
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(6); 2011 > Article
-
Original ArticleThe Relationship among Homocysteine, Bilirubin, and Diabetic Retinopathy
- Ho Chan Cho
-
Diabetes & Metabolism Journal 2011;35(6):595-601.
DOI: https://doi.org/10.4093/dmj.2011.35.6.595
Published online: December 26, 2011
Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea.
- Corresponding author: Ho Chan Cho. Department of Internal Medicine, Keimyung University Dongsan Medical Center, 56 Dalseong-ro, Jung-gu, Daegu 700-712, Korea. ho3632@kmu.ac.kr
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Diabetic retinopathy is a common microvascular complication of diabetes mellitus (DM) and the leading cause of blindness in adults. Homocysteine, a risk factor with toxic effects on vascular endothelial cells, and bilirubin, a protectant with antioxidant and anti-inflammatory properties on the vasculature, have been reported to be linked to vaso-occlusive disorders. Therefore, the author of the present study investigated the association between the levels of plasma homocysteine and serum total bilirubin and the incidence of diabetic retinopathy as a chronic microvascular complication in patients with type 2 diabetes mellitus (T2DM).
-
Methods
- A total of 102 patients with T2DM who visited our hospital from January 2009 to January 2010 were assessed.
-
Results
- Of the 102 patients, the prevalence of diabetic retinopathy was 67 cases (65.7%) according to clinical ophthalmic examination. The duration of DM (P<0.001), age (P=0.003), fasting blood glucose (P=0.045) and urine albumin-creatinine ratio (P=0.015) in univariate analysis and plasma homocysteine level (P=0.038), duration of DM (P=0.001), and total bilirubin level (P=0.012) in multiple logistic regression analysis were statistically significantly associated with the incidence of diabetic retinopathy.
-
Conclusion
- The present study indicates that homocysteine and bilirubin may be useful biomarkers for increased risk of diabetic retinopathy since retinopathy in patients with T2DM was linked to higher plasma homocysteine level and decreased serum total bilirubin level.
- The incidence of diabetes mellitus (DM) and its complications are increasing rapidly due to an aging population and the Westernization of life styles [1]. Diabetic retinopathy is a common microvascular complication that develops in the early period of DM and induces visual impairment and even blindness in adults. Thus early diagnosis and appropriate treatments are important [2]. Diabetic retinopathy is caused primarily by microvascular injury and the duration of DM, hyperglycemia, hypertension, and hyperlipidemia have been shown to be risk factors for diabetic retinopathy [3]. Recent studies have reported that homocysteine was linked to vaso-occlusive disorders in the eye and the level of plasma homocysteine may be a useful biomarker or a novel risk factor for increased risk of diabetic retinopathy in patients with type 2 diabetes mellitus (T2DM) [4,5]. Few studies exist on the relationship between bilirubin and microvasculopathy, such as diabetic retinopathy. However, bilirubin may exhibit strong antioxidant and anti-inflammatory properties on the vasculature [6,7]. Therefore, the authors of the present study suggest that bilirubin may have an endogenous protective effect on the retinal vasculature in patients with T2DM.
- In the present study, the association among the level of plasma homocysteine as a risk factor, serum total bilirubin as an endogenous protectant and the presence of diabetic retinopathy as a chronic common complication and peripheral microvascular disorder in patients with T2DM was investigated.
INTRODUCTION
- Study population
- The present study was conducted on 102 patients with T2DM who were confirmed with insulin secretion test in the Department of Internal Medicine and underwent fundoscopic examinations for the assessment of retinopathy in the Department of Ophthalmology in Daegu Medical Center from January 2009 to January 2010. Patients were excluded from the present study if they had a history of chronic alcohol drinking, hepatobiliary abnormalities, or any other acute disease. The patients with blood levels greater than three times the normal level of aminotransferase (AST) or alanine aminotransferase (ALT), or with problems in the evaluation of diabetic retinopathy due to other reasons were excluded. The present study was conducted under participant voluntary consent after explanation of the purpose, methods, and course.
- Study design and assessments
- A detailed questionnaire was completed for each of the 102 participating patients. Information obtained included age, gender, smoking history, history of alcohol consumption or hepatobiliary disorders, duration of DM, and history of hypertension or cardiovascular diseases. Additionally, height, waist circumference, blood pressure, fasting blood glucose (FBG), 2-hour postprandial blood glucose (2PPBG), C-peptide, and insulin levels were obtained. Fasting venous blood was drawn on the day of examination via a venipuncture from the patient's antecubital vein and baseline biochemical profiles including serum total bilirubin, AST, ALT, glycosylated hemoglobin (HbA1c), creatinine, C-reactive protein (CRP) and lipid profiles were analyzed using the ARCHITECT c8000 (Toshiba, Tokyo, Japan). The standard reference range of total bilirubin is 3.4 to 20.5 µmol/L. For plasma homocysteine measurement, blood samples were collected in tubes containing EDTA and plasma homocysteine concentrations were analyzed using a HITACHI 7600 (Hitachi, Tokyo, Japan). The standard reference range of plasma homocysteine is 5.0 to 15.0 µmol/L.
- All patients underwent full ophthalmologic examinations through dilated pupils including fundus with a binocular indirect ophthalmoscope (Keeler Instruments Inc., Broomall, PA, USA) and slit lamp biomicroscope using 90-diopter lens (Carl Zeiss, Jena, Germany). Diabetic retinopathy was clinically classified by an ophthalmologist as cases without diabetic retinopathy; proliferative diabetic retinopathy (PDR) with neovascularization, scars, vitreous hemorrhage, or retinal detachment; and non-proliferative diabetic retinopathy (NPDR) with increased capillary permeability, capillary obstruction and distention, microaneurysm formation, cotton wool spots, or hard exudate. Non-proliferative retinopathy was divided into mild, moderate and severe NPDR.
- Data analysis
- Statistical analysis was performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA) and the baseline characteristics of participants were presented as the mean±standard deviation and n (%). Data were compared using an independent-sample Student's t-test for continuous data, odds ratio (OR) and chi-square test for categorical variables, and the Mann-Whitney U test for nonparametric data with an irregular distribution. Multiple logistic regression analysis was performed to assess independent associations between the presence of key risk factors of diabetic retinopathy including statistically significant factors in univariate analysis and suggested biomarkers such as plasma homocysteine and total bilirubin levels. A P value less than 0.05 was considered statistically significant.
METHODS
- Baseline characteristics
- The baseline clinical and laboratory characteristics of the present study population are shown in Table 1. Among the participants, 54 were male and 48 were female, and the mean age was 59 years. The average duration of DM was 9.3 years. The laboratory data showed a mean HbA1c of 7.9%, FBG of 8.4 mmol/L, 2PPBG of 13.2 mmol/L, homocysteine of 18.3 µmol/L, and total bilirubin of 11.7 µmol/L.
- Clinical characteristics in patients with T2DM according to the incidence of retinopathy
- Characteristics of the participants according to the incidence of retinopathy are shown in Tables 2 and 3. The number of patients with diabetic retinopathy was 67 (65.7%; 62 cases of NPDR and 5 cases of PDR) and the number of patients without diabetic retinopathy was 35 (34.3%). As expected, the age of patients with diabetic retinopathy was significantly higher than that of patients without retinopathy (P<0.01) and patients with diabetic retinopathy had a significantly longer duration of DM, by 7.2 years on average (P<0.01) (Table 2). In addition, FBG of the retinopathy group was on average 8.7 mmol/L, and was significantly higher than the average of 7.7 mmol/L in the group without retinopathy (P<0.05). Total bilirubin was 10.1 µmol/L in the retinopathy group and 15.1 µmol/L in the group without retinopathy and the retinopathy group had significantly lower bilirubin levels (P<0.01). Urine albumin-creatinine ratio (ACR) was 4.3 in the retinopathy group and 0.7 in the group without retinopathy, with the diabetic retinopathy group showing significantly higher values (P<0.01). The level of plasma homocysteine in the group with retinopathy was an average of 19.2 µmol/L and it was higher in comparison with the average of 16.3 mmol/L in the group without retinopathy; however, the difference was not statistically significant (P>0.05) (Table 3). There were no significant differences between the two groups in gender, smoking, body mass index, blood pressure, waist to hip ratio, HbA1c, CRP, cholesterol concentrations, or renal function (Tables 2 and 3). There were no significant differences between the two groups in current medication except that the number of patients who took angiotensin II receptor blockers (ARBs) was higher in the group with retinopathy than in the group without retinopathy (49, 73.1% vs. 18, 51.4%, P<0.05).
- Independent risk factors for diabetic retinopathy
- To examine the independent associations between the key risk factors and the presence of diabetic retinopathy, a multiple logistic regression analysis was performed with the significant variables in univariate analysis including age, DM duration, FBG, total bilirubin, and urine ACR, with homocysteine as the biomarker as used in previous studies [4,5]. The analysis showed that variables independently associated with diabetic retinopathy were a longer duration of DM with an OR of 1.2 (95% confidence interval [CI], 1.1 to 1.4), homocysteine with an OR of 1.1 (95% CI, 1.0 to 1.1), and total bilirubin with an OR of 0.9 (95% CI, 0.7 to 1.0) (Table 4).
RESULTS
- Diabetic retinopathy is a common ophthalmic complication that occurs primarily in the microvasculature of the retina and has been estimated to account for 5% of all cases of global blindness [8]. Diabetic retinopathy is also known to be common in patients with newly diagnosed T2DM [9].
- The change in the retina of patients with DM includes formation of retinal capillary microaneurysms, increased vascular permeability, vascular occlusion, proliferation of new blood vessels, fibrosis of tissues in the surface of the retina and optic disk, and the contraction of fibrovascular proliferations and the vitreous [10]. Several hypotheses have been tested on the cause and pathogenesis of diabetic retinopathy. In non-proliferative retinopathy, prolonged hyperglycemia may produce microaneurysms because of the selective decrease of cells in the vicinity of the retinal microvasculature and may also induce thickening of the vascular fundus membrane, endothelial proliferation, microvascular dilatation due to decreased endothelin-1 synthesis, increased vascular permeability, and vascular occlusion in microvascular endothelial cells. In addition, prolonged hyperglycemia may increase blood flow and viscosity, resulting in an increase of shear stress against the vascular wall, as well as injury of the vascular wall, in severe cases, it is known to induce macular edema [11]. However, the main pathogenesis of proliferative retinopathy is known to be neovascularization caused by several factors including insulin-like growth factor released from a retinal ischemic area [11].
- Recently, four biochemical pathways including enhanced glucose flux through the polyol pathway, increased intracellular formation of advanced glycation end-products, activation of protein kinase C isoforms, and stimulation of the hexosamine pathway have been suggested for eye disorders caused by hyperglycemia-induced vascular injury in diabetes. These pathogenic mechanisms also appear to be associated with superoxide overproduction by the mitochondrial electron transport chain [12].
- A longer duration of diabetes appears to be the main risk factor for diabetic retinopathy, and aging, hyperglycemia, hyperlipidemia, proteinuria, severe obesity, early onset of diabetes, alcohol drinking, genetic factors, and various hormones including growth hormone have been reported as additional risk factors for diabetic retinopathy [13-16]. Similarly, the present study showed that a longer duration of DM and aging in the group with retinopathy were statistically significant risk factors for diabetic retinopathy in comparison to the group without retinopathy (Table 2). In addition, high FBG level and high urine ACR appear to be significant risk factors for diabetic retinopathy, and total bilirubin level is inversely associated with the incidence of diabetic retinopathy (Table 3). Regarding medications, there were more patients taking ARBs in the group with retinopathy, which may be due to the medication being used as preventative treatment for a relatively high ACR. A longer duration of diabetes was statistically significantly associated with diabetic retinopathy not only in univariate analysis but also in logistic regression analysis, and thus it was also confirmed to be an independent risk factor in the present study (Tables 2 and 4).
- Based on the results from the present study, the author suggest that plasma homocysteine and serum total bilirubin can be used as biomarkers of diabetic retinopathy. Homocysteine is an amino acid containing a sulfur group produced during the metabolism of methionine. Dietary methionine is converted to S-adenosyl methionine, and then demethylated to S-adenosyl homocysteine, which is hydrolyzed to homocysteine and adenosine [17]. The level of total plasma homocysteine varies widely depending on age, gender, genetics, geographic and environmental factors. In particular, homocysteine may be increased primarily in hereditary diseases and with deficiencies of folic acid and vitamins B12 and B6, which are required for homocysteine metabolism [18,19]. Recent studies have shown that homocysteine is associated with an increased risk of chronic vascular complications of diabetes including coronary artery diseases, stroke, and peripheral arterial diseases, and these mechanisms can be explained by direct toxic effects on vascular endothelial cells and an indirect effect on normal methylation in endothelial cells [17,20]. In particular, hyperhomocysteinemia causes toxic effects on vascular endothelial cells directly or indirectly through the impairment of vascular endothelial cells, promotion of platelet activation, enhanced coagulability, generation of reactive oxygen species with cellular toxicity, decreased antioxidant actions, and vascular smooth muscle cell proliferation [19,21-24]. Recent studies have reported that elevated homocysteine level may be associated with the onset of retinopathy as a chronic microvascular complication of diabetes [3-5,25]; however, the results were not confirmed and the issue remains controversial [17, 20,26]. In the present study, the levels of plasma homocysteine in the group with retinopathy were higher in comparison to those in the group without retinopathy in univariate analysis, although statistical significance was not shown (Table 3). Homocysteine level was added to the key factor list in univariate analysis for multiple logistic regression analysis since several previous studies have reported homocysteine level as a novel biomarker of diabetic retinopathy [3,4]. The homocysteine level was independently associated with diabetic retinopathy with an OR of 1.1 according to multiple logistic regression analysis (Table 4). Consequently, homocysteine level may be a useful biomarker for increased risk of diabetic retinopathy.
- Bilirubin is the metabolic end-product of heme degradation and is considered a toxic substance with adverse effects such as jaundice [27]. However, recent reports have suggested that bilirubin may exert anti-atherosclerotic effects through antioxidant actions [7], anti-inflammatory effects on the vasculature [28,29], and cytoprotectant properties [30]. These properties are explained by the mechanism of bilirubin inhibition of inflammatory cytokine-induced endothelial cell expression of vascular cell adhesion molecules [28], inhibition of transmigration of monocytes [31], prevention of the oxidation of low density lipoprotein [32], inhibition of inflammation and dysfunction of endothelial cells [29], inhibition of proliferation of vascular smooth muscles [33], as well as prevention of the formation of thrombi [7,34]. Notably, oxidative stress has been implicated in the pathogenesis of microvascular and macrovascular complications of diabetes [35]. A direct pathological connection of serum bilirubin with microvascular disorders has not been fully established. However, higher serum levels of bilirubin are inversely associated with the incidence of not only macrovascular diseases, such as coronary arterial disease [36-38], but also peripheral arterial disease through the anti-atherogenic and antioxidant properties of bilirubin [7]. Recently published studies have suggested that elevated serum bilirubin may provide protection from coronary microvascular dysfunction and coronary flow reserve impairment by improving microvascular integrity [39,40]. In the present study, the correlation between levels of serum total bilirubin and diabetic retinopathy as a chronic microvascular complication was investigated. The results showed an inverse association of bilirubin level with retinopathy not only in univariate but also multiple logistic regression analysis (Tables 3 and 4), which indicates that bilirubin may be an important biomarker of diabetic retinopathy as an endogenous protectant from microvascular complications due to antioxidant and anti-inflammatory properties.
- There were several limitations in the present study. First, examinations of dietary deficiencies of folic acid and vitamins involved in homocysteine metabolism were not performed. Second, testing for anti-hepatitis C virus or performing an ultrasonogram on the hepatobiliary system which may determine the bilirubin level, was not conducted in the present study. Third, the study was cross-sectional in a small group, and thus additional long term prospective studies are needed in a larger population.
- In summary, including homocysteine and bilirubin levels in predictions of diabetic retinopathy may be clinically useful since retinopathy in patients with T2DM was linked to higher plasma homocysteine level and decreased serum total bilirubin level in the present study. Additional studies are necessary to confirm these results and evaluate related mechanisms.
DISCUSSION
-
Acknowledgements
- The present research has been conducted by the Bisa Research Grant of Keimyung University in 2011.
ACKNOWLEDGMENTS
- 1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047-1053. ArticlePubMedPDF
- 2. Axer-Siegel R, Herscovici Z, Gabbay M, Mimouni K, Weinberger D, Gabbay U. The relationship between diabetic retinopathy, glycemic control, risk factor indicators and patient education. Isr Med Assoc J 2006;8:523-526. PubMed
- 3. Nguyen TT, Alibrahim E, Islam FM, Klein R, Klein BE, Cotch MF, Shea S, Wong TY. Inflammatory, hemostatic, and other novel biomarkers for diabetic retinopathy: the multi-ethnic study of atherosclerosis. Diabetes Care 2009;32:1704-1709. PubMedPMC
- 4. Brazionis L, Rowley K Sr, Itsiopoulos C, Harper CA, O'Dea K. Homocysteine and diabetic retinopathy. Diabetes Care 2008;31:50-56. ArticlePubMedPDF
- 5. Huang EJ, Kuo WW, Chen YJ, Chen TH, Chang MH, Lu MC, Tzang BS, Hsu HH, Huang CY, Lee SD. Homocysteine and other biochemical parameters in type 2 diabetes mellitus with different diabetic duration or diabetic retinopathy. Clin Chim Acta 2006;366:293-298. ArticlePubMed
- 6. Dekker D, Dorresteijn MJ, Pijnenburg M, Heemskerk S, Rasing-Hoogveld A, Burger DM, Wagener FA, Smits P. The bilirubin-increasing drug atazanavir improves endothelial function in patients with type 2 diabetes mellitus. Arterioscler Thromb Vasc Biol 2011;31:458-463. ArticlePubMed
- 7. Stocker R, Yamamoto Y, McDonagh AF, Glazer AN, Ames BN. Bilirubin is an antioxidant of possible physiological importance. Science 1987;235:1043-1046. ArticlePubMed
- 8. Chaturvedi N. The burden of diabetes and its complications: trends and implications for intervention. Diabetes Res Clin Pract 2007;76(Suppl 1):S3-S12. ArticlePubMed
- 9. Kohner EM, Aldington SJ, Stratton IM, Manley SE, Holman RR, Matthews DR, Turner RC. United Kingdom Prospective Diabetes Study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol 1998;116:297-303. ArticlePubMed
- 10. Rema M, Pradeepa R. Diabetic retinopathy: an Indian perspective. Indian J Med Res 2007;125:297-310. PubMed
- 11. Kim TW. Pathogenesis of diabetic retinopathy. J Korean Diabetes Assoc 1997;21:115-121.
- 12. Brownlee M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001;414:813-820. ArticlePubMedPDF
- 13. Choi CY, Lee JY, Kim JM, Park KH, Rhee EJ. Quantitative analysis of aqueous flare in diabetic patients. J Korean Ophthalmol Soc 2008;49:1954-1960.Article
- 14. Jin JH, Lee SJ, Lee HS, Kim SD. Prognostic factors of visual acuity in diabetes mellitus. J Korean Ophthalmol Soc 2006;47:755-762.
- 15. Kim HK, Oh TS, Lee SM, Lee JB. The initial fundus examination and severity of diabetic retinopathy at a primary eye clinic. J Korean Ophthalmol Soc 2005;46:982-988.
- 16. Seo WT, Song SO, Kim SY, Choi YS, Jang HR, Lee SJ. The risk factors of diabetic retinopathy in NIDDM patients. J Korean Diabetes Assoc 1999;23:162-171.
- 17. Yucel I, Yucel G, Muftuoglu F. Plasma homocysteine levels in noninsulin-dependent diabetes mellitus with retinopathy and neovascular glaucoma. Int Ophthalmol 2004;25:201-205. ArticlePubMedPDF
- 18. Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl J Med 1998;338:1042-1050. ArticlePubMed
- 19. Selhub J, Jacques PF, Wilson PW, Rush D, Rosenberg IH. Vitamin status and intake as primary determinants of homocysteinemia in an elderly population. JAMA 1993;270:2693-2698. ArticlePubMed
- 20. de Luis DA, Fernandez N, Arranz ML, Aller R, Izaola O, Romero E. Total homocysteine levels relation with chronic complications of diabetes, body composition, and other cardiovascular risk factors in a population of patients with diabetes mellitus type 2. J Diabetes Complications 2005;19:42-46. ArticlePubMed
- 21. Schreiner PJ, Wu KK, Malinow MR, Stinson VL, Szklo M, Nieto FJ, Heiss G. Hyperhomocyst(e)inemia and hemostatic factors: the atherosclerosis risk in communities study. Ann Epidemiol 2002;12:228-236. PubMed
- 22. Heinecke JW, Rosen H, Suzuki LA, Chait A. The role of sulfur-containing amino acids in superoxide production and modification of low density lipoprotein by arterial smooth muscle cells. J Biol Chem 1987;262:10098-10103. ArticlePubMed
- 23. Upchurch GR Jr, Welch GN, Fabian AJ, Freedman JE, Johnson JL, Keaney JF Jr, Loscalzo J. Homocyst(e)ine decreases bioavailable nitric oxide by a mechanism involving glutathione peroxidase. J Biol Chem 1997;272:17012-17017. ArticlePubMed
- 24. Tsai JC, Perrella MA, Yoshizumi M, Hsieh CM, Haber E, Schlegel R, Lee ME. Promotion of vascular smooth muscle cell growth by homocysteine: a link to atherosclerosis. Proc Natl Acad Sci U S A 1994;91:6369-6373. ArticlePubMedPMC
- 25. Goldstein M, Leibovitch I, Yeffimov I, Gavendo S, Sela BA, Loewenstein A. Hyperhomocysteinemia in patients with diabetes mellitus with and without diabetic retinopathy. Eye (Lond) 2004;18:460-465. ArticlePubMedPDF
- 26. Agardh CD, Agardh E, Andersson A, Hultberg B. Lack of association between plasma homocysteine levels and microangiopathy in type 1 diabetes mellitus. Scand J Clin Lab Invest 1994;54:637-641. ArticlePubMed
- 27. Perlstein TS, Pande RL, Beckman JA, Creager MA. Serum total bilirubin level and prevalent lower-extremity peripheral arterial disease: National Health and Nutrition Examination Survey (NHANES) 1999 to 2004. Arterioscler Thromb Vasc Biol 2008;28:166-172. PubMed
- 28. Pae HO, Oh GS, Lee BS, Rim JS, Kim YM, Chung HT. 3-Hydroxyanthranilic acid, one of L-tryptophan metabolites, inhibits monocyte chemoattractant protein-1 secretion and vascular cell adhesion molecule-1 expression via heme oxygenase-1 induction in human umbilical vein endothelial cells. Atherosclerosis 2006;187:274-284. ArticlePubMed
- 29. Kawamura K, Ishikawa K, Wada Y, Kimura S, Matsumoto H, Kohro T, Itabe H, Kodama T, Maruyama Y. Bilirubin from heme oxygenase-1 attenuates vascular endothelial activation and dysfunction. Arterioscler Thromb Vasc Biol 2005;25:155-160. ArticlePubMed
- 30. Baranano DE, Rao M, Ferris CD, Snyder SH. Biliverdin reductase: a major physiologic cytoprotectant. Proc Natl Acad Sci U S A 2002;99:16093-16098. ArticlePubMedPMC
- 31. Ishikawa K, Navab M, Leitinger N, Fogelman AM, Lusis AJ. Induction of heme oxygenase-1 inhibits the monocyte transmigration induced by mildly oxidized LDL. J Clin Invest 1997;100:1209-1216. ArticlePubMedPMC
- 32. Neuzil J, Stocker R. Free and albumin-bound bilirubin are efficient co-antioxidants for alpha-tocopherol, inhibiting plasma and low density lipoprotein lipid peroxidation. J Biol Chem 1994;269:16712-16719. ArticlePubMed
- 33. Ollinger R, Bilban M, Erat A, Froio A, McDaid J, Tyagi S, Csizmadia E, Graca-Souza AV, Liloia A, Soares MP, Otterbein LE, Usheva A, Yamashita K, Bach FH. Bilirubin: a natural inhibitor of vascular smooth muscle cell proliferation. Circulation 2005;112:1030-1039. ArticlePubMed
- 34. Lindenblatt N, Bordel R, Schareck W, Menger MD, Vollmar B. Vascular heme oxygenase-1 induction suppresses microvascular thrombus formation in vivo. Arterioscler Thromb Vasc Biol 2004;24:601-606. ArticlePubMed
- 35. Yeh SY, Doupis J, Rahangdale S, Horr S, Malhotra A, Veves A. Total serum bilirubin does not affect vascular reactivity in patients with diabetes. Vasc Med 2009;14:129-136. ArticlePubMedPMCPDF
- 36. Moon JS, Chang WJ, Lee CH, Lee JE, Chun KA, Yoon JS, Cho IH, Lee HW, Won KC. Relationship between serum bilirubin levels and coronary atherosclerosis in patients with type 2 diabetes. Korean Diabetes J 2008;32:338-345.Article
- 37. Schwertner HA, Jackson WG, Tolan G. Association of low serum concentration of bilirubin with increased risk of coronary artery disease. Clin Chem 1994;40:18-23. ArticlePubMedPDF
- 38. Hopkins PN, Wu LL, Hunt SC, James BC, Vincent GM, Williams RR. Higher serum bilirubin is associated with decreased risk for early familial coronary artery disease. Arterioscler Thromb Vasc Biol 1996;16:250-255. ArticlePubMed
- 39. Gullu H, Erdogan D, Tok D, Topcu S, Caliskan M, Ulus T, Muderrisoglu H. High serum bilirubin concentrations preserve coronary flow reserve and coronary microvascular functions. Arterioscler Thromb Vasc Biol 2005;25:2289-2294. ArticlePubMed
- 40. Choi UJ, Yoon MH, Choi SY, Lim HS, Yang HM, Woo SI, Hwang JW, Kang SJ, Choi BJ, Hwang GS, Shin JH, Park JS, Park SJ, Lee YH, Lee YS, Tahk SJ. Correlation between the serum bilirubin level and the coronary microvascular integrity in diabetic patients. Korean Circ J 2008;38:425-431.Article
REFERENCES

Values are presented as mean±standard deviation or median (min-max).
BMI, body mass index; DM, diabetes mellitus; CVA, cerebrovascular accident; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, glycosylated hemoglobin; FBG, fasting blood glucose; 2PPBG, 2-hour postprandial glucose; HDL-C, high density lipoprotein cholesterol; AST, aminotransferase; ALT, alanine aminotransferase; CRP, C-reactive protein; ACR, albumin-creatinine ratio.

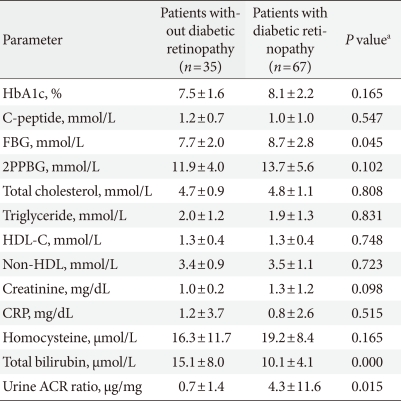
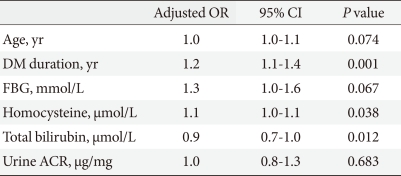
Figure & Data
References
Citations
- Role of hyperhomocysteinemia in the progression of diabetic retinopathy
Pooja H V, Lakshmi M S
Indian Journal of Clinical and Experimental Ophthalmology.2024; 10(1): 160. CrossRef - Plasma homocysteine is associated with nonproliferative retinopathy in patients with type 2 diabetes without renal disease
Martina Tomić, Romano Vrabec, Spomenka Ljubić, Tomislav Bulum, Dario Rahelić
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2022; 16(1): 102355. CrossRef - Blood Viscosity in Subjects With Type 2 Diabetes Mellitus: Roles of Hyperglycemia and Elevated Plasma Fibrinogen
Jiehui Sun, Keqin Han, Miao Xu, Lujuan Li, Jin Qian, Li Li, Xuejin Li
Frontiers in Physiology.2022;[Epub] CrossRef - Biliverdin/Bilirubin Redox Pair Protects Lens Epithelial Cells against Oxidative Stress in Age-Related Cataract by Regulating NF-κB/iNOS and Nrf2/HO-1 Pathways
Yang Huang, Jinglan Li, Wenzhe Li, Nanping Ai, Haiying Jin, Recep Liman
Oxidative Medicine and Cellular Longevity.2022; 2022: 1. CrossRef - Homocysteine and diabetes: Role in macrovascular and microvascular complications
Emir Muzurović, Ivana Kraljević, Mirsala Solak, Siniša Dragnić, Dimitri P. Mikhailidis
Journal of Diabetes and its Complications.2021; 35(3): 107834. CrossRef - Quantifying Fibrinogen-Dependent Aggregation of Red Blood Cells in Type 2 Diabetes Mellitus
Yixiang Deng, Dimitrios P. Papageorgiou, Xuejin Li, Nikolaos Perakakis, Christos S. Mantzoros, Ming Dao, George Em Karniadakis
Biophysical Journal.2020; 119(5): 900. CrossRef - Effect of folic acid supplementation on nerve conduction velocity in diabetic polyneuropathy patients
Tayebeh Mottaghi, Fariborz Khorvash, Mohammadreza Maracy, Nick Bellissimo, Gholamreza Askari
Neurological Research.2019; 41(4): 364. CrossRef - Association between serum total bilirubin levels and the risk of type 2 diabetes mellitus
Min Yang, Changlin Ni, Baocheng Chang, Zhenhuan Jiang, Yanjuan Zhu, Yunzhao Tang, Zhu Li, Chenguang Li, Bin Li
Diabetes Research and Clinical Practice.2019; 152: 23. CrossRef - Elevated Serum Total Bilirubin Concentrations Are Negatively Associated with Diabetic Retinopathy among the Chinese Northeastern Population
Dan Zhang, Wei Zhang, Shi Jin, Wei Wang, Dan Guo, Lu Wang
International Journal of Endocrinology.2018; 2018: 1. CrossRef - Serum bilirubin levels are negatively associated with diabetic retinopathy in patients with type 1 diabetes and normal renal function
Tomislav Bulum, Martina Tomić, Lea Duvnjak
International Ophthalmology.2018; 38(3): 1095. CrossRef - The Association between Serum Bilirubin Level and Electrochemical Skin Conductance in Chinese Patients with Type 2 Diabetes
Fei Mao, Xiaoming Zhu, Bin Lu, Yiming Li
International Journal of Endocrinology.2018; 2018: 1. CrossRef - Evaluation of kidney function and risk factors of retinopathy in Type 2 diabetes mellitus people in South Africa
F.A. Ganjifrockwala, J.T. Joseph, G. George
Diabetes Research and Clinical Practice.2017; 127: 218. CrossRef - Homocysteine and Its Relationship to Asymptomatic Carotid Stenosis in a Chinese Community Population
Jiaokun Jia, Anxin Wang, Jing Wang, Jianwei Wu, Xiujuan Yan, Yong Zhou, Shengyun Chen, Xingquan Zhao
Scientific Reports.2016;[Epub] CrossRef - A Novel Perspective on the Biology of Bilirubin in Health and Disease
Silvia Gazzin, Libor Vitek, Jon Watchko, Steven M. Shapiro, Claudio Tiribelli
Trends in Molecular Medicine.2016; 22(9): 758. CrossRef - The Negative Relationship between Bilirubin Level and Diabetic Retinopathy: A Meta-Analysis
Bo Zhu, Xiaomei Wu, Kang Ning, Feng Jiang, Lu Zhang, Demetrios G. Vavvas
PLOS ONE.2016; 11(8): e0161649. CrossRef - Circulating Biomarkers of Diabetic Retinopathy: An Overview Based on Physiopathology
Olga Simó-Servat, Rafael Simó, Cristina Hernández
Journal of Diabetes Research.2016; 2016: 1. CrossRef - Serum total bilirubin concentration is negatively associated with increasing severity of retinopathy in patients with type 2 diabetes mellitus
Risa Sekioka, Masami Tanaka, Takeshi Nishimura, Hiroshi Itoh
Journal of Diabetes and its Complications.2015; 29(2): 218. CrossRef - Plasma Homocysteine is Associated with Retinopathy in Type 1 Diabetic Patients in the Absence of Nephropathy
Tomislav Bulum, Kristina Blaslov, Lea Duvnjak
Seminars in Ophthalmology.2014; : 1. CrossRef - Relationship between homocysteine level and diabetic retinopathy: a systematic review and meta-analysis
Chong Xu, Yan Wu, Guodong Liu, Xiaoqiang Liu, Fang Wang, Jing Yu
Diagnostic Pathology.2014;[Epub] CrossRef - Alterations of Retinal Vasculature in Cystathionine–β-Synthase Heterozygous Mice
Amany Tawfik, Shanu Markand, Mohamed Al-Shabrawey, Jamie N. Mayo, Jason Reynolds, Shawn E. Bearden, Vadivel Ganapathy, Sylvia B. Smith
The American Journal of Pathology.2014; 184(9): 2573. CrossRef - Decreased Serum Bilirubin Is Associated With Silent Cerebral Infarction
Rui-Yan Li, Zhi-Gang Cao, Ji-Rong Zhang, Ying Li, Rui-Tao Wang
Arteriosclerosis, Thrombosis, and Vascular Biology.2014; 34(4): 946. CrossRef - Role of bile pigments in critical care medicine
Atsunori Nakao, Keisuke Kohama, Taihei Yamada, Noritomo Fujisaki, Norichika Yoshie, Takahiro Ueda, Takeshi Nishimura, Joji Kotani
Nihon Kyukyu Igakukai Zasshi.2014; 25(6): 239. CrossRef - Serum total bilirubin levels and prevalence of diabetic retinopathy in a Chinese population (中国人群血清总胆红素水平与糖尿病视网膜病变相关性的研究)
Syeda Sadia Najam, Jichao Sun, Jie Zhang, Min Xu, Jieli Lu, Kan Sun, Mian Li, Tiange Wang, Yufang Bi, Guang Ning
Journal of Diabetes.2014; 6(3): 221. CrossRef - Omentin changes following bariatric surgery and predictive links with biomarkers for risk of cardiovascular disease
Marc Lapointe, Paul Poirier, Julie Martin, Marjorie Bastien, Audrey Auclair, Katherine Cianflone
Cardiovascular Diabetology.2014;[Epub] CrossRef - Homocysteine Serum Levels in Diabetic Patients with Non Proliferative, Proliferative and without Retinopathy
Giulia Malaguarnera, Caterina Gagliano, Maria Giordano, Salvatore Salomone, Marco Vacante, Claudio Bucolo, Filippo Caraci, Michele Reibaldi, Filippo Drago, Teresio Avitabile, Massimo Motta
BioMed Research International.2014; 2014: 1. CrossRef - Mechanisms of Diabetic Complications
Josephine M. Forbes, Mark E. Cooper
Physiological Reviews.2013; 93(1): 137. CrossRef
 PubReader
PubReader Cite
Cite


