Efficacy of Moderate Intensity Statins in the Treatment of Dyslipidemia in Korean Patients with Type 2 Diabetes Mellitus
Article information

Abstract
Background
There has been evidences of ethnic differences in the low density lipoprotein cholesterol (LDL-C) lowering effect of statin. We aimed to evaluate the efficacy of moderate-intensity statins in the treatment of dyslipidemia among Korean patients with type 2 diabetes mellitus (T2DM).
Methods
We analyzed a retrospective cohort that consisted of Korean patients with T2DM aged 40 to 75 years who had been prescribed any of the moderate-intensity statins (atorvastatin 10 or 20 mg, rosuvastatin 5 or 10 mg, pitavastatin 2 mg, or pravastatin 40 mg). Among them, only patients with baseline lipid profiles before starting statin treatment were selected, and changes in their lipid profiles before and 6 months after statin therapy were analyzed.
Results
Following the first 6 months of therapy, the overall LDL-C reduction was −47.4% (interquartile range, −56.6% to −34.1%). In total, 92.1% of the participants achieved an LDL-C level of <100 mg/dL, 38.3% had a 30% to 50% reduction in their LDL-C levels, and 42.3% had a reduction in their LDL-C levels greater than 50%. The response rates of each drug for achieving a LDL-C level <100 mg/dL were 81.7%, 93.1%, 95.0%, 95.0%, 96.5%, and 91.7% for treatment with atorvastatin doses of 10 or 20 mg, rosuvastatin 5 or 10 mg, pitavastatin 2 mg, and pravastatin 40 mg, respectively.
Conclusion
In conclusion, the use of moderate-intensity statins reduced LDL-C levels less than 100 mg/dL in most of the Korean patients studied with T2DM. The efficacies of those statins were higher than expected in about 42% of Korean patients with T2DM.
INTRODUCTION
Statins are a mainstay treatment for reducing cardiovascular risk in type 2 diabetes mellitus (T2DM) patients. The current treatment objectives for dyslipidemia in T2DM patients have been based on the third report from the National Cholesterol Education Program-Adult Treatment Panel; that is, targeted at reducing low density lipoprotein cholesterol (LDL-C) levels to below 100 mg/dL as a primary prevention, and below 70 mg/dL as a secondary prevention [1]. However, the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guidelines on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults did not recommend specific treatment targets since most of the trials regarding statins and cardiovascular outcomes did not test for specific LDL-C goals [2]. In addition, ACC/AHA recommended a specific dose of statin based on lipid-lowering efficacy [2] from previous clinical trials [34567]. In contrast, the current treatment guidelines for dyslipidemia recommended by the Korean Society of Lipidology and Atherosclerosis, the Korean Academy of Medical Sciences, or the Korean Diabetes Association, provide actual LDL-C target levels [8910]. The discrepancies among the treatment guidelines for dyslipidemia have evoked many debates, one of which pertains to statin efficacy. The 2013 ACC/AHA guideline recommended that patients with T2DM aged between 40 and 75 years should be prescribed a moderate-intensity or high-intensity statin [2]. Specifically, they divided the statins by LDL-C lowering efficacy and defined a moderate-intensity statin as a statin that results in lowering the LDL-C level by 30% to 50%, and a high-intensity statin as a statin that results in lowering the LDL-C level by more than 50%.
Some reports have found that the LDL-C lowering effect of statins in Asians can be more prominent than in Caucasians [1112]; however, these results were not consistent [13]. There have been few studies that have compared the effects of several different statins among Korean patients. We found only one Korean study that compared the LDL-C lowering effects of six different statins [14]. This study suggested that the LDL-C lowering effects of the statins were greater in Korean patients than in Caucasians and concluded that using a low dose of statin was enough to manage dyslipidemia in most Korean patients with low-to-moderate cardiovascular risks. However, less than 10% of the patients enrolled in this study had T2DM and the percentage of LDL-C reduction was in the range of previously reported results.
In this study, we aimed to evaluate the efficacy of the moderate-intensity statins suggested by the 2013 ACC/AHA guidelines for use in the treatment of dyslipidemia among Korean patients with T2DM. Furthermore, we evaluated the proportion of patients who achieved a LDL-C level <100 mg/dL after treatment with moderate-intensity statins for 6 months.
METHODS
Study population
This was a single-center retrospective study with the primary objective of determining the effect of moderate-intensity statins on LDL-C levels in Korean patients with T2DM. Patient inclusion criteria was as follows: (1) diagnosed with T2DM and of Korean ethnicity; (2) aged 40 to 75 years; (3) began moderate-intensity statin therapy between January 2014 and May 2015; (4) did not have a history of cardiovascular disease; and (5) had an available baseline lipid profile before starting statin therapy. Moderate-intensity statins were defined following 2013 ACC/AHA guidelines [2]: atorvastatin 10 or 20 mg, rosuvastatin 5 or 10 mg, pitavastatin 2 mg, or pravastatin 40 mg. This study was approved by the Institutional Review Board of Seoul Metropolitan Government Seoul National University Boramae Medical Center.
Efficacy assessments
Pharmacological efficacy was evaluated by a retrospective analysis of the medical records of patients who were treated with atorvastatin 10 or 20 mg, rosuvastatin 5 or 10 mg, pitavastatin 2 mg, or pravastatin 40 mg for 6 months. The primary end-point was the percentage of patients who achieved a LDL-C level <100 mg/dL. The secondary end points were as follows: the percentage of patients whose LDL-C levels decreased from their baseline values by 30% to 50%, or by more than 50%, the absolute change and percentage of the change of LDL-C levels before and after treatment, and the percentage change of total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), and triglyceride (TG) levels before and after treatment.
Safety assessments
Safety was assessed by retrospective analysis of the medical records of patients who were treated with the aforementioned moderate-intensity statins for 6 months. The safety variables were musculoskeletal and hepatic adverse events, and the percentage change in glycosylated hemoglobin (HbA1c) levels. Musculoskeletal adverse events were defined as a musculoskeletal symptom described in the patient's electrical health record during the study. Hepatic adverse events were defined as an elevation in the levels of alanine aminotransferase (ALT) or aspartate aminotransferase (AST) over three times of the patient's baseline levels.
Laboratory and cardiovascular risk assessments
All participants fasted for 12 hours before blood samples were taken. Fasting TC, HDL-C, LDL-C, and TG levels were measured using an enzymatic colorimetric method (Toshiba Medical System Co. Ltd., Tokyo, Japan). HbA1c level was determined using high-performance liquid chromatography (SST; Becton, Dickinson and Company, Franklin Lakes, NJ, USA). Ten-year atherosclerotic cardiovascular disease (ASCVD) risk was assessed based on 2013 ACC/AHA guidelines on the assessment of cardiovascular risk [15].
Statistics
The continuous parameters were presented as mean±standard deviation. The categorical data were shown as proportions. Within group comparisons (treatment effects) were evaluated by paired t-test. Comparisons across the statin groups were calculated by analysis of variance with the use of P for the continuous parameter with normal distribution, Kruskal-Wallis analysis for the continuous parameter with non-normality distribution, and chi-square test with P for the linear-by-linear test for the categorical variables. A P<0.05 was considered significant. Statistical analyses were carried out using the SPSS version 22.0 statistical package (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics of study participants
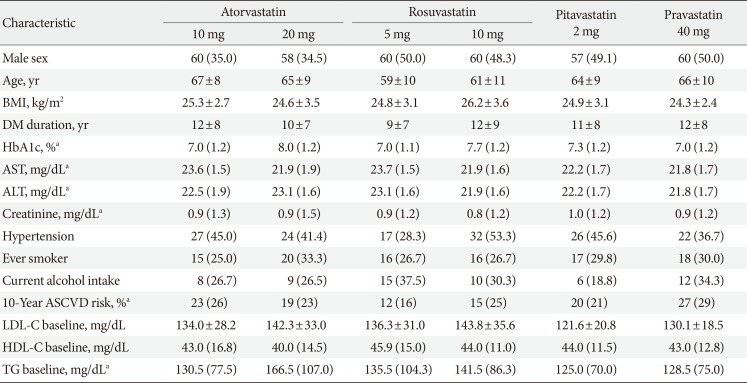
A total of 355 participants were evaluated for the efficacy and safety of their statin treatment. The characteristics of the study subjects according to the various statins are shown in Table 1. The mean age was 64±10 years, and the number of female participants was 197 (55.5%). The average duration of T2DM was 11±8 years, and the median HbA1c level was 7.4% with an interquartile range (IQR) of 1.4%. The baseline characteristics were not significantly different among the groups with regard to sex, body mass index (BMI), diabetes duration, serum AST, ALT, creatinine level, hypertension, tobacco use, and consumption of alcohol. The mean age of the participants in the rosuvastatin 5 mg group was 59±10 years, which was lower than that of the atorvastatin 10 mg group (67±8 years, P<0.001); however, the mean age was not significantly different among the other groups. In addition, serum HbA1c level was significantly higher in the atorvastatin 20 mg group than in the other groups (8.0%; IQR 1.2%; P<0.001). The 10-year ASCVD risk was relatively lower in the rosuvastatin 5 mg group than in the pravastatin 40 mg group (12%; IQR 16%). Baseline LDL-C levels were significantly higher in the atorvastatin 20 mg and the rosuvastatin 10 mg group than in the pitavastatin 2 mg group.

Baseline characteristics according to types of statin
Changes and goal achievement of LDL-C levels
After treatment with moderate-intensity statins for 6 months, the LDL-C levels were significantly decreased in all statin treatment groups (Table 2). The median changes in LDL-C levels over 6 months were −63.0 mg/dL ( −47.4%) in total, and −61.5 mg/dL (−44.1%), −67.0 mg/dL (−48.2%), −73.0 mg/dL (−51.6%), −84.0 mg/dL (−56.0%), −51.0 mg/dL (−41.7%), −56.0 mg/dL (−42.4%) in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively (Table 2).

The change of LDL-C levels after 6 months of statin treatment
Overall, a total of 92.1% of the participants achieved LDL-C level <100 mg/dL after 6 months, where 38.3% of the patients had reduction in their LDL-C levels between 30% and 50%, and 42.3% of the patients had reduction in their LDL-C levels greater than 50% from their baseline levels. The percentages of patients who achieved LDL-C level of <100 mg/dL were 81.7%, 93.1%, 95.0%, 95.0%, 96.5%, 91.7%, and the percentages of patients who achieved LDL-C level reduction of 30% to 50% from their baseline values were 46.7%, 31.0%, 36.7%, 16.7%, 50.9%, 48.3% in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively. The percentages of patients who had LDL-C level reduction greater than 50% from their baseline values were, 33.3%, 48.3%, 55.5%, 70.0%, 19.3%, and 26.7% in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively.
Changes in levels of HDL-C, TG, TC, and 10-year ASCVD risk
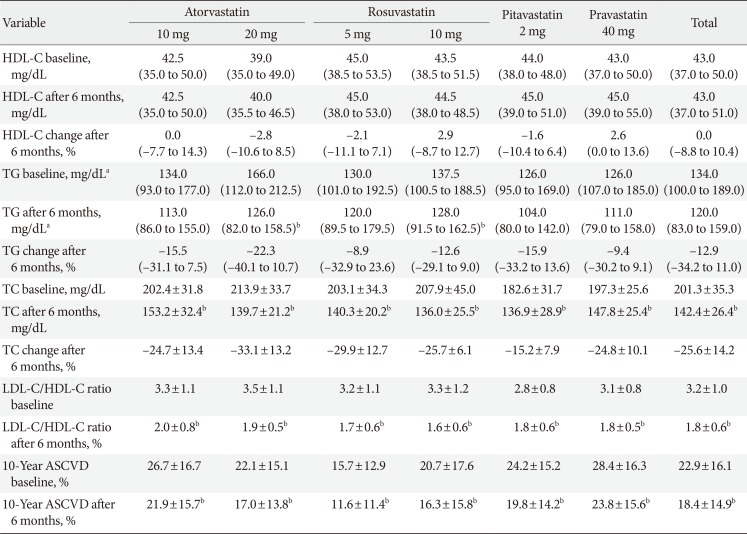
After treatment with moderate-intensity statins for 6 months, TC levels, LDL-C/HDL-C ratios, and 10-year ASCVD risks were decreased in all statin treatment groups. TG levels were decreased only in the atorvastatin 20 mg and rosuvastatin 10 mg groups. HDL-C levels were not significantly changed in all groups (Table 3).

The change of HDL-C, TG, TC levels, and 10-year ASCVD risks after 6 months of statin treatment
Overall, the median percentage change over 6 months was 0% for HDL-C levels, −12.9% for TG levels, and −25.6% for TC levels. The percentage changes for each of the drug groups in regards to HDL-C levels were 0%, −2.8%, −2.1%, 2.9%, −1.6%, and 2.6%, and the percentage changes in TG levels over 6 months were −15.5%, −22.3%, −8.9%, −12.6%, −15.9%, and −9.4% in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively. The percentage changes in TC levels were −24.7%, −33.1%, −29.9%, −25.7%, −15.2%, and −24.8% in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively.
The number of participants who achieved levels of LDL-C <100 mg/dL, HDL-C ≥50 mg/dL, TG <150 mg/dL [16] after 6 months was 18 (30.0%), 12 (20.7%), 18 (30.0%), 19 (31.7%), 20 (35.1%), 14 (23.3%) in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively. The percentages of each group showed no significant difference among the groups (P=0.526).
Safety assessment of the various statins
Musculoskeletal adverse events were not detected among all participants. Hepatic adverse events were found in a total of two subjects, one in the rosuvastatin 5 mg group and one in the rosuvastatin 10 mg group. The change in HbA1c levels was evaluated in 190 of the patients (53.5%) who did not change their oral hypoglycemic agents. The HbA1c levels did not change significantly after statin treatment, with the changes being 0.00% (IQR, −0.30% to 0.50%) in total, 0.05% (IQR, −0.35% to 0.30%), −0.10% (IQR, −1.20% to 0.50%), −0.30% (IQR, −0.20% to 0.60%), −0.05% (IQR, −0.60% to 0.40%), 0.00% (IQR, −0.45% to 0.35%), and 0.00% (IQR, −0.10% to 0.70%) in the atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg groups, respectively. The number of participants whose statin treatment was started at the same time with new hypoglycemic agents was 57 (16.1%); the number of participants whose hypoglycemic agents were reduced during statin treatment was 39 (10.9%), and those whose hypoglycemic agents were added or increased was 69 (19.4%). The proportion of patients whose hypoglycemic agents reduced or increased during the 6 months of statin treatment did not show a significant difference among the statin treatment groups (P=0.832).
DISCUSSION
In this study, treatment with a moderate-intensity statin in Korean patients with T2DM achieved the LDL-C target goal (<100 mg/dL) in 92.1% of the participants, and the LDL-C levels were reduced by 63.0 mg/dL (−47.4% from baseline). Among all participants, 38.3% achieved LDL-C reduction of 30% to 50% from baseline, and 42.3% achieved reduction in their LDL-C levels of more than 50%. The HDL-C and TG levels did not significantly change after 6 months of statin therapy.
In this study, most of the T2DM patients treated with a moderate-intensity statin suggested by the 2013 ACC/AHA treatment guidelines had achieved the target LDL-C level outlined by the Korean guidelines for dyslipidemia. However, 42.3% of the patients achieved greater than a 50% reduction in their LDL-C levels, and this result was as effective as treatment with a high-intensity statin. On the other hand, 19.4% of the participants achieved less than a 30% reduction in their LDL-C levels, despite being treated with a moderate-intensity statin. It has been suggested that the LDL-C lowering effect of statins could be more prominent in Asians than in Caucasians, and that a relatively low-dose statin could be used to manage dyslipidemia in Korean patients with low-to-moderate risks [1114]. The reported LDL-C level reduction rates in representative Caucasian studies were −35.7%±7.1% [3], −42.6%± 10.5% [4], −39.1%±9.0% [5], −52.1%±7.5% [4], −37.9%± 14.0% [6], and −26.0%±8.8% [7] for atorvastatin 10, 20 mg, rosuvastatin 5, 10 mg, pitavastatin 2 mg, and pravastatin 40 mg, respectively. A meta-analysis of randomized, double-blind statin trials showed similar findings with regard to the LDL-C level reduction rates such as 36.8% in patients treated with 10 mg of atorvastatin, 29.7% in patients treated with 40 mg of pravastatin, and 45.8% in patients treated with 10 mg of rosuvastatin [17]. Although a direct comparison could not be made owing to the lack of actual LDL-C level data, the LDL-C reduction rates found in our study were higher than the previous reported ranges of Caucasians. These findings suggest that some moderate-intensity statins could be prescribed for Korean patients with T2DM resulting in higher efficacies than we expect for Caucasian patients. In particular, rosuvastatin had a considerably higher LDL-C lowering effect than other statins in this study. The reason for this high efficacy could be explained by the different pharmacokinetics of rosuvastatin in Asian populations. Plasma levels of rosuvastatin and its metabolites such as N-desmethyl rosuvastatin and rosuvastatin-lactone were significantly higher in Asians than in Caucasians. This difference could be partly explained by an increased prevalence of polymorphisms in the SLCO1B1 and ABCG2 genes in Asian populations, which could influence hepatic clearance of the enzyme CYP2C9 [1218]. Further studies are needed to discover other genetic or epigenetic changes which could cause ethnic differences after administration of rosuvastatin.
Comparing the cholesterol-lowering effects of low-dose statins with one Korean study, the efficacies of atorvastatin 10 mg, rosuvastatin 5 mg, and pitavastatin 2 mg were similar to those of our study [14]. Another Korean study including T2DM patients treated with atorvastatin also showed a similar result to that of our study [19]. Since these data consistently show higher treatment efficacies than those of Caucasians using moderate-intensity statins, redefining moderate-intensity statins for the Korean population is needed in further research and official discussions.
Considering the interindividual variation in statin efficacy and a recent study that has demonstrated the progression of atheroma in hyporesponders to statin therapy [8], it is important to monitor LDL-C levels during and after statin treatment.
During statin therapy, the 2013 ACC/AHA guidelines recommend that the measurement of hepatic function is needed only when hepatotoxicity symptoms are suspected [2]. In this study, treatment with a moderate-intensity statin did not result in patients presenting with hepatotoxicity, which was statistically significant, in all the groups. Also, musculoskeletal adverse events were not reported, although these events were based on self-reported symptoms in the chart reviews. Moreover, recent studies suggest that statin treatment increases the risk of diabetes [20]. In this study, changes in the HbA1c levels were not significant after statin treatment in participants who did not change their diabetic medications during the study periods. Among participants who changed their diabetic medications, there was no significant difference between the proportion of participants who reduced or increased diabetic medications during 6 months of statin treatment (P=0.832). However, due to the retrospective design of this study, it would be difficult to evaluate the exact effect of statins on HbA1c levels in those who changed their hypoglycemic agents during the statin therapy.
The strength of this study is that we evaluated the efficacy of commonly prescribed statins in Korean patients with T2DM and analyzed the actual discrepancy between the policy of the 2013 ACC/AHA guidelines and the targeted goal approach recommended by the Korean Society of Lipidology and Atherosclerosis, the Korean Academy of Medical Sciences, or the Korean Diabetes Association. By providing results demonstrating a reduction in LDL-C levels in patients previously prescribed various moderate-intensity statins, this study will aid physicians in their decision regarding the appropriate intensity statin therapy for the treatment of dyslipidemia in patients with T2DM. In addition, we tried to solve the bias caused by poor adherence to drug therapy by reviewing the charts thoroughly and excluding those patients with poor adherence according to their prescription-refill records. There are some limitations in our study. First, this is a retrospective study that depends only on chart reviews; therefore, confounding factors could not be fully evaluated or matched. Importantly, in this retrospective analysis, factors including sex, BMI, and tobacco use from chart reviews did not show significant differences among the groups. Remaining confounding factors such as diet habits or physical activities must be considered in additional prospective studies. Second, the number of participants may not have been sufficient for comparing the efficacy among the different statins. Third, some patients who required a high-intensity statin were prescribed a moderate-intensity statin by the physicians' decision. According to the 2013 ACC/AHA guidelines, it has been suggested that diabetic patients who have a 10-year ASCVD risk of more than 7.5% should be treated with a high-intensity statin. Of note, the average 10-year ASCVD risk in our study subjects was more than 20%. However, whether the 10-year ASCVD risk assessment model fits well in the Korean population needs to be discussed in further research since the risk calculation model in the 2013 ACC/AHA guidelines is based on non-Hispanic Caucasian and African American population.
In summary, treatment with a moderate-intensity statin in Korean patients with T2DM achieved LDL-C less than 100 mg/dL in most of the study subjects. This study also showed that moderate-intensity statins defined by the 2013 ACC/AHA guidelines have higher efficacies than expected in about 42% of Korean patients with T2DM. Further research is needed to define moderate-intensity statins and to recommend an adequate statin therapy regimen for the Korean population.
ACKNOWLEDGMENTS
This study was supported from by grant No. 03-2012-0290 from the Seoul National University Hospital Research Fund.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.