Clinical Course and Risk Factors of Diabetic Retinopathy in Patients with Type 2 Diabetes Mellitus in Korea
Article information

Abstract
Background
We investigated clinical course and risk factors for diabetic retinopathy (DR) in patients with type 2 diabetes mellitus (T2DM).
Methods
A total of 759 patients with T2DM without DR were included from January 2001 to December 2004. Retinopathy evaluation was performed at least annually by ophthalmologists. The severity of the DR was classified into five categories according to the International Clinical Diabetic Retinopathy Severity Scales.
Results
Of the 759 patients, 523 patients (68.9%) completed the follow-up evaluation. During the follow-up period, 235 patients (44.9%) developed DR, and 32 patients (13.6%) progressed to severe nonproliferative DR (NPDR) or proliferative DR (PDR). The mean duration of diabetes at the first diagnosis of mild NPDR, moderate NPDR, and severe NPDR or PDR were 14.8, 16.7, and 17.3 years, respectively. After adjusting multiple confounding factors, the significant risk factors for the incidence of DR risk in patients with T2DM were old age, longer duration of diabetes, higher mean glycosylated hemoglobin (HbA1c), and albuminuria. Even in the patients who had been diagnosed with diabetes for longer than 10 years at baseline, a decrease in HbA1c led to a significant reduction in the risk of developing DR (hazard ratio, 0.73 per 1% HbA1c decrement; 95% confidence interval, 0.58 to 0.91; P=0.005).
Conclusion
This prospective cohort study demonstrates that glycemic control, diabetes duration, age, and albuminuria are important risk factors for the development of DR. More aggressive retinal screening for T2DM patients diagnosed with DR should be required in order to not miss rapid progression of DR.
INTRODUCTION
Diabetic retinopathy (DR) is one of the major microvascular complications of diabetes, and the most common cause of nontraumatic visual loss in the working-age population [1]. It has been estimated that the global prevalence of DR was 93 million (35%) and the prevalence of vision-threatening diabetic retinopathy (VTDR) was 28 million (10.2%) among diabetes patients in 2010 [2]. In Korea, the prevalence of retinopathy in diabetes was reported to be 18.6% according to the 2011 Korea National Health and Nutritional Examination Survey [3]. It is anticipated that the prevalence of DR and VTDR is likely to continue to rise, particularly in Asia and other developing areas [4]. In addition, DR is a risk marker for systemic vascular complications. Independent of conventional risk factors, the presence of retinopathy, even in its mildest form, was associated with a two to three times higher risk of cardiovascular disease (CVD) [5]. Thus, regular retinal screening is a cornerstone of diabetes care, and evidence-based retinal screening is helpful in reducing the development and progression of DR. To detect DR at an optimal stage for intervention, the American Diabetes Association and Korean Diabetes Association recommend that after the diagnosis of type 2 diabetes mellitus (T2DM), patients should receive an initial dilated and comprehensive eye examination by an ophthalmologist, and subsequent annual examinations [67].
Identifying the natural course and risk factors of DR is important because the screening strategy depends on the rates of development and progression of DR. The development and progression of DR have been evaluated through multiple epidemiologic studies. One previous study suggested that 38% of T2DM patients develop any type of DR in a 6-year period [8]. In the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR), approximately 10% of diabetic patients developed severe visual impairment within 15 years of being diagnosed with diabetes [9]. Several studies, including the Diabetes Control and Complication Trial (DCCT), the UK Prospective Diabetes Study (UKPDS), and the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, have noted risk factors related to DR such as poor glycemic control and hypertension [101112]. It is well known that optimum control of blood glucose and blood pressure level is associated with a reduced risk in the onset and progression of DR in T2DM [111213]. Although some lipid-lowering agents have recently emerged as possible therapeutic agents for DR [1415], there are conflicting studies examining the relationship between DR and long-term risk factor status, including serum lipid levels, and medications, especially in Asian populations [16171819].
Thus, the aim of this prospective study was to evaluate the natural course and predictive factors of DR among patients with T2DM in Korea.
METHODS
In this study, 1,195 patients aged 25 to 75 years old who were diagnosed with T2DM were consecutively enrolled from January 2001 to December 2004. We excluded 436 patients from the study cohort who had any type of DR, secondary diabetes, alcoholism, or had any severe illness such as heart failure, liver cirrhosis, severe infection, or had malignancy. Patients who had a history of gestational diabetes mellitus or who were pregnant during the study were also excluded. Patients received follow-up until between 2013 and 2015, depending on the individual and their treatment plan, at the university-affiliated Diabetes Center of St. Vincent's Hospital in South Korea. This prospective cohort study was approved by the Catholic Medical Center Ethics Committee and was performed according to the Declaration of Helsinki. Written informed consent was obtained from all participants.
A detailed questionnaire was collected from all patients to obtain information including age, gender, duration of diabetes, current smoking status, medical history, and use of medications. Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or current use of antihypertensive medication [20]. We defined smoking as current or past smokers within 3 years preceding enrollment in the study. Alcohol consumption was defined as drinking any type of alcoholic beverage at least once a week for a period of 6 months or longer. Glycosylated hemoglobin (HbA1c) was collected at baseline and at least every 6 months, and fasting plasma glucose (FPG), postprandial plasma glucose, serum creatinine, total cholesterol, triglyceride (TG), high density lipoprotein cholesterol (HDL-C), and low density lipoprotein cholesterol (LDL-C) were collected at baseline and at least annually. Lipid profiles were measured enzymatically using an automatic analyzer (model 736-40; Hitachi, Tokyo, Japan). The urinary albumin excretion rate was measured by enzyme immunoassay using immunoturbidimetry with a 24-hour urine collection (Eiken, Tokyo, Japan), and the presence of albuminuria was defined as urine albumin excretion over 30 mg/day. The estimated glomerular filtration rate (eGFR) was calculated using the four-component Modification of Diet in Renal Disease equation [21]. A cardiovascular autonomic function test using the Ewing method was performed in all enrolled patients at baseline. At least two abnormal results were defined as definite cardiovascular autonomic neuropathy [22]. Medication utilization was assessed for insulin, angiotensin-converting enzyme (ACE) inhibitor/angiotensin II receptor blocker (ARB), statin, fenofibrate, and aspirin from enrollment to the end of the follow-up period. Prior CVD history was defined as a diagnosed history of coronary artery disease or cerebrovascular disease. The clinical diagnosis of CVD based on verified medical records was confirmed by specialists from each clinical department including cardiology, neurology, and neurosurgery [23].
A standardized comprehensive eye examination was performed annually by experienced ophthalmologists. After maximal dilatation of the pupil, retinal images were obtained using a digital fundus camera (TRC-NW6S; Topcon, Tokyo, Japan) equipped with a Nikon D-80 digital camera (Nikon, Tokyo, Japan), and digital fundus images were obtained from all participants. For each of the participants, one 45 digital retinal image centered on the fovea was obtained per eye (two images per person in total). The comprehensive eye examination frequency was determined by the ophthalmologist, depending on the severity of the DR. Agreements of eye examination between ophthalmologists were evaluated as Cohen's κ coefficient and kappa statistics ranged from 0.76 to 0.84. The severity of the DR was classified according to the international clinical diabetic retinopathy severity scales into five categories: nondiabetic retinopathy (equivalent to the Early Treatment Diabetic Retinopathy Study [ETDRS] scale level 10), mild nonproliferative diabetic retinopathy (NPDR; equivalent to the ETDRS scale level 20), moderate NPDR (equivalent to the ETDRS scale level 35, 43, 47), severe NPDR (equivalent to the ETDRS scale level 53A–53E), and proliferative diabetic retinopathy (PDR; equivalent to the ETDRS scale level ≥61) [2425]. If both eyes were rated at different stages, then the grade of the worst eye was used. The primary endpoint was to identify the development of DR in patients who did not have any type of DR at baseline [12].
The normality test was performed to evaluate the distribution of data. Data are presented mean±standard deviation (SD) or, in the case of a skewed distribution, as median (interquartile range). Chi-square tests were used to test differences in the proportion of categorical variables, and independent Student t-tests were used to evaluate the difference between the mean of two continuous variables. The incidence rate of DR was determined by dividing the number of cases of incident retinopathy by the total number of patient-years accumulated in the study by patients without DR at baseline. The duration of DR was estimated by the measurement of the mean duration of diabetes at the first diagnosis at each stage of DR progression. We applied multivariate Cox proportional hazards models to test the associations between new onset DR and the related risk factors after adjusting for the following covariates: sex, age, duration of diabetes, presence of hypertension, body mass index (BMI), prior CVD history, mean HbA1c level, albuminuria, eGFR, use of insulin, ACE inhibitors, ARBs, aspirin, statin, or fenofibrate. Covariates were selected by considering the clinical and statistical relevance as identified in previously published literature and by using the current dataset between the primary outcome and variables. The proportional hazards assumption was confirmed using log-minus log-survival plots and tested with the methods previously described elsewhere [26]. These results were reported as hazard ratios (HRs) with a 95% confidence interval. Statistical analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). P<0.05 was considered significant.
RESULTS
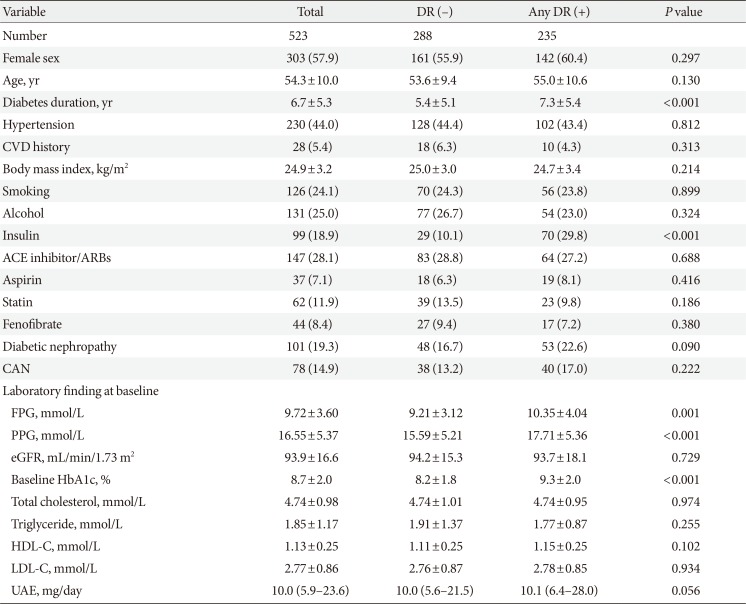
Of the 759 patients who were included the study, 523 patients (68.9%) completed the follow-up. Table 1 shows the baseline characteristics of the patients. The mean age was 54.3 years and mean duration of diabetes was 6.7 years. Compared with the 523 participants who completed the follow-up evaluation, the 236 patients who did not complete the follow-up evaluation did not differ with respect to age (54.3±10.0 years vs. 55.9±11.1 years, P=0.059), the female ratio (57.9% vs. 55.1%, P=0.463), the duration of diabetes (6.7±5.3 years vs. 6.3±5.3 years, P=0.329), the presence of hypertension (44.0% vs. 47.5%, P=0.372), or mean HbA1c (8.2%±1.2% vs. 8.2%±1.6%, P=0.950) during the follow-up period.

Comparison of baseline parameters between the patients with and without diabetic retinopathy
The median follow-up time was 11.8 years (interquartile range, 9.8 to 13.2). During the follow-up period, 235 patients (44.9%) developed DR. The incidence rate of DR was 38.1 per 1,000 patient-years. Among the 235 patients who developed DR, 32 patients (13.6%) progressed to the severe nonproliferative DR or proliferative DR during the follow-up period. Among them, 31 patients (13.2%) received panretinal photocoagulation treatment. The mean duration of diabetes of mild NPDR, moderate NPDR, and severe NPDR or PDR diagnosis are shown in Fig. 1.
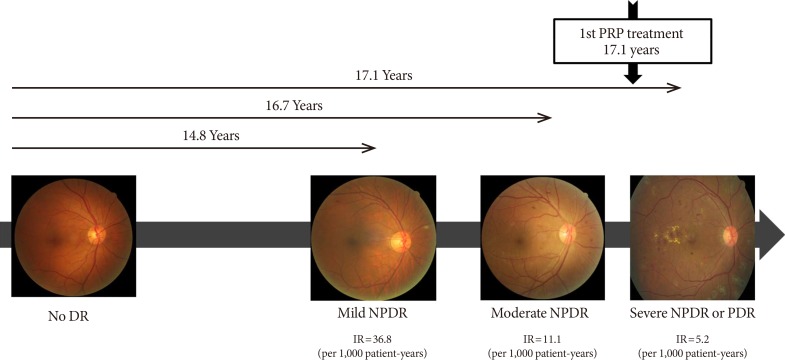
Clinical course of diabetic retinopathy in this cohort. PRP, panretinal photocoagulation; DR, diabetic retinopathy; NPDR, nonproliferative diabetic retinopathy; IR, incidence rate; PDR, proliferative.
For patients who received the follow-up care, data at the baseline visit showed that individuals who developed DR, had been diagnosed with diabetes for a longer time, had higher FPG and baseline HbA1c levels, and had greater use of insulin compared with nonincidence cases (Table 1). On the other hand, there were no differences in the presence of hypertension, BMI, prior CVD history, smoking, cardiovascular autonomic dysfunction, baseline eGFR, and serum lipid levels between the patients with DR and without DR.
The group with DR had a higher mean HbA1c during the follow-up period (8.0%±0.9% vs. 8.5%±1.1%, P=0.005). Two patients (0.9%) who maintained a mean HbA1c level below 6.5% and 16 patients (6.8%) who maintained a mean HbA1c level below 7.0% developed DR. The incidence rate of DR increased as the mean HbA1c level increased. The SD of HbA1c and the coefficient of variation (CV) of HbA1c during the study also showed significant differences between the group with and without DR.
Regarding the mean level of lipid profiles during the study, mean total cholesterol, mean TG, mean HDL-C, and mean LDL-C showed no significant difference between the groups with and without DR (Supplementary Table 1, Fig. 2). Also, mean TG/HDL ratio and mean non-HDL did not differ between the two groups (Supplementary Table 1). The use of statin, fenofibrate, and aspirin also had no influence on the incidence of DR. There were no differences in the incidence of DR between patients who used those medications during the follow-up and those who did not (Supplementary Table 1).
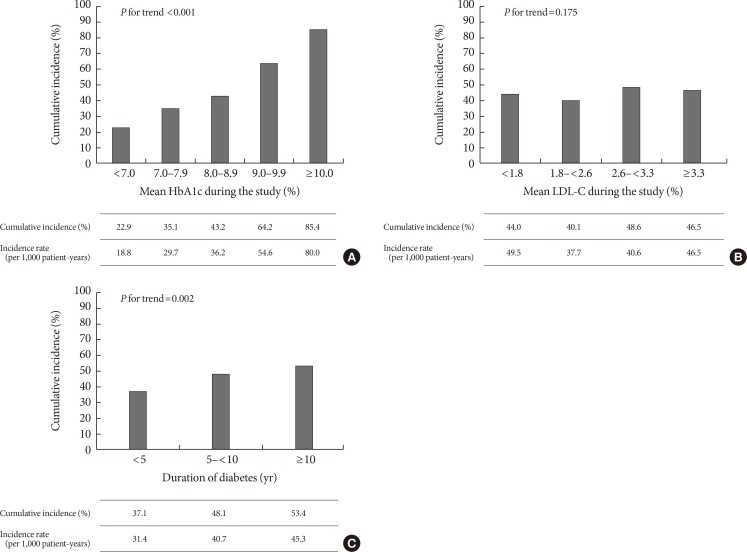
Cumulative incidence for diabetic retinopathy according to the (A) mean glycosylated hemoglobin (HbA1c), (B) mean low density lipoprotein cholesterol (LDL-C) level, and (C) duration of diabetes.
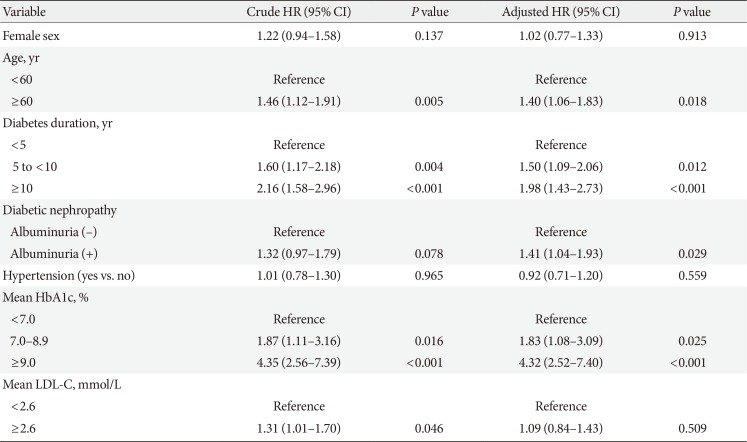
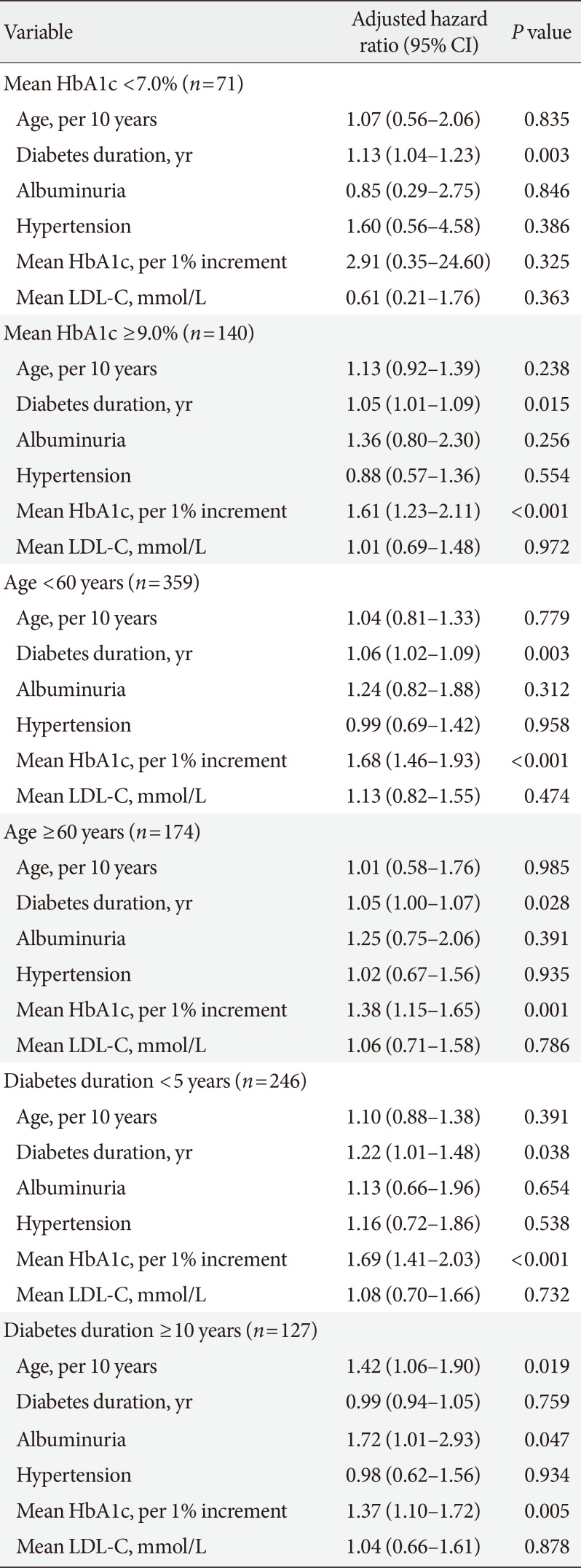
The univariable analysis for incidence of DR showed that age, diabetes duration, use of insulin, FPG, baseline HbA1c, mean HbA1c, and albuminuria were revealed as potential risk factors of DR. After adjusting for confounding factors, the group who had poor glycemic control during the follow-up (mean HbA1c ≥9%) showed 4.32 times higher risk of DR than those who had good glycemic control (mean HbA1c <7%) (Table 2). In addition, a 1% increase in mean HbA1c resulted in a 54% increase in the risk of developing DR during the follow-up (P<0.001). However, there was no significant association between mean lipid parameters during the follow-up periods, the presence of hypertension, BMI, use of medications, and the development of DR. We assessed an association between DR and related risk factors within the subgroup stratified by mean HbA1c, age, and diabetes duration (Table 3). Among the 140 patients who maintained poor glycemic status (mean HbA1c ≥9.0%), the significant predictive factors for DR included a longer diabetes duration and a higher level of mean HbA1c. In the 71 patients who maintained good glycemic status during the study (mean HbA1c <7.0%), only a longer duration of diabetes was a significant factor for the incidence of DR. In the group whose duration of diabetes was over 10 years at baseline, age, albuminuria, and mean HbA1c remained significant factors for developing DR. During the follow-up, a 1% decrease in HbA1c led to a 69% reduction in the risk of developing DR in the group who had a duration of diabetes less than 5 years at baseline. In addition, in the group who had a duration of diabetes for over 10 years at baseline, a 1% decrease in HbA1c led to a 37% reduction in the risk of developing DR. There was no additional increase of HR in patients who maintained higher glucose (mean HbA1c ≥9%) and higher lipid levels (mean LDL-C ≥3.3 mmol/L) simultaneously during the study (P for interaction =0.720, data not shown). SD- and CV-HbA1c did not have a significant result as a predictive factor for DR after adjusting for confounding factors (data not shown).

Crude and adjusted hazard ratio for the development of diabetic retinopathy

Association between major variables and development of diabetic retinopathy
DISCUSSION
In this long-term analysis, old age, longer duration of diabetes, higher mean HbA1c, and albuminuria appeared to significantly increase the incidence of DR risk in patients with T2DM in Korea. Dyslipidemia, hypertension, and BMI did not show any relationship with the development of DR even in the stratified subgroup analysis.
Glycemic control is a well-known factor that can prevent or delay the incidence of DR. The UKPDS found that strict control of blood glucose was essential for the prevention of DR. In the results, HbA1c was 7% in the intensive group as compared with 7.9% in the conventional group, and the risk of DR in the intensive group was 21% lower than in the conventional group [11]. The ACCORD trial also showed that the progression of DR was reduced in the intensive glycemic control group compared with the standard treatment group [12]. However, the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) and the Veterans Affairs Diabetes Trial (VADT) reported no ocular benefit for DR incidence of intensive glycemic control [2728]. Possible explanations for the discrepancy include differences between the studies in the patients' age, duration of diabetes, previous glycemic control status, and assessment of DR. In this study, we demonstrated that the strongest predictive factor of the incidence of DR was mean HbA1c during the follow-up, as expected. Another interesting finding of our study is that proper glycemic control can reduce the possibility of DR development, even in the patients with a long duration of diabetes. Several studies have suggested that diabetes duration is one of the strongest and nonmodifiable risk factors for DR [29]. Thus, achieving proper glycemic control might help to reduce the risk of DR in patients who have a long diabetes duration. Conflicting results have been reported about the effect of HbA1c variability on diabetic microvascular complications [303132]. A recent meta-analysis concluded that HbA1c variability did not appear to be associated with DR in T2DM [33]. However, most of the studies were retrospective, and inconsistency existed in the definition of HbA1c variability. Our findings were remarkably similar to the conclusion of a recent meta-analysis, and no significant associations were found between both SD-, CV-HbA1c, and DR.
There have been numerous clinical trials and observational studies on the association between dyslipidemia and DR [16343536]. However, it remains uncertain whether dyslipidemia is related with the incidence and progression of DR. In some studies, a significant association has been found between dyslipidemia and DR. The WESDR showed that serum total cholesterol was significantly associated with the presence and severity of hard exudates in young-onset diabetes [37]. In the Atherosclerosis Risk In Communities (ARIC) study, subjects with a higher LDL-C level were more likely to have retinal hard exudates [35]. It is plausible that serum lipid level might be associated with DR, since dyslipidemia are known to cause endothelial dysfunction by reducing the amount of biologically active nitric oxide, and this endothelial dysfunction was suggested to play a role in retinal exudate formation in DR [38]. However, most studies have reported that there is no association between traditional lipid levels and DR [16343639]. In our study, there was no association between total cholesterol, TG, HDL-C, LDL-C, TG/HDL-C, and non-HDL and DR among all patients. In addition, no additional benefit for DR was observed in the group with simultaneous glycemic and lipid control.
Previous studies suggested that use of statin, fenofibrate, or aspirin may affect the natural course of DR. Also, other conflicting results have been reported about the role of lipid-lowering agents and aspirin for DR. The results of the Effect of Fenofibrate on the need for Laser Treatment for Diabetic Retinopathy (FIELD) and ACCORD studies suggested that fenofibrate could reduce the need for laser treatment for DR [1214], and were also less likely to demonstrate the progression of a preexisting retinopathy. In the Steno-2 trial, multifactorial treatment such as intensive use of aspirin and lipid-lowering agents sustained benefits in microvascular complications including the progression of DR and laser treatment for PDR or diabetic macular edema [40]. The Collaborative Atorvastatin Diabetes Study suggested that statin showed no effect on the progression of DR [41]. A recent Spanish cohort study suggested that use of aspirin increased the risk of DR [42], while ETDRS reported there was no evidence for the effect of aspirin on the DR incidence [2443]. In our cohort, we adjusted for the long-term exposure (over 75% period during the follow-up) to medication as well as baseline medication use. As a result, the use of statin, fenofibrate, and aspirin did not affect the incidence of DR in this cohort. Also, the presence of hypertension and BMI at baseline was not associated with the development of DR.
There have been few studies that explore the natural course of DR because this requires a long-term investigation. The previous study suggested the average time for the development of NPDR from no DR was estimated as 14.5 years [44]. We indirectly measured the average time to develop DR as a calculation of duration of diabetes for the first diagnosis of DR for the patients who reached each stage of DR. As a result, the mean duration for the development of mild NPDR was approximately 14.8 years, and progression time to moderate NPDR, severe NPDR, or PDR was 16.7 and 17.3 years, which was similar to previous studies. This result showed that the rate of DR progression was considerably fast for the patients who progressed to severe form of DR. In agreement with previous studies, we re-confirmed that strict glycemic control and frequent retinal examination is important for T2DM patients after the first diagnosis of DR to not miss rapid progression of DR.
The strength of this study is that it was a long-term, prospectively designed cohort study with regular comprehensive examinations by ophthalmologists. Also, we used the long-term mean value of glycemic and lipid data to evaluate the accurate metabolic status of each patient. However, there are several limitations to this study. First, mean blood pressure and BMI data were incomplete during the follow-up in this study. Thus, we could not evaluate the exact effect of blood pressure and BMI on the development of DR. Second, we used the International Clinical Diabetic Retinopathy Severity Scales which categorize DR into five stages. We could not grade the DR stage more in detail or the ETDRS severity scale classification. However, the International Clinical Diabetic Retinopathy Severity Scale is also commonly used by ophthalmologists on a routine clinical basis. Third, lifestyle, such as eating habits and exercise patterns, in T2DM patients is an important factor that affects the progression of the complications [45]. However, we could not collect the data of patients' lifestyles in this study during the follow-up. These residual confounding factors due to unmeasured factors cannot be excluded. Finally, the participants in this study were the patients who attended the diabetes center of a general hospital. For generalization, larger studies using more defined populations are required to better understand the relationship between DR and related risk factors.
In conclusion, we suggest that risk factors such as glycemic control, duration of diabetes, age, and albuminuria are the important risk factors for the development of DR. Specifically, we suggest that glycemic control is the most important modifiable factor, even in the patients who had a long duration of diabetes. However, there were no significant relationships between traditional serum lipid levels, a presence of hypertension, BMI, and DR in this cohort study. From the results of the natural course of DR, annual to biennial screening for DR in accordance with current guidelines may be sufficient in patients without DR. However, for the patients who are diagnosed early with DR, more aggressive and frequent screening is needed for early detection of DR progression. Also, further identification of novel markers for the residual risk of retinopathy are needed to prevent the development of diabetic complication risk.
ACKNOWLEDGMENTS
The authors thank H.R. Kim and H.J. Kang (St. Vincent's Hospital, College of Medicine, The Catholic University of Korea) for their assistance collecting and analyzing data for this manuscript.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
Supplementary Material
Supplementary Table 1
Comparison of clinical parameters between the patients with and without diabetic retinopathy