Blood Pressure Target in Type 2 Diabetes Mellitus
Article information

Abstract
The prevalence of diabetes mellitus continues to increase worldwide, and it is a well-established cardiovascular risk factor. Hypertension is also an important cardiovascular risk factor to be controlled and is common among patients with diabetes mellitus. Optimal blood pressure (BP) goals have been the subject of great debate in the management of hypertension among patients with diabetes mellitus. This review provides detailed results from randomized controlled trials and meta-analyses of clinical outcomes according to the target BP in patients with type 2 diabetes mellitus. In addition, the target BP in patients with diabetes mellitus recommended by different guidelines was summarized and presented. A target BP of <140/90 mm Hg is recommended for patients with hypertension and diabetes mellitus, and BP should be controlled to <130/80 mm Hg in patients with diabetes mellitus who have high-risk clinical features. We hope that this review will be helpful to clinicians and patients by promoting the understanding and appropriate application of BP control in the comprehensive management of patients with diabetes mellitus.

INTRODUCTION
The prevalence of type 2 diabetes mellitus continues to increase worldwide, with 537 million adults aged 20 to 79 years suffering from diabetes mellitus in 2021. It is estimated that this number will increase to 783 million by 2045 according to the International Diabetes Federation Diabetes Atlas [1]. The prevalence of diabetes mellitus has also consistently increased in the last 7 years in Korea, with an estimated prevalence of 16.7% in 2020 [2]. Diabetes mellitus is a well-established modifiable risk factor for atherosclerotic cardiovascular disease (ASCVD) [3-6] and ranks among the top 10 leading causes of disability-adjusted life-years [7]. High blood pressure (BP) is also the most important risk factor for ASCVD which can be controlled, and hypertension is common among patients with diabetes mellitus [3,8]. According to the Korean hypertension fact sheet 2020, 26% of all hypertensive patients >20 years of age received diabetes mellitus treatment together [9]. In addition, 58.6% of patients with adult diabetes mellitus have hypertension, and only 55.5% of them have hypertension controlled with a BP of 140/85 mm Hg according to the Diabetes Fact Sheet in Korea 2021 [2]. Since uncontrolled high BP is an important risk factor for heart failure (HF), atrial fibrillation, chronic kidney disease, valvular heart disease, dementia, coronary heart disease (CHD), and stroke, it is necessary to properly control BP [3,10]. However, the optimal BP target has been a subject of great debate among patients with diabetes mellitus, and there are differences in the target BP of active control in previous studies and recommendations by each guideline. Considering these differences and the divergence of opinions, clinicians may be confused about BP management in patients with diabetes mellitus.
In this article, we have detailed reviews on how to set the optimal BP target in patients with diabetes mellitus and diabetes mellitus with various comorbidities, based on recent evidence and guidelines.
TARGET BLOOD PRESSURE IN PATIENTS WITH DIABETES MELLITUS ACCORDING TO CURRENT GUIDELINES
The optimal BP target for patients with diabetes mellitus has been debated and recommendations for the management of hypertension and diabetes mellitus have changed over time. Table 1 shows the guidelines containing recommendations on the BP target and thresholds in patients with diabetes mellitus from the Joint National Committee (JNC) 8 guidelines to the recent American Diabetes Association (ADA) 2022 guidelines. In most guidelines [8,11-17], the diagnostic threshold for hypertension was defined as ≥140/90 mm Hg, until the American College of Cardiology/American Heart Association (ACC/AHA) guidelines were published in 2017, and JNC 8 recommended that the BP target should be adjusted to <140/90 mm Hg in patients with diabetes mellitus as well as in the general population. In 2017, as the importance of intensive BP control was emphasized through the Systolic Blood Pressure Intervention Trial (SPRINT) [18] and the benefit of cardiovascular (CV) outcome was proven, there was a change in the diagnostic threshold for high BP and optimal BP targets than in the past. Based on evidence of the benefits of intensive BP control, the 2017 ACC/AHA guidelines recommended that optimal BP targets should be adjusted to less than office BP 130/80 mm Hg for both the general hypertensive population and those with diabetes mellitus [12]. In fact, the SPRINT trial was a study of a population excluding patients with diabetes mellitus; however, intensive BP control was applied to them without exception in this guideline. The European guidelines were different from the ACC/AHA guidelines regarding the target BP of the diabetic patients. The 2018 European Society of Cardiology (ESC)/European Society of Hypertension guidelines recommended that office systolic blood pressure (SBP) should be targeted to 130 mm Hg and lower if tolerated. For older patients (age ≥65 years), target SBP should be 130 to 140 mm Hg if tolerated. They recommended that diastolic blood pressure (DBP) should be lowered to <80 mm Hg. But BP should not be lowered to <120/70 mm Hg. They maintained the diagnostic threshold of hypertension at ≥140/90 mm Hg [13]. This is reflected because there is evidence that adjusting SBP and DBP to <120 and <70 mm Hg, respectively, may be more harmful than beneficial to clinical outcomes in high-risk patients, such as those with diabetes mellitus [19,20]. According to a reanalysis study of results from the ongoing telmisartan alone and in combination with ramipril global endpoint trial (ONTARGET) and telmisartan randomised assessment study in ace intolerant subjects with cardiovascular disease (TRANSCEND) trials [19,21,22], adjusting SBP to <120 mm Hg was related to an increased risk of poor CV outcome as well as adjusting DBP to <70 mm Hg in patients with high-risk hypertension. In the Action to Control Cardiovascular Risk in Diabetes Blood Pressure Trial (ACCORD-BP) [20], there was no benefit in CV outcomes, including nonfatal myocardial infarction (MI), nonfatal stroke, and CV death in the group with a target SBP of <120 mm Hg and a mean SBP of 119.3 mm Hg compared with a target SBP of 130 to 140 mm Hg and a mean SBP of 135 mm Hg, and the risk of stroke was reduced, but serious adverse events occurred more frequently. These data suggest that the lowest possible BP target is not necessarily optimal for high-risk patients. This BP target did not differ from the BP target for patients with diabetes mellitus in the 2019 ESH/European Association for the Study of Diabetes (EASD) guideline [16]. In particular, in patients with diabetes mellitus who have a high CV risk profile accompanied by cardiovascular disease (CVD) (coronary artery disease [CAD], peripheral vascular disease, aortic disease, HF, or left ventricular hypertrophy who are ≥50 years of age), intensive BP control of <130/80 mm Hg is recommended, as in the 2017 ACC/AHA guidelines. According to the results of a separate analysis of high-risk patients with diabetes mellitus who met the SPRINT study inclusion criteria in the ACCORD-BP trial (one or more among the presence of clinical or subclinical CVD, chronic kidney disease with estimated glomerular filtration rate 20 to 59 mL/min/1.73 m2, Framingham Risk Score for 10-year ASCVD risk ≥15%, or age ≥75 years), it was based on evidence that controlling BP <130/80 mm Hg for patients with diabetes mellitus, CVD and baseline characteristics of both study subjects could improve CV outcomes [23]. This recommendation is the same as the BP target for patients with diabetes mellitus and those with CVD in the recent 2021 Korean Diabetes Association guidelines [17]. The latest guidelines of the 2022 ADA recommend that BP should be controlled to <140/90 mm Hg in patients with diabetes mellitus, but <130/80 mm Hg if there is a higher CV risk with existing ASCVD or 10-year ASCVD risk of ≥15% [8]. These recommendations are similar to the BP target for high-risk patients with diabetes mellitus in the Korean guidelines and for patients with diabetes mellitus in the European guidelines. Although the recommendations about optimal BP target are slightly different from guideline to guideline, it is important to evaluate CV risk in patients with diabetes mellitus and to control BP by predicting CV outcomes. Therefore, the importance of individualized treatment is emphasized for patients with diabetes mellitus and hypertension, and since defining a high-risk profile and the presence of CVD are different for each guideline, careful review and appropriate application of these guidelines to patients with diabetes mellitus are important (Fig. 1). As shown in Fig. 1, strict BP control (BP <130/80 mm Hg) is recommended for diabetic patients with high-risk clinical features defined as having a CV risk factor one or more, the presence of CVD, subclinical organ damage, or stage 3, 4, or 5 chronic kidney disease.
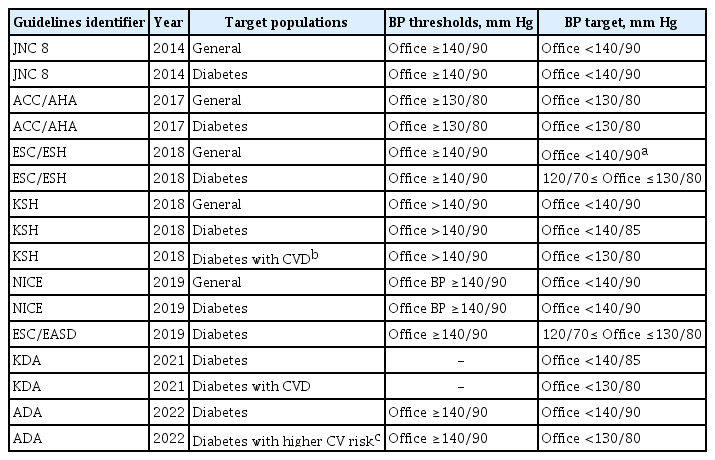
Recommended target BP in patients with diabetes mellitus according to current guidelines

Optimal target blood pressure (BP) for general and high-risk clinical features in patients with diabetes mellitus. Considering these guidelines and studies, it is important to apply individualized target BP for patients with diabetes mellitus. SBP, systolic blood pressure; DBP, diastolic blood pressure; CV, cardiovascular.
THE EVIDENCE BEHIND THE OPTIMAL BLOOD PRESSURE TARGET FROM RANDOMIZED CONTROL TRIALS
There are representative trials showing CV outcomes and clinical courses according to optimal target BP in patients with diabetes mellitus, and these trials are meaningful enough to be presented as a basis for guidelines. Table 2 summarizes representative clinical trials showing clinical CV outcomes according to the target BP in patients with diabetes mellitus.

Randomized controlled trials about blood pressure control in patients with diabetes mellitus
Prior to the ACCORD-BP trial [20], the UK Prospective Diabetes Study (UKPDS)-38 [5] and Hypertension Optimal Treatment (HOT) [24] trials in 1998 were used provide evidence on whether active BP control in patients with diabetes mellitus affects the prognosis and CV-related- and diabetes-related clinical outcomes. The target BP in the UKPDS 38 trial was <150/85 mm Hg, which is much higher than that suggested by recent guidelines; however, it has been proven to significantly reduce the risk of HF and microvascular complications. This trial provides the first evidence of the benefit of lowering BP in patients with diabetes mellitus. The HOT trial divided the target DBP into three groups in the general hypertensive population and suggested that there was no significant benefit to the CV event by controlling the DBP to ≤80, ≤85, and ≤90 mm Hg. However, a subgroup analysis of 1,501 patients with hypertension and diabetes mellitus showed that the risk of major CV events and mortality increased by two to three times when DBP was adjusted to ≤90 mm Hg compared to ≤80 mm Hg. This was the main evidence supporting the use of DBP <80 mm Hg that was recommended in most guidelines. Especially in this trial, the achieved DBPs of each group were 81.1, 83.2, and 85.2 mm Hg, suggesting that even a difference between DBP 85 and 81 mm Hg can lead to differences in clinical CV outcome in patients with diabetes mellitus.
The Action in Diabetes and Vascular Disease: preterAx and diamicroN-MR Controlled Evaluation trial (ADVANCE) [25] presented BP control goals in patients with diabetes mellitus who experience prior CVD or CV risk factors, providing evidence for setting target BP goals in high-risk patients with diabetes mellitus. This trial showed that the achieved BP was different from 136/73 and 140/73 mm Hg, and that as a result of active control, CV death, all-cause death, and major macrovascular or microvascular complications were significantly reduced. Although this was a trial emphasizing the importance of aggressively active BP control up to 130 mm Hg in patients with CVD or high CV risk, this was not direct evidence because it was a study comparing fixed perindopril-indapamide and placebo in patients with diabetes mellitus, and not comparing target BP itself.
A study reporting the clinical outcome according to the target BP in patients with diabetes mellitus who experience a high CV risk was also presented in a subgroup analysis of the International Verapamil SR-Trandolapril Study (INVEST) in 2010 [26]. The subjects were patients with diabetes mellitus and CAD, the achieved SBP of the group with SBP category of ≥140 mm Hg was 146.1 mm Hg, and the risk of adverse CV events was significantly increased compared to the group with an SBP of 131.2 mm Hg and SBP category of 130 to 140 mm Hg. However, the active control group with SBP <130 mm Hg, which achieved an SBP of 121.5 mm Hg, did not have a significant CV benefit compared to the 130 to 140 mm Hg group, but increased all-cause mortality 1.15 times in extended follow-up. This is probably because if CAD is documented, it is vulnerable to adverse effects on low BP control. Therefore, the presence of documented CAD should be considered in patients with diabetes mellitus because of its susceptibility to adverse effects on low target BP goals.
The ACCORD-BP trial [20] is a landmark trial that evaluated the benefits and risks of intensive BP control in patients with type 2 diabetes mellitus and is a pivotal study in several guidelines for BP control in patients with diabetes mellitus. This study also suggests a target BP in patients with diabetes mellitus who experience high CV risk and are aged 40 to 79 years with prior CVD or 55 to 79 years with CV risk factors; therefore, caution is needed in interpretation. In these high-risk patients with diabetes mellitus, adjusting the SBP to <120 mm Hg had no benefit in composite CV outcomes, including nonfatal MI, nonfatal stroke, and CV death, compared to controlling the SBP 130 to 140 mm Hg, whereas the risk of stroke was significantly reduced by 41%. The achieved BP was 119.3/64.4 mm Hg when the SBP target was <120 mm Hg, and it was proven that there was no benefit in DBP of <70 mm Hg. In addition, serious adverse events, including renal failure, increase when BP is controlled intensively in patients with diabetes mellitus. Therefore, this is a representative study showing that the harm is greater than the benefit of strict low-BP goals in high-risk patients with diabetes mellitus.
As mentioned above, the 2017 ACC/AHA guidelines recommend that the target BP should be <130/80 mm Hg in patients with hypertension, which also applies to patients with diabetes mellitus. This is a recommendation based on the results of the SPRINT trial [18], and this trial has a similar study design to that of the ACCORD-BP trial [20]. Although the SPRINT trial presented results excluding patients with diabetes mellitus, it is a landmark trial that presented evidence for the need of active BP control in patients with hypertension who experience high CV risk, in that it was targeted to this group of patients. In 2017, among the ACCORD-BP study population, a study presented post-hoc analysis results for patients with diabetes mellitus who experienced high CV risk and met the inclusion criteria of the SPRINT trial [23]. As a result of this analysis, controlling the SBP to <120 mm Hg significantly lowered the risk of composite of CV death, nonfatal MI, nonfatal stroke, any revascularization, and HF compared to controlling the SBP to <140 mm Hg, which provides evidence that active BP control in high-risk patients with diabetes mellitus has a benefit for CV outcome. However, there was a significantly increased risk of treatment-related adverse events. In particular, even in the group with a target SBP <120 mm Hg, the actual achieved SBP was 120.1 mm Hg, which serves as the basis for actively controlling BP in patients with diabetes mellitus but avoids lowering it below 120/70 mm Hg.
META-ANALYSES OF TRIALS
To clarify the optimal BP target for patients with diabetes mellitus, meta-analyses comparing mean baseline or achieved BP using previous randomized controlled trials (RCTs) were presented. Emdin et al. [27] presented a meta-analysis of data extraction from 45 RCTs that showed a correlation between BP-lowering treatment and clinical outcomes, including CV events, in patients with type 2 diabetes mellitus in 2015. When the baseline SBP was >140 mm Hg, BP-lowering treatment significantly reduced the risk of CHD, CVD, and mortality compared to patients with diabetes mellitus who have a baseline SBP of <140 mm Hg. In addition, when the achieved SBP was >130 mm Hg, the risk of mortality was reduced by 15% compared to achieved SBP <130 mm Hg, and the risk of CVD and CHD was significantly reduced by 26% and 30%, respectively, indicating that lowering the SBP to <130 mm Hg is not beneficial. Brunstrom and Carlberg [28] also evaluated the effect of antihypertensive treatment on CV outcomes according to baseline BP levels in patients with diabetes mellitus in 2016. A meta-analysis of 49 trials showed that BP-lowering treatment in patients with a baseline SBP of ≥140 mm Hg reduced the all-cause mortality risk by 13%, risk of MI by 16%, and risk of HF by 20%. However, when the baseline SBP was <140 mm Hg, BP-lowering treatment increased the risk of CV mortality and MI by 29% and 12%, respectively, for every 10 mm Hg decrease in SBP. Thomopoulos et al. [29] also presented the results of a meta-analysis of 41 trials consisting of BP-lowering RCTs and head-to-head drug comparison RCTs in patients with diabetes mellitus in 2017. In this study, there was no benefit in reducing the risk of CHD, HF, CV death, or all deaths when the achieved SBP was lowered to less than 130 mm Hg in patients with diabetes mellitus. Instead, when the achieved SBP was 130 to 140 mm Hg in these patients, the risks of stroke, CHD, and all deaths were significantly reduced. Moreover, when the achieved DBP was adjusted to <80 mm Hg, the risk of stroke, CHD, HF, and all-cause death significantly decreased. Taken together, these meta-analyses ultimately suggest that BP-lowering treatment has a beneficial effect on clinical outcomes, including CVD and death at baseline SBP ≥140 mm Hg in patients with diabetes mellitus, and that controlling the SBP target below 140 mm Hg is beneficial in clinical outcomes. Adjusting to a target SBP of 130 to 140 mm Hg will offer benefits for additional CV outcomes.
CONCLUSIONS
Hypertension and type 2 diabetes mellitus often coexist, and the presence of either of these risk factors increases the risk of CVD. Uncontrolled high BP is an important risk factor for CVD in patients with diabetes mellitus and leads to poor clinical outcomes. However, the optimal target BP in patients with diabetes mellitus has been debated.
Most RCTs of BP control in patients with diabetes mellitus showed that lowering SBP below 140 mm Hg was beneficial in reducing the risk of CV outcome and mortality. However, the results were less clear regarding whether a lower BP target was associated with additional benefits and the results for the DBP control were also less clear and limited. Most meta-analyses confirmed that lowering the SBP to <140 mm Hg in patients with diabetes mellitus was associated with a decrease in the risk of all CV events or mortality; in particular, they showed that adjusting to a lower target SBP of 130 to 140 mm Hg would be beneficial for additional CV outcomes. Moreover, caution is warranted for patients with diabetes mellitus and CAD because a very low BP target with a BP of <120/70 mm Hg may be susceptible to adverse events. Building on the evidence from these past studies, conflicting recommendations for optimal BP targets and thresholds for the treatment of patients with diabetes mellitus have been observed throughout the guidelines. Therefore, a general target BP of <140/90 mm Hg is recommended for patients with hypertension and diabetes mellitus, and BP should be controlled to <130/80 mm Hg in patients with diabetes mellitus who have high-risk clinical features, including CV risk factor one or more, CVD, subclinical organ damage, and stage 3, 4, or 5 chronic kidney disease.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
This study was supported by a research grant from the Korea National Institute of Health (grant number: 2021-ER0901, 2021–2023).
Acknowledgements
None