Efficacy and Safety of Omega-3 Fatty Acids in Patients Treated with Statins for Residual Hypertriglyceridemia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial
Article information
 , In-Kyung Jeong1,*, Jae Myung Yu2, Sung Rae Kim3, In Kye Lee4, Kyung-Ah Han5, Sung Hee Choi6, Soo-Kyung Kim7, Hyeong Kyu Park8, Ji-Oh Mok9, Yong-ho Lee10, Hyuk-Sang Kwon11, So Hun Kim12, Ho-Cheol Kang13, Sang Ah Lee14, Chang Beom Lee15, Kyung Mook Choi16, Sung-Ho Her17, Won Yong Shin18, Mi-Seung Shin19, Hyo-Suk Ahn20, Seung Ho Kang21, Jin-Man Cho22, Sang-Ho Jo23, Tae-Joon Cha24, Seok Yeon Kim25, Kyung Heon Won25, Dong-Bin Kim26, Jae Hyuk Lee27, Moon-Kyu Lee28
, In-Kyung Jeong1,*, Jae Myung Yu2, Sung Rae Kim3, In Kye Lee4, Kyung-Ah Han5, Sung Hee Choi6, Soo-Kyung Kim7, Hyeong Kyu Park8, Ji-Oh Mok9, Yong-ho Lee10, Hyuk-Sang Kwon11, So Hun Kim12, Ho-Cheol Kang13, Sang Ah Lee14, Chang Beom Lee15, Kyung Mook Choi16, Sung-Ho Her17, Won Yong Shin18, Mi-Seung Shin19, Hyo-Suk Ahn20, Seung Ho Kang21, Jin-Man Cho22, Sang-Ho Jo23, Tae-Joon Cha24, Seok Yeon Kim25, Kyung Heon Won25, Dong-Bin Kim26, Jae Hyuk Lee27, Moon-Kyu Lee28
Abstract
Background
Cardiovascular risk remains increased despite optimal low density lipoprotein cholesterol (LDL-C) level induced by intensive statin therapy. Therefore, recent guidelines recommend non-high density lipoprotein cholesterol (non-HDL-C) as a secondary target for preventing cardiovascular events. The aim of this study was to assess the efficacy and tolerability of omega-3 fatty acids (OM3-FAs) in combination with atorvastatin compared to atorvastatin alone in patients with mixed dyslipidemia.
Methods
This randomized, double-blind, placebo-controlled, parallel-group, and phase III multicenter study included adults with fasting triglyceride (TG) levels ≥200 and <500 mg/dL and LDL-C levels <110 mg/dL. Eligible subjects were randomized to ATOMEGA (OM3-FAs 4,000 mg plus atorvastatin calcium 20 mg) or atorvastatin 20 mg plus placebo groups. The primary efficacy endpoints were the percent changes in TG and non-HDL-C levels from baseline at the end of treatment.
Results
After 8 weeks of treatment, the percent changes from baseline in TG (−29.8% vs. 3.6%, P<0.001) and non-HDL-C (−10.1% vs. 4.9%, P<0.001) levels were significantly greater in the ATOMEGA group (n=97) than in the atorvastatin group (n=103). Moreover, the proportion of total subjects reaching TG target of <200 mg/dL in the ATOMEGA group was significantly higher than that in the atorvastatin group (62.9% vs. 22.3%, P<0.001). The incidence of adverse events did not differ between the two groups.
Conclusion
The addition of OM3-FAs to atorvastatin improved TG and non-HDL-C levels to a significant extent compared to atorvastatin alone in subjects with residual hypertriglyceridemia.
INTRODUCTION
Elevated low-density lipoprotein cholesterol (LDL-C) is one of the major cardiovascular risk factors, and remains a primary target in lipid lowering therapy. Statins have been proven to be the most effective medication to reduce LDL-C level and to further prevent cardiovascular disease (CVD). However, additional cardiovascular risk factors beyond LDL-C should be addressed, because a significant residual CVD risk was detected in patients achieving optimal LDL-C level by intensive statin therapy [1].
As a modifiable cardiovascular risk factor, hypertriglyceridemia is recently emerging as a reliable therapeutic target especially in Korea, where the prevalence of hypertriglyceridemia is greater than that of hypercholesterolemia [2]. Recent evidence supports an independent association of triglyceride (TG) level with CVD after adjustment for conventional risk factors and high-density lipoprotein cholesterol (HDL-C) level [34]. Elevated TG level over 5 years increased the incidence of coronary heart disease (CHD), regardless of baseline TG level [4]. Among hospitalized patients with acute coronary syndrome, those with TG level >150 mg/dL and LDL-C level <70 mg/dL exhibited a 15% higher CHD event rate than those with low TG level and high LDL-C level [5]. Particularly in patients with type 2 diabetes mellitus (DM), two large trials demonstrated that a combination of statins with TG-lowering medication reduced CVD events in a subgroup of subjects with marked hypertriglyceridemia and low HDL-C level [67].
Therefore, recent guidelines emphasized the importance of non-HDL-C as a secondary target for preventing CVD in patients with mixed dyslipidemia who achieved LDL-C target [8910]. Thus, TG-lowering therapy might be beneficial as an add-on to statin treatment in patients with well-controlled LDL-C, but high TG level. Among several treatment options to control the hypertriglyceridemia, omega-3 fatty acids (OM3-FAs) induced a greater reduction of TG and were associated with few adverse effects when added to statins [111213]. Thus, this phase III study was designed to assess the efficacy and tolerability of OM3-FAs 4,000 mg/day in combination with atorvastatin 20 mg/day in patients with persistent hypertriglyceridemia at high risk for CVD despite statin use, compared to atorvastatin 20 mg/day alone.
METHODS
Study design and procedures
This 8-week randomized, double-blind, placebo-controlled, parallel-group, and phase III multicenter study was conducted at 36 centers throughout Korea between May 4, 2016 and May 16, 2017. Adult subjects aged 20 to 79 years with high CVD risk according to the Korean dyslipidemia guideline [9] were screened at the first visit. Participants were selected according to the following criteria: (1) fasting TG level ≥300 mg/dL with LDL-C level ≥100 mg/dL and <160 mg/dL for the subjects who were not taking statins for the last 4 weeks; (2) fasting TG level ≥200 mg/dL and <500 mg/dL with LDL-C level <110 mg/dL for the subjects who were taking statins for the last 4 weeks; and (3) non-smoking during the study period.
These subjects underwent a 4-week run-in period of open label atorvastatin 20 mg/day, and were scheduled for the second screening. The participants who were taking 20 mg/day of atorvastatin over 4 weeks could visit for the second screening without a run-in period (Fig. 1). To be eligible for the second screening, the subjects should meet the following criteria: (1) residual hypertriglyceridemia with fasting TG level ≥200 mg/dL and <500 mg/dL with LDL-C level <110 mg/dL; (2) decreased LDL-C level during the run-in period compared to that at the first screening, if subjects were not taking statins previously; and (3) an adherence rate of ≥80% for statin during the run-in period. All participants received dietary counseling for dyslipidemia based on the Korean dyslipidemia guideline during their screening visit [9]. The following exclusion criteria were applied: (1) a history of unstable angina, acute myocardial infarction (MI), coronary artery revascularization, including coronary artery bypass surgery, or transient ischemic attack or stroke 3 months prior to screening; (2) a history of operation for aortic aneurysm within 6 months prior to screening; (3) symptoms of unexplained myalgia or a diagnosis of myalgia or rhabdomyolysis at screening; (4) a history of pancreatitis prior to screening; (5) significant comorbid medical illness in cardiovascular, hepatobiliary, neuropsychiatric, endocrine system that posed difficulties in continuing clinical trial and interpreting test results; (6) a history of positive antibody to Human Immunodeficiency Virus (HIV)-1 or positive HIV test result; (7) a history of malignant tumor within 2 years, except for complete resolution of basal cell or squamous cell carcinoma; (8) the use of prohibited concomitant medications; (9) sex hormone replacement or use of oral contraceptives 2 months prior to screening or during clinical trial; (10) uncontrolled hypertension (systolic blood pressure [BP] ≥180 mm Hg and/or diastolic BP ≥110 mm Hg); (11) serum creatinine level ≥2 times the upper limit of normal; (12) alanine aminotransferase (ALT) and/or aspartate aminotransferase levels ≥3 times the upper limit of normal; (13) creatine phosphokinase level five times the upper limit of normal; (14) a genetic disorder, including galactose intolerance, Lapp lactase deficiency, or galactose malabsorption; (15) allergy or hypersensitivity to the study medications; (16) drug or alcohol abuse within 2 years prior to screening; (17) pregnancy or breast-feeding at screening; (18) possible pregnancy or planning to be pregnant during clinical trial; (19) inclusion in another clinical trial 1 month prior to screening; (20) other conditions that were not appropriate for clinical trial. Finally, eligible subjects were randomly assigned in a 1:1 ratio to each of two groups (ATOMEGA or atorvastatin group) for 8 weeks. Individuals in the ATOMEGA group were prescribed four capsules of ATOMEGA that contained OM3-FAs 1,000 mg plus atorvastatin calcium 5 mg and one tablet of placebo of atorvastatin 20 mg. The individuals in the atorvastatin group were prescribed four capsules of placebo (olive oil 1,000 mg) and one tablet of atorvastatin calcium 20 mg (Fig. 1).
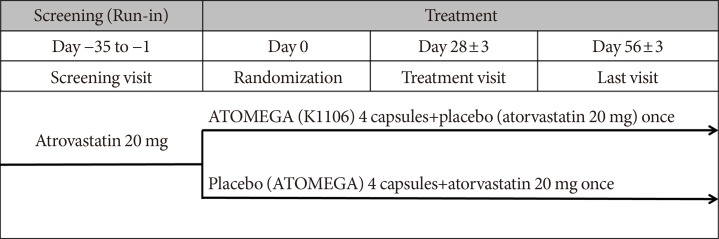
Study design. Adult subjects with high cardiovascular disease risk were screened, and eligible subjects underwent a 4-week run-in period of open label atorvastatin 20 mg/day, and were scheduled for a second screening. Enrolled subjects were randomly assigned in a 1:1 ratio to each of the two groups (ATOMEGA group or atorvastatin group) for 8 weeks of treatment. Individuals in ATOMEGA group were prescribed four capsules of ATOMEGA containing omega-3 fatty acids 1,000 mg plus atorvastatin calcium 5 mg and one tablet of placebo of atorvastatin 20 mg/day. Individuals in the atorvastatin group were prescribed four capsules of placebo (olive oil 1,000 mg) and one tablet of atorvastatin calcium 20 mg.
Study subjects
Among the 558 screened subjects, 268 subjects entered the run-in period, and 215 subjects were randomly assigned to the treatment groups (105 subjects to the ATOMEGA group and 110 subjects to the atorvastatin group). From the randomized population, eight subjects in the ATOMEGA group and seven subjects in the atorvastatin group were excluded from safety set due to violation of eligibility criteria or incomplete measurement of TG or non-HDL-C level. Finally, 200 subjects (97 subjects in the ATOMEGA group and 103 subjects in the atorvastatin group) were included in full analysis set population for evaluating the efficacy endpoints (Supplementary Fig. 1).
Study endpoints
The primary efficacy endpoints were the percentage changes in TG and non-HDL-C levels from baseline after 8 weeks of treatment. The secondary efficacy endpoints included the percentage changes in other lipid parameters, such as total cholesterol (TC), HDL-C, very low density lipoprotein cholesterol (VLDL-C), apolipoprotein (Apo) A–I, and Apo B, from baseline to the end of the treatment. Lipid samples, including LDL-C, were measured by the laboratories of each hospital using standard procedures.
Safety was assessed by monitoring adverse events (AEs), laboratory parameters, electrocardiograms, and vital signs, in addition to physical examinations. AEs were defined as occurred, worsened, or became serious during the study period, and included all unintended consequences of the individual receiving treatment, regardless of the causality. AEs were categorized as definitely related, probably related, possibly related, probably not related, definitely not related, and with unknown relationship to the study drug.
Definitions
Hypertension was defined as systolic BP/diastolic BP ≥140/90 mm Hg and/or a previous diagnosis of hypertension in the self-report. DM was defined as fasting plasma glucose (FPG) level ≥126 mg/dL, hemoglobin A1c (HbA1c) ≥6.5%, and/or previous diagnosis of DM in the self-report. A 10-year CHD risk was estimated by the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) Framingham risk score [14]. The categories of age, sex, TC, HDL-C, smoking status, systolic BP, and antihypertensive medication use were considered and calculated using a downloadable spreadsheet calculator.
Statistical analyses
A previous study calculated that a sample size of 214 patients (107 patients in each treatment group) has 90% power to detect a difference of 7.9% (treatment group) and 1.5% (control group) in mean percent change in non-LDL-C at week 8 of treatment with 5% two-sided significance level, assuming a common standard deviation of 14.4% (treatment group) and 11.2% (control group) in patients having an evaluable primary endpoint [11].
Continuous variables were presented as mean±standard deviation (SD) if normally distributed, or as median (25th to 75th percentile) if not normally distributed. The comparison of the two groups was performed by using t-test or Mann-Whitney U test. The outcomes of the two groups were compared according to several subgroups. Categorical variables were expressed as numbers and percentages, and analyzed by chi-square test. Univariate and multivariate linear regression analyses were performed to detect clinical factors associated with greater effect of OM3-FAs in lowering TG and non-HDL-C levels.
The intention-to-treat population included all randomized patients. Efficacy analyses involved full analysis set population who received at least one dose of the study drug and provided at least one post-randomized blood sample. The last observation carried forward method was used to impute missing non-baseline data for patients who did not complete the treatment period. Safety analyses were performed in the safety set population who received at least one dose of double-blind study drug and underwent at least one safety assessment after randomization. The chi-square test was used to compare the incidence of AEs between the two groups.
Ethical approval and consent to participate
All procedures involving human participants performed in this study were in accordance with the ethical standards of the relevant institutional and/or national research committees and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Institutional Review Board (IRB number: Appendix 1) or ethics committee at each participating center, and all patients provided written informed consent. This study was registered at ClinicalTrials.gov (NCT03482180).
RESULTS
Baseline characteristics
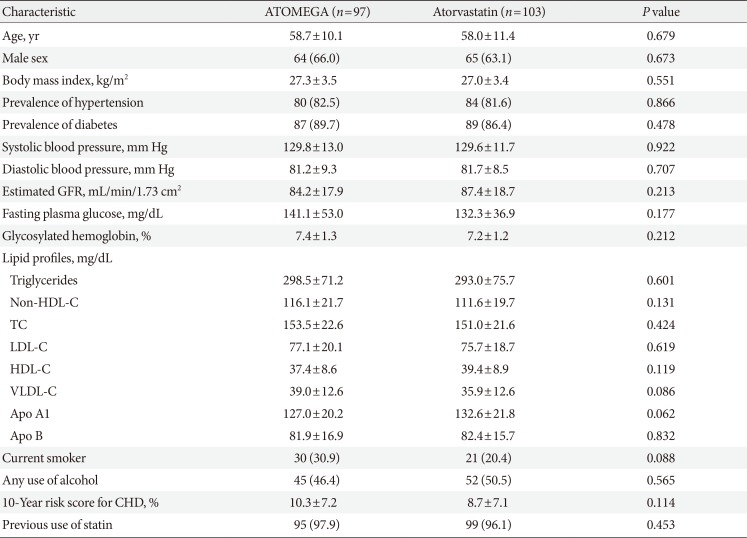
Baseline characteristics of the study subjects were generally similar, regardless of treatment allocation (Table 1). Enrolled subjects were middle-aged with a mean age of 58.3 years, obese with a mean body mass index (BMI) of 27.2 kg/m2, and with a high 10-year CHD risk score (mean 9.9%). The proportion of patients with DM were not different between the ATOMEGA and atorvastatin groups (89.7% vs. 86.4%, P=0.478). No significant differences in any variable, including baseline lipid parameters, were found between the two groups.

Baseline characteristics of the subjects
Changes in lipid and lipoprotein levels after 8 weeks of treatment
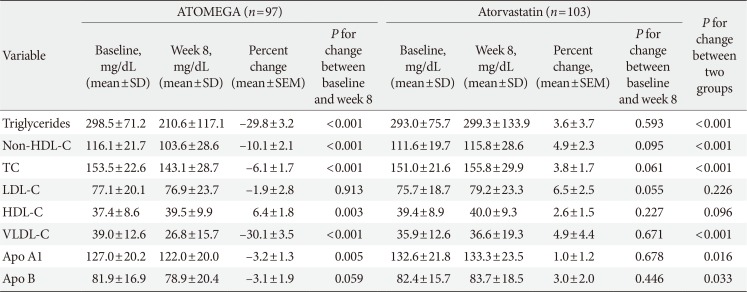
ATOMEGA group achieved significant reductions in TG and non-HDL-C levels after the 8-week treatment compared to baseline, while atorvastatin group showed no change in TG level and a slight increase in non-HDL-C level (Table 2). Percent changes in TG (−29.8% vs. 3.6%, P<0.001) and non-HDL-C level (−10.1% vs. 4.9%, P<0.001) were significantly decreased in the ATOMEGA group than in the atorvastatin group (Table 2, Fig. 2).

Lipid parameters at baseline and 8 weeks after treatment
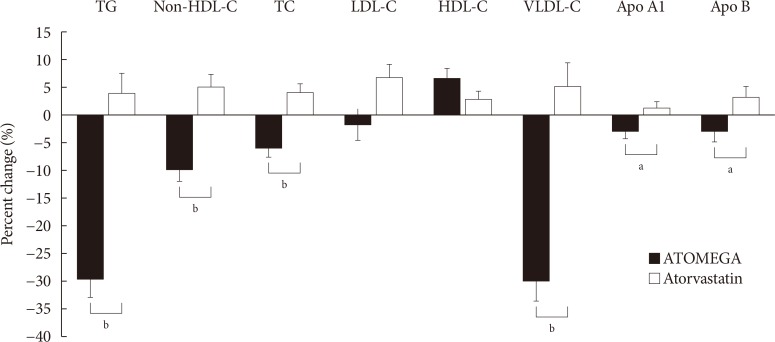
Percent change in lipid parameters from baseline after 8 weeks of treatment. Black bar represents the change in lipid parameters in the ATOMEGA group, while white vertical rectangle represents the change in lipid parameters in the atorvastatin group. TG, triglyceride; HDL-C, high density lipoprotein cholesterol; TC, total cholesterol; LDL-C, low density lipoprotein cholesterol; VLDL-C, very low density lipoprotein cholesterol; Apo A, apolipoprotein A; Apo B, apolipoprotein B. aP<0.05, bP<0.001 for the difference between ATOMEGA and atorvastatin group.
Among other lipid parameters, significant decreases in TC, VLDL-C, Apo A1, and Apo B levels in addition to a significant increase in HDL-C level were detected in the ATOMEGA group after 8 weeks of treatment compared to baseline (Table 2). Moreover, the decreases in TC, VLDL-C, Apo A1, and Apo B levels were significantly greater in the ATOMEGA group than in the atorvastatin group. However, the percent change in LDL-C and HDL-C levels after 8 weeks of treatment did not show a significant difference between the two groups (Table 2, Fig. 2). In addition, the proportion of total subjects reaching TG target of <200 mg/dL after treatment was significantly higher in the ATOMEGA group than in the atorvastatin group (62.9% vs. 22.3%, P<0.001) (Supplementary Fig. 2A), and it remained higher in the ATOMEGA group, both in men and in women (Supplementary Fig. 2B).
Changes in FPG and HbA1c levels after 8 weeks of treatment
The percent change in FPG level and HbA1c after 8 weeks of treatment did not differ between ATOMEGA group (n=95) and atorvastatin group (n=96) (Supplementary Table 1). No difference in FPG and HbA1c levels between baseline and after 8 weeks of treatment was found within each group, regardless of DM presence.
Subgroup analysis for the efficacy of ATOMEGA
In subgroup analysis comparing percent changes in TG and non-HDL-C levels according to age (≥65 years vs. <65 years), sex (male vs. female), BMI (≥25 kg/m2 vs. <25 kg/m2), presence of hypertension, presence of DM, estimated glomerular filtrationrate (eGFR) (≥60 mL/min/1.73 m2 vs. <60 mL/min/1.73 m2), and 10-year CHD risk (≥10% vs. <10%), ATOMEGA showed greater lowering effects on both TG and non-HDL-C levels after 8 weeks of treatment than atorvastatin in each subgroup, except in subjects without DM (Fig. 3). Both ATOMEGA and atorvastatin decreased TG (−16.9%±41.6% vs. −14.0%±30.6%, P=0.847) and non-HDL-C levels (−1.3%±30.0% vs. −7.1%±13.1%, P=0.524) with a similar extent in subjects without DM (Fig. 3). However, only ATOMEGA significantly reduced TG (−31.3%±29.8%) and non-HDL-C levels (−11.1%±19.6%) in subjects with DM after 8 weeks of treatment, while atorvastatin slightly increased TG (6.4%±38.0%) and non-HDL-C levels (6.7%±23.9%) compared to baseline (Fig. 3).

Comparison of triglyceride (TG) and non-high density lipoprotein cholesterol (non-HDL-C) lowering efficacy between ATOMEGA group (black bar) and atorvastatin group (white bar) in various subgroups. BMI, body mass index; eGFR, estimated glomerular filtration rate; CHD, coronary heart disease. aP<0.05, bP<0.01, cP<0.001 for the difference between the two groups.
Clinical factors affecting reduction in TG or non-HDL-C concentration by adding OM3-FAs
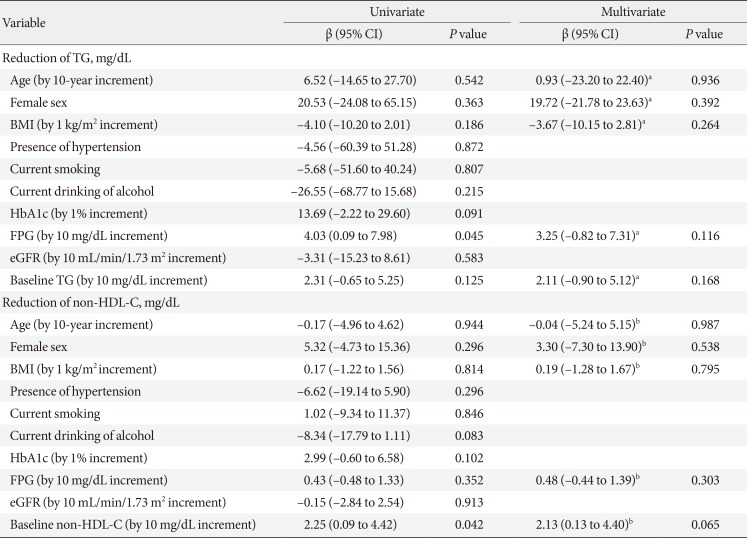
In univariate linear regression analysis, only higher FPG level was significantly associated with a reduction in TG level (β=4.03, P=0.045). However, this modest association disappeared after adjustment for age, sex, BMI, and baseline TG level in multivariate linear regression analysis (Table 3). Conversely, only higher baseline non-HDL-C level was positively associated with a reduction in non-HDL-C level in the univariate model (β=2.25, P=0.042); however, this association also lost statistical significance after adjustment for age, sex, BMI, and FPG level (Table 3).

Clinical factors affecting reduction in triglycerides or non-HDL-C concentration by adding omega-3 fatty acid
Safety analyses
The proportion of AEs (15.2% vs. 11.8%, P=0.463) and serious AEs (1.9% vs. 0.9%, P=0.615) did not differ between the ATOMEGA and atorvastatin groups (Supplementary Table 2). Two serious AEs in the ATOMEGA group were upper limb fracture (n=1, 0.95%) and hyperglycemia (n=1, 0.95%). Serum ALT level of the ATOMEGA group was significantly higher than that of the atorvastatin group, but was within the normal reference range. A mild increase in creatine phosphokinase level (less than three times the upper limit of the normal range) was only observed in the atorvastatin group (P=0.024) and was reported as adverse drug reaction.
DISCUSSION
This study demonstrated that the combination of OM3-FAs 4,000 mg/day and atorvastatin 20 mg/day in patients with residual hypertriglyceridemia resulted in significantly greater decreases in TG and non-HDL-C levels, compared to atorvastatin 20 mg/day monotherapy. These prominent TG and non-HDL-C lowering effects in ATOMEGA group were consistent regardless of age, sex, BMI, presence of hypertension, eGFR, and CHD risk. However, a greater decrease in TG and non-HDL-C levels in the ATOMEGA group was only found in subjects with DM. Finally, no significant differences in the incidence and profile of AEs were observed between the ATOMEGA and atorvastatin groups.
The residual risk of atherosclerotic cardiovascular disease (ASCVD) remains high despite statin treatment, and the presence of hypertriglyceridemia was found to be a potent predictor for residual ASCVD risk, even in the subjects with LDL-C <100 mg/dL [15]. This is related to the less robust effects of statins on TG and cholesterol carried by TG-rich lipoproteins, such as VLDL, intermediate density lipoproteins, and chylomicrons [16]. Achieved non-HDL-C (<100 mg/dL) and TG (<200 mg/dL) levels were found to modulate plaque progression-regression rates in patients with achieved LDL-C level <70 mg/dL [17]. Although potential effect of TG-lowering treatment on CVD risk showed mixed results [9], a meta-analysis of 14 statin trials suggested that the relative CHD risk decreases by approximately 1% for every 1% reduction in non-HDL-C level [18]. Therefore, many recent guidelines recommended non-HDL-C as the secondary target for preventing CVD in patients with mixed dyslipidemia who achieved LDL-C target goal [8910].
Randomized controlled trials on OM3-FAs as monotherapy or as an adjunct to statin therapy supported the efficacy of OM3-FAs for reducing TG or non-HDL-C levels in individuals with hypertriglyceridemia or mixed dyslipidemia [11121920212223]. Similar to our results, Combination of Prescription Omega-3 with Simvastatin (COMBOS) study demonstrated that the reduction in TG (−29.5% vs. −6.3%) and non-HDL-C (−9.0% vs. −2.2%) levels were significantly greater in subjects that received 4,000 mg/day of OM3-FAs in addition to 40 mg/day of simvastatin, compared to simvastatin alone [11]. Moreover, a combination of 4,000 mg/day of OM3-FAs and 20 mg/day of rosuvastatin had a greater reduction in TG (−26.3% vs. −11.4%) and non-HDL-C (−10.7% vs. −2.2%) levels after 8 weeks of treatment compared to rosuvastatin alone [12]. However, contrary to our data, TG-lowering efficacy was significant regardless of DM presence, while non-HDL-C level was significantly decreased only in subjects with DM when OM3-FAs was added to statin in the aforementioned study on rosuvastatin [12]. In this study, TG and non-HDL-C lowering effects were more evident in subjects with DM compared to those without, when OM3-FAs were added to atorvastatin. While both combination therapy and atorvastatin alone reduced TG and non-HDL-C levels in subjects without DM, only the combination therapy was effective for lowering them in subjects with DM. This finding suggested that the additional TG-lowering treatment might be needed to reduce TG and non-HDL-C levels in subjects with DM.
As a possible explanation, diabetic dyslipidemia is characterized by high TG and decreased HDL-C levels even before the onset of clinically relevant hyperglycemia [24], and a higher baseline TG or non-HDL-C level is more likely to be decreased by treatment [12]. In fact, a higher FPG level was positively associated with TG reduction, and a higher baseline non-HDL-C level was positively associated with non-HDL-C reduction in this study. Another explanation can be that the effect of OM3-FAs might be associated with the improvement of insulin resistance. The OM3-FA treatment increased insulin sensitivity in subjects with polycystic ovary syndrome [25], non-alcoholic fatty liver disease [26], and type 2 DM [27]. The mechanism of this effect of OM3-FAs on the insulin resistance has been suggested to be the OM3-FA-induced modulation of mitochondrial biogenesis and endoplasmic reticulum stress in order to reduce reactive oxygen species production and activation of inflammatory pathways [28], rather than direct regulation of body weight or hyperglycemia [29]. Therefore, the prominent TG and non-HDL-C lowering effects in patients with DM from our study were possibly mediated by the improvement of insulin resistance. However, the parameters of insulin resistance could not be analyzed due to the lack of insulin data.
The proposed TG-lowering mechanisms of OM3-FAs were reduced hepatic production of TG-rich VLDL particles and increased rate of conversion of VLDL to LDL particles [30], while atorvastatin was found to decrease VLDL-TG concentration by increasing VLDL-TG fractional catabolic rate [20]. Since statins affect lipid metabolism primarily by inhibiting the cholesterol biosynthesis, which in turn increases the number of hepatic Apo B receptors, the clearance of all Apo B-containing LDL and VLDL is accelerated when OM3-FAs are co-administrated [31]. Beyond the additive effect on TG lowering, some evidence suggests a synergetic effect of OM3-FAs and statin treatment on the metabolic profiles, since a combination of eicosapentaenoic acid (EPA) and lovastatin enhanced the regulatory effects on the gene expression of 3-hydroxy-3-methylglutaryl coenzyme A reductase and LDL receptor in the HepG2 cell line [32]. EPA potentiates peroxisome proliferator activated receptor-alpha effect, and consequently decreases hepatic lipogenesis [33]. Docosahexaenoic acid (DHA) not only enhances VLDL lipolysis, resulting in a greater conversion to LDL, but also increases the levels of HDL-C and larger, more buoyant LDL particles [33]. A combination of pitavastatin, which has a potent anti-inflammatory effect, and EPA, which has a potent suppressive effect on vascular smooth muscle cell activation, compensates their weak effectiveness on plaque formation, and synergistically produces a favorable effect on atherosclerosis [34].
Although adding OM3-FAs to statin leads to significant reductions in TG and non-HDL-C levels, the primary and secondary prevention trials of combination therapy have generally show mixed effects on CVD [35]. The Japan EPA Lipid Intervention Study (JELIS) found that Japanese patients who received both EPA and a statin had a significantly reduced risk of CVD, which was a composite of sudden cardiac death, MI, unstable angina, and coronary revascularization, compared to those treated with statin alone [36]. Reduction of Cardiovascular Events with Icosapent Ethyl–Intervention Trial (REDUCE-IT) revealed that 4,000 mg/day of icosapent ethyl prevented a composite event of cardiovascular death, nonfatal MI, nonfatal stroke, coronary revascularization, or unstable angina in patients with established CVD or with diabetes and other risk factors, who had been receiving statin therapy [37]. Early initiation of EPA (1,800 mg/day) with pitavastatin within 24-hour after percutaneous coronary intervention reduced cardiovascular events occurring within 1 year, including death from a cardiovascular cause, nonfatal stroke, nonfatal MI, and revascularization [38]. In contrast, an additional amount of OM3-FAs did not affect the secondary prevention in statin users with previous MI compared to non-users [39]. Potential explanations for these discrepant results might be the differences across the studies, such as the composition and dosage of OM3-FAs, duration of supplement administration, follow-up duration, study population, concurrent CVD treatment, and baseline TG levels.
Several limitations of this study should be acknowledged. First, this study mostly included middle-aged Asians with relatively high CVD risk who needed statins. Therefore, it is difficult to extrapolate the current results to general population. Second, this study only demonstrated the short-term effect of adding OM3-FAs on lipid parameters. Furthermore, we could not investigate the association between these improvements in TG or non-HDL-C and future CVD prevention. Finally, TG and non-HDL-C lowering effects of adding OM3-FAs were more significant in subjects with DM, compared to subjects without DM. These differences were at some extent caused by the diabetic dyslipidemia characterized by high TG and non-HDL-C levels, but could be also caused by the amelioration of insulin resistance which could not be assessed in this study, or by the small number of subjects without DM.
In conclusion, over 8 weeks of treatment, 4,000 mg/day of OM3-FAs, when added to atorvastatin, significantly reduced TG and non-HDL-C levels compared with atorvastatin alone in subjects with well-controlled LDL-C levels and residual hypertriglyceridemia. Particularly, in a post hoc analysis, the combination therapy conferred additional benefits to lowering TG and non-HDL-C levels in patients with DM. To prove clinical evidence of a reduction of cardiovascular events with a combination of high dose OM3-FAs and statin, more studies are needed to elucidate the association between the improvement of residual dyslipidemia and actual CVD prevention.
Notes
CONFLICTS OF INTEREST: This work was financially supported by the Kuhnil Pharmaceutical Co., Ltd. (Seoul, Republic of Korea). The company funder had no role in the study design, in the collection, analysis, and interpretation of data, in the writing of the manuscript, and in the decision to submit the article for publication.
AUTHOR CONTRIBUTIONS:
Conception or design: I.K.J., M.K.L.
Data acquisition: I.K.J., S.R.K., I.K.L., K.A.H., S.H.C., S.K.K., H.K.P., J.O.M., Y.L., H.S.K., S.H.K., H.C.K., S.A.L., C.B.L., K.M.C., S.H.H., W.Y.S., M.S.S., H.S.A., S.H.K., J.M.C., S.H.J., T.J.C., S.Y.K., K.H.W., D.B.K., J.H.L., M.K.L.
Analysis, or interpretation of data: J.E.J., I.K.J.
Drafting the work or revising: J.E.J., I.K.J.
Final approval of the manuscript: M.K.L.
Appendix
Appendix 1
List of IRB number
References
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2018.0265.
Supplementary Table 1
Glycemic parameters at baseline and 8 weeks after treatment
Supplementary Table 2
Adverse events in study groups
Supplementary Fig. 1
Flow chart of inclusion and exclusion of study subjects. FAS, full analysis set.
Supplementary Fig. 2
The proportions (%) of study subjects achieving triglyceride <200 mg/dL after 8 weeks of treatment in ATOMEGA group (black bar) and atorvastatin group (white bar). (A) The proportions in total subjects (n=200). (B) The proportions according to sex category (n=129 in male subjects and n=71 in female subjects). aP<0.001 for the difference between the two groups.