particularly hepatocellular, hepatobiliary, pancreas, breast, ovarian, endometrial, and gastrointestinal cancers. The association between DM and cancer has important implications for reiterating the importance of controlling lifestyle factors. Thus, cancer should be screened in routine diabetes assessment.
ACKNOWLEDGMENTS
This work was supported by the research fund of Dong-A University, Busan, Republic of Korea.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.