Screening for Prediabetes and Diabetes in Korean Nonpregnant Adults: A Position Statement of the Korean Diabetes Association, 2022
Article information
 , Dae Jung Kim2, Kyungdo Han3, Suk Chon4, Min Kyong Moon,5, on Behalf of the Committee of Clinical Practice Guideline of Korean Diabetes Association
, Dae Jung Kim2, Kyungdo Han3, Suk Chon4, Min Kyong Moon,5, on Behalf of the Committee of Clinical Practice Guideline of Korean Diabetes AssociationAbstract
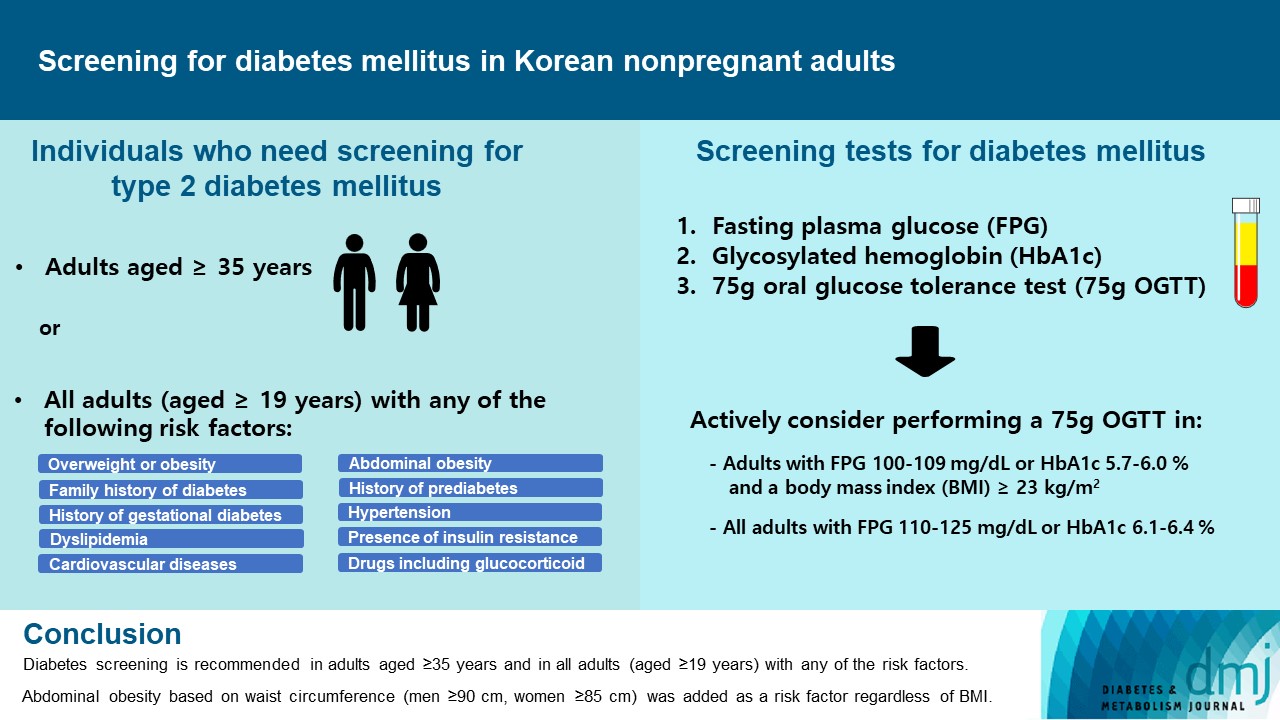
Diabetes screening serves to identify individuals at high-risk for diabetes who have not yet developed symptoms and to diagnose diabetes at an early stage. Globally, the prevalence of diabetes is rapidly increasing. Furthermore, obesity and/or abdominal obesity, which are major risk factors for type 2 diabetes mellitus (T2DM), are progressively increasing, particularly among young adults. Many patients with T2DM are asymptomatic and can accompany various complications at the time of diagnosis, as well as chronic complications develop as the duration of diabetes increases. Thus, proper screening and early diagnosis are essential for diabetes care. Based on reports on the changing epidemiology of diabetes and obesity in Korea, as well as growing evidence from new national cohort studies on diabetes screening, the Korean Diabetes Association has updated its clinical practice recommendations regarding T2DM screening. Diabetes screening is now recommended in adults aged ≥35 years regardless of the presence of risk factors, and in all adults (aged ≥19) with any of the risk factors. Abdominal obesity based on waist circumference (men ≥90 cm, women ≥85 cm) was added to the list of risk factors.
INTRODUCTION
In 2021, the global prevalence of diabetes mellitus in those aged 20 to 79 years was approximately 10.5%, which is expected to increase to 12.2% by 2045 [1]. According to the diabetes fact sheet (DFS), the estimated prevalence of diabetes in Korean adults aged ≥30 years increased from 13.8% in 2018 to 16.7% in 2020 [2,3]. As many people with type 2 diabetes mellitus (T2DM) have no specific symptoms, a significant number of patients are unaware of their condition, and cases frequently go undiagnosed until complications occur [4]. According to the 2021 International Diabetes Federation Diabetes Atlas, approximately one in two adults (aged 20 to 79 years) with diabetes was unaware of their diabetes status (44.7%, 239.7 million) [5]. In Korea, from 2019 to 2020, 34.2% of people with diabetes were unaware of their condition [2]. Therefore, screening for diabetes and prediabetes is essential in high-risk populations.
With the accumulated evidence from clinical studies, the Clinical Practice Guidelines Committee of the Korean Diabetes Association (KDA) has regularly updated the clinical guidelines for the diagnosis, treatment, and management of diabetes since the publication of the first edition last 1995. However, until the seventh edition in 2021, the screening criteria were minorly revised without changing the screening age [6]. Diabetes screening were previously recommended annually in adults aged ≥40 years regardless of the presence of risk factors and in adults aged ≥30 years with any of the risk factors [6]. However, it has recently been reported that the prevalence of obesity and/or abdominal obesity, which are major risk factors for diabetes, as well as diabetes has increased in adolescents and young adults [2,7-9]. Therefore, in this review, the Clinical Practice Guidelines Committee of the KDA presents a position statement on the screening of diabetes and the current evidence.
DIABETES SCREENING POLICIES IN DIFFERENT COUNTRIES
Age is one of the most well-known major risk factors for T2DM, and most diabetes treatment guidelines suggest age criteria for screening (Table 1) [6,10-15]. For instance, diabetes screening is recommended for individuals aged ≥45 years in the American Association of Clinical Endocrinology guidelines, and for individuals aged ≥40 years in the United Kingdom, Canada, and Australia [11,13-15]. Additionally, guidelines in the United Kingdom and Canada have suggested that the age at screening should be decreased for high-risk ethnic groups, including Asians [13,14]. Recently, the recommended age for diabetes screening has changed. The US Preventive Services Task Force recommends screening for prediabetes and T2DM in adults aged 35 to 70 years who are overweight or obese [12]. The screening age limit was lowered from 40 years in 2015 to 35 years in 2021. The American Diabetes Association (ADA) also changed the universal screening age from 45 to 35 years in their 2022 guideline [10]. The Australian Diabetes Society recently published a consensus statement on T2DM screening in young adults (aged 18 to 30 years) [16]. In this statement, screening for diabetes in young adults who are overweight or obese and with additional risk factors, including in utero exposure to T2DM or gestational diabetes mellitus, was recommended [16].

Recommendations for screening for diabetes and prediabetes in asymptomatic adults
In addition, although there are slight differences in each of the diabetes screening policies among different countries and organizations, various diabetes risk factors are suggested, and screening tests are recommended early if relevant risk factors are present (Table 1). As another method of identifying high-risk groups for diabetes, several prediction models for incident T2DM using modifiable and non-modifiable risk factors have also been suggested [17]. In Korea, clinical risk scores for predicting the risk of diabetes were developed based on the Korean National Health and Nutritional Examination Survey (KNHANES), encompassing adults aged ≥20 years, and the Anseong and Ansan cohort data, calculated based on data from adults aged ≥40 years [17,18].
CHANGES IN THE PREVALENCE OF DIABETES AND OBESITY IN KOREAN YOUNG ADULTS
In Korea, the prevalence of diabetes and prediabetes is rapidly increasing, among people aged <40 years. According to DFS, the estimated prevalence of diabetes in individuals aged 30 to 39 years increased, from 3.1% in men and 2.1% in women in 2014 to 3.7% in men and 2.7% in women in 2018 [3,19]. During the same period, the estimated prevalence of impaired fasting glucose increased from 20.0% in men and 11.2% in women to 22.9% in men and 11.4% in women (Fig. 1A) [3,19]. In the 2021 DFS, the prevalence of diabetes in people aged 19–29 and 30–39 years was 0.7% and 4.4%, respectively and the prevalence of prediabetes, defined by fasting plasma glucose (FPG) or glycosylated hemoglobin (HbA1c) criteria, was 16.6% and 30.8% in the same age groups, respectively [2]. However, awareness of diabetes is relatively low in the young adult population compared to the elderly [2].
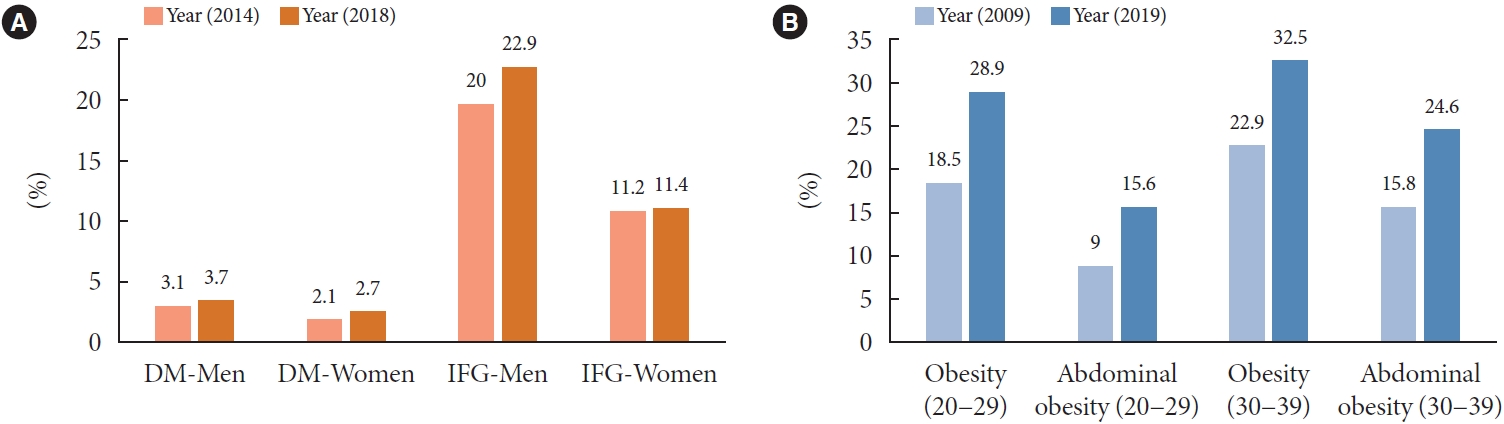
(A) Prevalence of diabetes and prediabetes in people aged 30 to 39 years from 2014 to 2018 and (B) prevalence of obesity and abdominal obesity in people aged 20 to 39 years from 2009 to 2019 in Korea. Obesity defined as body mass index ≥25 kg/m2 and abdominal obesity defined as waist circumference ≥90 cm and ≥85 cm in men and women, respectively. DM, diabetes mellitus; IFG, impaired fasting glucose.
In a recent national cohort study analyzing data from the National Health Insurance Service-National Sample Cohort (NHIS-NSC) from 2006 to 2015, there was an increased incidence of diabetes in the 20–29 and 30–39 years age groups, by 0.5 to 0.7 and 2.0 to 2.6 per 1,000 individuals, respectively [8]. Notably, the prevalence of obesity among adults aged 20 to 40 years with diabetes significantly increased from 51.4% in 2006 to 72.4% in 2015 [8].
A sedentary lifestyles and increase in obesity and/or abdominal obesity rates are major contributing factors. According to an obesity fact sheet of the Korean Society for the Study of Obesity, the prevalence of obesity and abdominal obesity has increased for the entire population over the past 11 years (2009 to 2019: obesity from 29.7% to 36.3% and abdominal obesity from 19.3% to 23.9%), particularly in individuals in their 20s (2009 to 2019: obesity from 18.5% to 28.9% and abdominal obesity from 9.0% to 15.6%) and 30s (2009 to 2019: obesity from 22.9% to 32.5% and abdominal obesity from 15.8% to 24.6%) (Fig. 1B) [9].
Similarly, the prevalence of dyslipidemia in younger age groups is high in Korea. The mean prevalence of dyslipidemia in 2016 to 2020 among individuals in their 20s (defined as low density lipoprotein cholesterol ≥160 mg/dL or the use of a lipid-lowering drug, triglycerides ≥200 mg/dL, or hypo-high density lipoprotein cholesterolemia [<40 mg/dL in men and <50 mg/dL in women]) was 25.4% and 26.0% in men and women, respectively [20]. In the same period, the prevalence among those in their 30s was 41.4% for men and 34.6% for women, which was higher than those people in their 20s [20]. Therefore, it is necessary to consider diabetes screening in individuals aged 20s and 30s.
SCREENING FOR DIABETES IN ASYMPTOMATIC KOREAN ADULTS: A NEW ESTIMATE OF THE NUMBER NEEDED TO SCREEN TO DETECT DIABETES
In 2021, the KDA recommended annual diabetes screening for adults aged ≥40 and ≥30 years with risk factors such as overweight or obesity [6]. However, the age thresholds for screening individuals were determined based on expert opinions, considering the guidelines of other countries, while the evidence for Koreans was limited. The only evidence available, as a result of a pooled analysis of four community-based cohort studies in Korea published in 2007, is that the prevalence of diabetes among the population aged ≥40 years has increased significantly [21]. Although the prevalence of diabetes has changed significantly in recent years, there is no evidence to recommend specific age thresholds for diabetes screening in Korea.
Therefore, the Committee of Clinical Practice Guidelines of the KDA performed a study to determine the age thresholds for diabetes screening to provide evidence for screening guidelines using the KNHANES 2016 to 2020 and the NHIS-NSC 2012 to 2017 [22]. The analysis, using two large datasets representative of Korea’s general population, was reliable in that it analyzed relatively recent data.
In that study, the number needed to screen (NNS) to obtain one positive test for diabetes diagnosis was calculated. As a result of analyzing the age groups by 5-year increments for adults aged ≥20 years, the NNS tended to decrease with age in both the KNHANES and NHIS-NSC. Notably, the NNS markedly decreased from 63 in the group aged 30 to 34 years to 34 in the following age group of 35 to 39 years in the KNHANES and from 71 to 42 for the same age groups in the NHIS-NSC, respectively (Fig. 2) [22], Therefore, it seems plausible to perform universal screening for diabetes or prediabetes in adults aged ≥35 years.
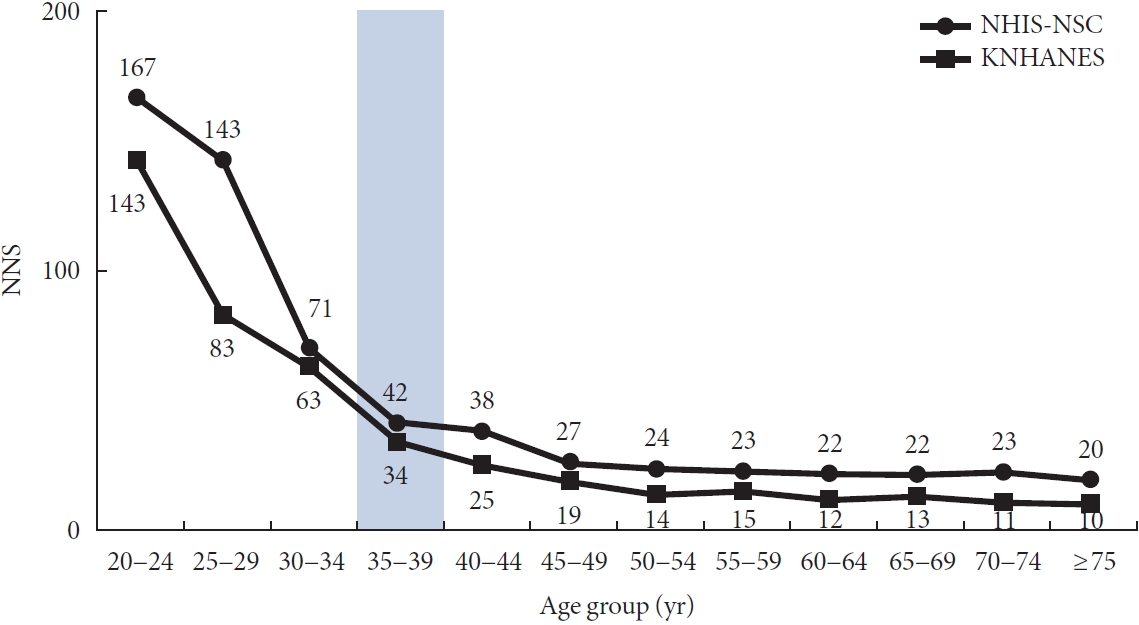
Number of needed to screen (NNS) to detect diabetes according to age group. Adapted from Ha et al. [22]. NHIS-NSC, National Health Insurance Service-National Sample Cohort; KNHANES, Korea National Health and Nutrition Examination Survey.
For adults aged 20 to 34 years, NNS was calculated according to the presence of diabetes risk factors using the KNHANES (Table 2) [22]. Among the suggested risk factors for diabetes according to the KDA guideline, data on overweight or obesity (defined as body mass index [BMI] ≥23 kg/m2 for overweight and ≥25 kg/m2 for obesity), family history of diabetes, hypertension, and dyslipidemia were available in the KNHANES. Abdominal obesity is not included in the KDA recommendation but was added to the analysis because some individuals may have abdominal obesity even at normal BMI, and it is well known that it plays an important role in the development of insulin resistance and diabetes [23,24]. Abdominal obesity was defined as waist circumference (≥90 cm in men and ≥85 cm in women) according to the guidelines of the Korean Society for the Study of Obesity [25]. The NNS values from lowest to highest were 17, 23, 26, 34, 34, and 48 for hypertension, abdominal obesity, dyslipidemia, obesity, family history of diabetes, and overweight or obesity, respectively (Table 2). The rates of missed screening positive in those with overweight or obesity, obesity, and abdominal obesity were 10.6%, 20.0%, and 17.6%, respectively. In the 20 to 34-year age group, if an individual had any of the risk factors, including being overweight, the NNS for diagnosing diabetes was 56, and the rate of missed screening positive was 3.8%.

Diabetes screening effectiveness in adults aged 20 to 34 years according to diabetes risk factors in the KNHANES
Based on these results, assuming universal screening for individual over the age of 35 and selective screening for adult aged 20 to 34 with risk factors, the total NNS for diabetes was 18 and the rate of missed screening positivity was 0.2% [22]. This could significantly reduce the rate of missed screening positive of 4%, calculated based on previous KDA guideline, without significantly increasing the NNS from 16 to 18 [22].
In addition, the committee calculated the NNS for the detection of prediabetes or diabetes in all age groups [22]. The NNS for prediabetes or diabetes was lower in all age groups than the NNS for diabetes only, and there was no sharp decrease between the age groups (the NNS value from the 20 to 24-year age group to the ≥75-year age group ranged from 1 to 8 in the KNHANES and 3 to 10 in the NHIS-NSC. It is well known that preventive interventions through lifestyle changes in people with prediabetes have positive effects in reducing the progression to T2DM and other cardiovascular risk factors [12,26]. In this regard, prevention of diabetes progression and/or cardiovascular disease through early detection of prediabetes or diabetes is considered an important role of diabetes screening.
Considering the above results and current recommendation for diabetes screening in children and adolescents (i.e., screen after 10 years of age or after the onset of puberty in children and adolescents who have risk factors for diabetes [6]), the Committee of Clinical Practice Guidelines of the KDA decided on universal screening for adults aged ≥35 years and selective screening for all adults (aged ≥19 years) with any of the risk factors. In addition, abdominal obesity was added as a risk factor regardless of BMI.
METHODS IN DIABETES SCREENING
FPG and a 75 g oral glucose tolerance test (OGTT) were initially recommended for diabetes screening; however, as the HbA1c measurement method became more accurate and standardized, the International Expert Committee recommended the use of HbA1c as the screening method of choice in 2009 [27]. These changes were also reflected in the 2010 ADA recommendations [28] and in the fourth edition of the KDA guidelines, published in 2011 [29].
There is insufficient evidence to recommend specific tests for initial screening, and possible tests may differ in clinical practice. Therefore, initial screening can be performed according to the clinical availability. After initial screening, in the case of prediabetes, based on the results of a large cohort study conducted in Korea, dividing individuals into two groups and performing additional tests to increase the diagnosis rate of diabetes is recommended [30]. With FPG levels of 110 to 125 mg/dL or HbA1c levels of 6.1% to 6.4%, 75 g OGTT is recommended, and annual follow-ups with FPG or HbA1c tests are suggested for FPG levels of 100 to 109 mg/dL or HbA1c of 5.7% to 6.0%. However, according to a recently published Korean Diabetes Prevention Study (KDPS), 75 g OGTT in individuals with BMIs of ≥23 kg/m2 among those who fell in the FPG 100 to 125 mg/dL group was associated with high rates of diabetes diagnosis [31]. Therefore, for FPG levels of 100 to 109 mg/dL or HbA1c levels of 5.7% to 6.0%, it is recommended to consider 75 g OGTT if there is overweight or obesity. As the KDPS continues, new evidence for a more appropriate screening method for prediabetes may be provided in the future.
CURRENT LIMITATIONS AND RESEARCH NEEDS
Further studies are required to better elucidate the optimal age and frequency to begin and end screening. In addition to universal screening based on age, high-quality studies focusing on earlier screening in otherwise asymptomatic patients in specific subpopulations are required. Diabetes and prediabetes are significantly increasing in Korean children and adolescents [32]; therefore, studies are also needed to develop evidencebased guidelines for diabetes screening. Further evidence for the most appropriate method in the initial screening and appropriate follow-up tests for prediabetes is required. Finally, it is necessary to analyze the effects of screening on health outcomes and their cost-effectiveness in the Korean population.
RECOMMENDATIONS
1. FPG, HbA1c, and 2-hour plasma glucose during 75 g OGTT each can be used as screening tests (Non-randomized controlled studies, General).
2. Annual screenings should begin at 35 years of age regardless of the presence of risk factors, and in all adults (aged ≥19) with any of the risk factors (Expert opinion, General).
3. If the FPG or HbA1c levels are as follows, additional testing should be considered (Expert opinion, General).
1) With an FPG of 100 to 109 mg/dL or an HbA1c of 5.7% to 6.0%, annual FPG or HbA1c tests should be performed. In such cases, if the BMI is ≥23 kg/m2, a 75 g OGTT should be considered.
2) With an FPG of 110 to 125 mg/dL or an HbA1c of 6.1% to 6.4%, a 75 g OGTT should be performed.
Notes
CONFLICTS OF INTEREST
Dae Jung Kim has been an associate editor of the Diabetes & Metabolism Journal since 2022. He is not involved in the review of this article. Otherwise, there are no conflicts of interest to declare.
FUNDING
None
Acknowledgements
None