Current Advances of Artificial Pancreas Systems: A Comprehensive Review of the Clinical Evidence
Article information

Abstract
Since Banting and Best isolated insulin in the 1920s, dramatic progress has been made in the treatment of type 1 diabetes mellitus (T1DM). However, dose titration and timely injection to maintain optimal glycemic control are often challenging for T1DM patients and their families because they require frequent blood glucose checks. In recent years, technological advances in insulin pumps and continuous glucose monitoring systems have created paradigm shifts in T1DM care that are being extended to develop artificial pancreas systems (APSs). Numerous studies that demonstrate the superiority of glycemic control offered by APSs over those offered by conventional treatment are still being published, and rapid commercialization and use in actual practice have already begun. Given this rapid development, keeping up with the latest knowledge in an organized way is confusing for both patients and medical staff. Herein, we explore the history, clinical evidence, and current state of APSs, focusing on various development groups and the commercialization status. We also discuss APS development in groups outside the usual T1DM patients and the administration of adjunct agents, such as amylin analogues, in APSs.

INTRODUCTION
Type 1 diabetes mellitus (T1DM), an insulin-dependent disease, is increasing in many countries, and it is known that serious complications and disease-related mortality are higher in T1DM than in type 2 diabetes mellitus (T2DM) [1,2]. In addition, the lifelong, intensive insulin treatment needed by T1DM patients creates many physical, psychological, and economic burdens [3]. Several treatments have been tried as alternatives to insulin, but many limitations remain. Immune modulation treatments such as teplizumab are being studied, but they remain prophylactic rather than curative [4]. Pancreatic transplantation is also performed, but it is not widely practiced because of the risks inherent in using immunosuppressive drugs and surgery [5]. Drugs other than insulin currently used in T2DM are also being studied for their applicability in T1DM, but they remain adjunctive [6]. Therefore, the best treatment to date for T1DM is proper blood glucose monitoring and appropriate insulin administration.
According to the results of one study, only 17% of children and 21% of adults with T1DM achieve their target glycemic levels, which is quite poor [7]. Moreover, severe hypoglycemia occurs frequently, with an annual incidence of 4.0% to 8.3%, depending on the degree of glycemic control [8]. Due to the complexity and difficulty of management, it is well-established that structured insulin dosing training is important for maintaining glycemic control and quality of life. However, the reality is that the process is neither easy nor comfortable [9].
When insulin pumps and continuous subcutaneous insulin infusion (CSII) were introduced in the 1970s, it became possible to reduce the number of injections to one every 3 or 4 days, replacing the need for manual multiple daily insulin injections (MDI) [10]. In a large retrospective study, CSII was reported to be more effective for glycemic control and hypoglycemia than MDI, but many randomized controlled trials (RCTs) did not show improvement [11-13]. Because CSII still requires manual insulin dose determination, difficulties for patients are inevitable. Therefore, an artificial pancreas system (APS), a closed-loop system that automatically administers an appropriate insulin dose according to the blood glucose level as mediated by the natural healthy pancreas, has been the goal for T1DM patients for many years. Recently, several APSs have been developed and validated very rapidly by various groups, and they are already being used in actual clinical practice. This review will focus on the clinical evidence for APSs and their application from various development groups in actual practice.
BASIC CONCEPT AND HISTORY OF THE ARTIFICIAL PANCREAS SYSTEMS
A workable closed-loop system must contain a real-time blood glucose monitor, a device for injecting insulin, and an algorithm to link them. In other words, it requires a continuous glucose monitoring system (CGM), a CSII or insulin pump, and autonomous control algorithms. The concept of an APS has been around for a long time; however, the opportunity for substantial development requires advances in CGMs [14]. Although many non-invasive blood glucose monitoring devices have been developed, the CGM currently used is operated by attaching a sensor to the subcutaneous tissue and detecting glucose in the interstitial fluid at 1- to 5-minute interval. Before mobile devices such as smartphones were developed, the CGM was linked to an insulin pump. Sensor augmented pumps (SAPs), which link an insulin pump to a CGM and display glucose data, were developed in the late 2000s and produced a marked improvement in glycemic control compared with MDI or an insulin pump alone (Figs. 1 and 2) [15]. Later, an SAP with a low glucose suspension (LGS) function (LGS SAP), which stops insulin infusion in cases of hypoglycemia, and an SAP with a predictive low glucose suspension (PLGS) function (PLGS SAP), which stops infusions before hypoglycemia occurs by predicting it, was sequentially developed and verified clinically (Figs. 2 and 3) [16-18]. Up to that point, the insulin dose still had to be manually determined and as such, these were not closed-loop systems.
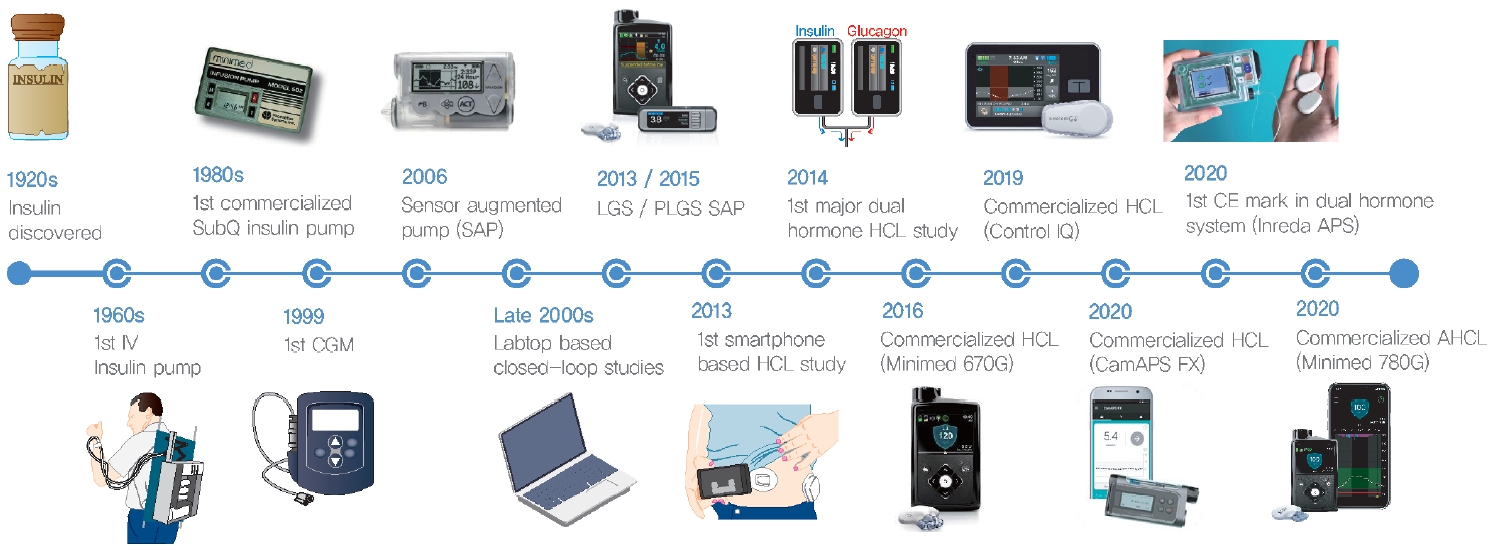
Timeline of development of the artificial pancreas system. IV, intravenous; SubQ, subcutaneous; CGM, continuous glucose monitoring system; SAP, sensor augmented pump; LGS, low glucose suspension; PLGS, predictive low glucose suspension; HCL, hybrid closed-loop; CE, Conformité Européenne; APS, artificial pancreas system; AHCL, advanced hybrid closed-loop.

Timeline of landmark studies of the artificial pancreas system. NEJM, New England Journal of Medicine; RCT, randomized control trial; SAP, sensor augmented pump; D Care, Diabetes Care; PLGS, predictive low glucose suspension; BMJ, British Medical Journal; PGCS, portable glucose control system; OCL, overnight closed-loop; T1DM, type 1 diabetes mellitus; HCL, hybrid closed-loop; T2DM, type 2 diabetes mellitus; JAMA, Journal of American Medical Association; Lancet D&E, Lancet Diabetes Endocrinol; Lancet Digit H, Lancet Digital Health; DBLG1, Diabeloop Generation 1; D Technol, Diabetes Technology & Therapeutics; IRCM, Institut de Recherches Cliniques de Montreal; DOM, Diabetes Obesity and Metabolism; AP, artificial pancreas. aSubgroups of the same study.

Key features of sensor augmented pump and artificial pancreas systems. CGM, continuous glucose monitoring system; LGS, low glucose suspension; PLGS, predictive low glucose suspension; TIR, time in range; TBR, time below range.
The first closed-loop system was developed quite early in the 2000s and operated using a personal computer (PC)-based control algorithm (Fig. 1) [19-22]. From the early to the mid2010s, it was developed into a portable form using a control algorithm installed on a smartphone or the pump itself [23,24]. The closed-loop system for insulin began as an overnight closed-loop (OCL) system for use during the fasting period at night, when the control algorithm application was relatively simple [21,25-27]. Subsequently, it was developed for use both in the day and at night, but the automatic control worked only for the basal rate, not for meal bolus insulin, which is complex to calculate; this was called a hybrid closed-loop system (HCL) (Figs. 2 and 3) [28-30]. The HCL has been commercialized and used in practice since the late 2010s (Fig. 1). Concurrently, a dual-hormone closed-loop system, dispensing glucagon as well as insulin, was developed in the late 2000s [31-33]. Although several short-term studies have revealed the superiority of the dual-hormone closed-loop system over the single-hormone closed-loop system in terms of hypoglycemia, it has not yet been used in practice [34-36]. Most recently, advanced HCL (single-hormone) was developed and commercialized with an additional auto-correction bolus feature, which frequently corrects blood glucose levels exceeding the target, and showed superior glycemic control compared to the previous HCL (Figs. 1-3) [37,38]. However, advanced HCL is still not a full closed-loop system (FCL) because a meal announcement is required.
Since 2013, patients and caregivers who are unsatisfied with the development rate of commercial APSs have developed do-it-yourself (DIY) APSs using open source platforms [39]. Furthermore, to overcome the limitations of insulin-based APSs, other peptide hormones such as amylin analogues and glucagon-like peptide 1 (GLP-1) receptor (GLP-1R) agonists have been investigated, and intraperitoneal (IP) insulin delivery systems have been in development [40-42]. Furthermore, several APS studies have been conducted in patients with T2DM and pregnant T1DM (Fig. 2) [43,44].
MAJOR GROUPS
A number of APSs have been developed and clinically validated; however, most of them were performed by only a few large groups (Fig. 4). Since various people and institutions were involved in the development and verification of APS, it is difficult to fully attribute the development groups. Therefore, in this article, we used the company names of APSs only if they were commercialized. Otherwise, we utilized the main institution name. For the insulin-only closed-loop system, the main groups comprise the companies CamDiab (Cambridge, UK), DreaMed (Petah Tikva, Israel), Medtronic (Minneapolis, MN, USA), and TypeZero Technology (Charlottesville, VA, USA) [24,25,28,45]. For convenience, we will call them the CamDiab, DreaMed, Medtronic, and TypeZero groups, respectively, in this article. CamDiab is an APS company that was mainly developed by colleagues at Cambridge University. CamDiab group developed a control algorithm, which was commercialized in 2020 as CamAPS FX, which runs as a mobile application. Colleagues at Jesse Z and Sara Lea Shafer Institute for Endocrinology and Diabetes (Israel) mainly conducted clinical trials and founded the DreaMed company. The DreaMed group developed the MD-Logic APS algorithm, which was commercialized in 2015 as GlucoSitter, and it developed a decision support software called Advisor Pro for insulin dosing in 2018. The Medtronic group developed its own HCL control algorithm, which became the Minimed 670G system, in 2016, and additionally adopted several algorithmic features of the MD-Logic algorithm from the DreaMed group for an advanced HCL that became Minimed 780G in 2020 [24,38]. TypeZero Technologies was founded by colleagues at Virginia University. The TypeZero group first developed the DiAs closed-loop platform, and developed it into the inControl algorithm that has since been used in the Tandem Control-IQ system [46]. Some other groups have entered this arena since the late 2010s. The Diabeloop group of France developed the Diabeloop Generation 1 (DBLG1) system, which was smartphone-based and received the Conformité Européenne (CE) mark in 2018, and subsequently made Diabeloop for highly unstable diabetes (DBLHU system) to treat brittle diabetes [47,48]. The Insulet group (United States) developed an HCL control algorithm called Omnipod 5, a later version of the Horizon system that worked with the Omnipod patch insulin pump and has not yet been commercialized [49].
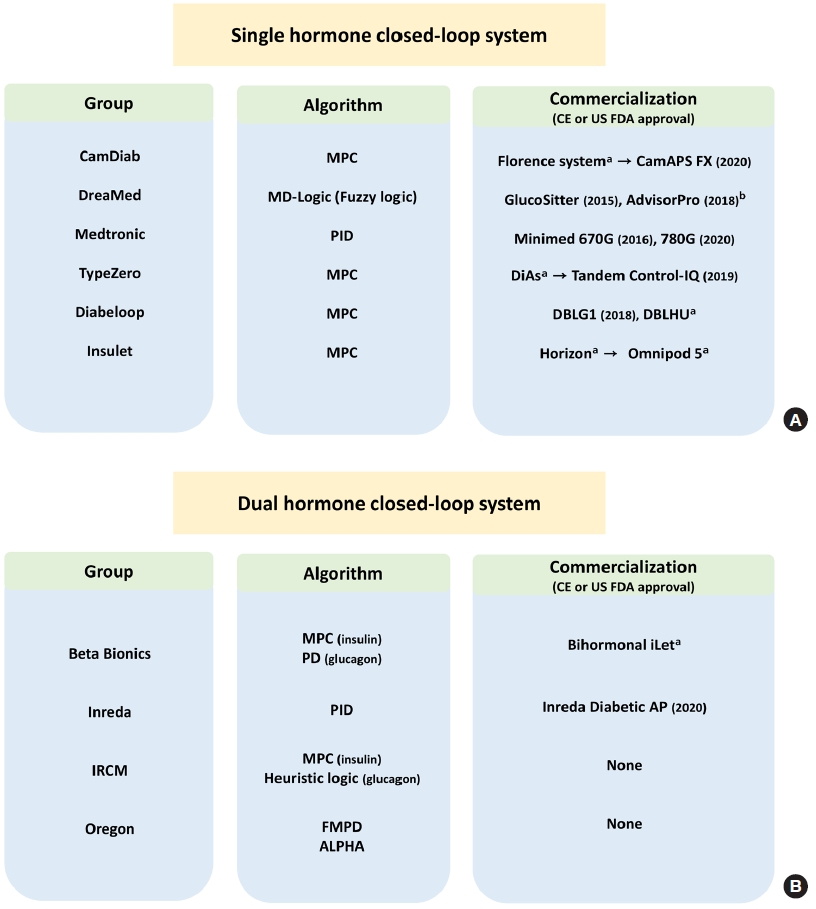
Schematic diagram of major research groups working on artificial pancreas system. (A) Single-hormone closed-loop system research groups, (B) dual-hormone closed-loop system research groups. MPC, model predictive control; PID, proportional integral derivative control; CE, Conformité Européenne; US FDA, U.S. Food and Drug Administration; DBLG1, Diabeloop Generation 1; DBLHU, Diabeloop for highly unstable diabetes; IRCM, Institut de Recherches Cliniques de Montreal; PD, proportional derivative control; IRCM, Institut de Recherches Cliniques de Montreal; ALPHA, adaptive learning postprandial hypoglycemia prevention algorithm; AP, artificial pancreas. aNot approved yet, bInsulin dosing support system (not closed loop system).
Regarding the dual-hormone closed-loop systems, Beta Bionics company (Irvine, CA, USA), Inreda Diabetic company (Goor, the Netherland), Institut de Recherches Cliniques de Montreal (IRCM, Montreal, QC, Canada), and Oregon Health and Science University (Portland, OR, USA) are the major groups [50-53]. We will refer to them as the Beta Bionics, Inreda, IRCM, and Oregon groups, respectively. The development and validation of APS from the Beta Bionics group were mainly conducted by Boston University and Harvard Medical School. They initially used two separate pumps for insulin and glucagon and then developed a dual-chamber pump called Bihormonal iLet, which they are preparing for commercialization [51,54]. The Inreda group, primarily led by Amsterdam University, also initially used two pumps from other companies for insulin and glucagon, respectively, but it has since developed and is using its own algorithm-embedded dual-chamber pump called the Inreda Artificial Pancreas [50,55]. It received the CE mark in 2020 and is preparing for commercialization. The IRCM and Oregon groups also independently developed their own control algorithms with two separate pump systems, but they have not yet commercialized them.
CONTROL ALGORITHMS
Currently, the main control algorithms used for closed loops are proportional, integral, and derivative control (PID) algorithms, model predictive control (MPC) algorithms, and fuzzy logic algorithms [56], all of which are widely used in other control applications, such as autonomous vehicles (Fig. 5). As a simple explanation of the PID concept, “proportional” can be understood to correspond to the present because it detects how far away the glucose level is from the target right now; “integral” corresponds to the past to see the area deviating from the target in the previous trajectory, and “derivative” corresponds to the future, predicting the future direction of changes in the glucose level [57]. It requires only a sensor glucose variable to operate, which makes it simple and easy to implement. MPC algorithms predict changes in the dependent variable after a specific time by adjusting the independent variables. In an APS, an MPC models the glucose level as the dependent variable and adjusts independent variables such as body mass index, carbohydrate intake, and insulin-on-board. This modeling is performed with updated information every few minutes. Generally, MPC shows better performance than PID, but it is more complex and challenging to operate [56]. Fuzzy logic algorithms produce correctness as a matter of degree instead of as a yes or no result [20]. In an APS, fuzzy logic operates through supervised learning based on expert opinions to establish a specific decision. In addition to these options, several modified algorithms have also been used. For example, the proportional and derivative (PD) algorithm is a PID algorithm without the integral feature, and the fading memory PD algorithm uses weighting to privilege more current data [33].

Schematic diagram of major control algorithms of artificial pancreas system. (A) Proportional integral derivative control (PID) algorithm, (B) model predictive control (MPC) algorithm, (C) fuzzy logic algorithm. CGM, continuous glucose monitor.
For their insulin-only closed-loop systems, the Medtronic group used a PID algorithm, the CamDiab, Diabeloop, Insulet, and TypeZero groups used MPC algorithms, and the DreaMed group adopted a fuzzy logic algorithm. Most DIY APSs are based on MPC algorithms. For their dual-hormone closedloop systems, the Inreda group used a PID algorithm for both insulin and glucagon, and the Oregon group used a fading memory PD algorithm. Both the Beta Bionics and IRCM groups adopted an MPC algorithm for insulin, but for glucagon, the Beta Bionics group used a PD algorithm, and the IRCM group used heuristic logical rules (Fig. 4).
CLINICAL EVIDENCE FOR PRE-STAGE ARTIFICIAL PANCREAS SYSTEMS
As a pre-stage for APSs, the first SAP that linked a CGM and an insulin pump was developed by the Medtronic group in 2006 (Table 1). Although it had no control algorithm, it still represented a big technological advance as it could control the glucose level while monitoring it in real-time. In 2010, during a study of 485 T1DM patients, the SAP decreased glycosylated hemoglobin (HbA1c) by 0.6% more than MDI for 1 year [15]. However, SAP still could not improve severe hypoglycemia [15,58] and so the group developed an SAP with an LGS function that automatically stops insulin infusion in the event of hypoglycemia and commercialized it as the Minimed 530G and later 630G (Medtronic). In 2013, the Medtronic group performed a study of 95 patients with hypoglycemia unawareness and found that hypoglycemic events were 3.6-fold fewer with LGS SAP than with CSII [59]. Another study in the same year compared the LGS SAP with the SAP alone in 247 patients and found that nocturnal hypoglycemic events were reduced by 31.8% with LGS SAP [16]. Next, instead of stopping the infusion upon hypoglycemia, the Medtronic group developed the PLGS SAP, commercialized as the Minimed 640G, to stop the infusion rate by predicting hypoglycemia 30 min in advance. After demonstrating superiority in preventing nocturnal hypoglycemia [17,18], the PLGS SAP was shown to decrease hypoglycemia, compared with the performance of SAP and CSII, in all-day and long-term studies in 2017 to 2019 [60-62]. In 2018, another PLGS SAP made by Tandem and named the Basal IQ algorithm was introduced, which showed a significant reduction in time below range (TBR) <70 mg/dL compared with that of SAP [63].
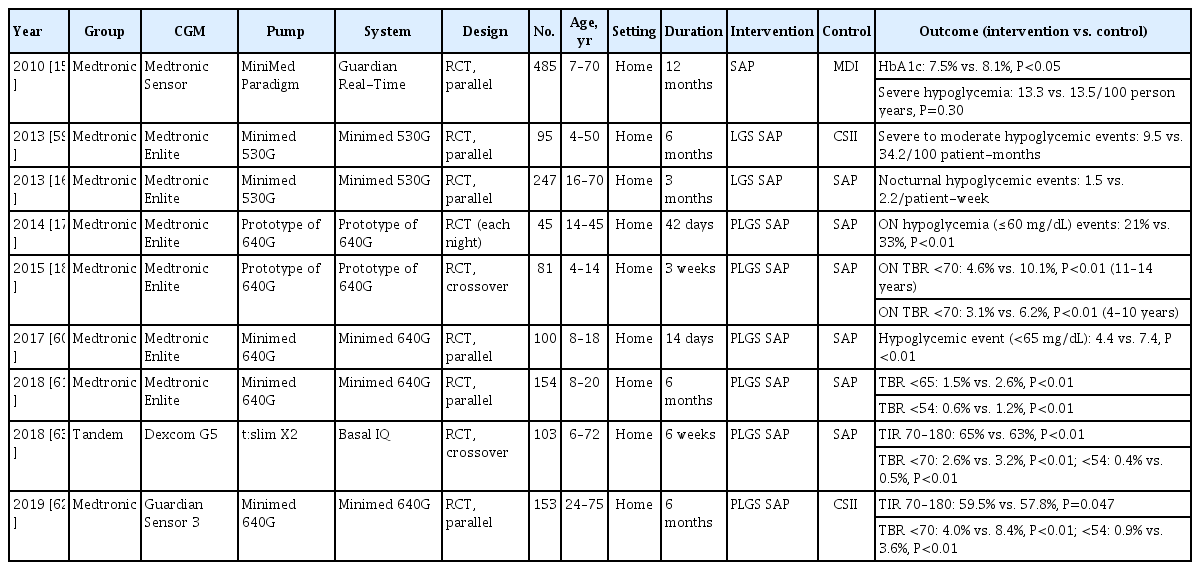
Clinical evidence of sensor augmented pumps in type 1 diabetes mellitus
CLINICAL EVIDENCE FOR SINGLE-HORMONE CLOSED-LOOP SYSTEMS
For the devices mentioned above, the insulin dose had to be set by the user. Therefore, the next step was a closed-loop system that automatically determined the insulin dose using a control algorithm. Research has been in progress for a long time, but its use in actual practice has been slowed by safety issues. First, an OCL was developed to automatically determine the infusion rate during the night, which is much simpler to calculate than the dynamic requirements of postprandial blood glucose control (Supplementary Table 1). In 2010 to 2011, the CamDiab group published small clinical studies of its OCL in hospitalized children and adults with T1DM and reported improvements in overnight time in range (TIR) 70 to 144 mg/dL and TBR <70 mg/dL compared with CSII [21,22]. In 2012, the Medtronic and DreaMed groups also showed improvements in overnight TIRs compared with those of the CSII and SAP, respectively, in small studies of inpatients though both studies had single arm designs [64,65]. Subsequently, the research expanded to non-hospital environments. In 2013, the DreaMed group compared OCL and SAP for 1 day in a diabetes camp for 56 adolescents with T1DM, the largest number at that time. During the night, hypoglycemic events of <63 mg/dL decreased (7 vs. 22, P=0.003), and mean overnight glucose levels were also kept lower (126.4 mg/dL vs. 140.4 mg/dL) [15]. Subsequently, the TypeZero group showed an improvement in the overnight TIR with OCL compared with SAP in a diabetes camp for 20 adolescents in a per-protocol study [66].
Since 2014, home-based OCL studies have been conducted in earnest, with the DreaMed group showing improvements over SAP in overnight TIR and TBR in a 6-week study of 24 adolescents and adults [67]. In the same year, the CamDiab group conducted home-based OCL studies for adolescents and adults for 3 and 4 weeks, respectively, and showed overnight TIR improvements compared with SAP [26,68]. In the following year, a 12-week home-based study, the longest study at that time, was conducted by the same group and showed improvements in overnight TIR compared with SAP in 25 children and adolescents (59.7% vs. 34.4%, P<0.001) [28]. In the same year, the TypeZero group also showed TIR improvements by using a control algorithm that covered dinner time in addition to overnight, in a 2-month home-based study of 32 adults (8:00 PM–8:00 AM TIR 70 to 180 mg/dL; 66.7% vs. 58.1%, P<0.001) [27]. In 2017, the DreaMed group performed an OCL study on 75 T1DM patients [69].
Next, OCL developed into HCL, which controls the basal rate both overnight and during the day (Table 2). First, the TypeZero and CamDiab groups conducted separate HCL studies in inpatient settings in 2013 [23,29] and short-term supervised outpatient settings in 2014, and reported heterogeneous TIR and TBR results [70,71]. In 2015, the Medtronic group conducted an HCL study and compared it with LGS SAP for 6 days at a diabetes camp. Although they failed to show a difference in TIR, it was the first clinical use of an algorithm-integrated pump [30]. In the same year, the CamDiab group demonstrated a TIR improvement for HCL over SAP in a home-based study of 33 adults for 12 weeks (67.7% vs. 56.8%, P<0.001) [28]. In 2016, HCL studies were expanded to younger ages, with the CamDiab and TypeZero groups demonstrating TIR or TBR improvement in children and adolescents in home-based and diabetes camp settings, respectively [72-74].

Clinical evidence of hybrid closed-loop system (single-hormone) in type 1 diabetes mellitus patients
At that point, HCLs began to be commercialized. In 2016, the Medtronic group conducted a pivotal single arm trial for 3 months with 124 adult and adolescent patients and showed improvement in HbA1c and TIR compared with CSII (HbA1c, 7.4% to 6.9%; TIR, 66.7% to 72.5%) [24]. Based on that study, the Minimed 670G (Medtronic) was approved by the U.S. Food and Drug Administration (FDA) as the first commercialized HCL in the world. After that, a single arm study of the Minimed 670G was conducted in 7 to 13-year-old children for 3 months. It showed an improvement over SAP in TIR and TBR, and its indication was expanded to children aged 7 years and older [75]. In 2020, because the previous Minimed 670G studies were single arm, a 6-month RCT was conducted among 120 adult T1DM patients, and it reported improvements in TIR and TBR compared with MDI and CSII [76].
In 2017, the CamDiab group demonstrated TIR improvements with HCL over SAP, even among well-controlled T1DM patients in the home setting [77]. In the following year, it performed the then-largest RCT of HCL (86 patients for 12 weeks) among adults and children older than 6 years, reporting improvements in TIR (65% vs. 54%, P<0.001) [78], after which the group further verified HCL safety in children aged 1 to 6 years [79]. Resultantly, CamAPS FX, a mobile APS application from the CamDiab group, received the CE mark and was commercialized in 2020 for T1DM patients 1-year-old or older.
After performing mid- to long-term single arm studies in 2016 to 2017 [80,81], the TypeZero group conducted the largest HCL study to date in 2019 of 168 adolescents and adults for 6 months using a Tandem pump called t:slim X2, and the results showed TIR (71% vs. 59%, P<0.001) and TBR (1.58% vs. 2.25%, P<0.001) improvements compared with SAP [45], and subsequently, the Tandem Control-IQ system received FDA approval. In an extension study, the HCL group was again divided into the HCL and PLGS SAP groups, and the HCL group still showed superior TIR (67.6% vs. 60.4%, P<0.001) [82]. In 2020, the study was expanded to 101 children aged 6 to 13 years, and their TIR improved compared with the SAP group for 16 weeks (67% vs. 55%, P<0.001) [83], which allowed the Tandem Control-IQ to gain approval for use in children aged 6 years and older. Control-IQ is also called advanced HCL because it has the feature of an automatic correction bolus, which automatically delivers 60% of the calculated correction factor up to once an hour when the predicted glucose value in 30 minutes is above 180 mg/dL.
In 2019 the DreaMed group, which had been quiet after the OCL era, conducted a short-term clinical study of an all-day HCL and added an automated bolus correction function using the MD-Logic algorithm [84]. Subsequently, the Medtronic group developed an advanced HCL using its own PID algorithm and some of the features of the DreaMed group [38]. With the combined control algorithms, if the sensor glucose rises, the automated correction function operates up to every 5 minutes to reach the target (100 to 120 mg/dL). Most recently, in 2021, the advanced HCL of the Medtronic group was compared with the PLGS SAP in 60 adults and children aged 6 years and older for 4 weeks, resulting in improved TIR and TBR (TIR, 70.4% vs.57.9%, P<0.001; TBR, 2.1% vs. 2.5%, P<0.032) [37]. In addition, Medtronic’s advanced HCL was compared with HCL (Minimed 670G) in 113 adolescents and adults for 3 months and showed superiority in daytime (6:00 AM to midnight) time above range >180 mg/dL (34% vs. 37%, P<0.0001) and all-day TIR (67% vs. 63%, P<0.0001) and non-inferiority in all-day TBR <54 mg/dL [38]. However, in contrast to expectations, greater effects were seen from 5:00 AM to 10:00 AM than in the rest of the time, which implies that the glycemic improvements shown in this study were not mainly due to postprandial glucose control. Although this feature might correct the postprandial glucose not controlled by the usual bolus infusion to some extent, it is still insufficient, and an advanced HCL requires carbohydrate counting. In 2020, it was commercialized as Minimed 780G (Medtronic), received CE mark approval and at the time of writing, is awaiting FDA approval.
Other groups have conducted HCL studies. After performing several non-RCT pilot studies [85,86], the Diabeloop group of France conducted a home-based 12-week RCT of its own HCL algorithm, called DBLG1, in 2019 among 63 adult T1DM patients, showing TIR improvement compared with SAP (68.5% vs. 59.4%, P<0.001) [47]. The following year, it conducted a short-term study of inpatient adult T1DM patients during meals and exercise environments and demonstrated TIR improvement compared with SAP [87]. The group performed another study in 2021 targeting brittle diabetes using the DBLHU algorithm; five highly unstable adult T1DM patients were studied for 8 weeks in two 4-week crossover studies [48]. Although the control group showed a poor TIR of 43.5%, even when using the PLGS SAP, this HCL improved the TIR to as much as 73.3%. This group also published a real-world single arm study of a pre-launch commercialized DBLG1 system in 2021 [88]. After receiving the CE mark in 2018, the group is currently preparing to launch a commercial HCL product that will work with various insulin pumps.
Separately, the Insulet group conducted APS studies using an Omnipod tubeless patch pump. Previously, HCL studies from another group had used the Omnipod pump (Insulet) [23,89], but the Insulet group began research using its own control algorithm in the late 2010s. After completing small safety and feasibility studies in 2018 to 2019 [90,91], the group performed several single arm studies of pump-embedded control algorithms called Horizon and Omnipod 5 and compared them with standard treatment using SAP, CSII, or MDI. Following a hotel and rental home-based study in 2020 [92], the group conducted home-based research for 2 weeks in 2021 among 36 child and adult T1DM patients and reported TIR improvements (75.1% vs. 65.6%, P<0.05 in the adult group) [49].
As explained above, single-hormone APS developed from OCL systems to day-and-night HCL systems, and testing has proceeded from small short-term hospital-based studies to large long-term home-based studies. At the same time, the control groups evolved from CSII to SAP, PLGS, and even older HCL systems. In recent years, studies conducted for 3 to 6 months with more than 100 patients have been published, changing the standard of APS research. Furthermore, commercialized APSs are now used in actual practice, quickly following the announcement of clinical studies.
REAL-WORLD EXPERIENCE AND USABILITY OF COMMERCIALIZED SINGLE-HORMONE CLOSED-LOOP SYSTEMS
In the present day, since several HCLs have been commercialized, there have been studies based in real-world experience. First, for Minimed 670G, a 3-month retrospective study of 3,141 children and adults revealed improvements in TIR of 7.3% (66.0% to 73.3%, P<0.001) and TBR of 0.6% (2.1 to 2.7%, P<0.001) [93]. Another retrospective study of 127 adults showed improvements in TIR of 11% (59.5% to 70.1%, P<0.001) and TBR of 1% (3.2% to 2.2%, P<0.05) after 6 months of follow-up [94]. Another study conducted in 92 children for 6 months revealed a 6% TIR reduction (50.7% to 56.9%, P=0.007) with no change in TBR [95]. Over all, the above real-world studies showed similar glycemic improvements to those which were observed in previous controlled trials.
However, auto-mode usage was as low as 51.2% to 80.8% in the above real-world studies compared to 87.2% in the previous pivotal trial, with an especially low rate in the study of children (51.2%) [24,93-95]. Moreover, a 1-year prospective study of 84 children and adults revealed that the number of participants who stopped using auto-mode was 33% (46%, if analyzed with those who provided data), and patients who used auto-mode more than 70% were only 32% [96]. The main reasons for this were frequent alarm and sensor calibration issues.
On the other hand, in another 1-year prospective cohort study of 30 children, the auto-mode was used in 85.6% of cases, and TIR was improved by as much as 26.5% (46.9% to 73.4%, P=0.01), far better than previous observational studies [97]. The difference between this and other studies was that the specific selection and initiation protocols were used, and structured education was provided with follow-up. Therefore, to successfully use this HCL in real-world practice, it seems that the user’s motivation and intensive education are crucial.
In addition, although there has been no real-world study of the Minimed 780G to date, auto-mode usage was 14% higher than 670G in the landmark RCT (83% vs. 69%, P<0.0001) [38]. This is thought to be due to the kick-out process in Minimed 670G, which stopped the auto-mode when sensor glucose levels were higher than the target for a certain time (>300 mg/dL for 1 hour or >250 mg/dL for 3 hours), and the auto-bolus correction of the Minimed 780G can encourage the patient to stay longer in auto-mode. Therefore, it is expected that auto-mode usage can be improved in real-world practice when using the Minimed 780G.
In the case of Control-IQ, there was a 1-year retrospective study of 9,451 child and adult patients who mostly used Basal IQ (PLGS SAP) in the past and changed to use Control-IQ (HCL) [98]. In this study, TIR was improved by 10% (63.6% to 73.6%, P<0.001), and TBR was kept as low as around 1%, so glycemic improvements seen in the RCTs were substantiated in the real-world study. In addition, the time spent in auto-mode was 95%, which is much higher than that in the Minimed 670G studies. Similarly, in a prospective cohort of 191 child patients, TIR was improved by 9% (57% to 66%, P<0.001) and TBR was reduced by 0.4% (2.2% to 1.8%, P=0.01) at 6-month follow-up [99]. Auto-mode usage was as high as 86.4%, and the number of patients who stopped using the device was only 3.5%, showing good usability even for children. This might be due to the feature of Control-IQ, which has no kick-out process for hyperglycemia, does not require calibration, and to some extent, has auto-correction bolus function. In addition, since most participants in those studies previously used Tandem insulin pumps, it seems that familiarity with the devices might have contributed to the results.
For CamAPS FX, because it was recently approved by CE, there have been few published real-world studies, despite many ongoing cohort studies. Auto-mode usage was as high as 95% in an RCT that used commercialized CamAPS FX [100]. This can be partly attributed to the features of CamAPS FX, which uses Dexcom G6, a factory-calibrated CGM.
CLINICAL EVIDENCE FOR DUAL-HORMONE CLOSED-LOOP SYSTEMS
Patients with T1DM often have impairments in counter-regulatory response to hypoglycemia as well as insulin secretion [101]. Single-hormone closed-loop systems can reduce hypoglycemia by suspending insulin administration or by decreasing the basal insulin rate. However, because of the time gap between the onset of insulin action and the rise in blood glucose, single-hormone APS users remain at high risk of developing hypoglycemia after meals, especially if they exercise [102]. Therefore, dual-hormone APSs have been designed to deliver small boluses of glucagon when hypoglycemia is predicted, in addition to suspending insulin delivery.
The first dual-hormone system began to develop early (Table 3). Since 2010, the Beta Bionics, Inreda, IRCM, and Oregon groups have conducted short-term (up to 28 hours) studies comparing CSII or single HCL in 10 to 15 hospitalized adult T1DM patients [32,33,55,103,104]. Some of these studies showed improvements in TIR and TBR, but others did not. In 2014, the Beta Bionics group conducted a study in hotel (adult) and diabetes camp (youth) environments for 5 days among 52 (20 adults, 32 adolescents) T1DM patients, the largest number of subjects to date in a dual-hormone study [51]. Unlike previous studies, the control algorithm in the Beta Bionics study was run on a smartphone rather than a PC. Compared with CSII, TIR 70 to 180 mg/dL was improved by approximately 30% in adults, reaching 79.5% (adult) with the dual-hormone HCL, which was remarkable compared with the TIR 70 to 180 mg/dL of about 70% reported in insulin-only HCL studies during the same period. However, that study compared a dual-hormone HCL with CSII and still did not significantly reduce hypoglycemia in children or adolescents. In 2015, the IRCM group published two 3-arm studies that compared dual-hormone HCL with both CSII and insulin-only HCL [34,52]. One was a short-term study of 24 hours in 30 inpatient adolescents and adults and showed an improving but statistically insignificant trend in TIR and TBR compared with single-hormone HCL [52]. On the other hand, the study of 33 children and adolescents conducted during 3 nights at a diabetes camp showed that with the dual-hormone HCL, TBR improved compared with a single-hormone HCL (0% vs. 3.1%) [34]. Therefore, it was suggested that dual-hormone HCL would be helpful in groups particularly vulnerable to hypoglycemia, such as children, but not in all groups. In 2016, the Beta Bionics group performed an additional 5-day pediatric study (ages 6 to 11) at a diabetes camp, and both TIR and TBR were improved compared with CSII [105]. In the same year, the Oregon and IRCM groups showed better hypoglycemia control with dual-hormone HCL than with SAP and single-hormone HCL, respectively, in short-term studies of exercising patients [106,107].

Clinical evidence of dual-hormone closed-loop system in type 1 diabetes mellitus
Up to that point, studies have been conducted in hospitals, hotels, and camps, with participants in so-called outpatient studies spending their nights at a hotel [51]. In 2016, the Inreda group performed the first truly home-based dual-hormone study for a short period and reported significantly improved TIR compared with CSII [108]. Notably, unlike the previous studies by other groups that used two pumps for insulin and glucagon, the Inreda group used one dual-chamber pump called the Inreda Artificial Pancreas (Inreda Diabetic). The IRCM group performed home-based dual-hormone studies in 2016 to 2017, with SAP or single-hormone HCL as the control condition, and succeeded in showing improvements only in comparison with SAP, not with single-hormone HCL [109,110]. In 2017, the Beta Bionics group conducted a home-based study in 43 adults for up to 11 days and reported considerable improvements in TIR and TBR compared with CSII or SAP [111].
Next, the Oregon group performed outpatient dual-hormone studies with single-hormone HCL as the control, focusing on efficacy during exercise. In 2018, the dual-hormone system in 20 exercising T1DM patients across 4 days showed improvement in TBR 70 mg/dL compared with single-hormone HCL (1.3% vs. 2.8%, P<0.001) [53]. In 2020, the group also showed the efficacy of dual-hormone HCL with a stable liquid glucagon formulation in an exercising outpatient setting [36]. In 2021, the Inreda group conducted a two-week home-based study, the longest of the dual-hormone studies so far, and showed an improvement in TIR and TBR compared with CSII or SAP [50]. Remarkably, all the other dual-hormone systems were HCL systems, but in this study, the bolus dose was determined without requiring the user to enter the carbohydrate amount, so it can be regarded as an FCL. In the most recent study at the time of writing, the Beta Bionics group reported a small (7 days with 10 patients) study comparing a dual-hormone HCL using a dual-chamber pump (iLet, Beta Bionics) and dasiglucagon [54] with a single-hormone HCL. Although that study did not report statistical differences, the dual-hormone HCL showed higher TIR and TBR values than the single-hormone HCL.
Dual-hormone APS studies have thus grown larger and longer over time, and studies using CSII or SAP as the control have provided comparisons with single-hormone HCL systems. The development of dual-chamber pumps (Inreda and Beta Bionics groups), rather than separate pumps, is also a remarkable change. In addition, as shown in the Inreda group study, FCL is nearly a reality. According to the clinical evidence to date, dual-hormone APSs produce superior TIR and TBR to those with CSII or SAP. However, compared with single-hormone HCL systems, APSs have shown improvements only in groups vulnerable to hypoglycemia, such as exercising patients or children. However, most studies have compared dual-hormone HCL with its own single-hormone HCL in relatively small samples, and they generally showed superior TIR of 80s% versus 70s%, compared with the single-hormone group’s HCL studies. More accurate results could be obtained by conducting dual-hormone studies on a larger scale and comparing those systems with single-hormone HCL systems from single-hormone groups. Due to the limitations of using two pumps or two chambers and glucagon instability, no large-scale or long-term dual-hormone study has yet been conducted in contrast to single-hormone HCL systems. Although the Inreda APS received the CE mark [50], no product has yet been commercialized. The glucagon pump needs to be replaced daily, and the infusion set needs to be exchanged every 24 hours because the current glucagon formulations are unstable in the infusion sets after 24 hours. These problems might be solved by using a novel glucagon analog that is currently under development.
Additionally, the side effects of glucagon may be an important issue. Although none of the available data seemed to report serious adverse events to date, glucagon can cause side effects such as nausea and vomiting, and erythema at the glucagon infusion site. Glucagon also has potential pleiotropic effects on cardiac contractility, renal function, and the central nervous system [112]. Therefore, patients should be monitored for potential side effects of glucagon on the cardiovascular system, renal system, liver, and lipoprotein levels in long-term trials [112]. Other possible safety concerns, such as potential hepatic glycogen depletion and impaired glucagon response, have been raised regarding the use of glucagon in APS. However, in a human study of 11 adults with T1DM, hepatic glycogen stores and the response to glucagon were maintained after repeated doses of glucagon [113]. Given the lack of evidence regarding the long-term safety of glucagon in APS, additional data from large, long-term follow-up studies are necessary to address these concerns.
ADVERSE EVENTS OF CLOSED-LOOP SYSTEMS
So far, we have focused on the effects of APS, but adverse events should not be overlooked. The main adverse events in the previous major clinical trials are presented in Supplementary Table 2. For single-hormone HCL studies, although each study presented a different form, TBR <54 or <50 mg/dL were significantly improved in HCL compared to CSII (Florence system, TBR <50 mg/dL, 0.3% vs. 1.0%, P<0.01; Minimed 670G, TBR <54 mg/dL, 0.2% vs. 0.9%, P<0.01) [24,77]. When compared with SAP, some studies of single-hormone HCL showed improvements (Control-IQ, TBR <54 mg/dL, 0.29% vs. 0.35%, P=0.02; DBLG1, TBR <50 mg/dL, 0.2% vs. 0.7%, P<0.01) [45,47], and some did not show any difference (Florence system, TBR <50 mg/dL, 0.3% vs. 0.5%, P=0.11; DBLG1, TBR <54 mg/dL, 0.24% vs. 0.32%, P=0.42) [78,88]. When it comes to advanced HCL, TBR <54 mg/dL was superior to PLGS SAP (Minimed 780G vs. 640G, TBR <54 mg/dL, 0.4% vs. 0.5%, P=0.03) and was non-inferior to HCL (Minimed 780G vs. 670G, TBR <54 mg/dL, 0.46% vs. 0.50%, P<0.01 [non-inferior test]) [37,38]. For dual-hormone closed-loop systems, despite presenting only TBR of <60 mg/dL rather than <54 mg/dL, they all showed significant improvements even when compared to SAP (Beta bionics, TBR <60 mg/dL, 0.6% vs. 1.9%, P<0.01; Inreda, TBR <60 mg/dL, 0% vs. 0.5%, P<0.01) [50,111].
For severe hypoglycemia, which requires assistance from another person, most clinical studies showed no events in either the closed-loop system group or the control group. There were a few cases where it was slightly higher in the closed-loop or advanced closed-loop group, although no statistical comparison was presented (Minimed 670G vs. MDI or CSII, 8 events vs. 7 events; DBLG1 vs. SAP, 5 events vs. 3 events; 780G vs. 670G, 1 events vs. 0 events); however, most events were not related to the control algorithm [38,47,76]. Diabetic ketoacidosis also did not occur in either group in most studies, and even if it occurred, most of the cases were caused by other reasons (e.g., infusion set error) rather than automated insulin delivery function [37,45,76,78]. Therefore, based on these results, it can be said that the current APS is safe in terms of adverse events.
CLINICAL EVIDENCE IN OTHER PATIENT GROUPS
Type 2 diabetes mellitus
Most APS studies have been conducted in patients with T1DM who are insulin-dependent. However, T2DM patients can also become insulin-dependent as the disease progresses. Therefore, APS could be of great help to these patients. T2DM studies have been conducted mainly by the CamDiab group, though all were short-term and conducted among hospitalized patients (Table 4). The first HCL study in T2DM patients was performed in 2014 in 12 insulin-naive patients and reported improvement in TIR 70 to 180 mg/dL with HCL compared with glucose-lowering medication (40% vs. 24%, P=0.016) [114]. In 2017, a study was conducted in T2DM patients on insulin treatment for 3 days, resulting in TIR 100 to 180 mg/dL improvements compared with conventional insulin treatment (59.8% vs. 38.1%, P=0.004) [115]. In the following year, a larger study (136 patients, mean 8 days) produced substantial TIR improvements (65.8% vs. 41.5%, P<0.001) [43]. Moreover, a subgroup analysis showed that dialysis patients had even more remarkable improvement in TIR 100 to 180 mg/dL (69.0% vs. 31.5%, P<0.001) [116]. The IRCM group, which has mainly studied dual-hormone APS, announced a T2DM patient study of a single-hormone HCL in 2019 [117]. This was a small pilot study of 15 patients using MDI, and TIR 70 to 180 mg/dL on plasma glucose (PG), but not on sensor glucose, which is an APS study standard, was improved by the HCL. In the CamDiab studies, TIR improved by approximately 20% compared with conventional treatment, and the TIR in the HCL group was somewhat lower than in T1DM studies, which seems to be because TIR 100 to 180 mg/dL was used in T2DM studies instead of TIR 70 to 180 mg/dL. T2DM APS studies have not yet been conducted in outpatient settings, have been limited to short-term studies, and have not yet been compared with SAP.

Clinical evidence of closed-loop system in T2DM and pregnant T1DM
Pregnant type 1 diabetes mellitus patients
Pregnant T1DM patients have different blood glucose targets than the general T1DM population, and insulin resistance increases as pregnancy progresses, so the insulin requirement also changes during pregnancy [118]. Glycemic control during pregnancy is crucial because it has a considerable influence on both fetal and maternal outcomes. A large-scale study in pregnant T1DM patients found that CGM improved maternal and fetal outcomes [119]. Few APS studies have been conducted in pregnant subjects, mostly performed by the CamDiab group (Table 4). In 2011, after a safety study of OCL [120], HCL was compared with CSII for 2 days in 12 pregnant T1DM patients in a hospital, resulting in TBR <45 mg/dL improvement (0.0% vs. 0.3%, P=0.04) but no change in TIR 63 to 140 mg/dL [121]. In 2016, the HCL was compared with SAP for 4 weeks in 16 outpatients, and overnight TIR 63 to 140 mg/dL was remarkably improved (74.7% vs. 59.6%, P=0.002) [44]. In 2018, a similar study design was used to assess similar subjects all-day, and TIR did not differ, but TBR <63 mg/dL was improved (1.6% vs. 2.7%, P=0.04) [122]. To date, although evidence is lacking for all-day TIR, HCL has been shown to improve all-day TBR and overnight TIR. Based on this evidence, CamAPS FX was approved by CE in 2020 for use in pregnant T1DM patients. However, obstetric and neonatal outcomes have not been examined or compared with conventional treatments and more evidence is needed to inform on the suitability of the approach in such cases.
DO-IT-YOURSELF CLOSED-LOOP SYSTEMS
Advances in technology such as closed-loop APSs have allowed patients with T1DM to have better glycemic control and improved quality of life. However, some T1DM patients and their caregivers were unsatisfied with the current pace of commercial APS development and thus began the #WeAreNotWaiting movement on social media in 2013 [39]. Initially, this DIY movement included only a few users who were developing and sharing programs to manage their CGM and insulin pumps independently. Since then, several open source platforms have been developed to allow T1DM patients to build artificial pancreas technology without regulatory approval, and the number of DIY closed-loop users has been growing steadily alongside several thousands of patients using commercial closed-loop systems [123]. A DIY closed-loop system uses a processor capable of receiving CGM data and open source control algorithms to control the rate of insulin delivery through a compatible insulin pump [123].
The three main DIY closed-loop software systems in use are OpenAPS, Loop, and AndroidAPS [39]. None of them had received regulatory approval because they had not undergone clinical trials, and all studies to date have been retrospective (Supplementary Table 3) [124-132]. One randomized clinical trial using AndroidAPS and the DANA-I pump is currently ongoing (ACTRN12620000034932) [133]. In addition, Tidepool, a non-profit software organization sponsored by Juvenile Diabetes Research Foundation and the Helmsley Charitable Trust, is developing an APS application based on the Loop DIY algorithm to receive FDA approval [39]. Although these DIY closed-loop systems have not yet been approved, they have the benefits of rapid development cycles and flexibility in terms of customization (such as individualized target glucose ranges) [125]. Observational studies conducted via online surveys and sentiment analyses of Twitter data suggest that DIY closedloop systems have beneficial effects on glycemic control and users’ quality of life [126]. For example, in an online survey, 56% of DIY closed-loop users reported a large improvement in sleep quality [134]. A study conducted in Italy reported a significant decrease in HbA1c (from 7.17% to 6.61%, P<0.05) after implementation of the OpenAPS in 30 patients with T1DM [135]. Data from T1DM patients in Korea using OpenAPS also showed a significant decrease in HbA1c (6.8% to 6.3%, P<0.001) and an increase in percent TIR (70.1% to 83.3%, P<0.001) [136]. However, these data have sample size and methodological limitations. Given the lack of regulatory approval and insufficient data regarding safety, the use of DIY closed-loop systems is considered risky. When a problem occurs in a DIY system, it can be difficult to solve. Moreover, when medical accidents occur, the subject of responsibility is unclear, and legal and ethical problems can arise [137].
In May 2020, Diabetes UK released a position statement about unapproved DIY closed-loop systems recommending that T1DM patients who wish to use such systems are aware that their choice is at their own risk [138]. DIY closed-loop systems cannot be ignored, but there is a paucity of research on their safety and efficacy. Therefore, patients using DIY closedloop systems should continue to receive care from healthcare professionals.
OTHER POTENTIAL ADJUNCTIVE HORMONES AND HORMONE-LIKE PEPTIDES
Researchers are looking for ways to address the challenges that result from the pharmacokinetics of insulin in APSs. To mimic the function of the pancreas more perfectly and reduce the time of postprandial hyperglycemia, researchers have been investigating other peptide hormones and hormone-like peptides.
Amylin analogues
Amylin is a peptide hormone that is co-secreted with insulin and is produced by pancreatic β-cells. It regulates postprandial glucagon secretion and hepatic glucose production, delays gastric emptying, and promotes satiety [139,140]. Patients with T1DM often have a deficiency in this peptide because of the destruction of β-cells [141]. In light of this, several studies have investigated the efficacy of co-administration of synthetic amylin (pramlintide) in closed-loop systems (Supplementary Table 4) [142,143]. These trials suggest that co-administration of pramlintide with insulin reduces the magnitude of postprandial increments in PG by delaying the time to peak postprandial PG compared with the treatment with insulin alone or insulin plus placebo [40,142-144]. In a study conducted by Weinzimer et al. [142], pramlintide administration delayed the time to peak blood glucose (2.5 hours vs. 1.5 hours, P<0.0001) compared with a closed-loop system alone. Another trial compared the post-meal incremental PG area under the curve (AUC) from a single dose of pramlintide (60 μg) with that of a control group (without pramlintide). Insulin with pramlintide reduced the post-meal incremental PG AUC (P=0.0002) [143]. In a randomized, single-blind, 24-hour, crossover inpatient study, mean 24-hour glucose measured by CGM was lower upon coadministration of pramlintide versus placebo (153 mg/dL vs. 174.6 mg/dL, P=0.012) [144]. In a randomized crossover trial comparing a rapid insulin alone APS with a rapid insulin and pramlintide system, the rapid insulin and pramlintide system increased TIR from 74% to 84% (P=0.0014) [40]. These studies were small and conducted under controlled conditions in the hospital. The most common adverse effects of pramlintide are gastrointestinal symptoms, such as nausea and vomiting, which occur in 9.5% to 59% of patients [145]. To determine whether chronic administration of pramlintide could improve glycemic control in patients with T1DM, longer studies with dose titration should be conducted under the conditions of daily life.
GLP-1 receptor agonist
GLP-1 is released mostly by intestinal L-cells, with small quantities secreted by pancreas [146]. GLP-1Rs are expressed not only in the gastrointestinal tract, but also in other tissues and organs, including the vascular smooth muscle, brain, heart, kidney, and lung [146]. Following several trials in T2DM patients, a GLP-1R agonist has been approved for diabetes management, and it also demonstrated cardiovascular benefits [147]. Therefore, GLP-1R agonists are under investigation as potential adjunctive therapies for closed-loop APSs [148].
An RCT with a crossover design suggested the efficacy of an adjuvant GLP-1 agonist (liraglutide) and insulin in patients with T1DM using a closed-loop system (Supplementary Table 4). In the study of Ilkowitz et al. [41], the mean blood glucose levels and postprandial blood glucose levels were lower in the liraglutide arm (liraglutide vs. insulin monotherapy, 144.6 mg/dL vs. 159.7 mg/dL, P=0.0002). In a head-to-head study comparing a GLP-1 agonist (exenatide) and pramlintide in T1DM patients using a closed-loop system, the GLP-1 agonist showed a postprandial glucose-lowering effect superior to that of pramlintide (TIR 70 to 180 mg/dL, 77% vs. 62%) [148]. These studies support the idea that the adjunctive use of a GLP-1 agonist could closely mimic the physiological state of the pancreas. However, it is important to note that both studies were performed for fewer than 2 days with only 10 to 15 participants. Further research in large samples is required to investigate the long-term use of a GLP-1 agonist in a closed-loop system.
Intraperitoneal delivery of insulin
To achieve suitable glycemic levels, IP insulin delivery is considered a viable alternative to the conventional route for insulin delivery [149]. IP insulin delivery systems are generally composed of a catheter inserted into the peritoneal cavity and an insulin infusion pump. Insulin is infused from an externally placed or implanted pump into the abdominal wall. Some researchers have suggested that IP insulin delivery has physiological advantages that result from faster pharmacokinetics and pharmacodynamics, which provide a better insulin/glucagon balance [150,151]. Other researchers have reported that IP insulin delivery might reduce the frequency of hypoglycemic events (Supplementary Table 4) [152,153]. Renard et al. [154] demonstrated the feasibility of a closed-loop IP insulin pump in a hospital setting. Recently, Dassau et al. [42] conducted a pilot study comparing an implantable IP insulin pump to subcutaneous insulin injection from an APS. In that study, the IP route provided better glucose control than subcutaneous insulin delivery. However, implantable IP insulin pumps are available in only a few European countries, and further studies are required to address safety issues such as infections or hematomas at the implant site.
LIMITATIONS AND FUTURE DIRECTIONS
Since the basic experiments in the 2000s, numerous APSs have been developed, clinically validated, commercialized, and used in actual practice for T1DM patients. Despite recent radical advances in APS technology, a genuinely FCL that effectively accomplishes glycemic control in every situation without meal or exercise announcements has not yet been demonstrated. Several early studies attempted automatic control of postprandial glucose without the need to enter carbohydrate contents, but most of them were non-comparative feasibility studies conducted for short periods in hospital settings [19,20,155-157]. Although FCL in early studies offers better glycemic control than open-loop systems [155], some studies showed that they were worse than HCL with meal announcements [19]. These shortcomings result from the inherent limitations of closed-loop systems. In healthy human bodies, blood glucose is detected, and insulin is directly secreted into the blood vessels by the pancreas. In contrast, in a closed-loop system, a CGM detects glucose in interstitial fluid, not blood, and insulin is injected into subcutaneous tissues instead of blood vessels, which incurs time lags. For this reason, controlling glucose without the help of manual bolus control remains difficult in situations where blood glucose changes rapidly, such as after meals or during exercise. In addition, as shown by real-world evidence, improving compliance is an important issue because of the difficulty in wearing current systems [158].
Several possibilities for solving these problems have been suggested and attempted. To solve the time lag during insulin infusion, it might be possible to develop and apply faster-acting insulin. APS studies using faster-acting insulin (e.g., Fiasp) are in progress and at the time of writing, CamAPS FX has been approved to use Fiasp [100,159]. In addition, it could be possible for an APS system to accurately predict the blood glucose response automatically by having the patient take a picture of their meal using an artificially intelligent camera instead of manually counting the carbohydrates [160]. As seen in the Inreda group study, advances in a dual-hormone closedloop system that can actively improve hypoglycemia might also lead to an FCL [50]. To that end, the instability of glucagon and the inconvenience of multiple insertion sites must be corrected. Building an all-in-one wearable APS system that combines CGM, a patch pump, and the control algorithm into one device to improve user comfort is another development direction. Because APS has only been evaluated in short-term hospital-based studies in T2DM patients, and no study has considered pregnant T2DM or gestational diabetes patients [43,117], APS development for those populations, who require intensive insulin treatment, is a task for future researchers. In addition, APS studies might also be needed in situations in which blood glucose goes rapidly out of control, such as during steroid treatments, transplantation, or chemotherapy.
Supplementary Materials
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2021.0177.
clinical evidence of overnight closed-loop system (single-hormone) in type 1 diabetes mellitus
Adverse events of closed-loop systems in major clinical trials
Clinical evidence of DIY closed-loop system in type 1 diabetes mellitus
Clinical evidence of amylin analogues, GLP-1 receptor agonist, and intraperitoneal insulin delivery in artificial pancreas system
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: 1711138946, KMDF_PR_20200901_0295), and by Lim Se-Won Medical Research Funds from Kangbuk Samsung Hospital.
Acknowledgements
None