Comparison of Insulin-Treated Patients with Ambiguous Diabetes Type with Definite Type 1 and Type 2 Diabetes Mellitus Subjects: A Clinical Perspective
Article information

Abstract
In clinical practice, the distinction between type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM) can be challenging, leaving patients with “ambiguous” diabetes type. Insulin-treated patients (n=115) previously diagnosed with T2DM had to be re-classified based on clinical phenotype and laboratory results, and were operationally defined as having an ambiguous diabetes type. They were compared against patients with definite T1DM and T2DM regarding 12 clinical and laboratory features typically different between diabetes types. Characteristics of patients with ambiguous diabetes type, representing approximately 6% of all patients with T1DM or T2DM seen at our specialized clinic, fell in between those of patients with definite T1DM and T2DM, both regarding individual features and with respect to a novel classification based on multi-variable regression analysis (P<0.0001). In conclusion, a substantial proportion of diabetes patients in a tertiary care centre presented with an “ambiguous” diabetes type. Their clinical characteristics fall in between those of definite T1DM or T2DM patients.
INTRODUCTION
Type 1 diabetes mellitus (T1DM; the result of autoimmune destruction of endocrine pancreatic β-cells [1]) and type 2 diabetes mellitus (T2DM; characterized by insulin resistance, often in association with obesity, and a β-cell secretory defect [2]) are commonly viewed as completely separate entities. Typically, T1DM and T2DM differ with respect to the presence of obesity and features of the insulin resistance syndrome, the age at onset, insulin requirement shortly after diagnosis, proneness to severe hypoglycaemic and ketoacidosis episodes, family history, and laboratory indicators of the autoimmune destruction of pancreatic β-cells and a deficiency in insulin production (C-peptide). T1DM subjects may have associated autoimmune diseases. T1DM subjects typically have more fluctuations in their plasma glucose profiles from day to day, whereas the variation is less pronounced in T2DM (For more details and references, see Supplementary methods, section “discriminating features characterizing T1DM vs. T2DM”) [3,4].
In clinical practice, such exhaustive assessment for the differentiation between T1DM and T2DM is rarely performed. The criteria dominating the tentative classification are age at onset [5] and obesity [6]. By clinical experience, our team had to revise a diagnosis of T2DM towards T1DM in a substantial number of cases, while changes in the opposite direction were not observed to any noticeable degree. This indicates that two or more physicians, clinics, or hospitals had disagreed regarding the type of diabetes in a given patient. Therefore, we suggest the operational definition (used for the current analysis) of “ambiguous diabetes type” for those, in whom both diagnoses had been considered. We aimed at further characterizing this subpopulation by comparing their clinical features to insulin-treated patients with definite T1DM and T2DM.
METHODS
Study design
In the year 2013, 205 out of 1,834 inpatients with a diagnosis of diabetes mellitus (11.2%) treated at the Diabetes Centre Bad Lauterberg, had been admitted with a diagnosis of T2DM (ICD E 11.xy), but later were discharged with a diagnosis of T1DM (ICD E 10.xy). Whereas “ambiguous diabetes” was operationally defined by contradicting features which could not unequivocally be assigned to either T1DM or T2DM, such contradictory findings were not present in patients with definite T1DM or T2DM in the view of practicing physicians working in a specialized diabetes centre. All patients had given general permission to the analysis of their clinical data for scientific purposes, and the present study was performed fully complying with pertinent ethical and data protection regulations. With respect to the present study, individual written informed consent was waived due to the retrospective nature of the study (written approval by the ethics committee of the Georg-August University Göttingen, December 19, 2019, approval number 13/1/20).
Data extraction and group comparisons
Patient characteristics and treatment details (at time of discharge) and laboratory results were extracted from medical records in a pseudonymized fashion. Laboratory results potentially suitable for the distinction between T1DM and T2DM were not systematically measured, but rather as felt appropriate to support diagnostic and treatment decisions. Patients with “ambiguous diabetes type” (n=115) were compared with two patient groups with definite T1DM (n=117) and T2DM (n=120), randomly selected from the total cohorts of patients with T1DM and T2DM in the same calendar year (2013; for details on inclusion and exclusion criteria, see Supplementary methods, section “inclusion and exclusion criteria” and Supplementary Fig. 1).
Multivariate regression analysis
Parameters with clearly significant differences between patients with T1DM and T2DM were used in a multivariate regression analysis aiming at a nominal output value of 1 for patients with T1DM and 2 for patients with T2DM (Statistica version 12.0, Statsoft Europe, Hamburg, Germany), based on data from definite T1DM or T2DM patients only. Parameters that did not improve the overall prediction were removed from the model. Based on this model, it was possible to make predictions regarding diabetes type by imputing the relevant input variables (predictors) into the model. A result near 1 or 2 predicted a diagnosis of T1DM or T2DM, respectively. Based on the multiple regression model, a score was designed for easier clinical application. For details and results, see Supplementary methods, section “diabetes type score.” For sample size considerations, see Supplementary methods, section “sample size.”
Statistical analysis
Patient characteristics are reported as mean±standard deviation or counts (proportions), results are reported as mean±standard error of the mean. Results of linear regression analysis are presented as the correlation coefficient squared (r2) and the related P value. Significances of differences were tested by (repeated measures) one-way analysis of variance (RM-ANOVA) (continuous variables) or contingency table analysis (Fisher’s exact test or chi-square test for larger tables; categorical variables). Results of RM-ANOVA are reported as P values (A) by category; (B): by time and (AB): by interaction of category and time. Duncan’s post hoc test was used to identify differences between any two groups. P values <0.05 were taken to indicate significant differences.
RESULTS
Patient characteristics
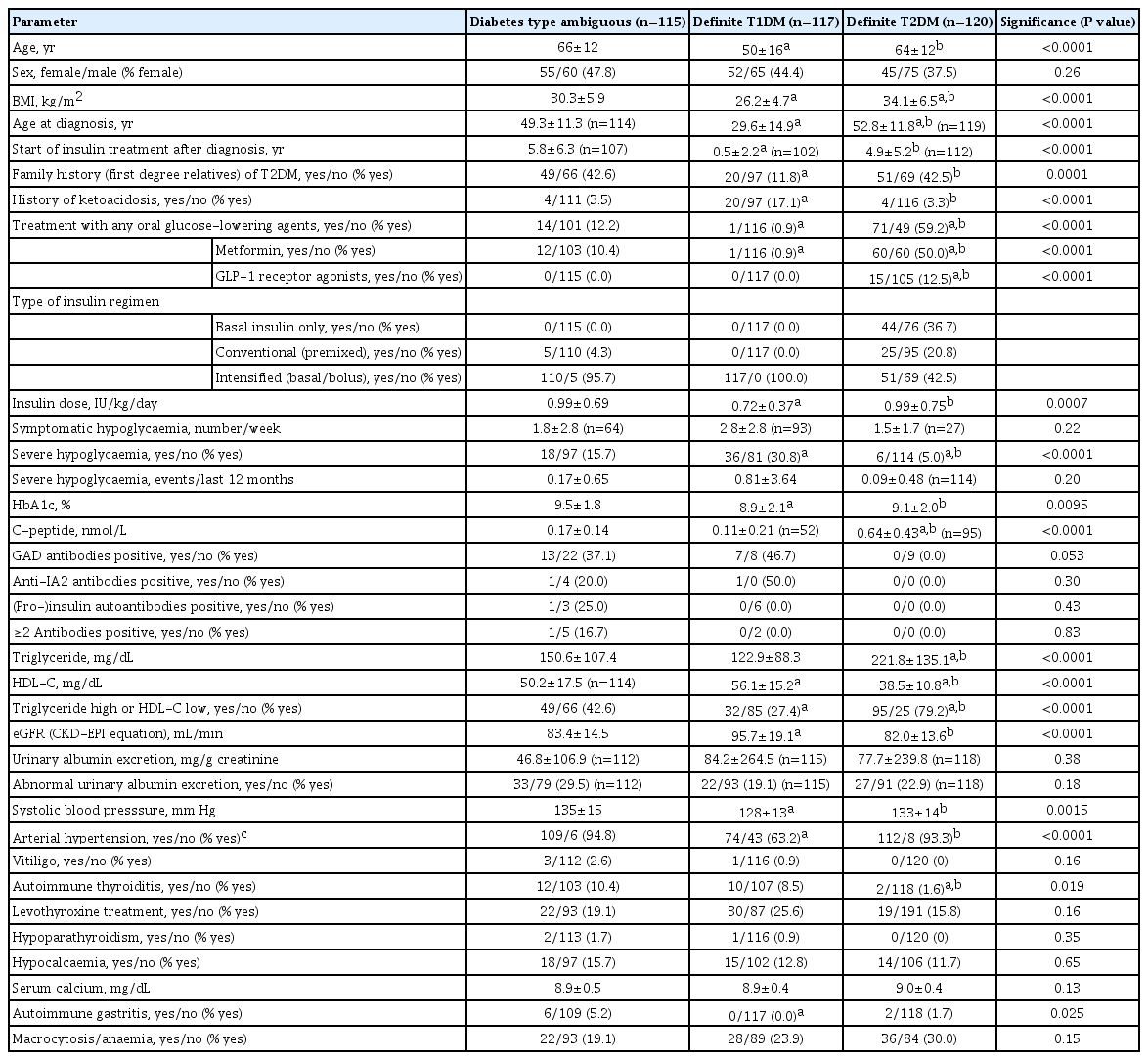
Clinical characteristics of patients with “ambiguous” diabetes type, T1DM, and T2DM are shown in Table 1, Supplementary Fig. 2. There were clear differences between subjects with definite T1DM and T2DM (P<0.05) (Table 1). Representative plasma glucose profiles taken after the optimization of glucoselowering therapy were not significantly different between patients with T1DM and T2DM (Fig. 1A), the coefficient of variation of fasting plasma glucose concentrations determined on subsequent days was significantly lower in patients with T2DM vs. the other groups (Fig. 1B). Patients in the category “ambiguous” diabetes type, as a rule, displayed intermediate results between those with definite T1DM and T2DM (Table 1, Fig. 1).
Patient characteristics of subjects with “ambiguous diabetes type”: T1DM and T2DM
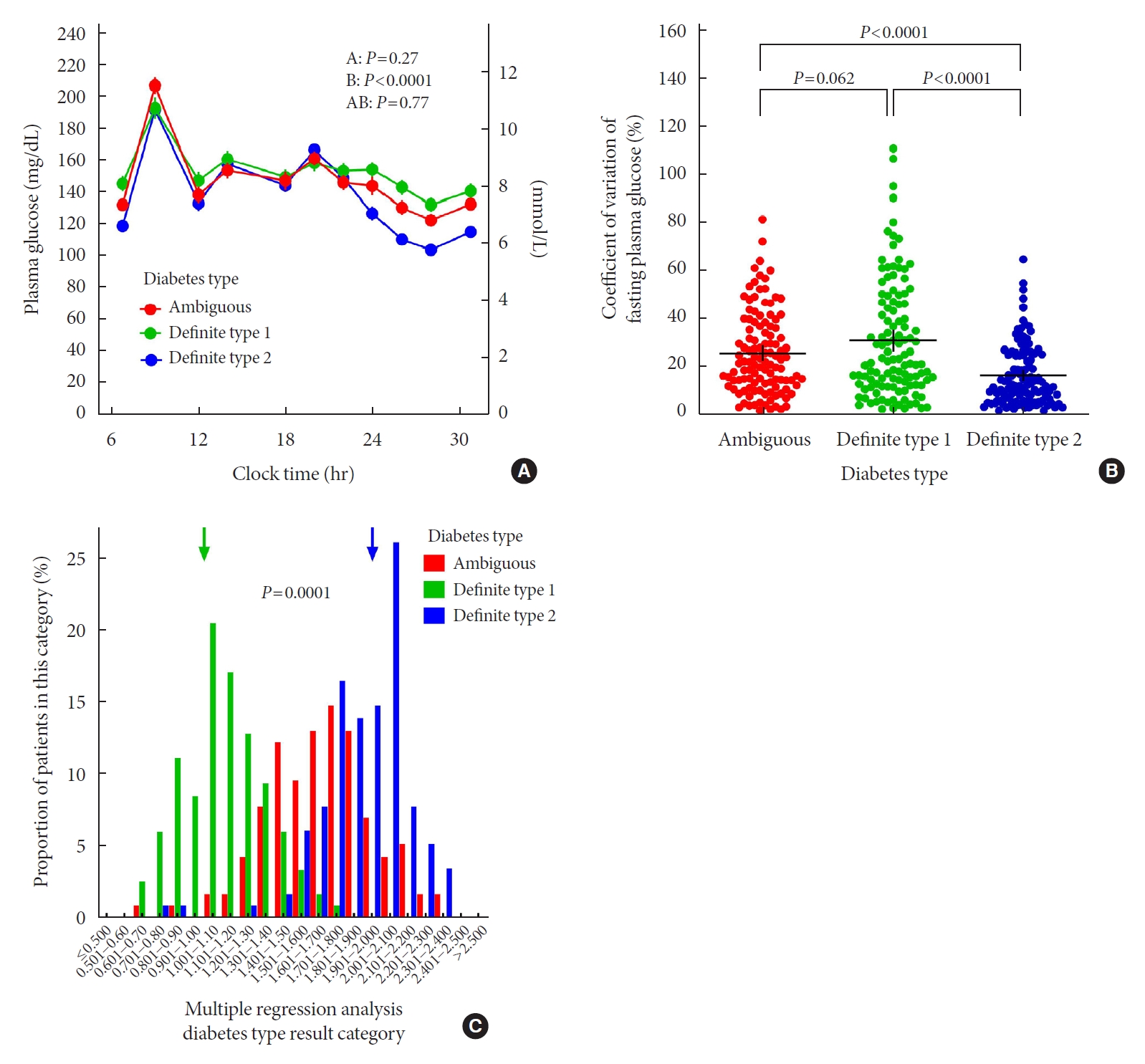
Plasma glucose concentration profiles (mean±standard error of the mean; and (A) coefficients of variation of fasting plasma glucose concentrations (bars indicate mean±95% confidence intervals; (B) determined after optimizing glucose-lowering therapy (e.g., insulin dose titration); and (C) frequency distribution of individually calculated diabetes type scores in our cohorts with unequivocal type 1 (green) and type 2 (blue) diabetes mellitus (T1DM and T2DM) and with ambiguous diabetes type (red). The scores were calculated such that, ideally, a subjects with T1DM should receive a score of 1, and subjects with T2DM should receive a score of 2. Repeated measures analysis of variance (A), analysis of variance with post hoc tests (Duncan’s test; B).
Differential diagnosis between T1DM and T2DM using multivariate regression analysis
It was possible to identify 12 input variables (body mass index [BMI, kg/m2], age at diagnosis [years], start of insulin therapy after diagnosis [years], family history of T2DM [yes/no], history of ketoacidosis [yes/no], insulin dose [IU/kg/day], severe hypoglycaemia [events/last 12 months], coefficient of variation of fasting plasma glucose [%], triglyceride high or high-density lipoprotein cholesterol low [yes/no], C-peptide [nmol/L], glutamic acid decarboxylase [GAD] antibodies positive [yes/no], and any associated autoimmune disease [yes/no]), which helped discriminating patients with T1DM (output approximately 1) and T2DM (output approximately 2) by employing multivariate regression analysis. The model summarized in Supplementary Table 1 allowed a significant (P<0.0001) prediction of the diabetes type, accounting for approximately 75% of the variance (corrected r2=0.753).
Results for patients with “ambiguous” diabetes type when applying the multivariate regression analysis
Output variables regarding patients with “ambiguous” diabetes type ranged from 0.63 to 2.36, thus encompassing the range typical for both T1DM and T2DM, with a mean of 1.67, intermediate between T1DM and T2DM patients (Fig. 1C). A score representing the weights of individual input factors as calculated by multivariate regression analysis (Supplementary Table 2) is distributed in a similar way, and correlates tightly with results from multivariate regression analysis (Supplementary Fig. 3).
DISCUSSION
Our findings indicate that there is a subgroup of insulin-treated patients, representing 6% of all diabetes patients in our German sample, who cannot easily be assigned to definite T1DM or T2DM. Their clinical characteristics fall in between those definite T1DM and T2DM (Table 1, Fig. 1C, Supplementary Figs. 2 and 3). Upon further scrutiny, the majority of patients with an ambiguous diabetes type according to our operational definition might turn out to have T1DM, but positive GAD antibodies are not specific for T1DM, and C-peptide concentrations of around 0.17 nmol/L are in the concentration range that does not allow a clear discrimination between T1DM and T2DM [7]. Along these lines, we do not believe that more extensive use of C-peptide and autoantibody measurements would have changed the results essentially, since there is a concentration range of C-peptide associated with a similar probability of T1DM and T2DM [7], and, in the case of autoantibodies, negative results may occur in a significant proportion of patients with definite T1DM [8,9].
It appears much more likely, that only a comprehensive approach based on the evaluation of multiple clinical and laboratory characteristics will optimize the differentiation between T1DM and T2DM in patients with an uncertain (“ambiguous”) diagnosis. However, obesity and insulin resistance also occur in T1DM [10,11]. Sometimes, this is referred to as “double diabetes” [12]. As reported by Park et al. [13] and Lee et al. [14], T1DM associated with features of the metabolic syndrome is quite common and rising in prevalence in Korea. Regarding the phenotypic similarity between patients with “ambiguous diabetes type” and T1DM, see Supplementary methods, section “phenotypic similarities between “ambiguous diabetes type” and T1DM. Taking a comprehensive panel of such parameters and employing multivariate regression analysis, it has been possible to reasonably discriminate between patients with T1DM and T2DM (Fig. 1C).
What then might be the correct diagnoses in patients in this “ambiguous” diabetes type category? (1) The fact that a previous (tentative) diagnosis of T2DM had been made, which later needed to be changed to T1DM, could be explained by obesity (70.4% with a BMI ≥27.0 kg/m2) and old age (55.7% above 65 years) in this group; (2) Latent autoimmune diabetes of adult onset [15] is a diagnosis that may apply to some patients in the “ambiguous” diabetes type group; (3) There may be patients who have had true T2DM, in whom later in their lives the disease process leading to autoimmune destruction of β-cells started, thereby changing the characteristics and proper classification of their diabetes [16]; (4) There may be similarities and overlaps in disease characteristics for T1DM and T2DM, e.g., islet immune cell infiltration and inflammatory cytokines contributing to β-cell destruction [17]; (5) There is increasing evidence that T2DM is heterogeneous, with some subtypes resembling T1DM [18].
The potential consequences of misclassifying T1DM could be wrong treatment approaches leading to ill glycaemic control, deferred insulin treatment or erroneous choice of simple insulin regimens, and ketoacidosis. Glycosylated hemoglobin was highest in our group of patients with “ambiguous” diabetes (Table 1), indicating a need for optimizing glucose-lowering treatment.
The present study has limitations. Owing to the retrospective study design, there are missing data, especially regarding the use of laboratory markers with the potential to differentiate between T1DM and T2DM. However, this may be typical for clinical practice. Since this is a single-centre study, the results probably cannot be generalized to other settings, e.g., other degrees of specialization and other countries.
In conclusion, the present analysis reveals a significant subgroup of patients with diabetes mellitus with an “ambiguous” phenotype falling in between characteristics of patients with definitive T1DM or T2DM. These findings highlight the clinical challenge of making the correct diagnosis [19] and recommending the most optimal treatment [20] to patients, in whom the differential diagnosis between T1DM and T2DM is not immediately obvious. As a universally accepted standard definition of “ambiguous diabetes type” is lacking, we suggest that our definition could be helpful, at least as a starting point, for additional studies addressing this diagnostic uncertainty.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2021.0322.
Multivariate regression analysis of clinical characteristics that contribute to the differential diagnosis of T1DM vs. T2DM
Calculation of a score determining diabetes type (T1DM, T2DM, or ambiguous)
Flow diagram demonstrating initial retrieval of patients according to their documented diabetes diagnosis at the time of hospital admission and before discharge, and reasons to not use data for those patients who did not fulfill the inclusion criteria or who were excluded because of the intentional reduction in patient numbers by selecting a random sample (to provide similar patient numbers in all three groups), or because an age below 18 years, missing data, or the absence of insulin therapy (in type 2 diabetes mellitus [T2DM] patients). T1DM, type 1 diabetes mellitus.
Histograms showing the frequency distribution by categories of body mass index (A), age at diagnosis (B), time of starting insulin therapy after diagnosis (C), current insulin dosage (D), coefficient of variation of fasting plasma glucose after optimizing glucose-lowering therapy (e.g., insulin dose titration) (E), fasting C-peptide (F), and number of antihypertensive medications prescribed (G) for patients with unequivocal type 1 (green) and type 2 (blue) diabetes mellitus and with ambiguous diabetes type (red). P values were calculated by chi-square test.
Histograms showing the frequency distribution by our novel diabetes type score (A) and linear regression analysis relating multiple regression analysis to diabetes scores for patients with definite type 1 (green) and type 2 (blue) diabetes mellitus and with ambiguous diabetes type (red). P values were calculated by chi-square test (A) and by linear regression analysis (B). Green and blue arrows indicate the positions of 1 and 2 (representing the ideal result for type 1 and type 2 diabetes mellitus, respectively).
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: I.L., M.A.N.
Acquisition, analysis, or interpretation of data: M.A.N.
Drafting the work or revising: I.L., M.A.N.
Final approval of the manuscript: I.L., J.J.M., M.A.N.
FUNDING
None
Acknowledgements
We thank Ms. Dipl. troph. Melanie Kahle-Stephan, Ms. Heike Schulze and Ms. Sabine Schminkel for help with retrieving documents and extracting data.