A Comparison of Predictive Performances between Old versus New Criteria in a Risk-Based Screening Strategy for Gestational Diabetes Mellitus
Article information

Abstract
Background
The definition of the high-risk group for gestational diabetes mellitus (GDM) defined by the American College of Obstetricians and Gynecologists was changed from the criteria composed of five historic/demographic factors (old criteria) to the criteria consisting of 11 factors (new criteria) in 2017. To compare the predictive performances between these two sets of criteria.
Methods
This is a secondary analysis of a large prospective cohort study of non-diabetic Korean women with singleton pregnancies designed to examine the risk of GDM in women with nonalcoholic fatty liver disease. Maternal fasting blood was taken at 10 to 14 weeks of gestation and measured for glucose and lipid parameters. GDM was diagnosed by the two-step approach.
Results
Among 820 women, 42 (5.1%) were diagnosed with GDM. Using the old criteria, 29.8% (n=244) of women would have been identified as high risk versus 16.0% (n=131) using the new criteria. Of the 42 women who developed GDM, 45.2% (n=19) would have been mislabeled as not high risk by the old criteria versus 50.0% (n=21) using the new criteria (1-sensitivity, 45.2% vs. 50.0%, P>0.05). Among the 778 patients who did not develop GDM, 28.4% (n=221) would have been identified as high risk using the old criteria versus 14.1% (n=110) using the new criteria (1-specificity, 28.4% vs. 14.1%, P<0.001).
Conclusion
Compared with the old criteria, use of the new criteria would have decreased the number of patients identified as high risk and thus requiring early GDM screening by half (from 244 [29.8%] to 131 [16.0%]).
INTRODUCTION
Gestational diabetes mellitus (GDM) is defined as any degree of glucose intolerance that is first recognized during pregnancy [1]. GDM is one of the most common complications during pregnancy, with a reported prevalence of 5.7% to 9.5% in pregnant Korean women [23]. GDM is related to not only maternal complications but also fetal/neonatal adverse outcomes; therefore, the diagnosis of GDM in the appropriate period and adequate glucose control are helpful to minimize these complications[456].
In the 4th International Workshop Conference on GDM in 1998, classifying pregnant women according to the risk for GDM into low-, intermediate-, and high-risk groups and determining a differential screening strategy for each risk group were recommended. The high-risk group was defined as those with maternal demographic risk factors (i.e., strong family history, marked obesity, history of GDM, glucose intolerance, and glucosuria), and a glucose tolerance test at their first prenatal visit was recommended for this high-risk group [7]. These criteria for the high-risk group were reaffirmed at the 5th International Workshop Conference in 2005 and have been also used in the clinical guidelines of the American College of Obstetricians and Gynecologists (ACOG) [89]. Until now, the clinical effectiveness of the criteria for the high-risk group has not been well evaluated in previous studies, although this strategy has been widely implemented in clinical practice [1011121314].
Otherwise, the American Diabetes Association (ADA) recommended in 2012 early testing for diabetes at the first prenatal visit in women with risk factors for type 2 diabetes mellitus [15]. Moreover, the new criteria for pregnant women was exactly derived from the criteria in non-pregnant adults for high risk of diabetes, because of increasing prevalence of type 2 diabetes mellitus in women of child-bearing age [16]. Therefore, the criteria for high risk for GDM suggested in this recommendation were different from those in the ACOG guidelines, consisting of 11 clinical factors (Supplementary Fig. 1). In 2017, ACOG also adopted this ADA recommendation and recommended early screening for GDM according to these new criteria [1]. Unlike criteria of the high-risk population in 5th International Workshop on GDM (old criteria), the criteria of the high-risk population by the ADA (new criteria) includes the degree of obesity and laboratory results [817].
In Korea, the screening strategy for the high-risk group and diagnosis of GDM has been conducted based on the ACOG guidelines. Although the acceptance of new criteria is an issue of paramount importance in clinical practice, these two criteria have not been compared in terms of their ability to predict the development of GDM until now. Furthermore, because some risk factors such as low high density lipoprotein cholesterol (HDL-C) and previous history of cardiovascular disease which are included in the new criteria are rare in young women, it is necessary to verify their significance for predicting the development of GDM. In this study, we compared the predictive performance for detecting GDM between the old and new criteria.
METHODS
Ethics
The current study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1810-047-977). Written informed consent was obtained from all participants at the time of enrollment of the original study.
Study design
This study is a secondary analysis of the ongoing large prospective cohort study designed to examine the risk of GDM in women with nonalcoholic fatty liver disease (“Fatty Liver in Pregnancy” registry, NCT02276144) [18]. The subjects of this study are non-diabetic Korean women with singleton pregnancy whose data contains the information for assessing clinical and demographic risk by both the old and new criteria and the results of the diagnostic tests for GDM during pregnancy. The predictive ability of these risk criteria for the development of GDM was compared between the old and new criteria.
The setting of a prospective cohort study
In 2014, there had been a large prospective cohort study of nonalcoholic fatty liver disease in pregnancy conducted in three centers (Incheon Seoul Women Hospital, Seoul Metropolitan Government Seoul National University Boramae Medical Center, and Seoul National University Hospital) in South Korea to examine the risk of GDM in women with nonalcoholic fatty liver disease. Incheon Seoul Women Hospital, as the primary obstetric care center, has approximately 4,000 deliveries annually; and Seoul National University Boramae Medical Center, as a referral center, has approximately 500 deliveries annually. Participants were recruited at these two hospitals, and investigators at Seoul National University Hospital designed the study protocol and analyzed data. The protocol of the original research is detailed in the previous report [18].
Study population of the current study
The women enrolled from October 2014 to October 2017 were included in the current study. All participants visiting antenatal care centers before 14 weeks of gestation were enrolled after obtaining informed consent. Women who agreed to secondary analysis and who completed diagnostic tests (two-step approach) for GDM were included. Women with pre-gestational diabetes mellitus or who wanted to withdraw from the study were excluded. Among them, the eligible study population fulfilled all of the data of clinical/demographic risk factors in old and new criteria. Cases with no information about at least one of the risk factors in the old and new criteria were excluded to compare sensitivity and specificity between old and new criteria.
The definition and evaluation of risk factors of GDM
The presence of each risk factor included in the old or new criteria was evaluated in the study population. Among the risk factors, clinical characteristics including pre-pregnancy body mass index (BMI), family history of diabetes, history of gestational diabetes in prior pregnancy, maternal underlying disease such as pre-pregnancy diabetes, hypertension, and cardiovascular disease were collected routinely at the time of enrollment. At 10 to 14 weeks of gestation, the degree of physical activity was also evaluated by The International Physical Activity Questionnaire [19], and fasting blood samples after an 8-hour fasting were collected at the time of liver ultrasound (which was conducted for the original cohort study) for measurement of fasting glucose and lipid parameters such as triglyceride (TG) and HDL-C. In addition, the presence of glucosuria in early pregnancy, the delivery history of macrosomia, and the diagnosis of polycystic ovarian syndrome (PCOS) before pregnancy were evaluated by review of medical records. The presence of glucosuria is routinely evaluated in early pregnancy in our institutions.
For BMI classification, World Health Organization criteria for an Asian population were adopted, because the study population consisted of only Korean pregnant women [2021]. Overweight and obese was defined as BMI ≥23 and ≥25 kg/m2, respectively, and severe obesity was defined as BMI ≥30 kg/m2, which are the suggested criteria for obesity class II (severe obesity) in an Asian population. Glucosuria was defined as +1 or more a dipstick at urinary analysis in early pregnancy [22]. Physical inactivity was defined as no leisure time physical activity in the last 7 days [23]. Impaired glucose metabolism was defined as fasting blood glucose level of ≥100 mg/dL [24]. Other criteria of impaired glucose metabolism (glycosylated hemoglobin and impaired glucose tolerance) were not available in the current study.
Diagnosis of GDM
GDM was diagnosed by the two-step approach, a 50 g screening glucose tolerance test (OGTT) followed by a diagnostic 100 g OGTT according to the ACOG guidelines [1]. Women with measured plasma glucose level ≥140 mg/dL at 50 g OGTT were examined for 100 g OGTT. A diagnosis for GDM required two or more elevated glucose values in 100 g OGTT with the cut-off values of the Carpenter and Coustan thresholds (95 mg/dL for fasting glucose, 180 mg/dL for 1-hour glucose, 155 mg/dL for 2-hour glucose, and >140 mg/dL for 3-hour glucose) [25].
Statistical analysis
Continuous variables were described by median and interquartile range, and categorical variables were described by numbers and percentage. The comparison of continuous variables was performed using the independent t-test or the Mann-Whitney U test. Categorical variable were compared with the chi-square test or the Fisher exact test, where appropriate. Using univariable logistic regression analysis, odds ratios (ORs) and 95% confidential intervals (CIs) of risk factors for GDM were evaluated. For determining the independent risk factors, multivariable logistic regression analysis was conducted using variables chosen with a P value of <0.05 in the univariable analysis with backward elimination. In the multivariable logistic regression, Firth's penalized likelihood bias reduction was used to avoid bias in parameter estimates due to the small sample size [26]. To compare predictive performance such as detection rate and false-positive rate between the old and new criteria, the McNemar test was applied. Missing data were treated as missing observations. A P value of <0.05 was considered statistically significant. IBM SPSS Statistics version 23.0 software (IBM Inc., Armonk, NY, USA) and R version 3.5.1 (http://www.r-project.org) were used for the analyses.
RESULTS
Study population
During the study period, a total of 1,077 women without pre-gestational diabetes were recruited between October 2014 and October 2017 and completed the test for GDM. Among these women, 257 subjects (132 women who did not have a fasting blood sample at 10 to 14 weeks of gestation, three women who did not report their degree of physical activity, 36 women without data on glucosuria, 23 women without data on the history of PCOS, and 63 women without data on history of macrosomia in a previous pregnancy) were excluded from the final analysis.
In 820 women in the final study population, 42 (5.1%) women were diagnosed with GDM and 12 (1.5%) women with GDM were managed on insulin (Fig. 1). Among 820 women, 29.8% (n=244) of women would have been identified as high risk using the old criteria, whereas 16.0% (n=131) would have been identified as high risk using the new criteria. Among 244 women who were assessed as high risk by the old criteria, 9.5% (n= 23) of women were diagnosed with GDM and 3.3% (n=8) of women were managed on insulin. Among the 131 women who were assessed as high risk by the new criteria, 16.0% (n=21) of women were diagnosed with GDM and 6.1% (n=8) of women were managed on insulin.
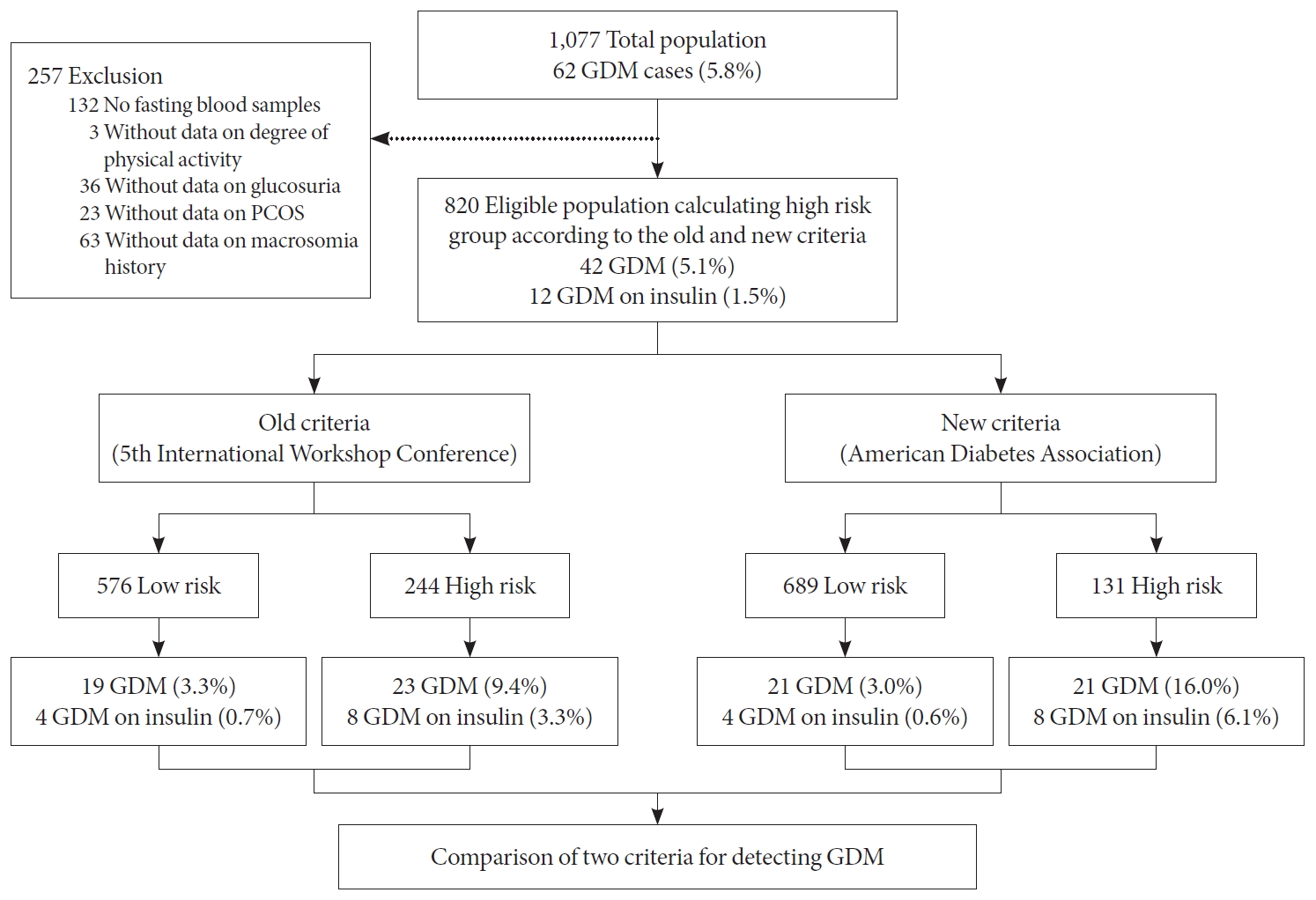
Study diagram. PCOS, polycystic ovarian syndrome; GDM, gestational diabetes mellitus.
Basal characteristics and obstetric outcome according to the presence of GDM
Basal characteristics and obstetric outcome of the study population according to the GDM status are presented in the Supplementary Table 1. The median maternal age and the frequency of nulliparity were not different between the two groups. Women who developed GDM had a higher median pre-pregnancy BMI and a higher rate of previous history of GDM and chronic hypertension. The gestational age at delivery, birth weight, and the risk of macrosomia or cesarean delivery were not different between the two groups. Women with GDM were more likely to have large for gestational age neonates, but this difference did not reach statistical significance.
Odds ratio of risk factors for GDM
Table 1 presents the OR of individual risk factors consisting of the old or new criteria for high risk of GDM. BMI ≥23 kg/m2, first-degree relative with diabetes, chronic hypertension, previous history of GDM, impaired fasting glucose, and TG >250 mg/dL were associated with the development of GDM. Similarly, BMI ≥23 kg/m2, chronic hypertension, previous history of GDM, glucosuria, impaired fasting glucose, HDL-C <35 mg/dL, and TG >250 mg/dL were associated with the development of GDM on insulin. However, PCOS history, physical inactivity, previous infant with macrosomia, glucosuria, and HDL-C <35 mg/dL were not related to the risk of GDM.
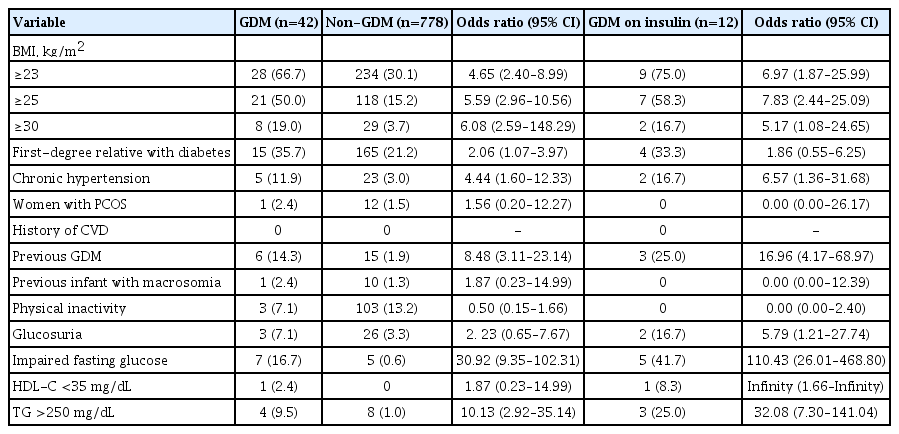
Odds ratio of risk factors for GDM and GDM on insulin using univariable logistic regression analysis
Odds ratio of risk factors by old and new criteria
Table 2 shows that all of the risk factors in the old criteria were significantly associated with the development of GDM, except glucosuria. Overall, the OR of the high-risk group for GDM by the old criteria was 3.05 (95% CI, 1.63 to 5.71). By the new criteria, overweight women who had one of the risk factors such as first-degree relative with diabetes, previous GDM, chronic hypertension, TG >250 mg/dL, impaired fasting glucose, or severe obesity increased the risk of the development of GDM significantly. Overall, the OR of the high-risk group by the new criteria was 6.07 (95% CI, 3.21 to 11.49), higher than those by the old criteria.
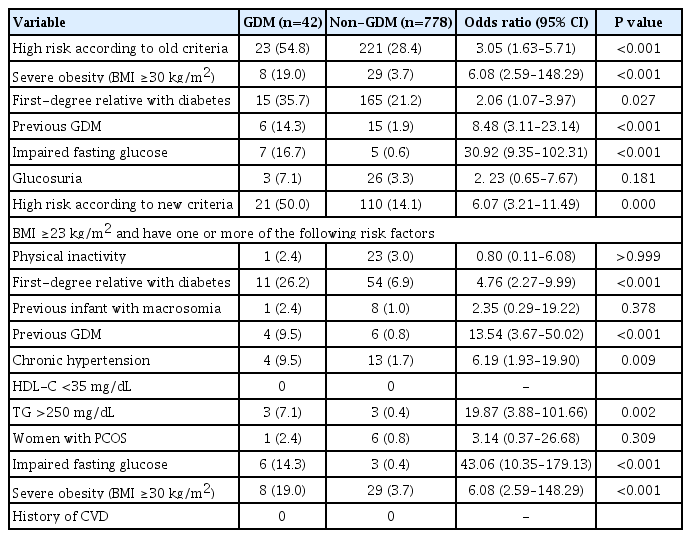
Odds ratio of risk factors by old and new criteria for detecting GDM using univariable logistic regression analysis
Table 3 also presents the OR of individual risk factors for GDM requiring insulin treatment according to the old or new criteria. The OR of the high-risk group by the old criteria and the new criteria was 5.04 (95% CI, 1.50 to 16.91) and 12.15 (95% CI, 3.60 to 41.02), respectively.
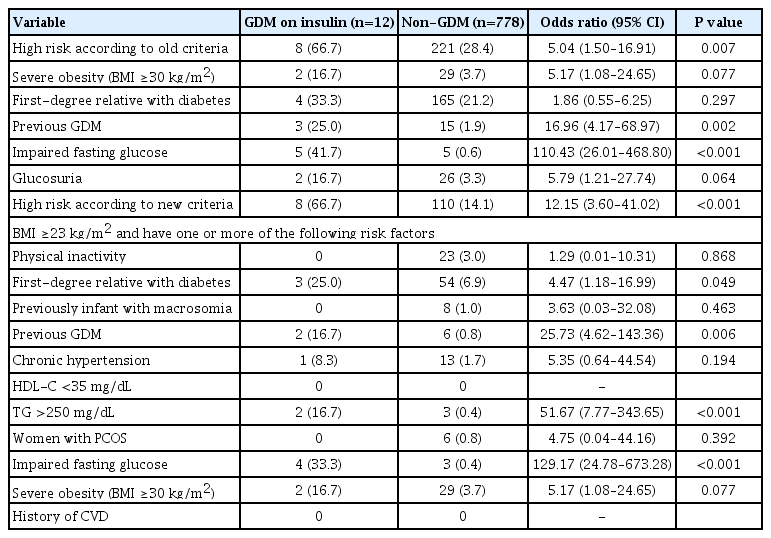
Odds ratio of risk factors by old and new criteria for detecting GDM on insulin using univariable logistic regression analysis
Predictive performance of old vs. new criteria
As shown in Table 4, the detection rate and false-positive rate were compared between the two criteria. Of the 42 women who developed GDM, the old criteria would have classified 54.8% of women as high risk, whereas the new criteria would have classified 50% of women as high risk (P>0.05). Among the 778 patients who did not develop GDM, 28.4% (n=221) would have been identified as high risk using the old criteria versus 14.1% (n=110) using the new criteria (P<0.001). For prediction of GDM requiring insulin treatment, the detection rate was 66.7% for both criteria, and the false-positive rate was lower when using the new criteria than the old criteria (29.2% vs. 15.2%, P<0.001).
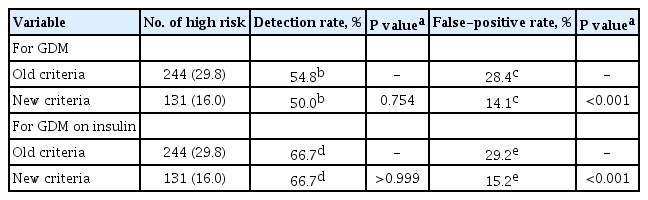
Predictive performance of old versus new criteria
Independent risk factors for GDM
Table 5 shows multivariable logistic regression analysis conducted to determine independent risk factors for GDM. Among various risk factors consisting of old or new criteria, only four factors (BMI, previous gestational diabetes, TG >250 mg/dL, and fasting blood gluocose ≥100 mg/dL) were independent risk factors.

Multivariable logistic regression analysis of risk factors for gestational diabetes mellitus
DISCUSSION
Principal findings of the study
(1) The prevalence of GDM and GDM managed on insulin was 5.1% and 1.5%, respectively. (2) Compared with the old criteria, the use of the new criteria would have decreased the number of patients identified as high risk and thus requiring early GDM screening by half (from 29.8% to 16.0%). (3) Although the detection rate for GDM was similar between the two criteria, the false-positive rate was significantly lower in the new criteria compared with the old criteria. (4) Among the suggested risk factors, only BMI, previous gestational diabetes, TG >250 mg/dL, and impaired fasting glucose were independent risk factors.
High-risk population for GDM
There has been so much effort to establish criteria by which the high-risk group of GDM can be classified, because the number of pregnant women who are examined with unnecessary screening tests could be reduced. Previous studies had researched validating the performances of the risk-based screening guidelines or scoring systems of GDM [272829]. According to the current systematic review study evaluating the association of risk factors with GDM, it was not possible to offer pregnant women gold standard screening methods for detecting of GDM [30]. To this day, the criteria for the high-risk group of GDM used in each country are not unified [153132]. The aim of the present study was to investigate which criteria had better predictive performance for developing GDM between the old and new criteria adopted by ACOG. Although the acceptance of the new criteria is an issue of paramount importance in clinical practice, the comparison between the old and new criteria has not been evaluated in the literature. To our knowledge, our study is the first report that compares predictive performances of the old and new high-risk criteria for GDM. In the current study, the detection rate of the new criteria is similar to the old criteria, but the false-positive rate is lower in the new criteria than in the old criteria. According to these findings, fewer people are classified as high risk and, thus, do not receive unnecessary screening tests. However, pregnant women should have their laboratory results such as TG and HDL-C level for their risk assessment by the new criteria. Therefore, for applying the new criteria in the clinical setting, cost-effective analysis is necessary. Moreover, both criteria missed around half of patients (45% vs. 50%) who subsequently developed GDM. More studies are needed to confirm the clinical utility of using the new criteria.
Independent risk factors for GDM
Among the new criteria risk factors for GDM, physical inactivity, macrosomia history, low HDL-C, and PCOS were not significant risk factors for GDM. After analyzing multivariable logistic regression, only four factors, including BMI ≥25 kg/m2, previous gestational diabetes, TG >250 mg/dL, and fasting blood gluocose ≥100 mg/dL were independent risk factors for GDM. There have been previous studies evaluating predictable markers for GDM using a maternal blood sample in early pregnancy. Elevated fasting glucose level in early pregnancy has been well known as a risk factor of GDM [333435]. The previous studies about the relationship of lipid concentrations in early pregnancy and GDM showed that only elevated triglyceride is significantly associated with GDM, whereas other lipids are not [3637]. These results are consistent with our findings. Thus, evaluating level of TG and fasting blood glucose at the early pregnancy visit might be clinically useful for predicting GDM. And, these findings are expected to help build a new model for GDM prediction. The determination of the clinical value of each risk factor is also needed in large study populations. Further studies regarding an optimal classification system of risk-based GDM screening are also needed.
Strength and limitation
This is the first study validating both the new and old criteria adopted by ACOG. According to the study protocol, which was designed to determine the risk of GDM in patients with nonalcoholic fatty liver disease, we prospectively collected the clinical factors that are known as risk factors for GDM, such as previous history of GDM and family history of diabetes. In addition, we also collected a fasting blood sample at 10 to 14 weeks of gestation, and measured HDL-C, TG, and glucose in these blood samples. This prospective collection of clinical data and laboratory results allowed accurate determination of the ability of the old and new criteria to predict GDM. It is very different from previous studies validating risk-based screening strategies. In addition, the current study evaluated the risk factors for GDM in an Asian population. As the frequency or risk factors for diabetes may be different among races or ethnicities, it is necessary to evaluate the effectiveness of the risk-based GDM screening strategies in an Asian population. Until now, there had been no research about risk-based screening strategies for GDM in Asian countries. Compared to the previous meta-analysis analyzed risk factors for GDM in Asia, the prevalence of GDM and the distributions of risk factors of GDM are similar to that of the subjects of our study [38]. We expect that our study provides clinical information of risk-based screening strategy to other Asian countries.
There are several points to be considered. First, we evaluated the false-positive rate and detection rate for GDM diagnosed during any period of gestation, although the high-risk criteria targets selection of the high-risk group for GDM diagnosed early in pregnancy or pre-gestational diabetes. Second, the criteria with laboratory results are based on the result of the blood taken at 10 to 14 weeks of gestation. The optimal blood testing period for judgment of high risk (i.e., pre-gestational blood test vs. blood test in early pregnancy) is not clear in the guidelines. Third, the number of patients with GDM and GDM on insulin is insufficient to show a significant difference in sensitivity between old and new criteria.
Further study
To confirm the clinical utility of the new criteria or selective risk-based screening for early GDM, more prospective studies and randomized controlled trials will be needed comparing outcome between populations managed according to the strategy and not. To suggest the appropriate screening strategy for GDM, comparison and validation of various screening strategies are also needed. As these criteria were originally designed to select the high-risk group at the first prenatal visit, further research is needed to determine the performances of these criteria for detecting early GDM.
Conclusion
Compared with the old criteria, use of the new criteria would have decreased the number of patients identified as high risk and, thus, reduced early GDM screening by half. Similarly, the use of the new criteria would have decreased by half the number of patients who did not develop GDM from having to undergo early screening. More studies are needed to confirm the clinical utility of using the new ADA criteria.
ACKNOWLEDGMENTS
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science and ICT of Korea (2016M3A9B6902061). Funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: S.H., S.M.L., S.H.K., J.S.P.
Acquisition, analysis, or interpretation of data: S.H., S.M.L., S.H.K., B.J.K., J.N.K., I.H.O., S.O., S.M.K., S.S., W.K., S.K.J., S.L., C.W.P., J.K.J.
Drafting the work or revising: S.H., S.M.L., S.O., E.R.N.
Final approval of the manuscript: J.S.P.
References
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2019.0126.
Supplementary Table 1
Basal characteristics and pregnancy outcomes
Supplementary Fig. 1
High-risk group for gestational diabetes mellitus (GDM) by old and new criteria. HDL, high density lipoprotein; TG, triglyceride; PCOS, polycystic ovarian syndrome; HbA1c, glycosylated hemoglobin. aHbA1c and 75 g oral glucose tolerance test were not available in this study