Effect of Granulocyte Colony-Stimulating Factor on the Peripheral Nerves in Streptozotocin-Induced Diabetic Rat
Article information
Abstract
There are controversial reports about the effect of granulocyte colony-stimulating factor (G-CSF) in peripheral nerve protection. Therefore, the present study aimed to investigate the effect of G-CSF on peripheral nerves in streptozotocin (STZ) induced diabetic rats. After STZ or vehicle injection, rats were divided into five groups (n=6) as follows: normal+vehicle, normal+G-CSF (50 µg/kg for 5 days), diabetes mellitus (DM)+vehicle, DM+G-CSF (50 µg/kg for 5 days), and DM+G-CSF extension (50 µg/kg for 5 days and followed by two injections per week up to 24 weeks). Our results showed that the current perception threshold was not significantly different among experimental groups. G-CSF treatment inhibited the loss of cutaneous nerves and gastric mucosal small nerve fibers in morphometric comparison, but statistical significance was not observed. The present results demonstrated that G-CSF has no harmful but minimal beneficial effects with respect to peripheral nerve preservation in diabetic rats.
INTRODUCTION
Granulocyte colony-stimulating factor (G-CSF), a member of the cytokine growth factor family, mainly stimulates the development of hematopoietic progenitor cells into neutrophils and modulates the actions and distribution of neutrophils actions [1]. Growing evidence has suggested that G-CSF has important nonhematopoietic functions in other tissues including nerve tissue. Recent experimental studies have demonstrated the beneficial effects of G-CSF in several neurological diseases [2-5]. However, some controversial data reported that the potent proinflammatory potential of G-CSF that can exacerbate inflammation related neuropathic pain [6,7]. Diabetic peripheral neuropathy (DPN), which occurs as a result of multiple etiologies and pathogenesis involving chronic inflammation, is the most common chronic microvascular complication of diabetes that affects quality of life and causes diabetic foot ulcers [8]. Most previous studies using G-CSF were based upon iatrogenic peripheral nerve injury models such as crush injury or constriction injury. Therefore, the present study aimed to investigate the effect of G-CSF on peripheral nerves in streptozotocin (STZ) induced diabetic rats which develop progressive peripheral neuropathy.
METHODS
Male Sprague-Dawley rats (160 to 180 g, 6 to 8 weeks old) were allowed adapt to their new environment for 1 week. To induce a diabetic condition, a single intraperitoneal injection of STZ (60 mg/kg body weight) (Sigma Chemical, St. Louis, MO, USA) dissolved in 0.1 mol/L citrate buffer (pH 4.5) was used. Age-matched control rats received an equal volume of vehicle (sodium citrate buffer) in the same manner and were cared for along with the diabetic rats. Forty-eight hours after STZ injection, the experimental rats with blood glucose levels ≥20 mmol/L were confirmed to have diabetes. The Precision Xtra Plus (Abbot Laboratories, MediSense Products, Bedford, MA, USA) system was used to measure blood glucose. A minimum 2-week period is required to induce the typical features of diabetes [9]. Therefore, following a 2-week intraperitoneal injection of STZ and sodium citrate buffer, diabetic rats and their age-matched controls were randomly assigned to five groups (n=6 per group) according to the treatment: rats with normal glucose levels that received sodium citrate buffer vehicle (control group, normal); normal+G-CSF (50 µg/kg for 5 days); diabetic rats with high blood glucose levels without treatment during the entire experimental period (diabetes mellitus, DM); DM+G-CSF (G-CSF, 50 µg/kg for 5 days); DM+G-CSF extension (G-CSF, 50 µg/kg for 5 days and followed by two injections per week up to 24 weeks). G-CSF was administered subcutaneously.
Body weight and blood glucose levels were measured after 8 hours of fasting in weeks 0, 12, and 24. Fasting glucose level was assessed using blood samples drawn from a tail vein, and hemoglobin A1c (HbA1c) levels were also compared using a commercially available kit (NycoCard, Oslo, Norway). The current perception threshold (CPT) to quantify nerve dysfunction was measured in weeks 0 and 24 using the same method described in a previous study [10]. All the subjects from each group were sacrificed at the 24th week according to the animal care and experimental protocols approved by the Institutional Animal Care and Use Committee of Chonbuk National University Medical School (CBU 2010-0005). To perform the cutaneous small nerve fiber comparison, tissue samples with a 3×3 mm area were taken from the dorsum of the hind leg by skin biopsy at baseline and at the time of sacrifice. The procedures for performing the immunohistochemistry were the same as in a previous report [10]. Images of all fluorescent nerve fibers at a magnification of ×100 were collected and analyzed using a Carl Zeiss Axioskop2 plus microscope (Carl Zeiss, Goettingen, Germany) and the Axiovision 5.1 program. Anti-protein gene product 9.5 (PGP 9.5)-immunoreactive nerve fibers in the epidermis of each section were counted as previously explained [10]. The peripheral nerves of the gastric mucosa were also examined to detect neuroprotective effects of G-CSF. To compare gastric mucosal nerve quantity among experimental groups, an arbitrary horizontal line connecting 100 µm distant points from the luminal side was drawn in addition to morphologic comparison.
The data were expressed as mean±standard deviation. Repeat measured analysis of variance (ANOVA) was used for comparing body weight and blood glucose levels according to time passage in each group. One-way ANOVA with Duncan's post hoc test was used for comparing the experimental groups. The data were considered statistically significant if the P value was less than 0.05. Statistical analysis was performed using SPSS version 12.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Body weight increased continuously during the experimental period in the normal glucose group. However, proper weight gain was not achieved in the STZ-induced diabetes groups. Food intake was greater in the diabetes groups than in the control groups. G-CSF treatment did not affect body weight in any of the experimental groups. The mean blood glucose level in the control group was within the normal range and was maintained around 5 mmol/L during the experimental period, whereas glucose levels in the diabetic groups were greater than 20 mmol/L. Treatment with G-CSF for 24 weeks did not affect blood glucose levels and HbA1c in either normal or diabetic groups (glucose level, DM vs. DM+G-CSF vs. DM+G-CSF extension; 21.74±1.43 vs. 20.45±2.57 vs. 22.32±1.71, P>0.05). CPT of animals in each group showed no differences between the G-CSF treated and nontreated diabetic groups over the 24 week period (2,000 Hz, DM vs. DM+G-CSF vs. DM+G-CSF extension, 748.75±147.89 vs. 723.33±60.28 vs. 764.83±40.85, P>0.05; 250 Hz, 332.22±36.72 vs. 380.56±103.18 vs. 377.22±92.32, P>0.05; 5 Hz, 285.83±7.77 vs. 261.25±15.46 vs. 261.25±15.46, P>0.05).
The intraepidermal nerve fiber density (IENFD) was similar in all five groups at week 0 (data not shown) and decreased significantly in the nontreated diabetic groups compared with that of the control group at the 24th week. However, among the diabetic groups, there was a smaller reduction in IENFD of the foot in the G-CSF treated diabetic group compared with the nontreated diabetic group although the difference was not significant (DM vs. DM+G-CSF vs. DM+G-CSF extension; 4.90±0.32 vs. 5.21±0.24 vs. 5.69±0.33, P>0.05) (Fig. 1). Immunostained small gastric nerve fibers that passed over an arbitrary line connecting 100 µm placed points from the luminal side were more shortened and in a more degenerated pattern in the diabetes groups. The G-CSF treated diabetic group showed less reduction in nerve fibers compared with the nontreated diabetic group, although significant differences were not observed (Fig. 2).
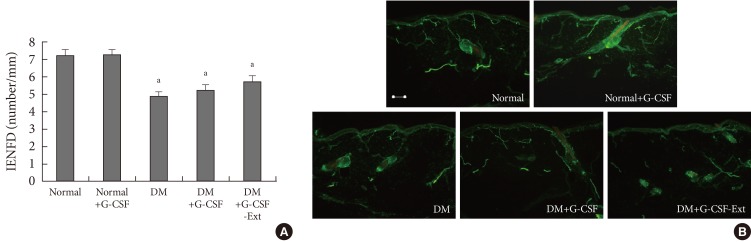
(A) Intraepidermal nerve fiber density (IENFD) on the dorsum of the foot at 24 weeks and (B) morphologic pattern of antiprotein gene product 9.5-positive small nerve fibers. IENFDs in the granulocyte colony-stimulating factor (G-CSF) treated diabetic groups were preserved compared with nontreated diabetic group, although statistical significance was not observed. Horizontal bar indicates 100 µm. DM, diabetes mellitus. aP<0.05 compared to normal group.

(A) The average number of mucosal nerve fibers and (B) antiprotein gene product 9.5-positive small nerve fibers in stomach. The nerve count was markedly decreased in the diabetic group. Granulocyte colony-stimulating factor (G-CSF) treated diabetic groups were preserved compared with non-treated diabetic group, although statistical significance was not observed. Horizontal bar indicates 100 µm. DM, diabetes mellitus. aP<0.05 compared to normal group.
DISCUSSION
DPN affects over half of diabetic patients and causes serious problems on the lower legs of diabetic patients such as foot ulcers or amputation. In addition, diverse neuropathic symptoms from DPN also impact the quality of life of diabetic patients. However, it is unsatisfactory to ameliorate peripheral neuropathy using current therapeutic strategies, so the development of new effective agents based on the pathogenesis of DPN is necessary. The pathogenesis of DPN is multifactorial and previous reports have suggested that DPN is associated with increased inflammatory cytokines and the reduced availability of nerve growth factor [11,12]. In this context, G-CSF, a member of the growth factor family, can be postulated to play the same role in diabetic neuropathy as other neurotropic factors. In addition, a recent series of clinical and experimental studies have demonstrated the beneficial effects of G-CSF in several neurologic diseases. It has been proposed that G-CSF exerts beneficial effects through different mechanisms, including mobilization of bone marrow cells, antiapoptosis, anti-inflammation, neuronal differentiation, and angiogenesis [13]. Another study demonstrated that G-CSF alleviates neuropathic pain via activation of polymorphonuclear cell-derived endogenous opioid secretion to activate opioid receptors in the injured nerve and down-regulate interleukin-6 and tumor necrosis factor-α inflammatory cytokines [14]. However, controversial data makes it difficult to determine whether the administration of G-CSF would be beneficial to the inflamed host or not. Campbell and coworkers [7] demonstrated that G-CSF exaggerates the symptoms of collagen-induced arthritis in mice. Liou et al. [6] highlighted the potent pro-inflammatory potential of G-CSF and suggested that it may be a target for therapeutic intervention in chronic neuropathic pain.
Until now, there have been few reports about the therapeutic potential of G-CSF in DPN. Therefore, we investigated whether or not G-CSF is beneficial in the protection of peripheral nerve damage of experimentally-induced diabetes. Our preliminary results show that the subcutaneous administration of G-CSF did not lead to a significant difference in CPT. However, there was less reduction in the IENFD of the foot and gastric small nerve fibers in the G-CSF treated diabetic group compared with the nontreated diabetic group although statistical significance was not observed.
It is obvious that DPN is caused by diverse pathogenic mechanisms and, as such, is difficult to be completely protected against using a single agent. The present study showed that G-CSF has minimal beneficial effects in morphologic parameters and no harmful effects in experimental diabetes. Therefore, G-CSF used in combination with well-established strategies including strict glucose control and antioxidative stress agents is worth investigating as a novel DPN therapeutic approach. Experimental variation in the scheduled administration of additional doses of G-CSF is also worth further investigation.
Several limitations were present in this study. The presence of the G-CSF receptor was not shown in the peripheral nerves. In addition, more precise and detailed signaling pathways and related mediators were not investigated. Further studies that take into account nerve conduction velocity and sensory or motor behavior tests are required to ascertain additional neuronal effects of G-CSF on DPN. In the future, diverse cytokines and inflammatory mediators related to neuropathic pain assessment should be investigated along with G-CSF administration.
Notes
No potential conflict of interest relevant to this article was reported.