A Clinical Practice Guideline to Guide a System Approach to Diabetes Care in Hong Kong
Article information

Abstract
The Hospital Authority of Hong Kong is a statutory body that manages all the public medical care institutions in Hong Kong. There are currently around 400,000 diabetic patients under its care at 17 hospitals (providing secondary care for 40%) and 73 General Outpatient Clinics (providing primary care for 60%). The patient population has been growing at 6% to 8% per year over the past 5 years, estimated to include over 95% of all diagnosed patients in Hong Kong. In order to provide equitable and a minimal level of care within resources and local system factors constraints, a Clinical Practice Guideline on the management of type 2 diabetes mellitus was drawn in 2013 to guide a system approach to providing diabetes care. There is an algorithm for the use of various hypoglycemic agents. An organizational drug formulary governs that less expansive options have to be used first. A number of clinical care and patient empowerment programs have been set up to support structured and systematic diabetes care. With such a system approach, there have been overall improvements in diabetes care with the percentage of patients with glycosylated hemoglobin <7% rising from 40% in 2010 to 52% in 2015.
INTRODUCTION
The prevalence of diabetes mellitus has continued to rise worldwide with the latest estimation by the International Diabetes Federation that, by the year 2040, one in 10 adults or 642 million people will have diabetes [1]. Tackling its rise and the health burden arising from the disease is a major challenge to almost all health care systems. Hong Kong, returned to the sovereignty of China as a Special Administrative Region from the United Kingdom, is no exception. Being the most developed region of China, its prevalence of diabetes is higher than the national average. The direct medical cost for managing diabetes and its complications was estimated to take up 3.9% of the total healthcare expenditure and 6.4% of the public health expenditure [2].
THE HEALTH CARE SYSTEM OF HONG KONG
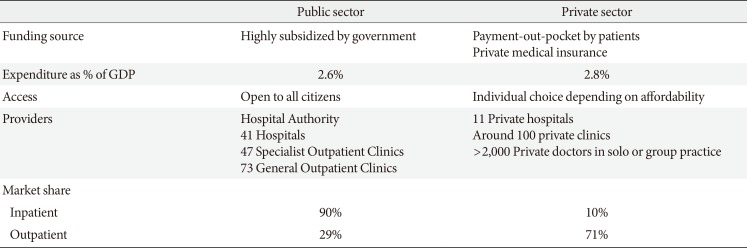
Hong Kong has a dual track system with public and private care along each other. For historical reasons, specialist and inpatient care is mainly provided by the public sector (90%), which also provides 29% of primary outpatient care through the General Outpatient Clinics (GOPCs). However, in the, hitherto, absence of an universal health insurance or co-payment scheme, much of the primary care provided by the public sector actually involves caring for people with chronic diseases, since most of them find long term treatment of their conditions by private doctors difficult to afford. The Hospital Authority (HA) of Hong Kong is a statutory body set up to provide all public health care services in the territory. It manages 41 hospitals and institutions, 47 Specialist Outpatient Clinics, which together provide inpatient and specialist care; and 73 GOPCs where primary care for the early stages of chronic diseases for most patients is delivered. These hospitals and clinics are organised into seven geographical clusters to provide a continuum of primary and specialist services to the citizens. The expenditure of the HA is largely dependent on government funding which amounts to HK$50.76 billion (~USD 6.5 billion) and constitutes less than half of the 5.4% of the gross domestic product (GDP) that is spent on health care in Hong Kong (Table 1). A recent Bloomberg news coverage ranked the health care system of Hong Kong the most efficient in the world [3]. Therefore, it is obvious that the HA has been running on a very tight budget.

The dual-track health care system of Hong Kong
THE BURDEN AND CHALLENGE OF DIABETES TO THE HOSPITAL AUTHORITY OF HONG KONG
The prevalence of diabetes in Hong Kong is about 10% [4]. With a population of 7.4 million, it is estimated that there are about 740 thousand diabetic patients, 40% to 50% of whom are undiagnosed. However, the number of diabetic patients under the care of the HA has been rising steadily from 397 thousand in 2009/2010 to 408 thousand in 2015/2016 (Fig. 1). Annually, 33 to 35 thousand new diabetic patients are added to the public health care system (Fig. 2). The rise is likely contributed to by earlier diagnosis among the undiagnosed because of increased awareness of diabetes in the community; attraction of more patients from the private to the public sector; an increase in the prevalence of diabetes due to an increase in the incidence among younger people, etc. Thus, diabetes is a major burden to the HA because it is estimated that more than 90% of the known diabetic patients are under its care.

Total number of diabetic patients under the care of the Hong Kong Hospital Authority.
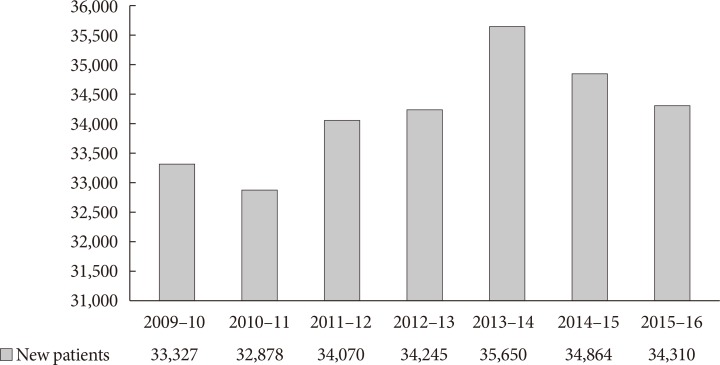
Number of diabetic patients new to the Hospital Authority.
With the background of forerunners in research and service development, the HA started a journey of a system approach to providing diabetes care across the whole public health care system in 2009. A Central Committee on Diabetic Services was set up to steer the development. The following strategies have been adopted:
Service data were captured and analysed through the electronic Clinical Management System.
Clinical modules in the Clinical Management System to facilitate clinical care for diabetes and capture diabetes specific clinical data.
Corporate Clinical Practice Guideline (CPG) on the management of type 2 diabetes: first published 2013; currently being reviewed to be updated in 2017.
Large scale programmes to enhance diabetes care including a territory-wide multi-disciplinary Risk Assessment and Management Program for diabetes (RAMP-DM) and a structured Patient Empowerment Program (PEP) in the GOPCs.
Regular monitoring of performance indicators.
THE HOSPITAL AUTHORITY CLINICAL PRACTICE GUIDELINE ON THE MANAGEMENT OF TYPE 2 DIABETES (2013)
The intent of the guideline was to describe the minimal level of care to be provided across the different care levels in the HA, with due consideration of available evidence and local systems factors. On the other hand, a service framework outlining the cycle of periodic assessment, risk stratification for different management and patient empowerment strategies and regular follow-up at the different care levels was included (Fig. 3). Importantly, patient empowerment is considered an integral component of diabetes care. An algorithm was drawn to guide the use of the various glucose lowering agents (Fig. 4). The management of hypertension and dyslipidemia was discussed with a view to minimizing cardiovascular risk. Although the targets for glycosylated hemoglobin (HbA1c), blood pressure and low density lipoprotein cholesterol (LDL-C) are to be individualized, those recommended by international guidelines in 2013 were adopted for suitable patients (Table 2). There is also guidance on the management of the various chronic complications of diabetes. Criteria for referral to specialists such as endocrinologists, ophthalmologists, orthopaedic, and vascular surgeons were outlined.
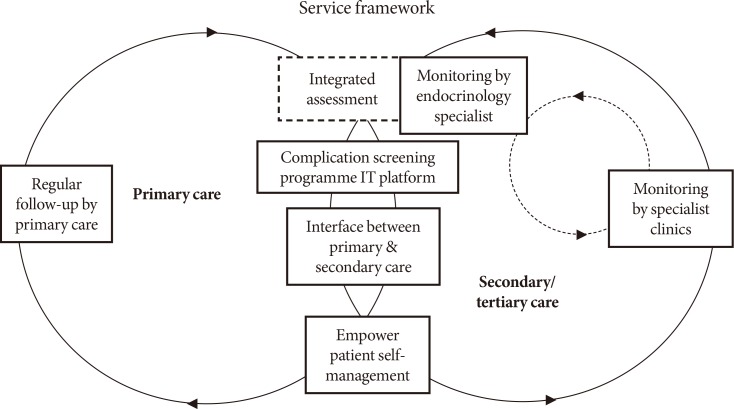
Hospital Authority's service framework for the provision of diabetes care.

Algorithm for blood glucose lowering therapy. DPP-4, dipeptidyl peptidase-4; CI, confidence interval; HbA1c, glycosylated hemoglobin.

Treatment target values for adult patients with type 2 diabetes
A special note should be made regarding the use of drugs, including glucose lowering agents, in the HA. There is a corporate drug formulary in which drugs are classified into general, special, and self-financed items. General drugs can be freely used by all doctors; special drugs can only be used for specific clinical indications by designated specialists; self-financed items are purchased by their patients out-of-pocket if the clinical indications are not met or present. The formulary effectively governs that less expensive options have to be used first unless or until they are not tolerated or effective, which helps contain the drug expenditure. The formulary is periodically reviewed to take into consideration new clinical evidence, changes in prize and introduction of new drugs or formulations. Thus, metformin, sulphonylureas, and human insulin are general drugs, to which pioglitazone was recently added as its price has come down. DDP-4 and sodium/glucose cotransporter 2 inhibitors are special drugs that can only be used when the combination of metformin and sulphonylureas with or without pioglitazone fail to control glycemia. Insulin analogues can only be used for patients with repeated hypoglycemia while on human insulin or patients with established cardiovascular and renal complications. Glucagon-like peptide-1 analogues are self-financed items because of the high prices.
MULTIDISCIPLINARY RAMP-DM
In 2009, the HA introduced a multidisciplinary RAMP-DM to improve the quality of care for patients receiving diabetic care in the GOPCs [5]. All patients with type 2 diabetes mellitus who are independent in their activities of daily living and being followed up regularly at the GOPCs are eligible for the RAMP. Enrolled patients undergo a comprehensive risk assessment with checking of relevant clinical parameters including HbA1c, blood pressure, LDL-C, and screening for diabetes-related complications according to a standardized protocol. After the assessment, patients are classified into different risk groups according to the Joint Asia Diabetes Evaluation (JADE) criteria [6] and are offered different management options to receive appropriate interventions and education provided by a team of multidisciplinary healthcare professionals. Low risk patients continue with the usual GOPC care; medium risk patients are given additional intervention by a nurse with special training in diabetes; and high risk/very high risk patients are reviewed by a specialist family physician for intensification. About two-thirds of the diabetic patients under the care of the GOPCs (277,309 in 2015/2016) have been enrolled.
The effect and effectiveness of the RAMP-DM has been evaluated by three prospective cohort studies. Thus, it was found that there was a significant decrease in HbA1c (−0.20%, P<0.01), systolic blood pressure (SBP; −3.62 mm Hg, P<0.01), 10-year cardiovascular disease (CVD) risks (total CVD risk, −2.06%, P<0.01; coronary heart disease [CHD] risk, −1.43%, P<0.01; stroke risk, −0.71%, P<0.01) at 12 months in a random sample of 1,248 patients enrolled to RAMP-DM compared with an age-, sex-, and HbA1c-matched group of unenrolled 1,248 patients under the usual primary care. There was a rise in the percentage of patients reaching treatment targets of HbA1c (5.4%, P<0.01), and SBP/diastolic blood pressure (5.77%, P<0.01) and a lower cardiovascular events incidence (1.21% vs. 2.89%, P=0.003) [7]. More significantly, in another prospective cohort study of 18,188 propensity score matched RAMP-DM participants and patients receiving the usual primary care with a median follow-up of 36 months (9,094 subjects in each group), there were significantly lowered adjusted hazard ratios (HRs) in the RAMP-DM group compared with the usual care group in all-cause deaths (0.363; 95% confidence interval [CI], 0.308 to 0.428; P<0.001); CHD (0.570; 95% CI, 0.470 to 0.691; P<0.001); stroke (0.652; 95% CI, 0.546 to 0.780; P<0.001); and congestive heart failure (0.598; 95% CI, 0.446 to 0.802; P=0.001) [8]. Further, a third study comparing RAMP-DM participants with subjects under the usual primary care (14,835 in each group) with a median follow-up of 36 months, RAMP-DM participants had a lower incidence of microvascular complications (760 vs. 935; adjusted HR, 0.73; 95% CI, 0.66 to 0.81; P<0.001) and lower incidences of all specific microvascular complications except neuropathy (adjusted HR, 0.94; 95% CI, 0.61 to 1.45; P=0.778). Adjusted HRs for the RAMP-DM versus control group for end stage renal disease, sight threatening diabetic retinopathy or blindness, and lower-limb ulcers or amputation were 0.40 (95% CI, 0.24 to 0.69; P<0.001), 0.55 (95% CI, 0.39 to 0.78; P=0.001), and 0.49 (95% CI, 0.30 to 0.80; P=0.005), respectively [9]. Although these are not randomized controlled trials, the careful matching, large numbers of patients and long duration of follow-up meant that a program of risk assessment and stratification followed by appropriate intervention is likely to be high effective in improving long term clinical outcomes.
PATIENT EMPOWERMENT PROGRAM
Life style modification through patient empowerment has long been considered an important and integral component of management of diabetes. Diabetic self-management education, whether delivered on an individual or group setting, has been shown to improve glycemic and cardiovascular risk factor control [101112]. In 2010, the Hong Kong Hospital Authority launched the PEP as a territory-wide primary care component with the purpose of improving the quality of care. The curriculum of the PEP, designed by a group of specialist diabetes nurse educators, was delivered in six sessions by trained healthcare workers in community centers run by non-government organizations. There was a generic component covering behavior modification, healthy diet and regular exercise habit, goal setting and problem solving skills, sharing on self-monitoring experience, stress coping management, psychosocial support and networking, and communications with healthcare professionals. A second, disease-specific component dealt with specific knowledge about diabetes, medications, and management of hypo- and hyperglycemia.
In an observational matched cohort study comparing a random sample of PEP participants with a group of matched control, each consisting of 1,141 subjects, the PEP group had an average decrease of 0.138% in the HbA1c level (95% CI, −0.252 to −0.024; P=0.017) more than the control group. The PEP group also achieved a significant decrease in the mean LDL-C value (0.254 mmol/L, P<0.001), and the decrease was significantly more (−0.136 mmol/L; 95% CI, −0.223 to −0.048; P<0.001) than that of the control group [13]. More importantly, three prospective cohort studies, each comparing a group of more than 12,000 PEP participants with a group of matched control of the same number of patients with a median follow-up of more than 21 months, have been published. PEP participants had a lower rate of all-cause mortality (HR, 0.564; 95% CI, 0.445 to 0.715; P<0.001), first CVD (HR, 0.807; 95% CI, 0.696 to 0.935; P=0.004), and stroke (HR, 0.702; 95% CI, 0.569 to 0.867; P=0.001) than those without PEP [14]. PEP participants were associated with a lower incidence of first microvascular event (HR, 0.85; 95% CI, 0.78 to 0.94; P=0.001) and nephropathy (HR, 0.71; 95% CI, 0.62 to 0.80; P<0.001) than non-PEP participants, after adjusting for confounding variables [15]. There were a significantly lower number of emergency department visits (incidence rate ratio, 0.903; P<0.001): 40.4 visits per 100 patients annually among the PEP group versus 36.2 per 100 patients annually in the control group; and significantly fewer hospitalization episodes (incidence rate ratio, 0.854; P<0.001): 20.0 hospitalizations per 100 patients annually in the PEP group versus 16.9 hospitalizations per 100 patients annually in the control group [16]. To date, the PEP is the first structured diabetic self-management education program shown to improve mortality, macro- and microvascular complications, and utilization of health services.
OVERALL IMPROVEMENT IN DIABETIC CONTROL
In order to monitor the overall improvement in diabetic control, the percentage of all the patients under the care of the Hospital Authority with HbA1c below 7% has been captured from the laboratory information system of the corporate electronic Clinical Management System. The percentage improved from 33% in 2008/2009 to over 50% in 2015/2016 (Fig. 5), reflecting that the strategies have been effective in improving the overall control. This will probably translate into a decrease in the incidence of complications. The experience of Hong Kong demonstrated that a system approach, comprising a CPG to guide clinical care, a system for ensuring that the key care processes of assessment, risk stratification and appropriate multidisciplinary interventions are implemented, is required to tackle the problem.

Percentage of diabetic patients under the care of Hospital Authority achieving glycosylated hemoglobin <7%.
CONCLUSIONS
Charged with the responsibility for providing a health care safety net for all citizens of Hong Kong, the HA has to provide efficient and effective care for the majority of people with diabetes in the city within a very tight budget. However, since all the public hospitals and clinics are under its management, it has the advantage of being able to adopt a system approach to organize diabetes care across the different levels of health care settings for the whole continuum of the disease. The organizational CPG sets the standard of care, covering the following areas: (1) diagnosis; (2) minimal processes in outpatient management; (3) patient self-education as an integral component of management; (4) glucose lowering therapy; (5) control of cardiovascular factors; (6) regular screening for diabetic complications at 1 to 3 years' intervals; and (7) inpatient management of hyperglycemic emergencies and perioperative situations. A number of programs have been set up to support systemic and structured care, including a 6-class interactive PEP for early disease run by non-governmental organizations; education through telephone calls by trained nurses; a structured complication assessment program; an insulin initiation program at the GOPCs; control intensification at diabetes centers at hospitals. Various key performance and clinical indicators are regularly monitored across different hospitals and clinics to assure quality. The provision of diabetes care by the HA is an integral and representative component of the highly efficient and regarded public health care system of Hong Kong, which many economies, including mainland China [17], can learn from.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.