Evaluation of Stress in Korean Patients with Diabetes Mellitus Using the Problem Areas in Diabetes-Korea Questionnaire
Article information
Abstract
Background
It is known that diabetes and stress are directly or indirectly related, and that it is important to evaluate stress in patients with diabetes. The relationship between Korean diabetics and diabetes-related stress has never been reported. The objective of this study was to develop a stress questionnaire suitable for use with Korean diabetics and to evaluate its utility.
Methods
This study subjects were 307 Korean diabetics, aged 40 to 74 years old, who visited the Department of Endocrinology and Metabolism at Gachon University Gil Hospital, Yeungnam University Medical Center, and Inha University Hospital in Korea between March 2006 and February 2008. We developed a Korean version of Polonsky's Problem Areas in Diabetes (PAID) stress questionnaire (PAID-K) and used it to assess degrees of stress in our sample of Korean patients. We evaluated the utility of the questionnaire and analyzed the relationships between clinical characteristics of the study subjects and degrees of stress.
Results
Cronbach's alpha for PAID-K was 0.95, and PAID-K scores were significantly correlated with Hypoglycemia Fear Survey scores (r=0.44, P<0.05) and State Trait Anxiety Inventory-6 scores (r=0.21, P<0.05). PAID-K scores were significantly higher in patients with longer durations of diabetes, patients using insulin, and female patients (P=0.02, P=0.038, and P=0.001, respectively). The score also tended to increase as HbA1c levels increased, except for very high HbA1c levels (above 11%) (P for trend<0.05).
Conclusion
We developed the PAID-K questionnaire and demonstrated its utility to evaluate levels of stress in diabetic patients in Korea.
INTRODUCTION
Diabetes is known to be directly and indirectly associated with stress [1,2]. Many researchers have reported that diabetes is actually induced by stress [3-7], and several hormones including cortisol are known to be involved [6]. Depression, eating disorders, and emotional stress make self-management more difficult, and adverse effects to glycemic control and complications can occur [8]. Severe stress can damage patient ability to benefit from basic health education about diabetes, and such education should therefore be postponed until self-management of stress is achieved [9]. Relief from stressors is thought to be absolutely necessary in order to improve the overall condition of diabetic patients. So, it is important to assess diabetes-related stresses as well as general stresses in diabetic patient. Many methods including the ATT39, the Questionnaire on Stress in Patients with Diabetes-Revised (QSD-R), Problem Areas in Diabetes (PAID), and the Diabetes Distress Scale (DDS) have been reported for assessing the stress levels in diabetic patients [10-13]. Among these methods, the PAID questionnaire, which was introduced by Polonsky in 1995, has been most commonly cited in the medical journals and used in more than 10 countries. The internal consistency (Cronbach's alpha=0.90), reliability (r=0.83), and responsiveness of the PAID are high [12,13].
Methods for evaluating diabetes-related stress levels in Korean diabetic patients have not been developed. We translated the American version of the PAID stress evaluation into Korean, yielding the Korean PAID stress evaluation questionnaire, or PAID-K. To evaluate the effectiveness of the PAID-K questionnaire, we analyzed the characteristics and stress levels of a sample of Korean diabetic patients, and assessed the relationships between PAID-K scores and correlates of stress.
METHODS
Methods
The present study was conducted by Department of Endocrinology and Metabolism at Gachon University Gil Hospital, Yongnam University Hospital, and Inha University Hospital, Korea, between March of 2006 and February of 2008. We included type 2 diabetic patients between the ages of 40 and 74. Patients with severe heart disease, kidney disease (over 2.0 mg/dL creatinine), liver disease, and acute infection were excluded from this study. Data from 307 individuals were used for final analysis. Psychiatric care was recommended for patients whose stress levels were determined to be severe.
Experimental methods
Development of the PAID-K
The PAID evaluation form was translated into Korean by three Korean diabetes specialists consistent with the Korean cultural context. We conducted 20 preliminary studies and modified a total of 20 questions. A 5-point scale was developed for each item (0 to 4 points), and each score was multiplied by 1.25 to yield a total score of 100 [12]. Examinations of preliminary results could be completed within 10 minutes.
Survey reliability and validity
Cronbach's alpha was calculated to confirm the internal reliability of the PAID-K. To assist in accurate validation, the Hypoglycemia Fear Survey (HFS) and State-Trait Anxiety Inventory-6 (STAI-6) were also translated and edited for comparison. The HFS consists of 26 questions and has a total possible score of 130 points, and the STAI-6 consists of 6 questions and has a total possible score of 24 points [14,15].
Subject evaluation
Data regarding family members, residence, income, education level, family history, and working conditions were compiled and evaluated for all participants, and exercise, alcohol, smoking, leisure activities, and dietary habits were also investigated. Height and weight measurements were taken while the patients wore light clothing and body weight (kg) was divided by height squared (m2) to calculate body mass index (BMI). Waist circumference was measured between the bottom rib and the iliac crest at the narrowest level near the navel after a relaxed exhale using a tape measure. Blood sampling was performed after 8 hours of fasting. Fasting blood glucose, 2 hour postprandial blood glucose, total cholesterol, and high density lipoprotein cholesterol (HDL-C) were measured using a triglyceride automatic chemical analyzer (Hitachi 7600-110; Hitachi, Tokyo, Japan), and low density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald formula (total cholesterol-[triglyceride/5]-[HDL-C]). The glycated hemoglobin test was performed using high performance liquid chromatography, and the spot urinary albumin/creatinine ratio (ACR) was measured by a one-time urine test. Cases for which ACR was between 30 and 300 µg/mg were defined as microalbuminuria and nephropathy was considered. The certainty of the length of diabetes treatment and insulin use in patients was assessed, and diabetic macrovascular complications and microvascular complications were diagnosed. Patients with macrovascular complications were defined as those having abnormalities in coronary angiography or single-photon emission computed tomography of the heart, those who had received coronary artery bypass grafts, and those with histories of acute cerebrovascular disease and peripheral vascular disease. Microvascular complications were identified as diabetic retinopathy, diabetic nephropathy, and diabetic neuropathy.
Statistical analyses
Statistical analyses of data were performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA). All results were expressed as means±standard deviations. The independent sample t-test and Spearman correlation analysis were performed to assess the relationships between PAID-K and variables. One-way ANOVA was used to compare the averages of three groups, and the Bonferroni method was used for forensic analysis. Independent factors affecting PAID-K scores were analyzed by linear regression analysis. P values less than 0.05 were considered to be statistically significant.
RESULTS
General characteristics of the study subjects
There were a total of 307 subjects, 170 men (55.4%) and 137 women (44.6%). The mean age of the study subjects was 52.0±11.2. The mean duration of diabetes was 6.4±5.8 years, and 52 (16.9%) subjects were taking insulin. The mean BMI was 25.8±9.7 kg/m2, mean waist circumference was 90.5±8.1 cm, mean glycated hemoglobin was 8.2±1.8%, mean fasting blood glucose was 154.0±54.0 mg/dL, and the mean 2 hour postprandial blood glucose was 233.7±88.9 mg/dL. The mean PAID-K score was 47.5±17.5, the mean HFS score was 39.7±13.9, and the mean STAI-6 score was 14.1±2.6 (Table 1).
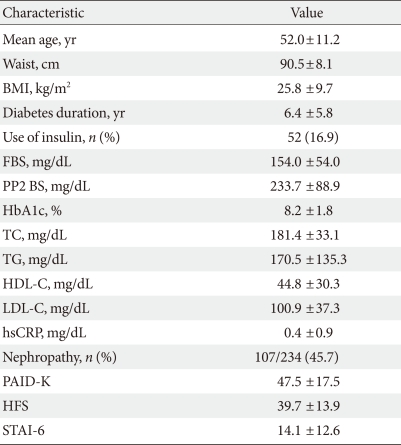
Clinical characteristics of study subjects (n=307)
Validation of PAID-K efficacy and correlations between PAID-K and characteristics
Cronbach's alpha for the translated PAID-K was 0.95. HFS was r=0.44 (P<0.05), and STAI-6 was r=0.21 (P<0.05). Here, we detected a significant correlation (Table 2). The PAID-K scores were significantly higher in patients with longer durations of diabetes and female patients (P=0.02, P=0.001, respectively), but there was no difference based on age. The PAID-K score in insulin group was significantly higher than in non-insulin group (51.6±15.7 vs. 46.6±17.9, P=0.038), and the PAID-K score in microalbuminuria group was also higher than in group without nephropathy, but this difference was not statistically significant (P=0.05) (Table 3). Glycated hemoglobin was directly related to the score (P for trend<0.05), but the group with very high glycated hemoglobin (over 11%) had lower PAID-K ratings (Fig. 1). PAID-K score was affected by gender (P=0.004) in a linear regression analysis, however, the score was unaffected by age, duration of diabetes, insulin usage, or the presence of diabetic nephropathy (Table 4).
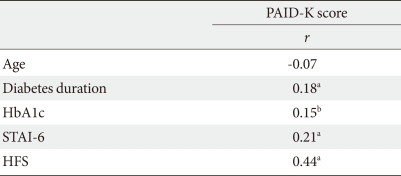
Correlations between PAID-K scores and age, diabetes duration, HbA1c, STAI-6, and HFS
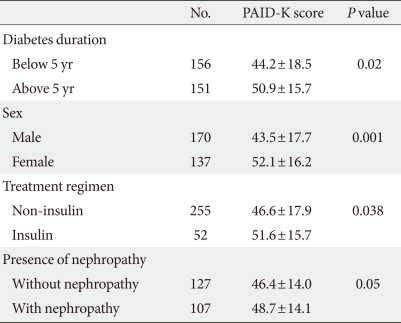
Comparisons of PAID-K scores according to clinical characteristics in study subjects
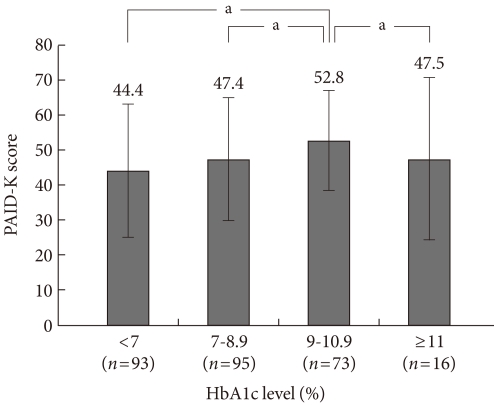
Problem Areas in Diabetes (PAID)-K score per category of HbA1c level. aP<0.05.

Multiple linear regression analysis between PAID-K scores and dependent variables
DISCUSSION
We developed the PAID-K questionnaire, and used it to assess stress of Korean type 2 diabetic patients at three medical centers. Scores for the PAID-K, STAI-6, and HFS were associated in our sample, and the PAID-K was shown to be an effective method to evaluate stress in diabetics.
Ismail et al. [8] noted that work-related stress and loss of family-induced stress were factors leading to diabetes, and Thernlund et al. [3] reported that experiencing stress or trauma in the first two years of life can put children at risk for developing type 1 diabetes. Stress stimulates the hypothalamus-pituitary-adrenal axis, and causes changes in the levels of several hormones, particularly increased serum cortisol concentrations and reduced sex hormone levels, which antagonize insulin action and elevate blood glucose levels [6]. Cortisol not only interferes with insulin action, but also plays a role in suppressing insulin secretion in pancreatic beta cells.
Diabetes itself is also a cause of stress. Compared to the general population, diabetes patients have higher levels of stress, and as stress levels increase, glycemic control deteriorates. Therefore, psychiatric supportive therapy is beneficial for controlling blood glucose levels [9,11].
The risk of depression is increased in diabetic patients [16]. However, early, appropriate diabetes treatment and stress management can help reduce suffering from diabetes and depression [17].
The methods that are used for evaluating and measuring stress are complex and diverse. Generally, the methods include measurements for stress-inducing factors, measurements of stress reactions, individual perception for stress reactions, and measurements of analysis and coping methods [18,19]. The evaluation of stress-inducing factors was previously performed using the Holmes and Rahe social readjustment rating scale [20], and events that cause continuous major changes in lifestyle, such as illness, divorce, or work were prioritized. In addition, there are other tests such as the daily life experience checklist, Hassle scale, inventory of small life events, daily stress scale, and daily stress inventory. In order to evaluate physiological responses related to stress, we evaluated autonomic nervous system response, stress hormone and endocrine response, neuropeptides, neurotransmitters and immune function. In order to assess cognitive-behavioral stress responses, we used the stress response perception scale. To assess individual coping methods and personality types for comparison to stress responses, the perceived stress factor scale, response strategy, coping method scale, and A type behavioral characteristic scale were used [18].
The PAID questionnaire used in this study was consulted as a simple method for measuring diabetes-related stress in American patients with type 1 and type 2 diabetes. The PAID questionnaire is clinically useful, and has been validated as an effective evaluation method, which is why has been translated into several languages and is widely used around the world [21]. The PAID questionnaire efficiently assesses diabetes-related factors affecting quality of life, and is advantageous due to its brevity compared with the ATT39 and QSD-R [13].
The 20 questions of the PAID questionnaire are divided into four categories: diabetes-related emotional problems (DP), treatment-related problems (TP), food-related problems (FP), and social support-related problems (SP). The PAID questionnaire was used in 2000 to evaluate Dutch and American diabetic patients. According to that comparative study, the mean scores of Dutch type 2 diabetic patients were DP 15.1±13.5, TP 2.3±3.0, FP 3.7±3.7, and SP 1.6±2.4, totaling 22.5±19.8, and in American type 2 diabetic patients, the mean scores were DP 17.9±15.6, TP 3.2±3.3, FP 4.8±3.9, and SP 1.8±2.4, totaling 27.8±23 [21]. The mean scores of the Korean participants of the present study were DP 31.8±11.6, TP 5.5±2.4, FP 6.4±2.7, and SP 3.7±2.1, totaling 47.5±17.5, and the category scores and total scores were higher than those of American and Dutch patients in the comparative study [21]. Generational differences, geographical differences, and healthcare environment differences are all thought to be factors explaining the discrepancies, however, even if these effects are considered, future research on why stress scores are so high in Korean diabetic patients is needed because the differences are so large. When the items of PAID questionnaire were examined, Dutch and American diabetic patients had the highest scores in response to the 'worrying about the future and the possibility of serious complications' question, and Korean patients had the highest scores in response to the 'feeling scared when you think about living with diabetes' question, with the second highest score was in response to the 'worrying about the future and the possibility of serious complications' question.
Snoek et al. [21] reported that PAID scores increase more as glycated hemoglobin increases and is higher in female patients than in male patients . Additionally, according to a study conducted by Polonsky et al. [22], PAID values appear higher as glycated hemoglobin increases and in diabetics with complications. In this study, the PAID-K scores of female patients were higher than those of male patients (P=0.001), and PAID-K scores were higher in patients with microalbuminuria but this difference was not statistically significant (P=0.05). In addition, as glycated hemoglobin increases, PAID-K scores show an increasing trend (P for trend<0.05), but in unusual cases in which glycated hemoglobin was extremely high (over 11%), the score was relatively low. It is thought that stresses about diabetes control and self-management may be lower in patients with high levels of glycated hemoglobin due to low personal interest in health.
Medication, diet control, and exercise are all essential to the treatment of diabetes, but it is also important to have mental and emotional support to continuously maintain these activities. Therefore, psychological and social factors must also be evaluated, and these evaluations can help the overall treatment of diabetic patients.
Many of the subjects of this study experienced diabetes-related stress. Patients stress management is equally as important as drug therapy, education and management of complications. Much of the stress can be ameliorated by support from physicians and caretakers, along with repeated education. Further studies are needed to investigate the degree to which stress can be improved by such support and education.
In practice, it is unreasonable to gauge the overall stress levels of diabetes patients through only a 20-item questionnaire. However, the PAID-K questionnaire is useful for evaluation of Korean diabetic patients in that diabetes-related stress levels can be indirectly identified for short periods of time using it. It is expected that implementing more detailed and ongoing psychological and social support would be helpful for overall diabetes management in patients with high PAID-K scores.
ACKNOWLEDGMENT
This study was supported by a grant of the Korea Healthcare Technology Research and Development Project, Ministry of Health and Welfare, Republic of Korea (A05-0463-B50704-05N1-00040B).