Lower Leg Fat Depots Are Associated with Albuminuria Independently of Obesity, Insulin Resistance, and Metabolic Syndrome (Korea National Health and Nutrition Examination Surveys 2008 to 2011)
Article information

Abstract
Background
Although the involvement of obesity in metabolic disorders is well known, leg fat depot influences on albuminuria have not been determined.
Methods
This population-based, cross-sectional study used a nationally representative sample of 2,076 subjects aged ≥20 years from the Korea National Health and Nutrition Examination Surveys of 2008 to 2011. The ratio of leg fat to total fat (LF/TF ratio) was assessed by dual X-ray absorptiometry, and albuminuria was defined as more than one positive dipstick test or an albumin-to-creatinine ratio of ≥30 mg/g.
Results
Individuals whose LF/TF ratio was in the lowest tertile showed a higher proportion of albuminuria than those in the highest tertile (odds ratio [OR], 2.82; 95% confidence interval [CI], 2.01 to 3.96; P<0.001). This association was observed in both sexes, all age groups, and all subgroups stratified by body mass index, waist circumference, homeostasis model assessments of insulin resistance, and the presence of metabolic syndrome (all, P<0.05). Multiple logistic regression analyses also demonstrated that the lowest LF/TF ratio was independently associated with albuminuria risk (OR, 1.55 to 2.16; all, P<0.05). In addition, the risk of albuminuria was higher in sarcopenic individuals with lower LF/TF ratios than in the highest LF/TF ratio subjects without sarcopenia (OR, 3.73; 95% CI, 2.26 to 6.13).
Conclusion
A lower LF/TF ratio was associated with an increased risk of albuminuria independent of obesity, insulin resistance, and metabolic syndrome, and when combined with sarcopenia, the albuminuria risk synergistically increased. Hence, our findings may have implications to improve risk stratification and recommendations on body fat distribution in the general population.
INTRODUCTION
A rapidly increasing prevalence of obesity has been threatening public health. With increasing body fat, the risk for cardiovascular diseases, nonalcoholic fatty liver disease, and mortality is also increasing [123]. Abdominal obesity is the most well-known fat depot associated with metabolic abnormalities in obesity [4]. In addition, ectopic fat in heart, liver, vessels, and kidney could contribute to cardiometabolic disease risks [5]. In contrast, subcutaneous fat and gluteofemoral fat depots seem to have beneficial effects on metabolism. Compared to visceral adipose tissue, subcutaneous adipose tissue is associated with insulin sensitivity [6], and therefore attenuates cardiovascular disease risk [7]. Furthermore, low thigh fat is linked with impaired glucose and lipid metabolism [8], and cardiometabolic risk components [9]. However, the differential effect of fat distribution and the benefits of leg fat components on metabolic disease have not been fully established.
Albuminuria is a marker for chronic kidney disease progression and could predict mortality and the development of chronic metabolic and cardiovascular disorders [1011]. Generally, albuminuria reflects systemic inflammation and insulin resistance [12]. Therefore, recent investigations have extended the predictive value of albuminuria to other metabolic disorders in clinical studies; individuals with albuminuria have a higher risk for sarcopenia [13], nonalcoholic fatty liver disease [14], and even increased mortality rate [15]. Based on this evidence, we hypothesized that decreased leg fat depot might be related to albuminuria, and conversely, increased lower-body fat distribution might attenuate the risk for albuminuria. Therefore, the aim of the present study was to investigate the independent association of leg fat depot, as measured by its ratio to total body fat, with albuminuria in the general population after adjusting for the potential effects of other established albuminuria risk factors. Furthermore, we evaluated the combined impact of lower leg fat depot and sarcopenia on the risk of albuminuria.
METHODS
Study population
This cross-sectional study extracted participant results from the Korea National Health and Nutrition Examination Surveys (KNHANES) of 2008 to 2011. Each KNHANES is composed of independent data sets from the general population of Korea, similar to the National Health and Nutrition Examination Survey in the United States [14]. As described in Fig. 1, of the 37,753 participants from the KNHANES of 2008 to 2011, we initially selected those aged ≥20 years. Case exclusion criteria were: (1) missing data for body fat measurements based on dual-energy X-ray absorptiometry (DXA); and/or (2) insufficient data for body mass index (BMI); (3) without urinalysis; and (4) with prevalent diabetes. Ultimately, 2,079 subjects (930 males, 1,149 females) were included in the analyses. All participants provided written informed consent and the survey protocol was approved by the Institutional Review Board of the Korean Centers for Disease Control and Prevention (2008-04EXP-01-C, 2009-07CON-03-2C, 2010-02CON-21-C, and 2011-02CON-06C).

Flow diagram of a study population in the Korean National Health and Nutrition Examination Surveys (KNHANES IV and V). DXA, dual-energy X-ray absorptiometry; BMI, body mass index.
Measurement of clinical and laboratory parameters
KNHANES data included the participants' medical history, nutritional status, and laboratory test results. Medical history included smoking habits, alcohol consumption, exercise level, and disease diagnosis and/or treatment status, based on direct interviews and self-reporting. Regular exercise was defined as that lasting more than 20 minutes per session and at least three times per week (e.g., running, jogging, mountain climbing, fast cycling, fast swimming, playing soccer, playing basketball, playing squash or singles tennis, or transporting heavy objects). Blood sample was assessed as a single measurement and blood pressure was manually measured using mercury sphygmomanometers (Baumanometer; W.A. Baum, Copiague, NY, USA) three times on the right arm in a resting, seated position, and final blood pressure values were calculated by averaging the second and third blood pressure readings. Overnight (at least 8 hours) fasting blood and spot urine samples were collected, refrigerated, and transported to a central laboratory (NeoDin Medical Institute, Seoul, Korea) within 24 hours of collection. Blood glucose, total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), triglyceride (TG), aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen, and creatinine were measured using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). Low density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald formula [LDL-C (mmol/L)=TC (mmol/L)−HDL-C (mmol/L)−TG (mmol/L)/2.17] if the TG level was low (≤4.4 mmol/L [400 mg/dL]) and measured directly using the Hitachi 7600 analyzer if the TG level was high (>4.4 mmol/L). Urinary albumin was measured using the turbidometric method (Roche, Mannheim, Germany) and urinary creatinine was determined using the Jaffe rate-blanked and compensated method (Wako, Osaka, Japan) with a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan).
Body fat assessment and clinical risk factor confirmation
Body fat and muscle mass were measured using DXA (QDR 4800A; Hologic Inc., Bedford, MA, USA). Leg fat was the sum of both legs from the thigh to the calf, and the ratio of leg fat to total fat (LF/TF) was categorized into sex-specific tertiles. Sarcopenia was defined according to the Consensus Report of the Asian Working Group for Sarcopenia, and appendicular muscle mass was divided according to height with a cutoff <7.4 kg/m2 for males and <5.6 kg/m2 for females [16]. Participants were considered obese when their BMI was ≥25 kg/m2 according to the Asian-Pacific regional criteria [17]. Central obesity was based on the waist circumference adopted cutoff for the Korean population: ≥90 cm for males and ≥85 cm for females [18]. Impaired fasting glucose (IFG) was characterized by fasting blood glucose ≥100 mg/dL but <126 mg/dL. Undiagnosed diabetes mellitus (DM) was defined based on fasting plasma glucose ≥126 mg/dL according to the American Diabetes Association guideline [913192021]. Individuals were considered to have hypertension (HTN) if their systolic/diastolic blood pressure was ≥140/90 mm Hg, or who were self-reported to take anti-hypertensive medications [91322] and uncontrolled HTN identification was determined according to the guidelines [23]. Metabolic syndrome was identified based on the modified National Cholesterol Education Program Adult Treatment Panel III criteria adopted for the Korean population [24]. Albuminuria was defined as more than one positive dipstick test or ≥30 mg/g urine albumin-to-creatinine ratio [25]. Estimated glomerular filtration rates (eGFR) were calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [26]. The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as followings: fasting glucose (mg/dL)×fasting insulin (µIU/L)/405, and insulin resistance was characterized by a HOMA-IR cutoff of 2.5 [27].
Statistical analyses
Data are presented as the mean±standard deviation, number, or percent. We analyzed the study participants' characteristics according to LF/TF ratio tertiles, using one-way analysis of variance (ANOVA) to compare continuous variables and chi-square tests for categorical variables, followed by post hoc analyses with the Bonferroni method. To evaluate the association of LF/TF ratio and albuminuria, the effects of comorbidities must be minimized. Therefore, subjects were divided according to age, obesity (BMI ≥25 kg/m2), central obesity, metabolic syndrome, insulin resistance, HTN, IFG, and diabetes, then chi-square tests were applied for each group. To assess the effect of elevated LF/TF ratios in the presence of sarcopenia, the highest LF/TF ratio tertile group was compared against lower LF/TF tertiles, including both the lowest and second tertile groups (T1&T2). In addition, we compared the prevalence of albuminuria in 1:1 (T3:T1&T2) matched subgroup analysis using propensity score. The covariates include sex, age, BMI, glucose, HTN, hyper LDL-C, and hypertriglyceridemia (based on the individual's LDL-C goals recommend by the 2004 update of the Adult Treatment Panel [ATP] III guidelines, serum TGs ≥150 mg/dL, or current use of cholesterol/TG lowering agents). Multiple logistic regression analyses were used to assess the independent association between LF/TF ratio and albuminuria risk, including other covariates. As TG, HDL-C, LDL-C, AST, ALT, insulin, HOMA-IR, and urine albumin-creatinine ratio values were not normally distributed, analyses were performed using log- and back-transformed data. Statistical analyses were performed using IBM SPSS version 24.0 for Windows (IBM Corp., Armonk, NY, USA). P<0.05 was considered statistically significant.
RESULTS
Participants' clinical characteristics by ratio of leg fat to total fat
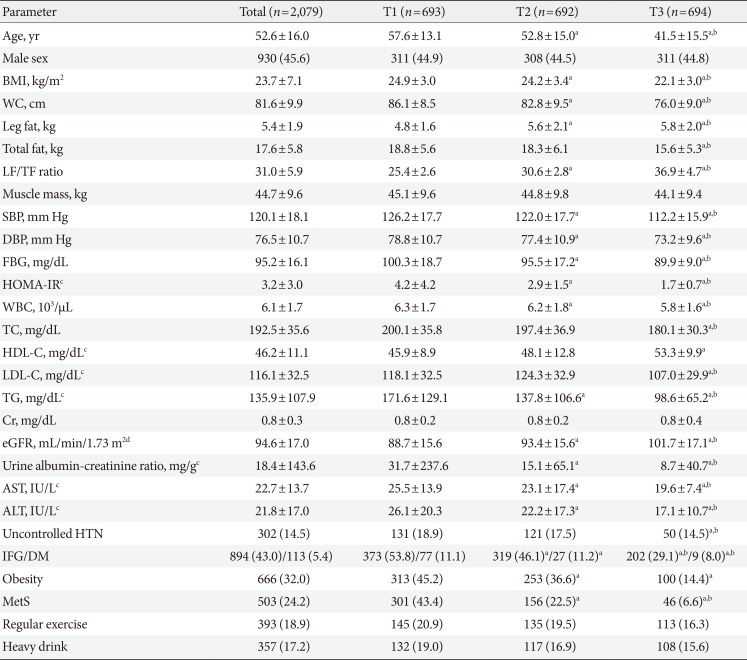
Of 37,753 participants in the KNHANES of 2008 to 2011, a total of 2,079 individuals were eligible in the present study (Fig. 1). The baseline characteristics of the study subjects by LF/TF ratio tertiles are presented in Table 1. The mean age of the study population was 52.6±6.0 years, the mean BMI was 23.7±7.1 kg/m2, and the mean LF/TF ratio was 31.0±5.9. Individuals with a higher LF/TF ratio had better metabolic conditions: lower BMI, lower waist circumference, lower blood pressure, better glycemic parameters (serum glucose concentration, insulin, and HOMA-IR), a decreased lipid panel (LDL-C and TG), and higher HDL-C. Additionally, serum creatinine levels were similar among the groups, while mean eGFR was increased the most in the highest LF/TF ratio group. Subsequently, a low prevalence of HTN, diabetes, metabolic syndrome, and chronic kidney disease were observed in the highest LF/TF ratio tertile group. Although the highest LF/TF ratio group reported a lower incidence of alcohol drinking, they did not seem to have healthier lifestyles in regards to exercise and smoking.

Study population baseline characteristics by the ratio of leg fat to total fat
A lower ratio of leg fat to total fat is associated with albuminuria
The prevalence of albuminuria was 13.3% (276 of 2,079) in the overall study population. Albuminuria showed a strong negative correlation with the LF/TF ratio (18.9% vs. 13.3% vs. 7.6% from the lowest LF/TF ratio group to the highest LF/TF ratio group, respectively; P<0.001) (Fig. 2A). This tendency was maintained in both sexes (19.9% vs. 13.3% vs. 8.0%; P<0.001 for males; and 18.1% vs. 13.3% vs. 7.3%, P<0.001 for females), and a similar prevalence of albuminuria was observed in males (13.8% vs. 12.9% for males and females; P=0.559). The association between albuminuria and LF/TF ratio was strong in all age groups with a striking prevalence of albuminuria in aged individuals (over age 65 years) with the lowest LF/TF ratio (18.8%) (Fig. 2B).
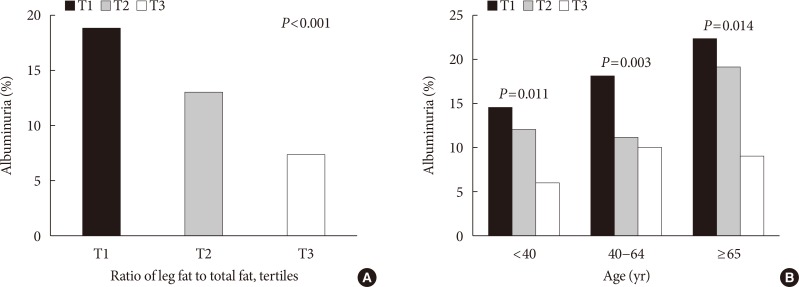
Differences in the prevalence of albuminuria according to the ratio of leg fat to total fat (LF/TF ratio). (A) Albuminuria prevalence by LF/TF tertiles, and (B) the association between albuminuria prevalence and LF/TF ratio by age groups. The black bars represent the lowest LF/TF ratio group, gray bars represent the 2nd lowest LF/TF ratio group, and the white bars represent the highest LF/TF ratio group.
Because obesity, metabolic syndrome, and insulin resistance are all well-established risk factors for albuminuria, we examined the independent association between albuminuria and the LF/TF ratio after stratification by these comorbidities. The prevalence of albuminuria was higher in the obesity, central obesity, insulin resistance, metabolic syndrome, HTN, and impaired glucose groups than in the normal population (17.4% vs. 11.3%, P<0.001 for obesity; 16.3% vs. 11.5%, P=0.002 for central obesity; 57.2% vs. 42.8%, P<0.001 for metabolic syndrome; 14.5% vs. 12.1%, P=0.114 for insulin resistance; 35.4% vs. 9.5%, P<0.001 for uncontrolled HTN; and 14.3% vs. 12.3%, P=0.001 for IFG/undiagnosed diabetes). Interestingly, the lowest LF/TF ratio was associated with an increased risk of albuminuria, regardless of comorbidities in subgroup analysis (Fig. 3). In the obese group, the prevalence of albuminuria decreased from the lowest LF/TF ratio group to the highest LF/TF ratio group (21.4% vs. 17.0% vs. 6.0%, P=0.001) and even in the non-obese group, the lowest LF/TF ratio was associated with a higher prevalence of albuminuria (16.8% vs. 11.3% vs. 7.9%, P<0.001). A similar trend was also observed regarding the status of central obesity (18.7% vs. 16.7% vs. 4.5%, P=0.005 for central obesity; 18.8% vs. 11.0% vs. 8.1%, P<0.001 for non-central obesity), metabolic syndrome (25.6% vs. 25.0% vs. 4.3%, P=0.015 for metabolic syndrome; 13.8% vs. 9.9% vs. 7.9%, P=0.003 for non-metabolic syndrome), insulin resistance (20.6% vs. 14.0% vs. 6.0%, P<0.001 for insulin resistance; 17.1% vs. 11.9% vs. 8.4%, P<0.001 for insulin sensitivity), uncontrolled HTN (40.5% vs. 37.2% vs. 18.0%, P=0.011 for uncontrolled HTN; 13.9% vs. 8.2% vs. 6.8%, P<0.001 for normotension/controlled HTN), and impaired glucose (19.3% vs. 12.1% vs. 7.1%, P<0.001 for IFG/DM; 18.1% vs. 14.5% vs. 7.9%, P<0.001 for normoglycemia). Among those comorbidities, subjects with metabolic syndrome and the lowest LF/TF ratio had the greatest risk of albuminuria (odds ratio [OR], 7.56; 95% confidence interval [CI], 1.79 to 31.94; P=0.006) compared to subjects with the highest LF/TF ratio (Table 2). Besides metabolic syndrome, individuals with the lowest LF/TF ratio and central obesity had the second highest albuminuria risk (OR, 4.84; 95% CI, 1.72 to 13.64; P=0.003) and individuals with the lowest LF/TF ratio and obesity followed (OR, 4.27; 95% CI, 1.72 to 10.17; P<0.001). Moreover, individuals with the lowest LF/TF ratio even without these comorbidities had comparable albuminuria risks ([OR, 2.36; 95% CI, 1.58 to 3.52; P<0.001 for non-obesity]; [OR, 2.64; 95% CI, 1.76 to 3.97; P<0.001 for non-central obesity]; [OR, 2.25; 95% CI, 1.45 to 3.48; P<0.001 for insulin sensitivity]; [OR, 2.20; 95% CI, 1.49 to 3.24; P<0.001 for normotension/controlled HTN]; and [OR, 2.59; 95% CI, 1.63 to 4.12; P<0.001 for normoglycemia]).

Differences in the prevalence of albuminuria after comorbidity stratification. (A) Obesity defined by a body mass index ≥25 kg/m2, (B) central obesity defined by waist circumference ≥90 cm for males and ≥85 cm for females, (C) metabolic syndrome, (D) insulin sensitivity defined by the homeostasis model assessment of insulin resistance (HOMA-IR) <2.5 and insulin resistance defined by HOMA-IR ≥2.5, (E) uncontrolled hypertension (HTN), and (F) impaired fasting glucose (IFG) and diabetes mellitus (DM). The black bars represent the lowest ratio of leg fat to total fat (LF/TF ratio) group, gray bars represent the 2nd lowest LF/TF ratio group, and the white bars represent the highest LF/TF ratio group.

Risk of albuminuria by the ratio of leg fat to total fat and other comorbidities
A lower ratio of leg fat to total fat is independently associated with the risk of albuminuria
To assess the association between LF/TF ratio and albuminuria risk independent of other covariates, we performed multiple logistic regression analyses (Table 2). In the basic model adjusted for age and sex (Model 1), the lower LF/TF ratio significantly raised the risk of albuminuria ([adjusted OR, 1.53; 95% CI, 1.06 to 2.21; P=0.023 for the second lowest LF/TF ratio group]; [adjusted OR, 2.16; 95% CI, 1.50 to 3.10; P<0.001 for the lowest LF/TF ratio group]). This association remained even after adjusting for life style factors that could affect albuminuria, including alcohol drinking, smoking, and exercise (Model 2: [adjusted OR, 1.51; 95% CI, 1.04 to 2.18; P=0.030 for the second lowest LF/TF ratio group]; [adjusted OR, 2.11; 95% CI, 1.47 to 3.04; P<0.001 for the lowest LF/TF ratio group]). After adding a sequential adjustment for demographical and laboratory confounding covariates such as BMI, waist circumference, systolic blood pressure, fasting plasma glucose, eGFR, HOMA-IR, AST, ALT, and TC (Model 3), individuals with lower LF/TF ratios were found to have significantly higher adjusted ORs for albuminuria risk (adjusted OR, 1.55; 95% CI, 1.02 to 2.36; P=0.041) compared to the subjects with the highest LF/TF ratio.
Lower leg fat depots and sarcopenia synergistically increase the risk of albuminuria
Because we previously found that albuminuria was associated with sarcopenia [13], the association among body fat distribution, muscle mass, and albuminuria was investigated. More prominent albuminuria prevalence was observed in the sarcopenic group (16.6% vs. 12.4%, P=0.030). In both the non-sarcopenic and sarcopenic populations, a low LF/TF ratio was significantly associated with albuminuria (28.3% vs. 17.4% vs. 10.6%, P<0.001 for non-sarcopenia; 17.5% vs. 12.3% vs. 6.5%, P<0.001 for sarcopenia) (Fig. 4A). Group comparisons were conducted according to the presence of sarcopenia and the LF/TF ratio. The proportions of albuminuria gradually increased in sequence among the four groups, with the highest albuminuria prevalence in the sarcopenic individuals with a lower LF/TF ratio (28.3% vs. 17.5% vs. 13.3% vs. 9.6%, P<0.001) (Fig. 4B). Sarcopenic participants with a lower LF/TF ratio had a more than five-fold increased OR compared with the non-sarcopenic and higher LF/TF ratio subjects (OR, 3.73; 95% CI, 2.26 to 6.13; P<0.001).
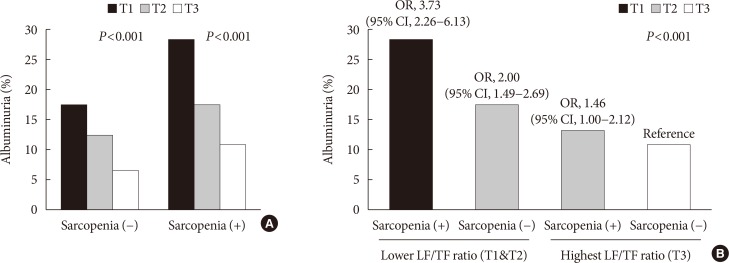
Differences in the prevalence and risk of albuminuria according to the lowest ratio of leg fat to total fat (LF/TF ratio) and sarcopenia. (A) LF/TF ratio by sarcopenia, and (B) sarcopenia and LF/TF ratio combination. OR, odds ratio; CI, confidence interval.
Propensity matching in subgroup analysis
We further performed subgroup analysis by using propensity matching. As shown in Table 3, of 402 subjects, the mean age of the subgroup population was 46.2±13.9 years, the mean BMI was 22.9±2.4 kg/m2, and the mean LF/TF ratio was 32.9±5.4. There was no significant differences between those two groups regarding metabolic and geographic condition except leg fat mass, fasting blood glucose, TC, TG, and ALT. Individuals with the highest LF/TF ratio had a lower urine albumin to creatinine ratio (12.3±50.6 mg/g vs. 5.0±18.5 mg/g, P<0.001).

Baseline characteristics in propensity score matching subgroup by the ratio of leg fat to total fat
The logistic regression models also showed the similar results; the lower LF/TF ratio significantly raised the risk of albuminuria (adjusted OR, 3.39; 95% CI, 1.22 to 9.44; P=0.019) in crude model. After sequential adjustment for confounding covariates such as age, sex, smoking, alcohol, exercise, BMI, waist circumference, systolic blood pressure, fasting blood glucose, HOMA-IR, AST, ALT, and TC, individuals with a lower LF/TF ratios were found to have significantly higher adjusted ORs for albuminuria risk (OR, 4.03; 95% CI, 1.37 to 11.87; P=0.012) compared to subjects with the highest LF/TF ratio (Table 4).

Risk of albuminuria by the ratio of leg fat to total fat and other comorbidities in propensity score matching subgroup
DISCUSSION
This nationally representative, population-based study clearly showed that subjects with a low LF/TF ratio had an increased risk of albuminuria compared with high LF/TF individuals, which was independent of obesity, central obesity, metabolic syndrome, HTN, diabetes, and insulin resistance. A low LF/TF ratio contributed to a more substantial risk of albuminuria in participants with the comorbidities. Moreover, sarcopenia and a low LF/TF ratio synergistically enhanced the risk of albuminuria. The association between LF/TF ratio and albuminuria risk remained significant after adjusting for other confounding factors.
Obesity is a well-known risk for chronic kidney disease. Like other chronic diseases, such as diabetes, HTN, and metabolic syndrome, visceral adiposity has a close relationship to chronic kidney disease [2829]. The associations between body fat distribution and kidney disease were reported in the Framingham cohort study. The kidney ectopic fat depot, referred to as renal sinus fat, had a 2.3-fold increased chronic kidney disease risk, which persisted after adjustment for BMI and visceral fat mass [30]. Conversely, a high BMI was linked with better survival among patients with end-stage renal disease. In dialysis patients, the survival rate and BMI showed a positive correlation, called the reverse epidemiology or obesity paradox [31]. A recent study of the obesity prevalence in hemodialysis patients showed that overtly obese patients (BMI ≥30 kg/m2) had higher fat stores and were better nourished, supporting the obesity paradox [32]. In addition, the BMI based obesity cutoff misdiagnosed the excess fat, while skinfold thickness reflected more precise fat distribution [32]. Considering that skinfold thickness mainly assesses the subcutaneous fat mass, the subcutaneous fat depot could be an important key in the obesity paradox. Our result that a high LF/TF ratio attenuated albuminuria risk in the obese population also provides epidemiological evidence to support the obesity paradox.
The role of fat depots differs from their distributions. Compared to visceral fat, subcutaneous fat in the gluteofemoral area has a low lipolysis rate, fatty acid uptake, and a high adiponectin concentration [3334]. In addition, visceral fat correlated with insulin resistance, whereas the subcutaneous fat depot determined the circulating leptin concentration, and this phenomenon was observed in both lean and obese individuals [35]. In lipodystrophy, loss of extremities adipose tissue and accumulated ectopic fat, insulin resistance is one of the main phenotype [33]. Plasminogen activator inhibitor-1 (PAI-1) expression, which involves vascular damage and cardiovascular diseases, was more enhanced in visceral adipose tissue than subcutaneous adipose tissue [36]. Moreover, PAI-1 expression in femoral subcutaneous fat areas was not associated with plasma PAI-1 levels, while abdominal subcutaneous PAI-1 expression positively correlated with plasma PAI-1 concentrations [37]. Additionally, the development of albuminuria is partly accounted for endothelial dysfunction which could be accelerated by the production of inflammatory cytokines and those are more secreted from visceral fat than gluteofemoral fat [38]. In insulin resistance status, mitochondrial reactive oxygen species is observed in adipose tissue, especially visceral fat [39], while gluteofemoral adipose tissue seems to secret less pro-inflammatory molecules and more favorable adipokines [33]. We previously demonstrated that the LF/TF ratio was superior in predicting high atherosclerotic cardiovascular disease risk among various anthropometric parameters [9]. In the same context, our current study clearly showed that a higher LF/TF ratio was inversely associated with albuminuria risk. Because albuminuria is an early stage of inflammation and a premature stage of vascular damage [40], it is plausible that a low LF/TF ratio reflects the systemic deterioration state and may require close follow-up to detect early chronic kidney disease.
Interestingly, sarcopenic individuals with lower LF/TF ratios had more abundant albuminuria prevalence. Sarcopenia per se is a risk factor for albuminuria [13], and when it is combined with a lower LF/TF ratio, the risk of albuminuria could be strikingly increased. Even in subjects without sarcopenia, the prevalence of albuminuria could be increased if their LF/TF ratio was lower. In addition, in the current study, the LF/TF ratio was associated with albuminuria independently of sarcopenic status. This implies that lower-body fat depots could be as important as the loss of muscle mass, and decreased leg fat mass and muscle may exert synergistic effects on metabolic conditions. There are some evidences of the mitochondrial dysfunction linked with albuminuria and this association is related to both adipose tissue and skeletal muscle [41]. When disoriented mitochondrial function increases reactive oxygen species in adipose tissue, the mitochondrial H2O2 emission is enhanced in skeletal muscle [42]. Moreover, antioxidants could restore insulin sensitivity in skeletal muscle through attenuating mitochondrial H2O2 emission [43].
The current study had several strengths. First, we analyzed a large, nationally representative population; thus our results guaranteed statistical reliability. The KNHANES represents the non-institutionalized general population of Korea; therefore, selection bias was minimized. Second, this investigation provided strong evidence of a close relationship between the LF/TF ratio and albuminuria by adjusting for other essential confounders. Third, the association between LF/TF ratio and albuminuria were still found in the propensity score matching analysis. To our knowledge, the current study is the first to clearly demonstrate the relationship between albuminuria and LF/TF ratio.
This study also has some limitations. First, the cross-sectional study design was insufficient to establish a causal relationship between LF/TF ratios and albuminuria. In addition, medication information, which could affect albuminuria (e.g., renin-angiotensin system inhibitors), was not considered in our analyses due to the lack of relevant data in the KNHANES. Although we excluded patients diagnosed diabetes, minimizing the effect of anti-diabetic medication on albuminuria, we could not account for anti-hypertensive medication, therefore, the detailed interaction between LF/TF and albuminuria should be investigated in future studies with refined participants. Moreover, HbA1c was not provided in patients without previous prevalent diabetes, we only accounted the fasting plasma glucose value for incident diabetes diagnosis. Finally, we performed analysis applying the sample weights. However, we analyzed nationwide data which represents general population and it is impossible to include the entire population in one dataset.
In summary, the results of our current study showed that the LF/TF ratio was significantly associated with albuminuria, independently of insulin resistance, metabolic syndrome, obesity, and other metabolic conditions. The LF/TF ratio could provide a key to the obesity paradox, and may be a modifiable risk factor for albuminuria. Sarcopenic individuals with lower LF/TF ratios could have a remarkably increased risk of albuminuria, and may need reinforced risk assessment. More prospective and longitudinal studies are warranted to establish the LF/TF ratio cutoff and identify mechanisms underlying the link between regional body fat distribution and albuminuria.
ACKNOWLEDGMENTS
The authors are very grateful to the individuals who conducted the KNHANES.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS:
Conception or design: E.H., H.S.K.
Acquisition, analysis, or interpretation of data: E.H., N.H.C., M.K.K.
Drafting the work or revising: E.H., H.S.K.
Final approval of the manuscript: E.H., N.H.C., M.K.K., H.S.K.