
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(6); 2011 > Article
-
Original ArticleLow Density Lipoprotein Cholesterol Target Goal Attainment Rate and Physician Perceptions about Target Goal Achievement in Korean Patients with Diabetes
- Jenie Yoonoo Hwang1, Chang Hee Jung1, Woo Je Lee1, Cheol Young Park2, Sung Rae Kim3, Kun-Ho Yoon3, Moon Kyu Lee4, Sung Woo Park2, Joong-Yeol Park1
-
Diabetes & Metabolism Journal 2011;35(6):628-636.
DOI: https://doi.org/10.4093/dmj.2011.35.6.628
Published online: December 26, 2011
1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
2Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
3Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea.
4Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding author: Joong-Yeol Park. Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, 388-1 Poongnap 2-dong, Songpa-gu, Seoul 138-736, Korea. jypark@amc.seoul.kr
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study aims to investigate the discrepancy between clinicians' perceptions and actual achievement rates of low density lipoprotein cholesterol (LDL-C) in Korean patients with diabetes according to updated American Diabetes Association (ADA)/American College of Cardiology Foundation (ACC) recommendations.
-
Methods
- This is a multi-center, retrospective, non-interventional, observational study. Diabetic patients aged 18 years or older were eligible if they had been diagnosed with hypercholesterolemia or were receiving a lipid-lowering therapy between May 2010 and August 2010. The information was obtained by reviewing medical records and using a self-completed questionnaire to examine physician perceptions.
-
Results
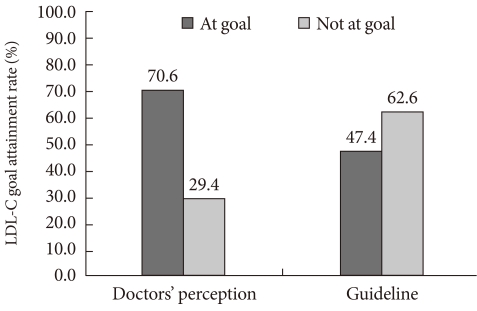
- A total of 2,591 subjects who satisfied the inclusion criteria were enrolled. Highest-risk and high-risk patients accounted for 61.9% and 38.1% of the patients, respectively. Although most (96.3%) underwent a statin monotherapy or a statin-based combination therapy, just 47.4% of patients attained the LDL-C target. However, the physicians' perceptions on target achievement rate (70.6%) were different from the actual results (47.4%). Many patients (65.3%) remained on the starting doses of statins, despite evidence of poor achievement of lipid goals.
-
Conclusion
- Only less than half of patients with diabetes attained the LDL-C goal. The surveys showed that poor physician performance might be due to the lack of recognition on ADA/ACC consensus causing a low LDL-C target attainment rate. Therefore, changes in doctor perception are needed to attain target LDL-C level and reduce cardiovascular risk in Korean patients with diabetes.
- Cardiovascular disease (CVD) is the major cause of mortality and morbidity in patients with type 2 diabetes [1]. The increased risk of CVD in subjects with type 2 diabetes consists of multiple factors such as hypertension, smoking, albuminuria and hypercholesterolemia [2]. Among them, hypercholesterolemia is one of the key factors that are amenable to intervention.
- A large body of research ranging from molecular to population studies indicates that elevated low density lipoprotein cholesterol (LDL-C) is a major predictor of CVD, including in populations with diabetes [3,4]. Treatments for lowering LDL-C below the target level recommended by several guidelines are emphasized in patients with type 2 diabetes due to the increased risk of CVD [5]. Patients with type 2 diabetes without a history of myocardial infarction are regarded to have the same risk of a coronary event as patients without diabetes who have a history of myocardial infarction [6]. This observation was part of the basis for the recommendation by the Adult Treatment Panel III (ATP III) of the National Cholesterol Education Program (NCEP) that diabetes should be considered a "coronary heart disease risk equivalent" and the resulting target for aggressive reduction of risk factors [7]. In line with this, recent guidelines from the American Diabetes Association (ADA) recommended the use of statins for primary prevention of CVD in type 2 diabetes patients [8]. Considering the results of previous study mentioned above [6], recent guidelines will provide good evidence on the quantitative relation between achieving target cholesterol concentration and the probability of cardiovascular events in subjects with diabetes [9].
- In 2008, the ADA, in consensus with the American College of Cardiology Foundation (ACC), released guidelines [10] following the NCEP 2003 updated recommendations which included an "optional" LDL-C goal <70 mg/dL for patients who are at the "highest risk" for CVD [11]. Highest-risk patients were defined as 1) patients with CVD or 2) patients with diabetes plus one or more additional major CVD risk factors (smoking, hypertension, and family history of premature CVD). High-risk patients was defined as 1) patients who have diabetes but have no major cardiovascular risk factors and 2) patients who do not have diabetes or CVD but have more than two major cardiovascular risk factors. For these patients, the guidelines recommended a target LDL-C less than 100 mg/dL.
- Despite available therapies and increased attention to hypercholesterolemia, many patients failed to achieve the LDL-C goals [12]. Data from the third U.S. National Health and Nutrition Examination Survey (NHANES;1988-1994) showed only 42% of patients with diabetes achieved an LDL-C <130 mg/dL [13]. More recent data with the NCEP 2004 updated recommendations demonstrated only 29.4% of very-high-risk patients with both diabetes and CVD reached the LDL-C goal of <70 mg/dL in the United States [14]. There is a need to better understand the reasons why most patients failed to reach these goals despite pharmacological treatment.
- Unfortunately, it is uncertain whether target LDL-C level is commonly reached in Korean patients with diabetes. Therefore, we aimed to investigate the lipid target attainment rates according to the ADA and ACC consensus recommendation in Korean patients with diabetes and investigate physician perceptions on lipid target attainment and compared them with actual attainment rates.
INTRODUCTION
- Subjects
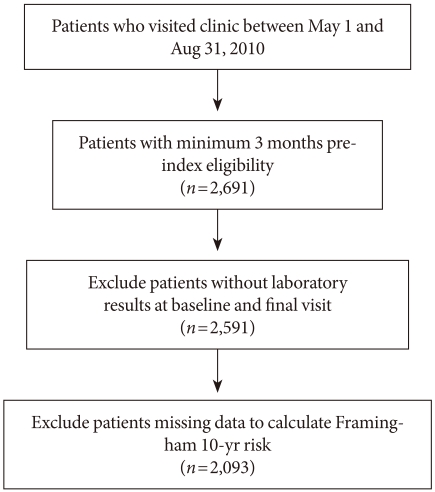
- The study population consisted of 2,661 patients who were under the care of diabetic specialists at the 53 secondary and tertiary hospitals in Korea between 1 May 2010 and 31 August 2010 (Fig. 1). Patients were selected from the outpatient clinics of these hospitals with the following selection criteria: 1) type 2 diabetes according to ADA criteria, 2) at least 18 years of age, 3) newly diagnosed with hypercholesterolemia or previously diagnosed with hypercholesterolemia but not on lipid-lowering medication for at least one month prior to the initial visit, 4) on lipid-lowering treatment for at least 3 months. Hypercholesterolemia was defined according to NCEP-ATP III [15]. Patients were eligible for enrollment if they had visited the hospital at least once during the last 3 months. Detailed information on baseline characteristics including age, sex, body mass index (BMI), smoking status, the duration of diabetes, hypertension status, past history of CVD, family history of premature CVD and concomitant medication use was collected by study site personnel through review of medical records. Hypertension was defined as a systolic blood pressure (SBP) ≥140 mm Hg and/or diastolic BP (DBP) ≥90 mm Hg or taking antihypertensive medications. History of CVD was based on each subject's history of angina, myocardial infarction and/or cerebrovascular accidents. Smoking status was classified into non-smoker, ex-smoker and current smoker. The self-completed questionnaire on physicians' perceptions of the achievement rates of LDL-C targets was additively completed through an online survey.
- We excluded subjects who met at least one of the following criteria: 1) current enrollment in other clinical studies, 2) participation in any clinical studies within the previous 90 days (except non-interventional and registry studies), 3) unable or unwilling to reveal medical records. After exclusion of ineligible subjects, 2,591 subjects (1,278 men, mean age 56.1±10.8; and 1,313 women, mean age 61.1±10.2) were included in this study.
- Study design
- This study was a multi-center, non-interventional study using retrospective medial chart reviews. Doctors provided detailed information on patient characteristics and their perception of LDL-C treatment goal achievement. All data were entered and collected in an eCRF, and the eCRF manual was provided separately to the investigator. This study was approved by the Institutional Review Board of the hospitals to which the participating investigators belonged.
- Study variables
- The values of LDL-C were determined by direct measurement when triglyceride (TG) was higher than 400 mg/dL or patients were on fibrates. Except those conditions, LDL-C was calculated from the Friedwald formula as following: Total cholesterol (TC)-[high density lipoprotein cholesterol (HDL-C)+TG/5]. These values were recorded using the web database. Laboratory records included the date of testing. The Framingham risk score modified by ATP III, which incorporated age, gender, LDL-C, HDL-C, BP, smoking status and TC, was used.
- Use of lipid-lowering medication was determined by medical records. Patients were considered to be on a lipid lowering therapy if they had at least one subscription for any lipid-modifying medications during the follow-up period. Statin titration was defined as an increase in the strength of the dispensed statin. A switch was defined as a change of lipid drugs, either statin or non-statin.
- Study Objectives
- The objective of this study was to investigate the discrepancy between clinicians' perceptions and the actual achievement of LDL-C targets in Korean diabetic patients according to the updated ADA/ACC recommendations.
- Statistical methods
- Continuous variables are expressed as mean±standard deviation, and categorical variables are expressed as number and proportions (%). Most data are summarized with descriptive statistics. Student's t-tests or paired t-tests were used for continuous variables, and chi-squared tests were used for categorical variables. Multivariate logistic regression analysis was performed to identify the factors contributing to the failure of LDL-C target attainment. Significance was set at 0.05. All statistical analysis was performed using SPSS version 14.0 for Windows (SPSS Inc., Chicago, IL, USA).
METHODS
- Clinical and biochemical characteristics of the subjects
- Baseline characteristics of study participants are presented in Table 1. The mean age of patients was 60.8±10.5 years. On average, the patients had a mean BMI of 25.2 kg/m2. Male subjects had a higher proportion of CVD and atrial fibrillation and were younger, more often at highest-risk, and current smokers (P<0.05 for each). Patients with previously diagnosed CVD compromised 10.8% of subjects.
- Attainment of target LDL-C level
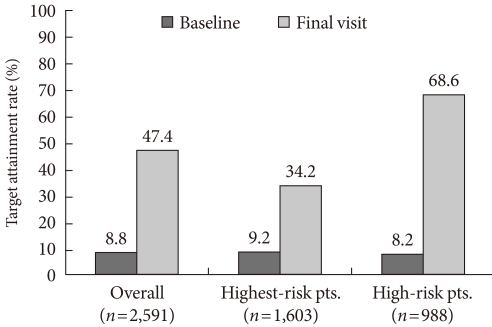
- According to the 2008 ADA/ACC guidelines, 1,603 (61.9%) of the 2,591 patients were highest-risk and 988 (38.1%) were high-risk (Table 1). The mean observed duration of statin use was 23.1±26.2 months. The achievement rate of target LDL-C level (<70 mg/dL in the highest-risk group and <100 mg/dL in the high-risk group, respectively) was 8.8% at baseline. After treatment during the follow-up period, LDL-C target attainment increased up to 47.4% (Fig. 2). Among the high-risk patients (n=988), LDL-C goal attainment increased from 8.2% to 68.6%. For the highest-risk group (n=1,603), target LDL-C attainment increased from 9.2% to 34.2%.
- Further analyses of the proportion of patients achieving the goal were conducted according to sex. The percentage of patients reaching the LDL-C goal was similar between female (46.2%) and male patients (48.5%).
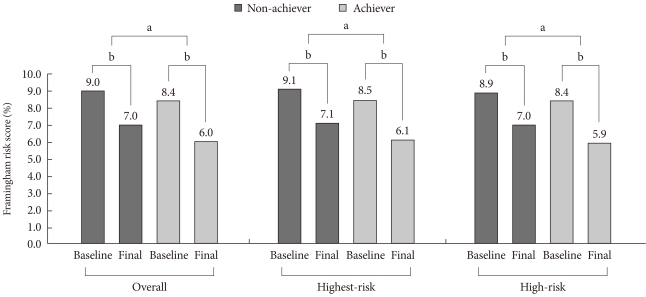
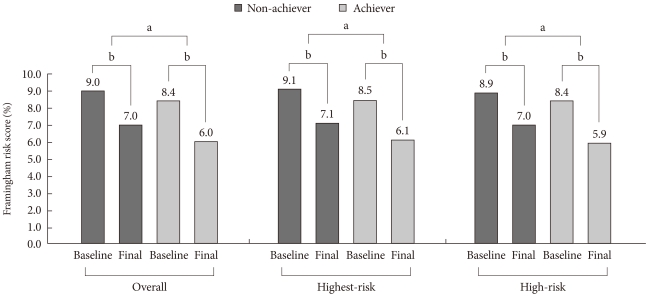
- Regarding the reduction of risk for future CVD by decreased LDL-C level, Framingham risk score was significantly lower after using lipid-lowering drug at final visit compared to the baseline Framingham risk score, as shown in Fig. 3 (P<0.0001). When we compared the scores by stratifying the subjects who achieved the LDL-C target into high- and highest-risk groups, a significant difference was observed in the both group at the initial visit and the final visit (8.5±3.3 vs. 6.1±3.2, P<0.0001 in the highest risk patients; 8.4±3.2 vs. 5.9±3.2, P<0.001 in the high risk patients). Furthermore, goal-achievers at final visit had significant reduction of Framingham risk score at the final visit compared to non-achievers (P<0.05).
- Physician treatment strategies and factors affecting LDL-C goal attainment
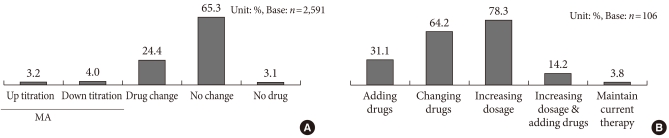
- In general, 65.3% of patients did not switch drugs between baseline and the final visit (Fig. 4A). Increased titration was prescribed in only 3.2% of patients, while 4.0% were prescribed decreased titration. Among 3-hydroxy-3-methyl-CoA reductase (HMG-CoA reductase) inhibitors, rosuvastatin was the most frequently used one (48.8%). Fibrates were being taken by 6.9% of patients at the initial visit and were newly subscribed to 3.4% of patients during the follow-up period.
- To identify the factors affecting LDL-C goal attainment, we compared the baseline characteristics between target LDL-C achievers and non-achievers regarding to sex, age, BMI, HbA1c, LDL-C, HDL-C, TC, smoking history and blood pressure. The results showed that patients who did not attain the LDL-C goal were more likely to be current smokers, have a family history of premature CVD, hypertension, lower HDL-C level, and higher LDL-C level (P<0.05 each). A logistic regression analysis was performed with these variables, which showed that subjects with older patients, patients with higher baseline LDL-C and current smokers tended to fail to achieve target LDL-C level. When we analyzed the factors in high-risk and highest-risk group separately, age, smoking, and higher baseline LDL-C level were the significant factors affecting LDL-C target attainment in the high-risk group, while age and smoking history were those in the highest-risk group (P<0.05, respectively). The effects of non-statins, statin titration, and switching between lipid-lowering drugs on goal achievement were not analyzed. The average treatment doses were not statistically different between groups.
- Physician perceptions of LDL-C goal achievement
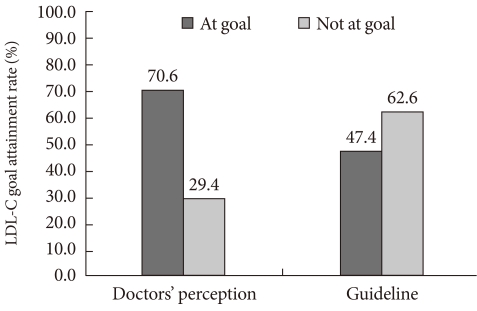
- To analyze the possible factors contributing to the low target goal attainment rate (47.4% overall, Fig. 2), physicians completed a self-reporting survey. As shown in Fig. 5, we found that physician perceptions of target LDL-C achievement differed from the guidelines. Of those who were initially tested for LDL-C after diagnosis of diabetes, a majority (83.2%) were classified as high-risk by the physicians, while only 14.8% were classified as highest-risk. After treatment, while 70.6% were perceived to have achieved the target LDL-C by physicians, only 47.4% achieved the goal according to the ADA/ACC guidelines.
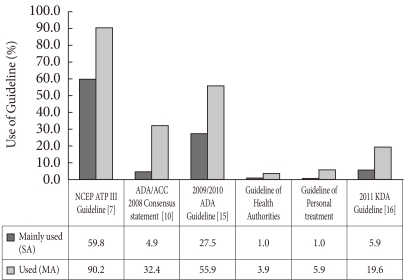
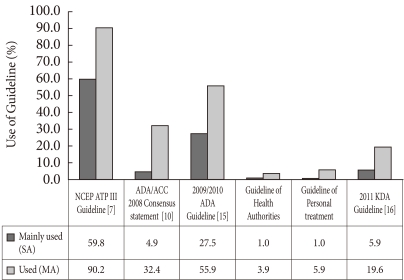
- For the diagnosis of hypercholesterolemia, physicians considered the following lipid levels most important (in descending order): LDL-C (92.5%), TG (46.2%), HDL-C (38.7%), and TC (57.5%). From the survey, doctors reported that 96.2% used guidelines for setting target cholesterol level. The guidelines commonly used are shown in Fig. 6, with the NCEP ATP III guidelines being the most frequent.
- Ninety-eight percent of physicians reported that they informed patients of their cholesterol value, and most (86.8%) also informed patients of their LDL-C level. Regular follow-ups on cholesterol level were completed every 6 months in 56.6% of cases, every 3 months in 25.5%, and once a year in 13.2%. When the target goal was not achieved, physicians replied that they would increase dosage (78.3%) or change medication (64.2%) (Fig. 4B). However, increased titration was carried out in only 3.2% of patients (Fig. 4A).
RESULTS
- In this study, the ADA/ACC recommended LDL-C goal was achieved in approximately 47.4% of Korean patients with diabetes, which was significantly lower than physicians' perceptions (70.6%). Compared to those who did not reach the target LDL-C level, the risk of future coronary heart disease (CHD) was substantially lower among those who did achieve the goal, as shown in the reduction of the Framingham risk score.
- This study also demonstrated that there was a large gap between physicians' perceptions and guidelines in categorizing the severity of hypercholesterolemia. Although most physicians answered that they would increase the dosage of lipid-lowering medications if the target LDL-C goal was not reached, only 3.2% prescribed increased titration (Fig. 4A). Although factors affecting physicians' recognition were not analyzed, inferring by the fact that most patients were considered high-risk but not highest-risk to physicians, the updated guidelines might not be fully recognized.
- During the treatment period, 65.3% of patients did not have any drug adjustment, including up-titration, add-on, or drug switching (Fig. 4A). Factors such as old age, multi-drug usage, and adverse effects of up-titration or combination therapy might have affected physician decisions. Also, the guidelines used by the physicians may have affected LDL-C level. From the survey, NCEP APT III guidelines [7] (59.8%) were the most frequently used. The 2009/2010 ADA guidelines [8] (27.5%), ADA/ACC consensus statement (4.9%), and Korean Diabetes Association (KDA) guidelines [16] (5.9%) were applied less frequently.
- A few studies have evaluated the attainability of the more aggressive LDL-C treatment goal recommended by the NCEP ATPIII or ADA guidelines [14,17]. Kennedy et al. [14] reported that it would be extremely difficult to reach an LDL-C goal of <70 mg/dL in patients with diabetes and CVD in the United States. They estimated that 25% of patients would require more than two lipid-lowering drugs at maximal doses to attain this goal [14]. In a recent survey of 4,888 patients treated with statins, only 38% reached the recommended LDL-C level according to the NCEP guidelines [12]. Although our study was conducted ten years later and used the ADA/ACC guidelines, our findings were consistent with the results of above studies.
- It has been suggested that if LDL-C goals are not met, it is necessary to take patient opinions about their illness into account. A prospective survey in Australia using prescription renewals as a surrogate for drug discontinuation found that 60% of patients stopped their medication after 1 year, and half of them discontinued within 3 months of therapy initiation. A major reason for discontinuation was lack of self-perception regarding the need for further treatment [18]. However, when patients were compliant, there were many possible pitfalls underlying patient non-achievement with current treatment goals such as inappropriate drug or dose selection, limited drug efficacy. Failure to achieve target LDL-C level was in large part due to inadequate doses or titration by physicians. Most patients who began treatment with a statin remained at the initial dose [19,20].
- In other studies [19,21], patients with diabetes had the lowest success rate in the treatment with lipid lowering drugs. However, subjects with diabetes are known to be at a substantially higher risk for stroke [22], CHD, and death [5]. Moreover, diabetics with [23] or without [24] established CHD benefit from statin treatment in a manner equal to or greater than that of nondiabetic subjects [20,21]. A subgroup analysis of the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) study which compared structured care and usual care in clinical practice in Greece [23] found that diabetic patients showed early reductions of more than 50% in total mortality, coronary mortality, coronary morbidity, and stroke in the structured care arm. The Collaborative Atorvastatin Diabetes Study (CARDS) showed that, over a 3-year period, a daily 10 mg dose of atorvastatin reduced the risk of a major cardiovascular event in patients with type 2 diabetes mellitus without incident CHD by 37% and that of stroke by almost half (48%) [24]. In our study population, 10.8% of subjects had previous CVD, and a majority (61.9%) was classified as at highest-risk. Although the current treatment gap in LDL-C targets is comparable with published international data, this gap is unacceptable, and undoubtedly leads to an excess number of cardiovascular deaths, infarcts, strokes and need for revascularization. To improve the management of hypercholesterolemia, physicians should be aware of and focus on patients with diabetes. A recent randomized controlled trial demonstrated the incremental impact of team-based care approach to cholesterol management in patients with diabetes [25]. Although primary study outcome was set as achieving LDL-C level of 100 mg/dL regardless of CVD risk, it showed that physician-paramedical staff approach can be considered to improve LDL-C goal attainment.
- A major strength of this study was the large sample size; nearly 2,600 patients were included in the main analysis. Another advantage is the inclusion of a survey concerning physician perceptions in the diagnosis of hypercholesteroelemia and treatment strategy. However, this study had several limitations. The diagnosis of CVD used to classify patients into high-risk and highest-risk categories was based on a chart review. Thus, misclassification of LDL-C severity and outcome may have occurred. Also, we did not have detailed dietary information for the patients and therefore could not estimate the effects of dietary intervention on LDL-C level [26]. Another limitation was that the study population did not reflect patients with diabetes who were receiving primary care. Finally, the sex-specific Framingham CHD predictions have not been validated in Koreans. The Framingham prediction was first demonstrated in Caucasians and was later applied to Japanese-Americans and other ethnic groups after recalibration for differing prevalence of risk factors [27]. However, no validation or recalibration has been carried out in Koreans. Furthermore, our study was able to measure the effect of statins over only a short-term period. In many instances, statin treatment had been ongoing for a long period of time. Additionally, patient compliance with the lipid-modifying drugs was not monitored.
- In conclusion, this study showed that actual LDL-C target attainment rates according to the ADA/ACC consensus statement were low in Korean patients with diabetes. However, more than 70% of physicians perceived their patients to have achieved these goals. Thus, our results suggested that changes in clinical practices and physician perceptions might be needed to reach cholesterol target goals recommended by updated guidelines.
DISCUSSION
-
Acknowledgements
- This study was funded by AstraZeneca Korea.
ACKNOWLEDGMENTS
- 1. Bloomgarden ZT. Diabetes and cardiovascular disease. Diabetes Care 2011;34:e24-e30. ArticlePubMedPMCPDF
- 2. Webb DR, Khunti K, Gray LJ, Srinivasan BT, Farooqi A, Wareham N, Griffin SC, Davies MJ. for the ADDITION-Leicester study group. Intensive multifactorial intervention improves modelled 5-year coronary heart disease risk in screen-detected type 2 diabetes mellitus: a cluster randomized controlled trial. Diabet Med Epub 2011 Sep 13. DOI: 10.1111/j.1464-5491.2011.03441.x.
- 3. Pedersen TR, Kjekshus J, Berg K, Haghfelt T, Faergeman O, Faergeman G, Pyorala K, Miettinen T, Wilhelmsen L, Olsson AG, Wedel H. Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). 1994. Atheroscler Suppl 2004;5:81-87. PubMed
- 4. Sato H, Kinjo K, Ito H, Hirayama A, Nanto S, Fukunami M, Nishino M, Lim YJ, Kijima Y, Koretsune Y, Nakatani D, Mizuno H, Shimizu M, Hori M. Osaka Acute Coronary Insufficiency Study (OACIS)-LIPID Study Investigators. Effect of early use of low-dose pravastatin on major adverse cardiac events in patients with acute myocardial infarction: the OACIS-LIPID Study. Circ J 2008;72:17-22. ArticlePubMed
- 5. Almdal T, Scharling H, Jensen JS, Vestergaard H. The independent effect of type 2 diabetes mellitus on ischemic heart disease, stroke, and death: a population-based study of 13,000 men and women with 20 years of follow-up. Arch Intern Med 2004;164:1422-1426. ArticlePubMed
- 6. Bulugahapitiya U, Siyambalapitiya S, Sithole J, Idris I. Is diabetes a coronary risk equivalent? Systematic review and metaanalysis. Diabet Med 2009;26:142-148. ArticlePubMed
- 7. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497. ArticlePubMed
- 8. American Diabetes Association. Standards of medical care in diabetes--2011. Diabetes Care 2011;34(Suppl 1):S11-S61. ArticlePubMedPMCPDF
- 9. LaRosa JC. At the heart of the statin benefit. J Am Coll Cardiol 2005;46:1863PubMed
- 10. Brunzell JD, Davidson M, Furberg CD, Goldberg RB, Howard BV, Stein JH, Witztum JL. American Diabetes Association. American College of Cardiology Foundation. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care 2008;31:811-822. PubMed
- 11. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC Jr, Stone NJ. National Heart, Lung, and Blood Institute. American College of Cardiology Foundation. American Heart Association. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004;110:227-239. ArticlePubMed
- 12. Pearson TA, Laurora I, Chu H, Kafonek S. The lipid treatment assessment project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med 2000;160:459-467. ArticlePubMed
- 13. Saaddine JB, Engelgau MM, Beckles GL, Gregg EW, Thompson TJ, Narayan KM. A diabetes report card for the United States: quality of care in the 1990s. Ann Intern Med 2002;136:565-574. ArticlePubMed
- 14. Kennedy AG, MacLean CD, Littenberg B, Ades PA, Pinckney RG. The challenge of achieving national cholesterol goals in patients with diabetes. Diabetes Care 2005;28:1029-1034. ArticlePubMedPDF
- 15. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-3421. ArticlePubMed
- 16. Ko SH, Kim SR, Kim DJ, Oh SJ, Lee HJ, Shim KH, Woo MH, Kim JY, Kim NH, Kim JT, Kim CH, Kim HJ, Jeong IK, Hong EK, Cho JH, Mok JO, Yoon KH. Committee of Clinical Practice Guidelines, Korean Diabetes Association. 2011 clinical practice guidelines for type 2 diabetes in Korea. Diabetes Metab J 2011;35:431-436. ArticlePubMedPMC
- 17. Yan AT, Yan RT, Tan M, Hackam DG, Leblanc KL, Kertland H, Tsang JL, Jaffer S, Kates ML, Leiter LA, Fitchett DH, Langer A, Goodman SG. Vascular Protection (VP) and Guidelines Oriented Approach to Lipid Lowering (GOALL) Registries Investigators. Contemporary management of dyslipidemia in highrisk patients: targets still not met. Am J Med 2006;119:676-683. ArticlePubMed
- 18. Simons LA, Levis G, Simons J. Apparent discontinuation rates in patients prescribed lipid-lowering drugs. Med J Aust 1996;164:208-211. ArticlePubMedPDF
- 19. Diamantopoulos EJ, Athyros VG, Yfanti GK, Migdalis EN, Elisaf M, Vardas PE, Manolis AS, Karamitsos DT, Ganotakis ES, Hatseras D. OLYMPIC Study Group. The control of dyslipidemia in outpatient clinics in Greece (OLYMPIC) Study. Angiology 2005;56:731-741. ArticlePubMedPDF
- 20. Hobbs FD, Southworth H. Achievement of English National Service Framework lipid-lowering goals: pooled data from recent comparative treatment trials of statins at starting doses. Int J Clin Pract 2005;59:1171-1177. ArticlePubMed
- 21. Alzahrani T, Marrat S, Haider A. Management of dyslipidemia in primary care. Can J Cardiol 2003;19:1499-1502. PubMed
- 22. Tuomilehto J, Rastenyte D, Jousilahti P, Sarti C, Vartiainen E. Diabetes mellitus as a risk factor for death from stroke. Prospective study of the middle-aged Finnish population. Stroke 1996;27:210-215. ArticlePubMed
- 23. Athyros VG, Papageorgiou AA, Symeonidis AN, Didangelos TP, Pehlivanidis AN, Bouloukos VI, Mikhailidis DP. GREACE Study Collaborative Group. Early benefit from structured care with atorvastatin in patients with coronary heart disease and diabetes mellitus. Angiology 2003;54:679-690. ArticlePubMedPDF
- 24. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, Thomason MJ, Mackness MI, Charlton-Menys V, Fuller JH. CARDS investigators. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685-696. ArticlePubMed
- 25. Pape GA, Hunt JS, Butler KL, Siemienczuk J, LeBlanc BH, Gillanders W, Rozenfeld Y, Bonin K. Team-based care approach to cholesterol management in diabetes mellitus: two-year cluster randomized controlled trial. Arch Intern Med 2011;171:1480-1486. ArticlePubMed
- 26. Yu-Poth S, Zhao G, Etherton T, Naglak M, Jonnalagadda S, Kris-Etherton PM. Effects of the National Cholesterol Education Program's Step I and Step II dietary intervention programs on cardiovascular disease risk factors: a meta-analysis. Am J Clin Nutr 1999;69:632-646. ArticlePubMed
- 27. D'Agostino RB Sr, Grundy S, Sullivan LM, Wilson P. CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA 2001;286:180-187. ArticlePubMed
REFERENCES

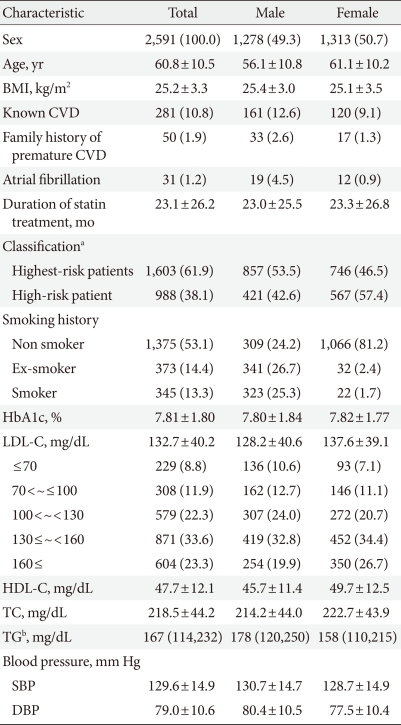
Values are presented as mean±standard deviation or number (%).
BMI, body mass index; CVD, cardiovascular disease; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; SBP, systolic blood pressure; DBP, diastolic blood pressure.
aClassification of CVD risk according to ADA/ACC consensus, bMedian, interquartile values.
Figure & Data
References
Citations
- Lipid Management in Korean People With Type 2 Diabetes Mellitus: Korean Diabetes Association and Korean Society of Lipid and Atherosclerosis Consensus Statement
Ye Seul Yang, Hack-Lyoung Kim, Sang-Hyun Kim, Min Kyong Moon
Journal of Lipid and Atherosclerosis.2023; 12(1): 12. CrossRef - Lipid Management in Korean People with Type 2 Diabetes Mellitus: Korean Diabetes Association and Korean Society of Lipid and Atherosclerosis Consensus Statement
Ye Seul Yang, Hack-Lyoung Kim, Sang-Hyun Kim, Min Kyong Moon
Diabetes & Metabolism Journal.2023; 47(1): 1. CrossRef - Impact of physician's perception about LDL cholesterol control in clinical practice when treating patients in Spain
Juan Cosín-Sales, Raquel Campuzano Ruiz, José Luis Díaz Díaz, Carlos Escobar Cervantes, María Rosa Fernández Olmo, Juan José Gómez-Doblas, José María Mostaza, Juan Pedro-Botet, Núria Plana Gil, Pedro Valdivielso
Atherosclerosis.2023; 375: 38. CrossRef - Current Status of Low-Density Lipoprotein Cholesterol Target Achievement in Patients with Type 2 Diabetes Mellitus in Korea Compared with Recent Guidelines
Soo Jin Yun, In-Kyung Jeong, Jin-Hye Cha, Juneyoung Lee, Ho Chan Cho, Sung Hee Choi, SungWan Chun, Hyun Jeong Jeon, Ho-Cheol Kang, Sang Soo Kim, Seung-Hyun Ko, Gwanpyo Koh, Su Kyoung Kwon, Jae Hyuk Lee, Min Kyong Moon, Junghyun Noh, Cheol-Young Park, Sung
Diabetes & Metabolism Journal.2022; 46(3): 464. CrossRef - Lipid-lowering treatment intensity, persistence, adherence and goal attainment in patients with coronary heart disease
Faizan Mazhar, Paul Hjemdahl, Catherine M Clase, Kristina Johnell, Tomas Jernberg, Juan Jesus Carrero
American Heart Journal.2022; 251: 78. CrossRef - Evaluation of efficacy and safety of combined rosuvastatin and atorvastatin in treating with coronary heart disease
Ke Li, Meng-Meng Liu, Xin Yang, Li Chen, Hui Geng, Wei Luo, Jie Ma
Medicine.2021; 100(24): e26340. CrossRef - Achievement of LDL-C Targets Defined by ESC/EAS (2011) Guidelines in Risk-Stratified Korean Patients with Dyslipidemia Receiving Lipid-Modifying Treatments
Ye Seul Yang, Seo Young Lee, Jung-Sun Kim, Kyung Mook Choi, Kang Wook Lee, Sang-Chol Lee, Jung Rae Cho, Seung-Jin Oh, Ji-Hyun Kim, Sung Hee Choi
Endocrinology and Metabolism.2020; 35(2): 367. CrossRef - Low-density lipoprotein cholesterol goal attainment rates in high-risk patients with cardiovascular diseases and diabetes mellitus in Korea: a retrospective cohort study
Ye Seul Yang, Bo Ram Yang, Mi-Sook Kim, Yunji Hwang, Sung Hee Choi
Lipids in Health and Disease.2020;[Epub] CrossRef - Dyslipidemia and Rate of Under-Target Low-Density Lipoprotein-Cholesterol in Patients with Coronary Artery Disease in Korea
Sang-Hak Lee, Woo-Hyuk Song, Myung Ho Jeong, Seung-Ho Hur, Dong Woon Jeon, Wonju Jeung, Anselm K Gitt, Martin Horack, Ami Vyas, Dominik Lautsch, Baishali Ambegaonkar, Philippe Brudi, Yangsoo Jang
Journal of Lipid and Atherosclerosis.2019; 8(2): 242. CrossRef - Statin use and site-specific risk of colorectal cancer in individuals with hypercholesterolemia from the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS)
Jae-Woo Lee, Na-Young You, Yeseul Kim, Yonghwan Kim, Joungyoun Kim, Hee-Taik Kang
Nutrition, Metabolism and Cardiovascular Diseases.2019; 29(7): 701. CrossRef - Efficacy and safety of rosuvastatin versus atorvastatin in high-risk Chinese patients with hypercholesterolemia: a randomized, double-blind, active-controlled study
Shuiping Zhao, Daoquan Peng
Current Medical Research and Opinion.2018; 34(2): 227. CrossRef - Effect of physician characteristics and knowledge on the quality of dyslipidemia management and LDL–C target goal achievement in China: Subgroup analysis of the Dyslipidemia International Study
Rongjing Ding, Ping Ye, Shuiping Zhao, Dong Zhao, Xiaowei Yan, Yugang Dong, Jihu Li, Yuqin Ran, Dayi Hu
Journal of Global Health.2017;[Epub] CrossRef - Trends in the management levels of metabolic risk factors in middle-aged and elderly patients with type 2 diabetes mellitus: The Korean National Health and Nutrition Examination Survey 1998–2014
Sukyung Cho, Haeun Jang, Kyong Park, Stefan Kiechl
PLOS ONE.2017; 12(12): e0189361. CrossRef - Increased postprandial apolipoprotein B-48 level after a test meal in diabetic patients: A multicenter, cross-sectional study
Cheol-Young Park, Joong-Yeol Park, Jongwon Choi, Dae Jung Kim, Kyong Soo Park, Kun-Ho Yoon, Moon-Kyu Lee, Sung-Woo Park
Metabolism.2016; 65(6): 843. CrossRef - Physicians’ behavior following changes in LDL cholesterol target goals
Shlomo Vinker, Haim Bitterman, Doron Comaneshter, Arnon D Cohen
Israel Journal of Health Policy Research.2015;[Epub] CrossRef - Prevalence of dyslipidaemia in patients treated with lipid-lowering agents in China: Results of the DYSlipidemia International Study (DYSIS)
Shuiping Zhao, Yongjun Wang, Yiming Mu, Bilian Yu, Ping Ye, Xiaowei Yan, Zhanquan Li, Yidong Wei, Baishaili M. Ambegaonakr, Dayi Hu
Atherosclerosis.2014; 235(2): 463. CrossRef - First-line treatment patterns and lipid target levels attainment in very high cardiovascular risk outpatients
Ioanna Xanthopoulou, Periklis Davlouros, Simos Siahos, Angelos Perperis, Evangelia Zaharioglou, Dimitrios Alexopoulos
Lipids in Health and Disease.2013;[Epub] CrossRef - Statin Prescription Adhered to Guidelines for Patients Hospitalized due to Acute Ischemic Stroke or Transient Ischemic Attack
Keun-Sik Hong, Mi Sun Oh, Hye-Yeon Choi, A-Hyun Cho, Hyung-Min Kwon, Kyung-Ho Yu, Hee-Joon Bae, Juneyoung Lee, Byung-Chul Lee
Journal of Clinical Neurology.2013; 9(4): 214. CrossRef - LDL-cholesterol target values and actual values in patients with type 2 diabetes (T2D) uncontrolled on oral antidiabetic monotherapy: The lipid results of the French ESCALADE survey
Alfred Penfornis, Alain Baleydier, Thierry Clavel, Sylvie Picard
Annales d'Endocrinologie.2012; 73(6): 503. CrossRef - Clinical evaluation of the use of statins in diabetic dyslipidemia
김나영, 류재곤, 정효근, 백소영, 남상민
Journal of Korean Society of Health-System Pharmacists.2012; 29(3): 288. CrossRef
 PubReader
PubReader Cite
Cite- Figure
-


- Related articles
-
- Association between Low-Density Lipoprotein Cholesterol Level and Cardiovascular Outcomes in Korean Adults: A Nationwide Cohort Study
- Optimal Low-Density Lipoprotein Cholesterol Level for Primary Prevention in Koreans with Type 2 Diabetes Mellitus
- Current Status of Low-Density Lipoprotein Cholesterol Target Achievement in Patients with Type 2 Diabetes Mellitus in Korea Compared with Recent Guidelines



