
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 44(3); 2020 > Article
-
ReviewGuideline/Fact Sheet Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus: A Position Statement of the Fatty Liver Research Group of the Korean Diabetes Association
-
Byung-Wan Lee1
 , Yong-ho Lee1, Cheol-Young Park2, Eun-Jung Rhee2, Won-Young Lee2, Nan-Hee Kim3, Kyung Mook Choi3, Keun-Gyu Park4, Yeon-Kyung Choi4, Bong-Soo Cha1, Dae Ho Lee5, on Behalf of The Korean Diabetes Association (KDA) Fatty Liver Research Group
, Yong-ho Lee1, Cheol-Young Park2, Eun-Jung Rhee2, Won-Young Lee2, Nan-Hee Kim3, Kyung Mook Choi3, Keun-Gyu Park4, Yeon-Kyung Choi4, Bong-Soo Cha1, Dae Ho Lee5, on Behalf of The Korean Diabetes Association (KDA) Fatty Liver Research Group -
Diabetes & Metabolism Journal 2020;44(3):382-401.
DOI: https://doi.org/10.4093/dmj.2020.0010
Published online: May 11, 2020
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
4Division of Endocrinology and Metabolism, Department of Internal Medicine, School of Medicine, Kyungpook National University, Daegu, Korea.
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Gachon University Gil Medical Center, Gachon University College of Medicine, Incheon, Korea.
- Corresponding author: Bong-Soo Cha. Division of Endocrinology and Metabolism, Department of Internal Medicine, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. bscha@yuhs.ac
- Corresponding author: Dae Ho Lee. Division of Endocrinology and Metabolism, Department of Internal Medicine, Gachon University Gil Medical Center, Gachon University College of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea. drhormone@naver.com
Copyright © 2020 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- This clinical practice position statement, a product of the Fatty Liver Research Group of the Korean Diabetes Association, proposes recommendations for the diagnosis, progression and/or severity assessment, management, and follow-up of non-alcoholic fatty liver disease (NAFLD) in patients with type 2 diabetes mellitus (T2DM). Patients with both T2DM and NAFLD have an increased risk of non-alcoholic steatohepatitis (NASH) and fibrosis and a higher risk of cardiovascular diseases and diabetic complications compared to those without NAFLD. With regards to the evaluation of patients with T2DM and NAFLD, ultrasonography-based stepwise approaches using noninvasive biomarker models such as fibrosis-4 or the NAFLD fibrosis score as well as imaging studies such as vibration-controlled transient elastography with controlled attenuation parameter or magnetic resonance imaging-proton density fat fraction are recommended. After the diagnosis of NAFLD, the stage of fibrosis needs to be assessed appropriately. For management, weight reduction achieved by lifestyle modification has proven beneficial and is recommended in combination with antidiabetic agent(s). Evidence that some antidiabetic agents improve NAFLD/NASH with fibrosis in patients with T2DM is emerging. However, there are currently no definite pharmacologic treatments for NAFLD in patients with T2DM. For specific cases, bariatric surgery may be an option if indicated.
- This clinical practice position statement, a product of the Fatty Liver Research Group (FLRG) of the Korean Diabetes Association (KDA), proposes recommendations for the diagnosis, progression and/or severity assessment, management, and follow-up of non-alcoholic fatty liver disease (NAFLD) in patients with type 2 diabetes mellitus (T2DM). The literature was retrieved by an extensive PubMed search up to April 2019. After extensive reviews and discussions for the last 3 years by the research group, two sentinel reviews were published in Diabetes and Metabolism Journal in 2019. The draft of the statement was presented and discussed in a session of the FLRG during the 32nd KDA scientific meeting in 2019. Then, the statement was further discussed, edited and updated until the final acceptance of the statement in the journal. Epidemiological evidence suggests a strong bidirectional relationship between type 2 diabetes mellitus (T2DM) and non-alcoholic fatty liver disease (NAFLD), including the development and severity of NAFLD, progression to non-alcoholic steatohepatitis (NASH), and advanced fibrosis, independent of liver enzymes [1]. Furthermore, the coexistence of T2DM and NAFLD results in an unfavorable metabolic profile and an increasing cardiovascular (CV) risk [234]. Although steatosis can be defined by various clinically available diagnostic tools, it can be numerically and strictly defined by assessing liver fat: ≥5% of fat-containing hepatocytes in histology; proton density fat fraction (PDFF) ≥5% on magnetic resonance imaging (MRI), or >5.5% on proton magnetic resonance spectroscopy (1H-MRS) [56]. The definitive diagnosis of NASH requires a liver biopsy.
- Among many treatments for NAFLD in patients with T2DM, weight reduction is the only approved option for NAFLD. However, it is not easy to maintain weight loss by only lifestyle modification strategies, so additional pharmacological options should be supported. To date, although many drugs have been investigated, pioglitazone could be the first-line therapy in patients with T2DM and NAFLD. Many drugs are currently being developed and investigated, and combination strategies will be introduced for the treatment of NAFLD and diabetes in the future.
INTRODUCTION
- Keynotes
- -The prevalence of NAFLD in patients with T2DM is more than two times higher than that in the normal population.
- -NAFLD is a risk factor for T2DM.
- NAFLD is the most common liver disorder, affecting 20% to 40% of adults; the prevalence rates differ according to the diagnostic method, age, sex, and ethnicity [678]. In patients with T2DM, NAFLD prevalence ranges from 70% to 95%; the rate is extremely high, up to 98%, in patients with morbid obesity [8]. In the general Korean population, NAFLD prevalence ranges from 16.1% to 25.2% (Table 1) [910].
- Half of patients with T2DM have NAFLD despite having normal alanine aminotransferase (ALT) levels [1112]. Population based studies have reported the prevalence of NASH to be 17.6% to 22%% in individuals with T2DM and 3.7% in nondiabetic individuals [13]. Furthermore, the prevalence of NASH among biopsied patients with diabetes can be as high as 64.0%, whereas the prevalence of advanced fibrosis (≥F3) in patients with T2DM is approximately 10.4% [14]. The NAFLD prevalence in Asians is not lower than that in Caucasians. In a study involving Korean patients with T2DM who were subjected to ultrasonography (US) examination in a university-based diabetes clinic, 63.3% of patients had NAFLD (Table 1) [11121315161718].
- Furthermore, the risk of diabetes in subjects with NAFLD has been shown to be 2-fold higher than that in control subjects, even after adjustment for various risk factors [1920]. When obesity, insulin resistance, or hyperglycemia is combined with NAFLD, T2DM risk is dramatically increased [2]. In line with these studies, the resolution of steatosis in patients with NAFLD decreases T2DM risk by 39% to 82% [2122].
PREVALENCE OF NAFLD IN PATIENTS WITH T2DM
- Keynotes
- -Patients with T2DM and NAFLD have an increased risk of NASH and fibrosis.
- -Patients with both T2DM and NAFLD have a higher risk of CV diseases and diabetic complications compared to those without NAFLD.
- Approximately 10% to 35% of subjects with normal liver histology progress to steatosis, 12% to 44% of those with hepatic steatosis progress to steatohepatitis, and up to 15% of patients with NASH are known to progress to cirrhosis [23]. In patients with NAFLD, the prevalence of NASH is approximately 60% in biopsy-indicated patients and 29.9% in patients without such an indication [8]. Studies have shown that increasing age, diabetes, and hypertension are predictive clinical parameters for fibrosis [2425].
- NAFLD and NASH can progress to cirrhosis and liver failure in up to 15% of affected patients [26]. These patients are also at risk of developing hepatocellular carcinoma (HCC). Advanced age, high aspartate aminotransferase (AST) levels, thrombocytopenia (marker of progression of liver fibrosis), and diabetes were identified as risk factors for the development of HCC in Japanese patients with US-diagnosed NAFLD. Patients with NAFLD with advanced stages of fibrosis have a 7-fold higher risk of HCC compared to those without liver disease [27]. However, the cause of cirrhosis remains unclear in 30% of cases, and most of these cases are now considered NAFLD-related [28]. Cryptogenic cirrhosis was reported to be an underlying disease in approximately 7% of HCC cases in Korea and Japan compared with 13% in the United States [2829]. T2DM is also closely associated with progression to NASH, advanced fibrosis and the development of HCC [17].
- NAFLD is a consequence but also a precursor of metabolic comorbidities, including diabetes, dyslipidemia, and hypertension, and thus, NAFLD increases CV events, and mortality even in the absence of these comorbidities [30]. Furthermore, hepatic fibrosis is a key predictor of liver-related outcomes and is also associated with all-cause and CV mortality as well as mortality due to cirrhosis, HCC, and infectious diseases in NAFLD patients [3132]. Diabetes is an important factor affecting all-cause and CV mortality in patients with NAFLD [31]. Thus, after the diagnosis of NAFLD, the stage of fibrosis needs to be assessed appropriately [31]. There is evidence that the presence of NAFLD in patients with T2DM is associated with increased risks of macrovascular and diabetic microvascular complications as well as chronic kidney disease [2].
THE PROGRESSION OF NAFLD AND DIABETES
- Keynotes
- - NAFLD can be diagnosed by a two-step process: (1) confirmation of he-patic steatosis, either by imaging modalities or histology and (2) exclu-sion of secondary causes of liver steatosis.
- Routine screening for NAFLD in patients with T2DM is not currently recommended because of the unclear cost-effectiveness and uncertainties with diagnostic testing and treatments [33]. In individuals with and without diabetes, three important processes should be used to diagnose and assess NAFLD: (1) determine the existence of hepatic steatosis, either by imaging or histology; (2) exclude secondary causes of liver steatosis; and (3) assess NAFLD severity by establishing the presence of moderate-to-severe fibrosis (fibrosis stage of at least F2) [2]. Before making the diagnosis of NAFLD, secondary causes of hepatic fat accumulation and significant alcohol consumption (≥21 drinks/week for men and ≥14 drinks/week for women) need to be excluded [5]. Alcohol consumption over a 2-year time frame needs to be surveyed in detail using validated questionnaires [5]. However, it is noteworthy that there is also a synergy between alcohol intake and obesity or genetic risk factors of NAFLD progression for any given level of alcohol intake [6]. Even in patients whose alcohol consumption level is low, meeting the diagnostic criteria of NAFLD, small amounts of alcohol intake may affect outcomes in NAFLD, which warrants further study [534]. After performing a history and examination, the next investigations are to establish whether the patient has NAFLD or another liver condition.
- A consensus regarding initial blood tests for NAFLD has not been reached among guidelines [33]. The decision on the extent of liver blood tests and interpretation of the results should be determined in a clinical context. In adults, initial screening tests may include abdominal US, hepatitis B surface antigen, hepatitis C antibody (with follow-on polymerase chain reaction if positive), anti-mitochondrial antibody, anti-smooth muscle antibody, antinuclear antibody, serum immunoglobulins, and simultaneous serum ferritin and transferrin saturation [33]. Although ALT levels have been shown to be the best single biochemical correlate of hepatic steatosis, liver enzyme levels can be normal, fluctuating, or elevated in patients with NAFLD [23]. There have been suggestions that the current reference intervals for ALT may be too high [3536], and a recent guidance recommending an ALT of >30 U/L as being significant in males and >25 U/L significant for females [37].
- Noninvasive imaging studies to assess hepatic steatosis and hepatic fibrosis
- Keynotes
- - Despite its limited accuracy, US is a useful screening tool to detect hepatic steatosis with other possible structural abnormalities in patients who are suspected of having NAFLD.
- - Vibration-controlled transient elastography (VCTE) with controlled at-tenuation parameter (CAP) is a simple quantitative index to detect ste-atosis in clinical practice, but CAP values should be carefully interpreted with patient factors such as obesity.
- - As the MRI-PDFF is a highly reliable modality for detecting steatosis, comparable to liver biopsy, it is useful for sequent monitoring, such as in clinical trials.
- Currently, US, computed tomography (CT), MRI, 1H-MRS, and VCTE are available tools to measure NAFLD depending on the center or clinic (Table 2, Fig. 1).
- US is the recommended first line screening method for patients with T2DM by the European NAFLD guidelines [34]. US has interobserver variability and limited sensitivity to detect mild (<20%) steatosis [38], while optimum sensitivity for liver US was reported to be achieved at a liver fat content of ≥12.5% (sensitivity of approximately 80% to 85%) [3940].
- Similar to US, CT has limited sensitivity to detect mild steatosis (<30% liver fat). Radiation exposure is an additional drawback. Thus, CT scans cannot be recommended for the diagnosis of hepatic steatosis [2].
- VCTE measures the speed of a mechanically induced shear wave across the liver using pulse-echo ultrasonic acquisitions to obtain a liver stiffness measurement (LSM), as a marker of hepatic fibrosis, and ultrasonic attenuation through the liver to derive the CAP, as a marker of hepatic steatosis. VCTE is an easy-to-perform tool to obtain both LSM and CAP values using an M (3.5 MHz, at 2.5 to 6.5 cm-depth) or XL (2.5 MHz, at 3.5 to 7.5 cm-depth) ultrasound probe. Although LSM and CAP values are relatively reliable and well-validated, these parameters are affected by various patient factors, especially body mass index which may lead to an overestimation [4142]. With the availability of the XL probe, which has been proven for use in patients with morbid obesity, the failure rate of VCTE for obtaining the LSM and CAP values was reported to be less than 5%, while the significant disagreement between the first and second readings for LSM and CAP when obtained back to back was 18% and 11%, respectively [43].
- MRI-PDFF can provide fast, quantitative, accurate, and generalized hepatic fat measurements for the entire liver, thereby overcoming the heterogeneity of fat deposition [4445], while magnetic resonance elastography (MRE) is a useful diagnostic tool for the differentiation of histologically determined advanced liver fibrosis from non-advanced fibrosis [4647]. Additionally, LSM measured by MRE may reflect whole liver pathology rather than that of a very small area. MRI-PDFF is becoming the gold standard for hepatic steatosis quantification [48]. MRI-PDFF or 1H-MRS can measure liver fat more precisely than biopsy [4950]. In a secondary analysis of a clinical trial involving patients with biopsy-proven NASH, it was shown that histologic responders (≥2-point reduction in NAFLD activity score [NAS], without any worsening of fibrosis on liver biopsy) had a proportional reduction in the MRI-PDFF of 29.3% from baseline which was statistically significant when compared with histologic nonresponders [51]. However, at the present time, magnetic resonance techniques cannot be used for the assessment of NASH resolution or the exact assessment of fibrosis progression or improvement. Thus, these issues need to be addressed when designing future clinical trials.
- Liver biopsy
- Liver biopsy provides an accurate diagnosis in approximately 90% of patients with unexplained abnormalities revealed by liver function tests [52]. Noninvasive tools for fibrosis staging are not reliable for therapeutic or other decisions but may be helpful for excluding the probability of significant fibrosis and for predicting advanced fibrosis, thus guiding the decision to perform liver biopsy or not in a patient with NAFLD [53].
- Further studies are required to determine whether an active NASH screening strategy in patients with T2DM and active therapy on the basis of the currently available evidence are cost-effective and beneficial for long-term CV and liver-related outcomes. Health care providers taking care of patients with diabetes are strongly encouraged to be vigilant for any signs and symptoms of chronic liver disease and, if indicated, further assessment of the stage of hepatic fibrosis should be conducted [5455].
- Further assessment after the diagnosis of hepatic steatosis
- Keynotes
- - Staged approaches are recommended to determine the extent of liver fi-brosis in patients with NAFLD.
- - To estimate hepatic fibrosis using nonimaging modalities, noninvasive biomarker models such as fibrosis-4 (FIB-4) or the NAFLD fibrosis score (NFS) are well-validated and widely used for screening high-risk patients.
- - To assess liver fibrosis, VCTE is a point-of-care imaging device with moderate accuracy and high accessibility, while MRE has better accuracy performance, but it is not widely available.
- The severity of hepatic fibrosis is the most powerful determinant of long-term outcomes, including mortality [31]; thus, the assessment of fibrosis is essential to manage patients with NAFLD. Although quantitative noninvasive imaging assessment of steatosis is feasible in the clinical setting, none of the current imaging technologies can reliably differentiate simple steatosis from NASH or detect its progression to early stage fibrosis [56]. Several prediction scores have been developed and validated to identify or exclude advanced fibrosis (≥F3). First-line testing should use either FIB-4 or the NFS. As an alternative, the AST to platelet ratio index [APRI] may also be used. Those patients with indeterminate FIB-4 (1.3 to 2.67) or NFS scores (−1.455 to 0.676) require a second-line test in a context dependent manner: VCTE, serum enhanced liver fibrosis (ELF) score, or MRE. The ELF score is a surrogate index based on extracellular matrix panel consisting of plasma concentrations of hyaluronic acid, tissue inhibitor of metalloproteinase 1, and procollagen type III amino-terminal peptide [57] However, the ELF test seems to need further validation, even though European guidelines recommend the test [34]. Patients with high FIB-4 (>2.67) or NFS (>0.676) values should be considered for referral to a specialist clinic irrespective of second-line tests (Fig. 1) [33]. Thus, the use of these scores in combination with imaging studies seems to be more reasonable. The cytokeratin 18 fragment test did not outperform AST measurement in discriminating NASH from simple steatosis [58].
- By using VCTE, the threshold values of CAP (≥263 to 288 dB/m) for steatosis and the LSM (≥8.6 to 9.6 kPa) for advanced fibrosis have been variably reported [3948]. The very low values of the LSM (e.g., <5.6 or <6.5 kPa combined with a result from other noninvasive tests) suggest an exclusion of moderate fibrosis (Fig. 1) [59]. Although the threshold levels for the changes of MRI-PDFF to define improvement of steatosis seem to be 25% to 30%, the cutoff value for percent change in MRE to define the improvement of fibrosis needs further studies; it seems that more than a 20% difference is required to be confident [60].
- Genetic variant study
- Keynotes
- - Genetic tests for the assessment of NAFLD are not officially recommend-ed, but identifying the carriers of high-risk genetic variants may be help-ful in some specific conditions.
- Genetic factors are also important factors that determine susceptibility to the development and progression of NAFLD, considering that heritable factors account for approximately 50% of the interindividual differences in the prevalence of NASH with cirrhosis in a twin study [61]. Among several genetic risk factors, single-nucleotide polymorphisms (SNPs) in patatin-like phospholipase domain–containing 3 (PNPLA3) (rs738409 c.444 C>G, p.I148M), transmembrane 6 superfamily, member 2 (TM6SF2) (rs58542926 c.449 C>T, p.E167K), and membrane bound O-acyltransferase domain containing 7-transmembrane channel-like 4 (MBOAT7) (rs641738 C>T) have been relatively well validated to promote the development of NAFLD and its progression (i.e., cirrhosis, HCC, or both) [6263646566].
- PNPLA3 encodes adiponutrin, a triglyceride (TG) lipase that regulates both TG and retinoid metabolism. The PNPLA3 I148M variant is resistant to proteasomal degradation by evading ubiquitylation and accumulates on lipid droplets, which interferes with lipolysis and causes a change in phospholipid remodeling [67]. The PNPLA3 SNP rs738409 is strongly associated with hepatic steatosis, steatohepatitis, fibrosis, and HCC [66].
- TM6SF2 is involved in very low-density lipoprotein (VLDL) secretion from hepatocytes. The SNP rs58542926 C>T in TM6SF2 results in a loss-of-function, inducing a higher liver TG content and lower circulating lipoproteins. As with PNPLA3, the TM6SF2 minor (T) allele is associated with greater hepatic steatosis, more severe NASH and greater hepatic fibrosis/cirrhosis, but intriguingly, the more common major (C) allele is associated with the promotion of VLDL excretion, conferring an increased risk of dyslipidemia and cardiovascular disease (CAD) [6568]. In line with this, in a large exome-wide association study of plasma lipids in more than 300,000 individuals, the PNPLA3 I148M and TM6SF2 E167K variants were strongly associated with hepatic steatosis and progression to NASH, cirrhosis, and HCC, but also with increased risk of diabetes, lower blood TG, lower low-density lipoprotein cholesterol (LDL-C) concentrations, and protection from CAD [66].
- The MBOAT7 rs641738 T allele is associated with reduced MBOAT7 protein expression and has been shown to be associated with an increase in the risk of steatosis and histologic liver damage in NAFLD (i.e., higher severity of necro-inflammation and fibrosis) independent of obesity [69]. The variant may also predispose patients to HCC in patients without cirrhosis [6570]. The MBOAT7 gene encodes lysophosphatidylinositol (LPI) acyltransferase 1, known as LPIAT1 or MBOAT7, which selectively uses LPI and arachidonoyl-CoA to form 2-arachidonoyl phosphatidylinositol (PI) [7172]. Consistent with this function, lipidome changes in the plasma and liver of patients with NAFLD have been reported: decreases in plasma levels of PI (36:4), PI (38:3), and PI (38:5) and decreases in hepatic concentrations of PI (36:4) and PI (38:3) in proportion to the number of MBOAT7 variant alleles [6973]. LPIAT1 contributes to the regulation of free arachidonic acid in the cell through the remodeling of phospholipids [74]. MBOAT7 deficiency is thus predicted to increase free polyunsaturated fatty acids and their pro-inflammatory eicosanoid lipids [7075].
- Interestingly, in an Italian cohort study that evaluated the relationship between HCC risk and the total number of risk alleles including PNPLA3 I148M, TM6SF2 E167K, and MBOAT7 rs641738 T, there was a significant association between the number of risk alleles and HCC [70].
- In addition, several protective variants have also been reported [76]. In particular, SNPs (rs72613567, rs62305723, and rs6834314) in HSD17B13, a gene that encodes the hepatic lipid droplet protein 17β-hydroxysteroid dehydrogenase type 13, were reported to be associated with decreased inflammation, ballooning, and liver enzyme levels in patients with NAFLD [7778]. Recently, HSD17B13 was identified as a lipid droplet enzyme retinol dehydrogenase, highlighting the importance of retinoid homeostasis in NAFLD and its progression [78]. The splice variant rs72613567 produces a truncated, nonfunctional protein that was associated with lower odds of various liver diseases and HCC [77]. It was also found that the isoform encoded by the protective allele is catalytically defective against estradiol [77].
- Nutritional factors are very important even when considering genetic factors, as adiposity has been shown to amplify the effect of the NAFLD risk alleles in PNPLA3, TM6SF2, and glucokinase regulatory protein (GCKR) [7980]. Currently, genetic tests are not officially recommended, but identifying carriers of high risk genetic variants may be helpful in some specific conditions.
DIAGNOSIS OF NAFLD
Ultrasonography and computed tomography
Vibration-controlled transient elastography
Magnetic resonance imaging-based techniques
- Keynotes
- - Management for patients with T2DM and NAFLD should be aimed at reducing the risk factors associated with their high CV risk as well as de-creasing hepatic fat accumulation and delaying the progression of inflam-mation and fibrosis.
- - Lifestyle modification is the first step in the management for all patients with T2DM and NAFLD to improve NAFLD as well as hyperglycemia, dyslipidemia, and blood pressure levels.
- Epidemiological evidence suggests a strong bidirectional relationship between T2DM and NAFLD. Furthermore, NAFLD resolution attenuates T2DM risk, but when obesity, insulin resistance, or hyperglycemia is combined with NAFLD, the T2DM risk is significantly increased [4]. In a long-term follow-up study of patients with NAFLD, diabetes and smoking, along with fibrosis, age, and absence of statin use, contributed to mortality, underscoring the need for a comprehensive approach to patient management [32]. Additionally, spontaneous regression of NASH and even NASH-related fibrosis has been observed in clinical trials and may be related to lifestyle modifications and behavioral changes [81]. However, pharmacological treatment is more powerful than lifestyle modification for glucose control. Moreover, lifestyle modification plus anti-diabetic drugs are likely to have a synergistic effect on reducing the risk factors associated with CV risk and decreasing hepatic fat accumulation in these patients, thereby delaying the progression of inflammation and fibrosis. Therefore, all patients with T2DM and NAFLD should be strongly encouraged to adopt both lifestyle changes and anti-diabetic medication use (Fig. 2) [382].
- Weight reduction
- Keynotes
- - Weight loss induced by either lifestyle modification or bariatric surgery improves glucometabolic profiles and reduces liver fat in subjects with T2DM.
- - Regarding lifestyle modification, specific diets rather than calorie restric-tion or specific types of exercise protocols (aerobic or resistance) were not clearly defined for their efficacy at the present time.
- It is well established that weight loss induced by either lifestyle modification or bariatric surgery in overweight or obese individuals with T2DM results in significant improvement or resolution of T2DM and its comorbidities such as hypertension, and hyperlipidemia [38384]. In addition, weight reduction has been associated with alleviated intrahepatic fat contents and aminotransferase levels [81]. Even relatively small amounts of weight loss can reduce liver fat and improve hepatic insulin resistance independent of any changes in insulin-stimulated peripheral glucose metabolism [85]. In adult populations with NAFLD, a systematic review that included a total of 23 studies evaluating the effect of lifestyle interventions, such as diet, physical activity, and/or exercise, on the hepatic indicators of steatosis, inflammation and fibrosis as well as glucose control/insulin sensitivity showed that the reductions in liver fat and/or liver aminotransferase concentrations were strongly correlated with weight loss [86]. However, it should be noted that sustainable maintenance of weight loss with lifestyle interventions for long-term periods was achievable in only 3% to 6% of the subjects [915].
- Keynotes
- - The improvement in histology is proportional to the magnitude of the weight loss, but this proportional trend might not be applicable to gluco-metabolic profiles.
- - A magnitude of weight loss in the range of approximately 5% to 7% may clearly decrease steatosis but approximately 8% to 10% weight reduction is needed to reverse steatohepatitis.
- In adult populations with NAFLD, a greater degree of weight loss, induced by either lifestyle modifications or bariatric surgical procedures, is associated with a greater improvement in histologic features [82]. Summarizing all current available reports, it appears that a magnitude of weight loss in the range of approximately 5% to 7% may clearly decrease steatosis and the associated metabolic parameters, but 8% to 10% weight reduction is needed to reverse steatohepatitis [38385868788]. Although a ≥7% weight loss also improved NAS, fibrosis was unchanged. Furthermore, the highest rates of NAS reduction, steatohepatitis resolution, and fibrosis regression occurred in patients with ≥10% weight loss [89]. The threshold of 7% weight loss was achieved by <50% of patients, even with intensive multidisciplinary lifestyle intervention.
- Lifestyle modification
- Keynotes
- - The weight reduction achievable by dietary program remains the corner-stone of lifestyle modification for patients with T2DM and NAFLD.
- - Caloric restriction, rather than dietary macronutrient composition, has a greater role in preventing the development and progression of T2DM, in reducing hepatic steatosis and in delaying inflammation and fibrosis.
- - Exercise per se can reduce hepatic fat even in the absence of weight loss. Both aerobic and resistance exercise leading to a similar weight reduction are similarly effective in hepatic fat reduction in patients with T2DM.
- - Individually tailored approaches combining a mainly hypocaloric diet in conjunction with a progressive increase in aerobic exercise/resistance training are associated with the magnitude of the weight reduction.
- Of the ways to achieve weight reduction, lifestyle modification that includes a programmed diet and exercise is an effective and sound treatment for all patients with NAFLD and NASH [348290]. In addition, lifestyle modification improves hyperglycemia, atherogenic dyslipidemia, and blood pressure levels [919293]. Of the lifestyle programs, however, weight reduction achievable by dietary programs or interventions remains the cornerstone of lifestyle modification for all patients with T2DM and NAFLD [348290]. It seems that caloric restriction, rather than dietary macronutrient composition, has a greater role in reducing hepatic fat and delaying the progression of inflammation and fibrosis in patients with NAFLD [81838586949596]. Regarding the macronutrient composition, comparable effects have been observed with equally hypocaloric low-carbohydrate versus high-carbohydrate diets [97] and low-fat versus low-carbohydrate diets [98]. Exercise trials have reported an inconsistent amount of weight loss or changes in surrogate biomarkers achieved after exercise interventions, but the heterogeneities of the baseline characteristics of the study subjects and the exercise protocols must also be considered [399100]. Even with these findings, physical activity, either aerobic or resistance type, should be strongly promoted for the management of fatty liver in patients with T2DM because the benefits are not exclusively contingent upon weight loss [101]. It seems that, despite the unclear beneficial roles of exercise on weight loss and hepatic fat reduction, exercise itself has been shown to improve liver enzymes and insulin resistance in all patients with diabetes with NAFLD and NASH [102103]. A comprehensive approach with combined dietary and exercise interventions has shown significant benefit on NAFLD, especially for long-term intervention periods. However, whether a combined lifestyle intervention has synergistic effects compared to the separate approaches of diet and exercise is unclear. A meta-analysis by Keating et al. [102] showed that a combined dietary and exercise intervention had no significant pooled effects size (ES) when compared to diet alone (ES: −0.05; 95% confidence interval, −0.38 to 0.27; P=0.76). However, another systematic review that included eighteen studies to investigate whether a diet-plus-exercise intervention for a minimum of 6 months was more effective for weight loss than a diet-only intervention among obese or overweight adults showed that a combined diet-plus-exercise intervention provided greater long-term weight loss than a diet-only intervention [104]. Although the effects of lifestyle modification in the absence of weight loss on NAFLD and NASH might not be clear, it is clear that lifestyle changes with either or both a hypocaloric diet and exercise reduce the risk of CV disease and the onset and progression of T2DM [3482105].
- Pharmacologic treatment
- For patients with T2DM and NAFLD, however, pharmacological treatment is more powerful than lifestyle modification for glucose control. Moreover, lifestyle modification plus anti-diabetic drugs are likely to offer synergistic benefits for reducing the risk factors associated with their high CV risk [391] as well as decreasing hepatic fat accumulation and delaying the progression of inflammation and fibrosis. Therefore, especially in patients with T2DM, all patients should adopt both lifestyle changes and anti-diabetic medication use [82].
- Keynotes
- - Patients with T2DM and NAFLD should adopt both lifestyle changes and anti-diabetic medication use.
- - There are no definite pharmacologic treatments for NAFLD in patients with T2DM.
- - Metformin is not recommended for treating NAFLD in patients with T2DM.
- - Currently, pioglitazone could be a 1st-line option to improve NASH in patients with T2DM with some improvement in fibrosis.
- - Evidence that sodium-glucose cotransporter 2 (SGLT2) inhibitors im-prove NAFLD/NASH with fibrosis in patients with T2DM is emerging. Although not generally recommended, these agents may be considered as an initial treatment option in specific conditions for the treatment of NAFLD in patients with T2DM.
- - Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have some evi-dence of improving NAFLD/NASH with fibrosis, but these agents are not generally recommended for the treatment of NAFLD in patients with T2DM.
- - Dipeptidyl peptidase-4 (DPP-4) inhibitors are not recommended for treating NAFLD in patients with T2DM.
- Studies on metformin use in NAFLD failed to show any improvement in liver histology in patients with NAFLD and NASH [106107]. Thus, metformin is not recommended for treating NAFLD in patients with T2DM. However, T2DM is now considered an independent risk factor for HCC and metformin may have a protective role in HCC occurrence [108].
- Pioglitazone, one of the thiazolidinediones, is a peroxisome proliferator-activated receptor (PPAR)-γ agonist with insulin-sensitizing effects. An randomized controlled trial (RCT) evaluating the efficacy and safety of long-term pioglitazone (45 mg/day) treatment in patients with biopsy-proven NASH and prediabetes or T2DM showed that compared with the placebo group, only patients with T2DM showed a significant resolution of NASH (60% vs. 16%) and reduction in fibrosis from baseline [109]. Currently available data from previous studies suggest that, although it may reduce fibrosis, the clinical effect of pioglitazone may come from the suppression of rapid fibrosis progression rather than from fibrosis regression by turning off the metabolic drivers of liver fibrosis in T2DM [109110]. Pioglitazone could be a first-line therapy for patients with NASH and T2DM. However, pioglitazone should not be routinely used to treat NAFLD in patients with T2DM because of limited data and the common side effects of weight gain, fluid retention, and bone mass loss.
- Lobeglitazone is currently being prescribed for T2DM in Korea. In a multicenter, prospective clinical trial, patients with T2DM and NAFLD treated with lobeglitazone (0.5 mg daily) for 24 weeks had improved liver enzymes and ameliorated hepatic fat contents assessed by VCTE-CAP [111].
- SGLT2 inhibitors, including dapagliflozin, canagliflozin, empagliflozin, ipragliflozin, and luseogliflozin are being used increasingly in the treatment of T2DM; they promote weight loss which is an attractive property for the treatment of patients with NAFLD. Although SGLT2 inhibitors are not yet generally recommended for the treatment of NAFLD in patients with T2DM, emerging data suggest that SGLT2 inhibitors reduce the risk of progression of NAFLD [112], as the following results have been reported: a decrease in hepatic fat content [113114]; a decrease in AST and ALT [114115]; a decrease in the measures of fibrosis, such as the FIB-4 index [115116], the fibrosis index calculated from hyaluronic acid and type IV collagen 7S [116], and VCTE-measured LSM [117]; an improvement in hepatic insulin sensitivity [114]; and histology [118]. Well-designed RCTs are needed to elucidate whether SGLT2 inhibitors should be used as the first-line drug choice in patients with NAFLD/NASH with T2DM. In the meantime, these agents may be considered as an initial option to treat NAFLD in patients with T2DM and specific cardio-renal conditions [119].
- GLP-1 RAs, including exenatide, lixisenatide and liraglutide, are promising candidates for the treatment of NAFLD and NASH because they can reduce weight and enhance insulin action. However, GLP-1 RAs are not generally recommended for the treatment of NAFLD in patients with T2DM because of the limited data to date [112]. In a well-performed clinical trial in patients with biopsy-proven NASH, liraglutide (1.8 mg daily) treatment for 48 weeks was associated with greater resolution of steatohepatitis and less progression of fibrosis [120].
- DPP-4 inhibitors including sitagliptin, vildagliptin, linagliptin, saxagliptin, gemigliptin, alogliptin, teneligliptin, and anagliptin are commonly used in patients with T2DM, but there are few studies about the efficacy of DPP-4 inhibitors in patients with T2DM and NAFLD; they are not yet believed to have a beneficial effect on NAFLD. Only vildagliptin showed a clinically significant decrease in hepatic TG levels measured by MRI-PDFF (27% with vildagliptin, from 7.3%±1.0% [baseline] to 5.3%±0.9% [endpoint]), unrelated to changes in body weight, during 6 months of therapy in patients with T2DM and NAFLD [121]. Mixed results have been reported for sitagliptin. A pilot clinical study demonstrated that sitagliptin could improve hepatocyte ballooning and liver enzymes in patients with T2DM and NASH after 1 year of treatment [122]. However, many other studies have failed to show an effect of sitagliptin treatment on liver fat content or liver stiffness [123124].
- Keynotes
- - Vitamin E is not recommended to treat NAFLD in patients with T2DM.
- - Lipid-lowering agents such as statins, ezetimibe, fibrates, niacin, omega-3 polyunsaturated fatty acids, and colesevelam did not improve hepatic ste-atosis in patients with NAFLD.
- - Ursodeoxycholic acid (UDCA) and pentoxifylline are not recommended for the treatment of NAFLD or NASH.
- - Obeticholic acid may improve NASH without progression of fibrosis in patients with T2DM and NASH. Further studies are required to prove its efficacy and long-term effects as well as its adverse effects.
- Vitamin E is an antioxidant that prevents liver injury by blocking intrinsic apoptotic pathways and protecting against oxidative stress. Vitamin E improves liver histology in nondiabetic adults with biopsy-proven NASH [125], but is not recommended in patients with diabetes because of a lack of evidence [582]. In addition, there are some concerns that long-term use of vitamin E may be associated with increased all-cause mortality, an increased incidence of hemorrhagic stroke, and an increased risk of prostate cancer.
- Although statins are beneficial in the management of dyslipidemia and high CV risk as well as in reducing the risk of HCC and mortality, especially in patients with diabetes, lipid-lowering agents such as statins, ezetimibe, fibrates, niacin, omega-3 polyunsaturated fatty acids, and colesevelam did not improve hepatic steatosis in patients with NAFLD [582126]. There was also no evidence for the use of one of these agents for the treatment of NAFLD in patients with T2DM.
- UDCA, a naturally occurring bile acid, reduced oxidative stress and had antiapoptotic properties. Although several studies reported that UDCA improved liver enzymes and hepatic steatosis in patients with NAFLD [127128], both conventional (13 to 15 mg/kg daily) and high (23 to 28 mg/kg daily) doses of UDCA failed to induce histologic improvement in patients with NASH [129130].
- Pentoxifylline inhibits a number of proinflammatory cytokines including tumor necrosis factor-α. Although pentoxifylline (400 mg three times a day) improved the histological features of NASH in 55 adults with biopsy-confirmed NASH, only 9.1% of participants had T2DM [131]; another study reported no histological improvement in 30 patients, so larger studies are needed to establish the role of pentoxifylline in the management of patients with NASH and T2DM [132].
- Obeticholic acid is a natural agonist of the farnesoid X receptor and decreases insulin resistance and hepatic steatosis in animal models. Obeticholic acid (25 mg daily) treatment for 72 weeks, where 52.7% of patients had T2DM, improved liver histology in patients with NASH but increased LDL-C levels and caused pruritus [133]. Further studies are needed to clarify the long-term benefit and safety of obeticholic acid in patients with T2DM and NAFLD.
- Carnitine is a modulator of mitochondrial free fatty acid transport and oxidation and has antioxidative activity in hepatocytes [98]. In patients with NASH, L-carnitine treatment (1 g daily) for 24 weeks improved liver enzymes and histological manifestations [134]. Treatment with the carnitine-orotate complex (824 mg, three times daily) for 12 weeks in patients with T2DM and NAFLD improved serum ALT and improved hepatic steatosis as assessed by CT in 78 patients [135].
- Elafibranor is a dual agonist of PPAR-α and PPAR-δ and improves insulin resistance in liver and peripheral tissue. In a phase 2b trial, elafibranor treatment (120 mg daily) for 52 weeks tended to induce resolution of NASH without fibrosis progression despite some methodological limitations. The predefined endpoint was not met in the intention to treat population and 39.1% of study participants had T2DM [136].
- Cenicriviroc, a dual antagonist of the C-C chemokine receptor types 2 and 5, has potent anti-inflammatory and antifibrotic activity in animal models. In a phase 2b study, in which half of subjects had T2DM and two-thirds had metabolic syndrome, cenicriviroc treatment (150 mg daily) for 1 year achieved improvement in fibrosis and no worsening of steatohepatitis compared with placebo [137].
- Because weight reduction is a key component for the treatment of NAFLD, anti-obesity drugs can be potential candidates. However, few studies have investigated the efficacy of anti-obesity drugs for the treatment of NAFLD. Orlistat (120 mg three times daily for 6 months), an inhibitor of fat absorption, showed improved steatosis assessed by US and confirmed by liver biopsy in patients with NAFLD [138]. Another study evaluated the effect of orlistat on NAFLD in patients who received a 1,400 kcal/day diet plus vitamin E (800 IU) daily. Orlistat (120 mg three times a day) did not enhance weight loss or improve liver enzymes and histopathology in fifty overweight subjects (10% of subjects had T2DM) [139].
- Bariatric surgery
- Keynotes
- - In addition to its effects on body weight and metabolic profiles, bariatric surgery can decrease long-term mortality related to diabetes, CV diseas-es, and cancers.
- - Bariatric surgery can be considered in obese patients with NAFLD and T2DM to resolve NASH and improve fibrosis.
- Bariatric surgery has been accepted as a treatment option in obese patients with T2DM who do not achieve durable weight loss and improvement in comorbidities (including hyperglycemia) with nonsurgical methods [119]. A meta-analysis showed that the majority of patients undergoing bariatric surgery appear to improve or completely resolve the histopathological features of steatosis, inflammation, and ballooning. Fibrosis also improved by a weighted mean decrease of 11.9% in the incidence of fibrosis [140]. Another recent meta-analysis including 3,093 biopsies also reported the resolution of steatosis in 66% of patients, inflammation in 50%, ballooning degeneration in 76%, and fibrosis in 40% [141]. With regard to procedure selection, there is still a lack of data on which method, i.e., sleeve gastrectomy or Roux-en Y gastric bypass, is more effective. However, considering the safety of the surgery itself, sleeve gastrectomy is recommended in patients with NASH cirrhosis [82142143].
TREATMENT OF NAFLD
The magnitude of weight reduction
Anti-diabetic agents
1) Metformin
2) Thiazolidinediones
3) Sodium-glucose cotransporter 2 inhibitors
4) Glucagon-like peptide-1 receptor agonists
5) Dipeptidyl peptidase-4 inhibitors
Non-antidiabetic agents
1) Vitamin E
2) Lipid-lowering agents
3) Ursodeoxycholic acid
4) Pentoxifylline
5) Obeticholic acid
6) Carnitine
7) Elafibranor
8) Cenicriviroc
9) Anti-obesity drugs
-
Acknowledgements
- None
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
- 1. Loomba R, Abraham M, Unalp A, Wilson L, Lavine J, Doo E, Bass NM. Nonalcoholic Steatohepatitis Clinical Research Network. Association between diabetes, family history of diabetes, and risk of nonalcoholic steatohepatitis and fibrosis. Hepatology 2012;56:943-951. ArticlePubMedPMC
- 2. Lee YH, Cho Y, Lee BW, Park CY, Lee DH, Cha BS, Rhee EJ. Nonalcoholic fatty liver disease in diabetes. Part I: epidemiology and diagnosis. Diabetes Metab J 2019;43:31-45. ArticlePubMedPDF
- 3. Bril F, Cusi K. Management of nonalcoholic fatty liver disease in patients with type 2 diabetes: a call to action. Diabetes Care 2017;40:419-430. ArticlePubMedPDF
- 4. Han E, Lee YH. Non-alcoholic fatty liver disease: the emerging burden in cardiometabolic and renal diseases. Diabetes Metab J 2017;41:430-437. ArticlePubMedPMCPDF
- 5. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, Harrison SA, Brunt EM, Sanyal AJ. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67:328-357. ArticlePubMedPDF
- 6. Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, Grundy SM, Hobbs HH. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 2004;40:1387-1395. ArticlePubMed
- 7. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274-285. ArticlePubMed
- 8. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73-84. ArticlePubMed
- 9. Park SH, Jeon WK, Kim SH, Kim HJ, Park DI, Cho YK, Sung IK, Sohn CI, Keum DK, Kim BI. Prevalence and risk factors of non-alcoholic fatty liver disease among Korean adults. J Gastroenterol Hepatol 2006;21(1 Pt 1):138-143. ArticlePubMed
- 10. Jeong EH, Jun DW, Cho YK, Choe YG, Ryu S, Lee SM, Jang EC. Regional prevalence of non-alcoholic fatty liver disease in Seoul and Gyeonggi-do, Korea. Clin Mol Hepatol 2013;19:266-272. ArticlePubMedPMC
- 11. Portillo-Sanchez P, Bril F, Maximos M, Lomonaco R, Biernacki D, Orsak B, Subbarayan S, Webb A, Hecht J, Cusi K. High prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus and normal plasma aminotransferase levels. J Clin Endocrinol Metab 2015;100:2231-2238. ArticlePubMedPMCPDF
- 12. Hyysalo J, Mannisto VT, Zhou Y, Arola J, Karja V, Leivonen M, Juuti A, Jaser N, Lallukka S, Kakela P, Venesmaa S, Simonen M, Saltevo J, Moilanen L, Korpi-Hyovalti E, Keinanen-Kiukaanniemi S, Oksa H, Orho-Melander M, Valenti L, Fargion S, Pihlajamaki J, Peltonen M, Yki-Jarvinen H. A population-based study on the prevalence of NASH using scores validated against liver histology. J Hepatol 2014;60:839-846. ArticlePubMed
- 13. Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, Contreras M, Landt CL, Harrison SA. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124-131. ArticlePubMed
- 14. Younossi ZM, Marchesini G, Pinto-Cortez H, Petta S. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: implications for liver transplantation. Transplantation 2019;103:22-27. ArticlePubMed
- 15. Kim BY, Jung CH, Mok JO, Kang SK, Kim CH. Prevalences of diabetic retinopathy and nephropathy are lower in Korean type 2 diabetic patients with non-alcoholic fatty liver disease. J Diabetes Investig 2014;5:170-175.ArticlePubMedPDF
- 16. Mohan V, Farooq S, Deepa M, Ravikumar R, Pitchumoni CS. Prevalence of non-alcoholic fatty liver disease in urban south Indians in relation to different grades of glucose intolerance and metabolic syndrome. Diabetes Res Clin Pract 2009;84:84-91. ArticlePubMed
- 17. Kim SK, Choi YJ, Huh BW, Park SW, Lee EJ, Cho YW, Huh KB. Nonalcoholic fatty liver disease is associated with increased carotid intima-media thickness only in type 2 diabetic subjects with insulin resistance. J Clin Endocrinol Metab 2014;99:1879-1884. ArticlePubMed
- 18. Targher G, Bertolini L, Rodella S, Tessari R, Zenari L, Lippi G, Arcaro G. Nonalcoholic fatty liver disease is independently associated with an increased incidence of cardiovascular events in type 2 diabetic patients. Diabetes Care 2007;30:2119-2121. ArticlePubMedPDF
- 19. Kim CH, Park JY, Lee KU, Kim JH, Kim HK. Fatty liver is an independent risk factor for the development of type 2 diabetes in Korean adults. Diabet Med 2008;25:476-481. ArticlePubMed
- 20. Sung KC, Kim SH. Interrelationship between fatty liver and insulin resistance in the development of type 2 diabetes. J Clin Endocrinol Metab 2011;96:1093-1097. ArticlePubMedPMCPDF
- 21. Sung KC, Wild SH, Byrne CD. Resolution of fatty liver and risk of incident diabetes. J Clin Endocrinol Metab 2013;98:3637-3643. ArticlePubMedPDF
- 22. Yamazaki H, Tsuboya T, Tsuji K, Dohke M, Maguchi H. Independent association between improvement of nonalcoholic fatty liver disease and reduced incidence of type 2 diabetes. Diabetes Care 2015;38:1673-1679. ArticlePubMedPDF
- 23. Bhatia LS, Curzen NP, Calder PC, Byrne CD. Non-alcoholic fatty liver disease: a new and important cardiovascular risk factor? Eur Heart J 2012;33:1190-1200. ArticlePubMed
- 24. Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643-654. ArticlePubMed
- 25. McPherson S, Hardy T, Henderson E, Burt AD, Day CP, Anstee QM. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol 2015;62:1148-1155. ArticlePubMed
- 26. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med 2002;346:1221-1231. ArticlePubMed
- 27. Mittal S, Sada YH, El-Serag HB, Kanwal F, Duan Z, Temple S, May SB, Kramer JR, Richardson PA, Davila JA. Temporal trends of nonalcoholic fatty liver disease-related hepatocellular carcinoma in the veteran affairs population. Clin Gastroenterol Hepatol 2015;13:594-601. ArticlePubMed
- 28. Pocha C, Kolly P, Dufour JF. Nonalcoholic fatty liver disease-related hepatocellular carcinoma: a problem of growing magnitude. Semin Liver Dis 2015;35:304-317. ArticlePubMed
- 29. Lee SS, Jeong SH, Byoun YS, Chung SM, Seong MH, Sohn HR, Min BY, Jang ES, Kim JW, Park GJ, Lee YJ, Lee KH, Ahn S. Clinical features and outcome of cryptogenic hepatocellular carcinoma compared to those of viral and alcoholic hepatocellular carcinoma. BMC Cancer 2013;13:335. ArticlePubMedPMCPDF
- 30. Allen AM, Therneau TM, Larson JJ, Coward A, Somers VK, Kamath PS. Nonalcoholic fatty liver disease incidence and impact on metabolic burden and death: a 20 year-community study. Hepatology 2018;67:1726-1736. ArticlePubMedPMCPDF
- 31. Ekstedt M, Hagstrom H, Nasr P, Fredrikson M, Stal P, Kechagias S, Hultcrantz R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015;61:1547-1554. ArticlePubMed
- 32. Angulo P, Kleiner DE, Dam-Larsen S, Adams LA, Bjornsson ES, Charatcharoenwitthaya P, Mills PR, Keach JC, Lafferty HD, Stahler A, Haflidadottir S, Bendtsen F. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2015;149:389-397. ArticlePubMedPMC
- 33. Newsome PN, Cramb R, Davison SM, Dillon JF, Foulerton M, Godfrey EM, Hall R, Harrower U, Hudson M, Langford A, Mackie A, Mitchell-Thain R, Sennett K, Sheron NC, Verne J, Walmsley M, Yeoman A. Guidelines on the management of abnormal liver blood tests. Gut 2018;67:6-19. ArticlePubMed
- 34. European Association for the Study of the Liver (EASL). European Association for the Study of Diabetes (EASD). European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016;59:1121-1140. ArticlePubMedPDF
- 35. Prati D, Colli A, Conte D, Colombo M. Spectrum of NAFLD and diagnostic implications of the proposed new normal range for serum ALT in obese women. Hepatology 2005;42:1460-1461. ArticlePubMed
- 36. Kwo PY, Cohen SM, Lim JK. ACG clinical guideline: evaluation of abnormal liver chemistries. Am J Gastroenterol 2017;112:18-35. ArticlePubMedPDF
- 37. Terrault NA, Lok ASF, McMahon BJ, Chang KM, Hwang JP, Jonas MM, Brown RS Jr, Bzowej NH, Wong JB. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018;67:1560-1599. ArticlePubMedPMCPDF
- 38. Hernaez R, Lazo M, Bonekamp S, Kamel I, Brancati FL, Guallar E, Clark JM. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 2011;54:1082-1090. ArticlePubMedPMC
- 39. Stefan N, Haring HU, Cusi K. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol 2019;7:313-324. ArticlePubMed
- 40. Bril F, Ortiz-Lopez C, Lomonaco R, Orsak B, Freckleton M, Chintapalli K, Hardies J, Lai S, Solano F, Tio F, Cusi K. Clinical value of liver ultrasound for the diagnosis of nonalcoholic fatty liver disease in overweight and obese patients. Liver Int 2015;35:2139-2146. ArticlePubMedPDF
- 41. Petta S, Ciminnisi S, Di Marco V, Cabibi D, Camma C, Licata A, Marchesini G, Craxi A. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2017;45:510-518. ArticlePubMedPDF
- 42. Shen F, Zheng RD, Shi JP, Mi YQ, Chen GF, Hu X, Liu YG, Wang XY, Pan Q, Chen GY, Chen JN, Xu L, Zhang RN, Xu LM, Fan JG. Impact of skin capsular distance on the performance of controlled attenuation parameter in patients with chronic liver disease. Liver Int 2015;35:2392-2400. ArticlePubMedPMCPDF
- 43. Vuppalanchi R, Siddiqui MS, Van Natta ML, Hallinan E, Brandman D, Kowdley K, Neuschwander-Tetri BA, Loomba R, Dasarathy S, Abdelmalek M, Doo E, Tonascia JA, Kleiner DE, Sanyal AJ, Chalasani N. NASH Clinical Research Network. Performance characteristics of vibration-controlled transient elastography for evaluation of nonalcoholic fatty liver disease. Hepatology 2018;67:134-144. ArticlePubMedPDF
- 44. Kim KY, Song JS, Kannengiesser S, Han YM. Hepatic fat quantification using the proton density fat fraction (PDFF): utility of free-drawn-PDFF with a large coverage area. Radiol Med 2015;120:1083-1093. ArticlePubMedPDF
- 45. Capitan V, Petit JM, Aho S, Lefevre PH, Favelier S, Loffroy R, Hillon P, Krause D, Cercueil JP, Guiu B. Macroscopic heterogeneity of liver fat: an MR-based study in type-2 diabetic patients. Eur Radiol 2012;22:2161-2168. ArticlePubMedPDF
- 46. Loomba R, Wolfson T, Ang B, Hooker J, Behling C, Peterson M, Valasek M, Lin G, Brenner D, Gamst A, Ehman R, Sirlin C. Magnetic resonance elastography predicts advanced fibrosis in patients with nonalcoholic fatty liver disease: a prospective study. Version 2. Hepatology 2014;60:1920-1928. ArticlePubMedPDF
- 47. Kim D, Kim WR, Talwalkar JA, Kim HJ, Ehman RL. Advanced fibrosis in nonalcoholic fatty liver disease: noninvasive assessment with MR elastography. Radiology 2013;268:411-419. ArticlePubMedPMC
- 48. Caussy C, Alquiraish MH, Nguyen P, Hernandez C, Cepin S, Fortney LE, Ajmera V, Bettencourt R, Collier S, Hooker J, Sy E, Rizo E, Richards L, Sirlin CB, Loomba R. Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis. Hepatology 2018;67:1348-1359. ArticlePubMedPMCPDF
- 49. Nasr P, Forsgren MF, Ignatova S, Dahlstrom N, Cedersund G, Leinhard OD, Noren B, Ekstedt M, Lundberg P, Kechagias S. Using a 3% proton density fat fraction as a cut-off value increases sensitivity of detection of hepatic steatosis, based on results from histopathology analysis. Gastroenterology 2017;153:53-55. ArticlePubMed
- 50. Bannas P, Kramer H, Hernando D, Agni R, Cunningham AM, Mandal R, Motosugi U, Sharma SD, Munoz del, Fernandez L, Reeder SB. Quantitative magnetic resonance imaging of hepatic steatosis: validation in ex vivo human livers. Hepatology 2015;62:1444-1455. ArticlePubMedPMC
- 51. Patel J, Bettencourt R, Cui J, Salotti J, Hooker J, Bhatt A, Hernandez C, Nguyen P, Aryafar H, Valasek M, Haufe W, Hooker C, Richards L, Sirlin CB, Loomba R. Association of noninvasive quantitative decline in liver fat content on MRI with histologic response in nonalcoholic steatohepatitis. Therap Adv Gastroenterol 2016;9:692-701.ArticlePubMedPMCPDF
- 52. Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med 2001;344:495-500. ArticlePubMed
- 53. Gunn NT, Shiffman ML. The use of liver biopsy in nonalcoholic fatty liver disease: when to biopsy and in whom. Clin Liver Dis 2018;22:109-119. PubMed
- 54. Wong VW, Chalasani N. Not routine screening, but vigilance for chronic liver disease in patients with type 2 diabetes. J Hepatol 2016;64:1211-1213. ArticlePubMed
- 55. Corey KE, Klebanoff MJ, Tramontano AC, Chung RT, Hur C. Screening for nonalcoholic steatohepatitis in individuals with type 2 diabetes: a cost-effectiveness analysis. Dig Dis Sci 2016;61:2108-2117. ArticlePubMedPMCPDF
- 56. Bedossa P, Patel K. Biopsy and noninvasive methods to assess progression of nonalcoholic fatty liver disease. Gastroenterology 2016;150:1811-1822. ArticlePubMed
- 57. Lichtinghagen R, Pietsch D, Bantel H, Manns MP, Brand K, Bahr MJ. The Enhanced Liver Fibrosis (ELF) score: normal values, influence factors and proposed cut-off values. J Hepatol 2013;59:236-242. ArticlePubMed
- 58. Tada T, Kumada T, Toyoda H, Saibara T, Ono M, Kage M. New scoring system combining the FIB-4 index and cytokeratin-18 fragments for predicting steatohepatitis and liver fibrosis in patients with nonalcoholic fatty liver disease. Biomarkers 2018;23:328-334. ArticlePubMed
- 59. Siddiqui MS, Vuppalanchi R, Van Natta ML, Hallinan E, Kowdley KV, Abdelmalek M, Neuschwander-Tetri BA, Loomba R, Dasarathy S, Brandman D, Doo E, Tonascia JA, Kleiner DE, Chalasani N, Sanyal AJ. NASH Clinical Research Network. Vibration-controlled transient elastography to assess fibrosis and steatosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2019;17:156-163. ArticlePubMed
- 60. Jayakumar S, Middleton MS, Lawitz EJ, Mantry PS, Caldwell SH, Arnold H, Mae Diehl A, Ghalib R, Elkhashab M, Abdelmalek MF, Kowdley KV, Stephen Djedjos C, Xu R, Han L, Mani Subramanian G, Myers RP, Goodman ZD, Afdhal NH, Charlton MR, Sirlin CB, Loomba R. Longitudinal correlations between MRE, MRI-PDFF, and liver histology in patients with non-alcoholic steatohepatitis: analysis of data from a phase II trial of selonsertib. J Hepatol 2019;70:133-141. ArticlePubMed
- 61. Loomba R, Schork N, Chen CH, Bettencourt R, Bhatt A, Ang B, Nguyen P, Hernandez C, Richards L, Salotti J, Lin S, Seki E, Nelson KE, Sirlin CB, Brenner D. Genetics of NAFLD in Twins Consortium. Heritability of hepatic fibrosis and steatosis based on a prospective twin study. Gastroenterology 2015;149:1784-1793. ArticlePubMed
- 62. Krawczyk M, Rau M, Schattenberg JM, Bantel H, Pathil A, Demir M, Kluwe J, Boettler T, Lammert F, Geier A. NAFLD Clinical Study Group. Combined effects of the PNPLA3 rs738409, TM6SF2 rs58542926, and MBOAT7 rs641738 variants on NAFLD severity: a multicenter biopsy-based study. J Lipid Res 2017;58:247-255. ArticlePubMed
- 63. Koo BK, Joo SK, Kim D, Bae JM, Park JH, Kim JH, Kim W. Additive effects of PNPLA3 and TM6SF2 on the histological severity of non-alcoholic fatty liver disease. J Gastroenterol Hepatol 2018;33:1277-1285. ArticlePubMedPDF
- 64. Romeo S, Kozlitina J, Xing C, Pertsemlidis A, Cox D, Pennacchio LA, Boerwinkle E, Cohen JC, Hobbs HH. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461-1465. ArticlePubMedPMCPDF
- 65. Del Campo JA, Gallego-Duran R, Gallego P, Grande L. Genetic and epigenetic regulation in nonalcoholic fatty liver disease (NAFLD). Int J Mol Sci 2018;19:E911.
- 66. Liu DJ, Peloso GM, Yu H, Butterworth AS, Wang X, Mahajan A, Saleheen D, Emdin C, Alam D, Alves AC, Amouyel P, Di Angelantonio E, Arveiler D, Assimes TL, Auer PL, Baber U, Ballantyne CM, Bang LE, Benn M, Bis JC, Boehnke M, Boerwinkle E, Bork-Jensen J, Bottinger EP, Brandslund I, Brown M, Busonero F, Caulfield MJ, Chambers JC, Chasman DI, Chen YE, Chen YI, Chowdhury R, Christensen C, Chu AY, Connell JM, Cucca F, Cupples LA, Damrauer SM, Davies G, Deary IJ, Dedoussis G, Denny JC, Dominiczak A, Dube MP, Ebeling T, Eiriksdottir G, Esko T, Farmaki AE, Feitosa MF, Ferrario M, Ferrieres J, Ford I, Fornage M, Franks PW, Frayling TM, Frikke-Schmidt R, Fritsche LG, Frossard P, Fuster V, Ganesh SK, Gao W, Garcia ME, Gieger C, Giulianini F, Goodarzi MO, Grallert H, Grarup N, Groop L, Grove ML, Gudnason V, Hansen T, Harris TB, Hayward C, Hirschhorn JN, Holmen OL, Huffman J, Huo Y, Hveem K, Jabeen S, Jackson AU, Jakobsdottir J, Jarvelin MR, Jensen GB, Jorgensen ME, Jukema JW, Justesen JM, Kamstrup PR, Kanoni S, Karpe F, Kee F, Khera AV, Klarin D, Koistinen HA, Kooner JS, Kooperberg C, Kuulasmaa K, Kuusisto J, Laakso M, Lakka T, Langenberg C, Langsted A, Launer LJ, Lauritzen T, Liewald DCM, Lin LA, Linneberg A, Loos RJF, Lu Y, Lu X, Magi R, Malarstig A, Manichaikul A, Manning AK, Mantyselka P, Marouli E, Masca NGD, Maschio A, Meigs JB, Melander O, Metspalu A, Morris AP, Morrison AC, Mulas A, Muller-Nurasyid M, Munroe PB, Neville MJ, Nielsen JB, Nielsen SF, Nordestgaard BG, Ordovas JM, Mehran R, O'Donnell CJ, Orho-Melander M, Molony CM, Muntendam P, Padmanabhan S, Palmer CNA, Pasko D, Patel AP, Pedersen O, Perola M, Peters A, Pisinger C, Pistis G, Polasek O, Poulter N, Psaty BM, Rader DJ, Rasheed A, Rauramaa R, Reilly DF, Reiner AP, Renström F, Rich SS, Ridker PM, Rioux JD, Robertson NR, Roden DM, Rotter JI, Rudan I, Salomaa V, Samani NJ, Sanna S, Sattar N, Schmidt EM, Scott RA, Sever P, Sevilla RS, Shaffer CM, Sim X, Sivapalaratnam S, Small KS, Smith AV, Smith BH, Somayajula S, Southam L, Spector TD, Speliotes EK, Starr JM, Stirrups KE, Stitziel N, Strauch K, Stringham HM, Surendran P, Tada H, Tall AR, Tang H, Tardif JC, Taylor KD, Trompet S, Tsao PS, Tuomilehto J, Tybjaerg-Hansen A, van Zuydam NR, Varbo A, Varga TV, Virtamo J, Waldenberger M, Wang N, Wareham NJ, Warren HR, Weeke PE, Weinstock J, Wessel J, Wilson JG, Wilson PWF, Xu M, Yaghootkar H, Young R, Zeggini E, Zhang H, Zheng NS, Zhang W, Zhang Y, Zhou W, Zhou Y, Zoledziewska M, Howson JMM, Danesh J, McCarthy MI, Cowan CA, Abecasis G, Deloukas P, Musunuru K, Willer CJ, Kathiresan S. Charge Diabetes Working Group. EPIC-InterAct Consortium. EPIC-CVD Consortium. GOLD Consortium. VA Million Veteran Program. Exome-wide association study of plasma lipids in >300,000 individuals. Nat Genet 2017;49:1758-1766. ArticlePubMedPMCPDF
- 67. BasuRay S, Smagris E, Cohen JC, Hobbs HH. The PNPLA3 variant associated with fatty liver disease (I148M) accumulates on lipid droplets by evading ubiquitylation. Version 2. Hepatology 2017;66:1111-1124. ArticlePubMedPMCPDF
- 68. Kahali B, Liu YL, Daly AK, Day CP, Anstee QM, Speliotes EK. TM6SF2: catch-22 in the fight against nonalcoholic fatty liver disease and cardiovascular disease? Gastroenterology 2015;148:679-684. ArticlePubMed
- 69. Mancina RM, Dongiovanni P, Petta S, Pingitore P, Meroni M, Rametta R, Boren J, Montalcini T, Pujia A, Wiklund O, Hindy G, Spagnuolo R, Motta BM, Pipitone RM, Craxi A, Fargion S, Nobili V, Kakela P, Karja V, Mannisto V, Pihlajamaki J, Reilly DF, Castro-Perez J, Kozlitina J, Valenti L, Romeo S. The MBOAT7-TMC4 variant rs641738 increases risk of nonalcoholic fatty liver disease in individuals of European descent. Gastroenterology 2016;150:1219-1230. ArticlePubMedPMC
- 70. Donati B, Dongiovanni P, Romeo S, Meroni M, McCain M, Miele L, Petta S, Maier S, Rosso C, De Luca L, Vanni E, Grimaudo S, Romagnoli R, Colli F, Ferri F, Mancina RM, Iruzubieta P, Craxi A, Fracanzani AL, Grieco A, Corradini SG, Aghemo A, Colombo M, Soardo G, Bugianesi E, Reeves H, Anstee QM, Fargion S, Valenti L. MBOAT7 rs641738 variant and hepatocellular carcinoma in non-cirrhotic individuals. Sci Rep 2017;7:4492. ArticlePubMedPMCPDF
- 71. Yamashita A, Hayashi Y, Nemoto-Sasaki Y, Ito M, Oka S, Tanikawa T, Waku K, Sugiura T. Acyltransferases and transacylases that determine the fatty acid composition of glycerolipids and the metabolism of bioactive lipid mediators in mammalian cells and model organisms. Prog Lipid Res 2014;53:18-81. ArticlePubMed
- 72. D'Souza K, Epand RM. Enrichment of phosphatidylinositols with specific acyl chains. Biochim Biophys Acta 2014;1838:1501-1508. ArticlePubMed
- 73. Luukkonen PK, Zhou Y, Hyotylainen T, Leivonen M, Arola J, Orho-Melander M, Oresic M, Yki-Jarvinen H. The MBOAT7 variant rs641738 alters hepatic phosphatidylinositols and increases severity of non-alcoholic fatty liver disease in humans. J Hepatol 2016;65:1263-1265. ArticlePubMed
- 74. Zarini S, Hankin JA, Murphy RC, Gijon MA. Lysophospholipid acyltransferases and eicosanoid biosynthesis in zebrafish myeloid cells. Prostaglandins Other Lipid Mediat 2014;113-115:52-61. ArticlePubMed
- 75. Perez-Chacon G, Astudillo AM, Balgoma D, Balboa MA, Balsinde J. Control of free arachidonic acid levels by phospholipases A2 and lysophospholipid acyltransferases. Biochim Biophys Acta 2009;1791:1103-1113. ArticlePubMed
- 76. Danford CJ, Yao ZM, Jiang ZG. Non-alcoholic fatty liver disease: a narrative review of genetics. J Biomed Res 2018;32:389-400. ArticlePubMedPMC
- 77. Abul-Husn NS, Cheng X, Li AH, Xin Y, Schurmann C, Stevis P, Liu Y, Kozlitina J, Stender S, Wood GC, Stepanchick AN, Still MD, McCarthy S, O'Dushlaine C, Packer JS, Balasubramanian S, Gosalia N, Esopi D, Kim SY, Mukherjee S, Lopez AE, Fuller ED, Penn J, Chu X, Luo JZ, Mirshahi UL, Carey DJ, Still CD, Feldman MD, Small A, Damrauer SM, Rader DJ, Zambrowicz B, Olson W, Murphy AJ, Borecki IB, Shuldiner AR, Reid JG, Overton JD, Yancopoulos GD, Hobbs HH, Cohen JC, Gottesman O, Teslovich TM, Baras A, Mirshahi T, Gromada J, Dewey FE. A protein-truncating HSD17B13 variant and protection from chronic liver disease. N Engl J Med 2018;378:1096-1106. ArticlePubMedPMC
- 78. Ma Y, Belyaeva OV, Brown PM, Fujita K, Valles K, Karki S, de Boer YS, Koh C, Chen Y, Du X, Handelman SK, Chen V, Speliotes EK, Nestlerode C, Thomas E, Kleiner DE, Zmuda JM, Sanyal AJ, Kedishvili NY, Liang TJ, Rotman Y. for the Nonalcoholic Steatohepatitis Clinical Research Network. 17-Beta hydroxysteroid dehydrogenase 13 is a hepatic retinol dehydrogenase associated with histological features of nonalcoholic fatty liver disease. Hepatology 2019;69:1504-1519. ArticlePubMedPMCPDF
- 79. Sliz E, Sebert S, Wurtz P, Kangas AJ, Soininen P, Lehtimaki T, Kahonen M, Viikari J, Mannikko M, Ala-Korpela M, Raitakari OT, Kettunen J. NAFLD risk alleles in PNPLA3, TM6SF2, GCKR and LYPLAL1 show divergent metabolic effects. Hum Mol Genet 2018;27:2214-2223. ArticlePubMedPMC
- 80. Stender S, Kozlitina J, Nordestgaard BG, Tybjærg-Hansen A, Hobbs HH, Cohen JC. Adiposity amplifies the genetic risk of fatty liver disease conferred by multiple loci. Nat Genet 2017;49:842-847. ArticlePubMedPMCPDF
- 81. Younossi ZM, Loomba R, Rinella ME, Bugianesi E, Marchesini G, Neuschwander-Tetri BA, Serfaty L, Negro F, Caldwell SH, Ratziu V, Corey KE, Friedman SL, Abdelmalek MF, Harrison SA, Sanyal AJ, Lavine JE, Mathurin P, Charlton MR, Chalasani NP, Anstee QM, Kowdley KV, George J, Goodman ZD, Lindor K. Current and future therapeutic regimens for nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology 2018;68:361-371. ArticlePubMedPMCPDF
- 82. Kim KS, Lee BW, Kim YJ, Lee DH, Cha BS, Park CY. Nonalcoholic fatty liver disease and diabetes: part II. Treatment. Diabetes Metab J 2019;43:127-143. ArticlePubMedPMCPDF
- 83. Lazo M, Solga SF, Horska A, Bonekamp S, Diehl AM, Brancati FL, Wagenknecht LE, Pi-Sunyer FX, Kahn SE, Clark JM. Fatty Liver Subgroup of the Look AHEAD Research Group. Effect of a 12-month intensive lifestyle intervention on hepatic steatosis in adults with type 2 diabetes. Diabetes Care 2010;33:2156-2163. ArticlePubMedPMCPDF
- 84. Ikramuddin S, Korner J, Lee WJ, Connett JE, Inabnet WB, Billington CJ, Thomas AJ, Leslie DB, Chong K, Jeffery RW, Ahmed L, Vella A, Chuang LM, Bessler M, Sarr MG, Swain JM, Laqua P, Jensen MD, Bantle JP. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes, hypertension, and hyperlipidemia: the Diabetes Surgery Study randomized clinical trial. JAMA 2013;309:2240-2249. ArticlePubMedPMC
- 85. Petersen KF, Dufour S, Befroy D, Lehrke M, Hendler RE, Shulman GI. Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes 2005;54:603-608. ArticlePubMedPMCPDF
- 86. Thoma C, Day CP, Trenell MI. Lifestyle interventions for the treatment of non-alcoholic fatty liver disease in adults: a systematic review. J Hepatol 2012;56:255-266. ArticlePubMed
- 87. Mummadi RR, Kasturi KS, Chennareddygari S, Sood GK. Effect of bariatric surgery on nonalcoholic fatty liver disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2008;6:1396-1402. ArticlePubMed
- 88. Musso G, Cassader M, Rosina F, Gambino R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomized trials. Diabetologia 2012;55:885-904. ArticlePubMedPDF
- 89. Romero-Gomez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol 2017;67:829-846. ArticlePubMed
- 90. Rinella ME. Nonalcoholic fatty liver disease: a systematic review. JAMA 2015;313:2263-2273. ArticlePubMed
- 91. Kim MK, Ko SH, Kim BY, Kang ES, Noh J, Kim SK, Park SO, Hur KY, Chon S, Moon MK, Kim NH, Kim SY, Rhee SY, Lee KW, Kim JH, Rhee EJ, Chun S, Yu SH, Kim DJ, Kwon HS, Park KS. Committee of Clinical Practice Guidelines, Korean Diabetes Association. 2019 Clinical practice guidelines for type 2 diabetes mellitus in Korea. Diabetes Metab J 2019;43:398-406. ArticlePubMedPMCPDF
- 92. Ko SH, Hur KY, Rhee SY, Kim NH, Moon MK, Park SO, Lee BW, Kim HJ, Choi KM, Kim JH. Committee of Clinical Practice Guideline of Korean Diabetes Association. Antihyperglycemic agent therapy for adult patients with type 2 diabetes mellitus 2017: a position statement of the Korean Diabetes Association. Diabetes Metab J 2017;41:337-348. ArticlePubMedPMCPDF
- 93. Jang JE, Cho Y, Lee BW, Shin ES, Lee SH. Effectiveness of exercise intervention in reducing body weight and glycosylated hemoglobin levels in patients with type 2 diabetes mellitus in Korea: a systematic review and meta-analysis. Diabetes Metab J 2019;43:302-318. ArticlePubMedPDF
- 94. Promrat K, Kleiner DE, Niemeier HM, Jackvony E, Kearns M, Wands JR, Fava JL, Wing RR. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010;51:121-129. ArticlePubMedPMC
- 95. Wong VW, Wong GL, Chan RS, Shu SS, Cheung BH, Li LS, Chim AM, Chan CK, Leung JK, Chu WC, Woo J, Chan HL. Beneficial effects of lifestyle intervention in non-obese patients with non-alcoholic fatty liver disease. J Hepatol 2018;69:1349-1356. ArticlePubMed
- 96. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, Friedman SL, Diago M, Romero-Gomez M. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015;149:367-378. ArticlePubMed
- 97. Kirk E, Reeds DN, Finck BN, Mayurranjan SM, Patterson BW, Klein S. Dietary fat and carbohydrates differentially alter insulin sensitivity during caloric restriction. Gastroenterology 2009;136:1552-1560. ArticlePubMedPMC
- 98. Haufe S, Engeli S, Kast P, Bohnke J, Utz W, Haas V, Hermsdorf M, Mahler A, Wiesner S, Birkenfeld AL, Sell H, Otto C, Mehling H, Luft FC, Eckel J, Schulz-Menger J, Boschmann M, Jordan J. Randomized comparison of reduced fat and reduced carbohydrate hypocaloric diets on intrahepatic fat in overweight and obese human subjects. Hepatology 2011;53:1504-1514. ArticlePubMed
- 99. Tamura Y, Tanaka Y, Sato F, Choi JB, Watada H, Niwa M, Kinoshita J, Ooka A, Kumashiro N, Igarashi Y, Kyogoku S, Maehara T, Kawasumi M, Hirose T, Kawamori R. Effects of diet and exercise on muscle and liver intracellular lipid contents and insulin sensitivity in type 2 diabetic patients. J Clin Endocrinol Metab 2005;90:3191-3196. ArticlePubMed
- 100. Keating SE, Hackett DA, Parker HM, O'Connor HT, Gerofi JA, Sainsbury A, Baker MK, Chuter VH, Caterson ID, George J, Johnson NA. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J Hepatol 2015;63:174-182. ArticlePubMed
- 101. Johnson NA, Sachinwalla T, Walton DW, Smith K, Armstrong A, Thompson MW, George J. Aerobic exercise training reduces hepatic and visceral lipids in obese individuals without weight loss. Hepatology 2009;50:1105-1112. ArticlePubMed
- 102. Keating SE, Hackett DA, George J, Johnson NA. Exercise and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Hepatol 2012;57:157-166. ArticlePubMed
- 103. Bacchi E, Negri C, Targher G, Faccioli N, Lanza M, Zoppini G, Zanolin E, Schena F, Bonora E, Moghetti P. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease (the RAED2 Randomized Trial). Hepatology 2013;58:1287-1295. ArticlePubMed
- 104. Wu T, Gao X, Chen M, van Dam RM. Long-term effectiveness of diet-plus-exercise interventions vs. diet-only interventions for weight loss: a meta-analysis. Obes Rev 2009;10:313-323. ArticlePubMed
- 105. Maruthur NM, Wang NY, Appel LJ. Lifestyle interventions reduce coronary heart disease risk: results from the PREMIER trial. Circulation 2009;119:2026-2031. ArticlePubMedPMC
- 106. Musso G, Gambino R, Cassader M, Pagano G. A meta-analysis of randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology 2010;52:79-104. ArticlePubMed
- 107. Lavine JE, Schwimmer JB, Van Natta ML, Molleston JP, Murray KF, Rosenthal P, Abrams SH, Scheimann AO, Sanyal AJ, Chalasani N, Tonascia J, Unalp A, Clark JM, Brunt EM, Kleiner DE, Hoofnagle JH, Robuck PR. Nonalcoholic Steatohepatitis Clinical Research Network. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA 2011;305:1659-1668. ArticlePubMedPMC
- 108. Fujita K, Iwama H, Miyoshi H, Tani J, Oura K, Tadokoro T, Sakamoto T, Nomura T, Morishita A, Yoneyama H, Masaki T. Diabetes mellitus and metformin in hepatocellular carcinoma. World J Gastroenterol 2016;22:6100-6113. ArticlePubMedPMC
- 109. Bril F, Kalavalapalli S, Clark VC, Lomonaco R, Soldevila-Pico C, Liu IC, Orsak B, Tio F, Cusi K. Response to pioglitazone in patients with nonalcoholic steatohepatitis with vs without type 2 diabetes. Clin Gastroenterol Hepatol 2018;16:558-566. ArticlePubMed
- 110. Musso G, Cassader M, Paschetta E, Gambino R. Thiazolidinediones and advanced liver fibrosis in nonalcoholic steatohepatitis: a meta-analysis. JAMA Intern Med 2017;177:633-640. ArticlePubMedPMC
- 111. Lee YH, Kim JH, Kim SR, Jin HY, Rhee EJ, Cho YM, Lee BW. Lobeglitazone, a novel thiazolidinedione, improves non-alcoholic fatty liver disease in type 2 diabetes: its efficacy and predictive factors related to responsiveness. J Korean Med Sci 2017;32:60-69. ArticlePubMedPDF
- 112. Ranjbar G, Mikhailidis DP, Sahebkar A. Effects of newer antidiabetic drugs on nonalcoholic fatty liver and steatohepatitis: think out of the box! Metabolism 2019;101:154001. ArticlePubMed
- 113. Kuchay MS, Krishan S, Mishra SK, Farooqui KJ, Singh MK, Wasir JS, Bansal B, Kaur P, Jevalikar G, Gill HK, Choudhary NS, Mithal A. Effect of empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: a randomized controlled trial (E-LIFT trial). Diabetes Care 2018;41:1801-1808. ArticlePubMedPDF
- 114. Cusi K, Bril F, Barb D, Polidori D, Sha S, Ghosh A, Farrell K, Sunny NE, Kalavalapalli S, Pettus J, Ciaraldi TP, Mudaliar S, Henry RR. Effect of canagliflozin treatment on hepatic triglyceride content and glucose metabolism in patients with type 2 diabetes. Diabetes Obes Metab 2019;21:812-821. ArticlePubMedPDF
- 115. Itani T, Ishihara T. Efficacy of canagliflozin against nonalcoholic fatty liver disease: a prospective cohort study. Obes Sci Pract 2018;4:477-482. ArticlePubMedPMCPDF
- 116. Seko Y, Nishikawa T, Umemura A, Yamaguchi K, Moriguchi M, Yasui K, Kimura M, Iijima H, Hashimoto T, Sumida Y, Okanoue T, Itoh Y. Efficacy and safety of canagliflozin in type 2 diabetes mellitus patients with biopsy-proven nonalcoholic steatohepatitis classified as stage 1-3 fibrosis. Diabetes Metab Syndr Obes 2018;11:835-843. PubMedPMC
- 117. Shimizu M, Suzuki K, Kato K, Jojima T, Iijima T, Murohisa T, Iijima M, Takekawa H, Usui I, Hiraishi H, Aso Y. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes Metab 2019;21:285-292. ArticlePubMedPDF
- 118. Akuta N, Kawamura Y, Watanabe C, Nishimura A, Okubo M, Mori Y, Fujiyama S, Sezaki H, Hosaka T, Kobayashi M, Kobayashi M, Saitoh S, Suzuki F, Suzuki Y, Arase Y, Ikeda K, Kumada H. Impact of sodium glucose cotransporter 2 inhibitor on histological features and glucose metabolism of non-alcoholic fatty liver disease complicated by diabetes mellitus. Hepatol Res 2019;49:531-539. ArticlePubMedPDF
- 119. American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes. 2020. Diabetes Care 2020;43(Suppl 1):S98-S110. ArticlePubMedPDF
- 120. Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, Hazlehurst JM, Guo K, Abouda G, Aldersley MA, Stocken D, Gough SC, Tomlinson JW, Brown RM, Hubscher SG, Newsome PN. LEAN trial team. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016;387:679-690. ArticlePubMed
- 121. Macauley M, Hollingsworth KG, Smith FE, Thelwall PE, Al-Mrabeh A, Schweizer A, Foley JE, Taylor R. Effect of vildagliptin on hepatic steatosis. J Clin Endocrinol Metab 2015;100:1578-1585. ArticlePubMedPMC
- 122. Yilmaz Y, Yonal O, Deyneli O, Celikel CA, Kalayci C, Duman DG. Effects of sitagliptin in diabetic patients with nonalcoholic steatohepatitis. Acta Gastroenterol Belg 2012;75:240-244. PubMed
- 123. Cui J, Philo L, Nguyen P, Hofflich H, Hernandez C, Bettencourt R, Richards L, Salotti J, Bhatt A, Hooker J, Haufe W, Hooker C, Brenner DA, Sirlin CB, Loomba R. Sitagliptin vs. placebo for non-alcoholic fatty liver disease: a randomized controlled trial. J Hepatol 2016;65:369-376. ArticlePubMedPMC
- 124. Kato H, Nagai Y, Ohta A, Tenjin A, Nakamura Y, Tsukiyama H, Sasaki Y, Fukuda H, Ohshige T, Terashima Y, Sada Y, Kondo A, Sasaoka T, Tanaka Y. Effect of sitagliptin on intrahepatic lipid content and body fat in patients with type 2 diabetes. Diabetes Res Clin Pract 2015;109:199-205. ArticlePubMed
- 125. Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, Neuschwander-Tetri BA, Lavine JE, Tonascia J, Unalp A, Van Natta M, Clark J, Brunt EM, Kleiner DE, Hoofnagle JH, Robuck PR. NASH CRN. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med 2010;362:1675-1685. ArticlePubMedPMC
- 126. Loomba R, Sirlin CB, Ang B, Bettencourt R, Jain R, Salotti J, Soaft L, Hooker J, Kono Y, Bhatt A, Hernandez L, Nguyen P, Noureddin M, Haufe W, Hooker C, Yin M, Ehman R, Lin GY, Valasek MA, Brenner DA, Richards L. San Diego Integrated NAFLD Research Consortium (SINC). Ezetimibe for the treatment of nonalcoholic steatohepatitis: assessment by novel magnetic resonance imaging and magnetic resonance elastography in a randomized trial (MOZART trial). Hepatology 2015;61:1239-1250. ArticlePubMedPMCPDF
- 127. Laurin J, Lindor KD, Crippin JS, Gossard A, Gores GJ, Ludwig J, Rakela J, McGill DB. Ursodeoxycholic acid or clofibrate in the treatment of non-alcohol-induced steatohepatitis: a pilot study. Hepatology 1996;23:1464-1467. ArticlePubMed
- 128. Dufour JF, Oneta CM, Gonvers JJ, Bihl F, Cerny A, Cereda JM, Zala JF, Helbling B, Steuerwald M, Zimmermann A. Swiss Association for the Study of the Liver. Randomized placebo-controlled trial of ursodeoxycholic acid with vitamin E in nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 2006;4:1537-1543. ArticlePubMed
- 129. Lindor KD, Kowdley KV, Heathcote EJ, Harrison ME, Jorgensen R, Angulo P, Lymp JF, Burgart L, Colin P. Ursodeoxycholic acid for treatment of nonalcoholic steatohepatitis: results of a randomized trial. Hepatology 2004;39:770-778. ArticlePubMed
- 130. Leuschner UF, Lindenthal B, Herrmann G, Arnold JC, Rossle M, Cordes HJ, Zeuzem S, Hein J, Berg T. NASH Study Group. High-dose ursodeoxycholic acid therapy for nonalcoholic steatohepatitis: a double-blind, randomized, placebo-controlled trial. Hepatology 2010;52:472-479. ArticlePubMed
- 131. Zein CO, Yerian LM, Gogate P, Lopez R, Kirwan JP, Feldstein AE, McCullough AJ. Pentoxifylline improves nonalcoholic steatohepatitis: a randomized placebo-controlled trial. Hepatology 2011;54:1610-1619. ArticlePubMedPMC
- 132. Van Wagner LB, Koppe SW, Brunt EM, Gottstein J, Gardikiotes K, Green RM, Rinella ME. Pentoxifylline for the treatment of non-alcoholic steatohepatitis: a randomized controlled trial. Ann Hepatol 2011;10:277-286. ArticlePubMed
- 133. Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, Chalasani N, Dasarathy S, Diehl AM, Hameed B, Kowdley KV, McCullough A, Terrault N, Clark JM, Tonascia J, Brunt EM, Kleiner DE, Doo E. NASH Clinical Research Network. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet 2015;385:956-965. ArticlePubMed
- 134. Malaguarnera M, Gargante MP, Russo C, Antic T, Vacante M, Malaguarnera M, Avitabile T, Li Volti G, Galvano F. L-carnitine supplementation to diet: a new tool in treatment of nonalcoholic steatohepatitis. A randomized and controlled clinical trial. Am J Gastroenterol 2010;105:1338-1345. ArticlePubMedPDF
- 135. Bae JC, Lee WY, Yoon KH, Park JY, Son HS, Han KA, Lee KW, Woo JT, Ju YC, Lee WJ, Cho YY, Lee MK. Improvement of nonalcoholic fatty liver disease with carnitine-orotate complex in type 2 diabetes (CORONA): a randomized controlled trial. Diabetes Care 2015;38:1245-1252. ArticlePubMedPDF
- 136. Ratziu V, Harrison SA, Francque S, Bedossa P, Lehert P, Serfaty L, Romero-Gomez M, Boursier J, Abdelmalek M, Caldwell S, Drenth J, Anstee QM, Hum D, Hanf R, Roudot A, Megnien S, Staels B, Sanyal A. GOLDEN-505 Investigator Study Group. Elafibranor, an agonist of the peroxisome proliferator-activated receptor-α and -δ, induces resolution of nonalcoholic steatohepatitis without fibrosis worsening. Gastroenterology 2016;150:1147-1159. ArticlePubMed
- 137. Friedman SL, Ratziu V, Harrison SA, Abdelmalek MF, Aithal GP, Caballeria J, Francque S, Farrell G, Kowdley KV, Craxi A, Simon K, Fischer L, Melchor-Khan L, Vest J, Wiens BL, Vig P, Seyedkazemi S, Goodman Z, Wong VW, Loomba R, Tacke F, Sanyal A, Lefebvre E. A randomized, placebo-controlled trial of cenicriviroc for treatment of nonalcoholic steatohepatitis with fibrosis. Hepatology 2018;67:1754-1767. ArticlePubMedPMCPDF
- 138. Zelber-Sagi S, Kessler A, Brazowsky E, Webb M, Lurie Y, Santo M, Leshno M, Blendis L, Halpern Z, Oren R. A double-blind randomized placebo-controlled trial of orlistat for the treatment of nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2006;4:639-644. ArticlePubMed
- 139. Harrison SA, Fecht W, Brunt EM, Neuschwander-Tetri BA. Orlistat for overweight subjects with nonalcoholic steatohepatitis: a randomized, prospective trial. Hepatology 2009;49:80-86. ArticlePubMed
- 140. Bower G, Toma T, Harling L, Jiao LR, Efthimiou E, Darzi A, Athanasiou T, Ashrafian H. Bariatric surgery and non-alcoholic fatty liver disease: a systematic review of liver biochemistry and histology. Obes Surg 2015;25:2280-2289. ArticlePubMedPDF
- 141. Lee Y, Doumouras AG, Yu J, Brar K, Banfield L, Gmora S, Anvari M, Hong D. Complete resolution of nonalcoholic fatty liver disease after bariatric surgery: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2019;17:1040-1060. ArticlePubMed
- 142. Jan A, Narwaria M, Mahawar KK. A systematic review of bariatric surgery in patients with liver cirrhosis. Obes Surg 2015;25:1518-1526. ArticlePubMedPDF
- 143. Seo MH, Lee WY, Kim SS, Kang JH, Kang JH, Kim KK, Kim BY, Kim YH, Kim WJ, Kim EM, Kim HS, Shin YA, Shin HJ, Lee KR, Lee KY, Lee SY, Lee SK, Lee JH, Lee CB, Chung S, Cho YH, Choi KM, Han JS, Yoo SJ. Committee of Clinical Practice Guidelines, Korean Society for the Study of Obesity (KSSO). 2018 Korean Society for the Study of Obesity Guideline for the management of obesity in Korea. J Obes Metab Syndr 2019;28:40-45. ArticlePubMedPMC
REFERENCES
Algorithm for non-alcoholic fatty liver disease (NAFLD) evaluation. CV, cardiovascular; NFS, NAFLD fibrosis score; BMI, body mass index; IFG, impaired fasting glucose; DM, diabetes mellitus; AST, aspartate aminotransferase; ALT, alanine aminotransferase; FIB-4, fibrosis-4; PLT, platelet; APRI, AST to platelet ratio index; ULN, upper limit of normal; VCTE, vibration-controlled transient elastography; ELF, enhanced liver fibrosis; MRE, magnetic resonance elastography. aHigher cutoffs for patients aged >65 years, bVariable cutoffs have been suggested. Measured values are affected by body factors, cFurther validation is required.
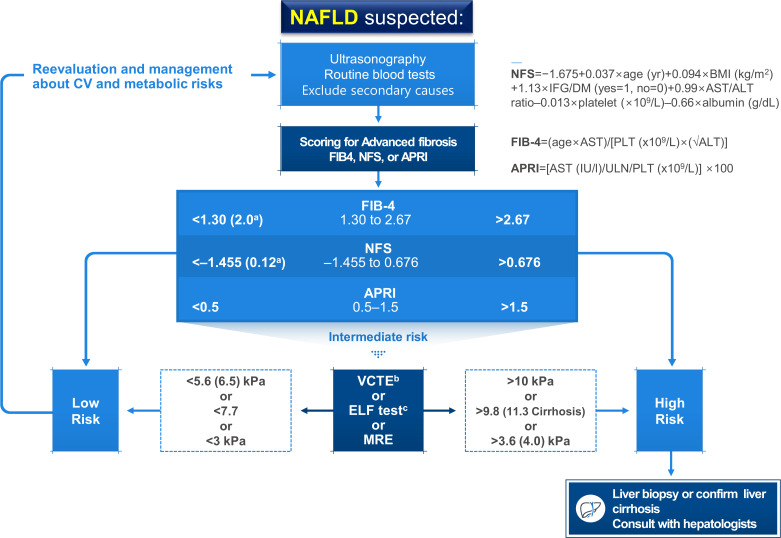
Suggested algorithm for the management of patients with non-alcoholic fatty liver disease (NAFLD) and type 2 diabetes mellitus (T2DM).

The prevalence of NAFLD and NASH in patients with diabetes
| Study | Study population | Diagnostic methods | Categories | Prevalence, % |
|---|---|---|---|---|
| Mohan et al. (2009) [16] | In 132 Indian adults with diabetes | US | NAFLD | 54.5 |
| Kim et al. (2014) [17] | In 4,437 Korean patients with T2DM | US | NAFLD | 72.7 |
| Targher et al. (2007) [18] | In 2,839 Italian patients with T2DM | US | NAFLD | 69.5 |
| Portillo-Sanchez et al. (2015) [11] | In 103 American patients with diabetes with normal plasma aminotransferases | 1H-MRS | NAFLD | 50 |
| Williams et al. (2011) [13] | In 54 biopsied patients with diabetes | Liver biopsy | NASH | 22 |
| Hyysalo et al. (2014) [12] | In 115 biopsied participants in in the Finnish population-based D2D-study | Liver biopsy | NASH | 17.6 |
| Kim et al. (2014) [15] | In 929 Korean patients with diabetes | US | NAFLD | 63.3 |
Summary of the currently used imaging devices for the quantification of hepatic steatosis and fibrosis
US, ultrasonography; CT, computed tomography; MRI-PDFF, magnetic resonance imaging-proton density fat fraction; 1H-MRS, proton magnetic resonance spectroscopy; CAP, controlled attenuation parameter; VCTE, vibration-controlled transient elastography; BMI, body mass index; MRE, magnetic resonance elastography; LSM, liver stiffness measurement.
Figure & Data
References
Citations
- A combined extract containing Schisandra chinensis (SCE) reduced hepatic triglyceride accumulation in rats fed a high-sucrose diet
Haneul Lee, Eun Young Kang, Joowon Lee, Yejin Kim, Sumin Kang, Hayoon Kim, Hyun Kyung Kim, Gyoungok Gang, Sang-gil Lee, Cao Lei, Gwang-woong Go
Food Science and Biotechnology.2024; 33(6): 1449. CrossRef - Association of non-alcoholic fatty liver disease with cardiovascular disease and all cause death in patients with type 2 diabetes mellitus: nationwide population based study
Kyung-Soo Kim, Sangmo Hong, Kyungdo Han, Cheol-Young Park
BMJ.2024; : e076388. CrossRef - Risk Scores for Prediction of Major Cardiovascular Events in Non-Alcoholic Fatty Liver Disease: A No Man’s Land?
Liliana Gheorghe, Roxana Nemteanu, Andreea Clim, Gina Eosefina Botnariu, Irina Iuliana Costache, Alina Plesa
Life.2023; 13(4): 857. CrossRef - Increased expression of sodium-glucose cotransporter 2 and O-GlcNAcylation in hepatocytes drives non-alcoholic steatohepatitis
Hye Jin Chun, Eun Ran Kim, Minyoung Lee, Da Hyun Choi, Soo Hyun Kim, Eugene Shin, Jin-Hong Kim, Jin Won Cho, Dai Hoon Han, Bong-Soo Cha, Yong-ho Lee
Metabolism.2023; 145: 155612. CrossRef - Association between fatty liver index and risk of end-stage renal disease stratified by kidney function in patients with type 2 diabetes: A nationwide population-based study
Goh Eun Chung, Kyungdo Han, Kyu-Na Lee, Jung Ho Bae, Sun Young Yang, Su-Yeon Choi, Jeong Yoon Yim, Nam Ju Heo
Diabetes & Metabolism.2023; 49(4): 101454. CrossRef - Comparison of glucagon-like peptide-1 receptor agonists and thiazolidinediones on treating nonalcoholic fatty liver disease: A network meta-analysis
Min Jeong Park, Hayeon Kim, Myeong Gyu Kim, Kyungim Kim
Clinical and Molecular Hepatology.2023; 29(3): 693. CrossRef - Histological analysis of hypoglycemic agents on liver fibrosis in patients with non-alcoholic fatty liver disease: a systematic review
Qingxing Xie, Xiaohui Pan, Xinyue Zhang, Jinfang Ma, Ge Peng, Nanwei Tong
Chinese Medical Journal.2023; 136(16): 2014. CrossRef - Hepatotropc effects of glucose-lowering drugs: non-alcoholic fatty liver disease in focus
E. V. Uzhakova, Z. E. Zshanko, E. N. Smirnova
Experimental and Clinical Gastroenterology.2023; (6): 121. CrossRef - Complementary effects of dapagliflozin and lobeglitazone on metabolism in a diet-induced obese mouse model
Yun Kyung Lee, Tae Jung Oh, Ji In Lee, Bo Yoon Choi, Hyen Chung Cho, Hak Chul Jang, Sung Hee Choi
European Journal of Pharmacology.2023; 957: 175946. CrossRef - Hepatic T-cell senescence and exhaustion are implicated in the progression of fatty liver disease in patients with type 2 diabetes and mouse model with nonalcoholic steatohepatitis
Byeong Chang Sim, Yea Eun Kang, Sun Kyoung You, Seong Eun Lee, Ha Thi Nga, Ho Yeop Lee, Thi Linh Nguyen, Ji Sun Moon, Jingwen Tian, Hyo Ju Jang, Jeong Eun Lee, Hyon-Seung Yi
Cell Death & Disease.2023;[Epub] CrossRef - 2023 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association
Jong Han Choi, Kyung Ae Lee, Joon Ho Moon, Suk Chon, Dae Jung Kim, Hyun Jin Kim, Nan Hee Kim, Ji A Seo, Mee Kyoung Kim, Jeong Hyun Lim, YoonJu Song, Ye Seul Yang, Jae Hyeon Kim, You-Bin Lee, Junghyun Noh, Kyu Yeon Hur, Jong Suk Park, Sang Youl Rhee, Hae J
Diabetes & Metabolism Journal.2023; 47(5): 575. CrossRef - Circ_0004535/miR-1827/CASP8 network involved in type 2 diabetes mellitus with nonalcoholic fatty liver disease
Min Li, Ai Zeng, Xinle Tang, Hui Xu, Wei Xiong, Yanying Guo
Scientific Reports.2023;[Epub] CrossRef - Stratification by obesity class, rather than age, can identify a higher percent of children at risk for non‐alcoholic fatty liver disease and metabolic dysfunction
Aurelia Radulescu, Adam J. Dugan, Mary Killian, Suzanna L. Attia, Marialena Mouzaki, George J. Fuchs, Rohit Kohli, Henrietta Bada, Philip A. Kern, Samir Softic
Pediatric Obesity.2022;[Epub] CrossRef - Renal Tubular Damage Marker, Urinary N-acetyl-β-D-Glucosaminidase, as a Predictive Marker of Hepatic Fibrosis in Type 2 Diabetes Mellitus
Hae Kyung Kim, Minyoung Lee, Yong-ho Lee, Eun Seok Kang, Bong-Soo Cha, Byung-Wan Lee
Diabetes & Metabolism Journal.2022; 46(1): 104. CrossRef - Dulaglutide Ameliorates Palmitic Acid-Induced Hepatic Steatosis by Activating FAM3A Signaling Pathway
Jinmi Lee, Seok-Woo Hong, Min-Jeong Kim, Sun Joon Moon, Hyemi Kwon, Se Eun Park, Eun-Jung Rhee, Won-Young Lee
Endocrinology and Metabolism.2022; 37(1): 74. CrossRef - State-of-the-Art Overview of the Pharmacological Treatment of Non-Alcoholic Steatohepatitis
Yongin Cho, Yong-ho Lee
Endocrinology and Metabolism.2022; 37(1): 38. CrossRef - Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: an open-label randomized controlled trial (ESSENTIAL study)
Yongin Cho, Hyungjin Rhee, Young-eun Kim, Minyoung Lee, Byung-Wan Lee, Eun Seok Kang, Bong-Soo Cha, Jin-Young Choi, Yong-ho Lee
BMC Medicine.2022;[Epub] CrossRef - Obesity is an important determinant of severity in newly defined metabolic dysfunction-associated fatty liver disease
Ji Hye Huh, Kwang Joon Kim, Seung Up Kim, Bong-Soo Cha, Byung-Wan Lee
Hepatobiliary & Pancreatic Diseases International.2022; 21(3): 241. CrossRef - Anti-Obesity and Anti-Hyperglycemic Effects of Meretrix lusoria Protamex Hydrolysate in ob/ob Mice
Min Ju Kim, Ramakrishna Chilakala, Hee Geun Jo, Seung-Jae Lee, Dong-Sung Lee, Sun Hee Cheong
International Journal of Molecular Sciences.2022; 23(7): 4015. CrossRef - The associations of hepatic steatosis and fibrosis using fatty liver index and BARD score with cardiovascular outcomes and mortality in patients with new-onset type 2 diabetes: a nationwide cohort study
Jiyun Park, Gyuri Kim, Bong-Sung Kim, Kyung-Do Han, So Yoon Kwon, So Hee Park, You-Bin Lee, Sang-Man Jin, Jae Hyeon Kim
Cardiovascular Diabetology.2022;[Epub] CrossRef - Cumulative Exposure to High γ-Glutamyl Transferase Level and Risk of Diabetes: A Nationwide Population-Based Study
Ji-Yeon Park, Kyungdo Han, Hun-Sung Kim, Jae-Hyoung Cho, Kun-Ho Yoon, Mee Kyoung Kim, Seung-Hwan Lee
Endocrinology and Metabolism.2022; 37(2): 272. CrossRef - SGLT-2 inhibitors and GLP-1 receptor agonists in metabolic dysfunction-associated fatty liver disease
Jun Sung Moon, Jun Hwa Hong, Yong Jin Jung, Ele Ferrannini, Michael A. Nauck, Soo Lim
Trends in Endocrinology & Metabolism.2022; 33(6): 424. CrossRef - Plasma Aldo-Keto Reductase Family 1 Member B10 as a Biomarker Performs Well in the Diagnosis of Nonalcoholic Steatohepatitis and Fibrosis
Aron Park, Seung Joon Choi, Sungjin Park, Seong Min Kim, Hye Eun Lee, Minjae Joo, Kyoung Kon Kim, Doojin Kim, Dong Hae Chung, Jae Been Im, Jaehun Jung, Seung Kak Shin, Byung-Chul Oh, Cheolsoo Choi, Seungyoon Nam, Dae Ho Lee
International Journal of Molecular Sciences.2022; 23(9): 5035. CrossRef - Chinese Herbal Medicine for Type 2 Diabetes Mellitus With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis
Sihan Peng, Lu Liu, Ziyan Xie, Xiyu Zhang, Chunguang Xie, Sha Ye, Xiangeng Zhang, Xiaoli Liang, Hongyan Wang, Ya Liu
Frontiers in Pharmacology.2022;[Epub] CrossRef - Non-alcoholic fatty liver disease and sarcopenia is associated with the risk of albuminuria independent of insulin resistance, and obesity
Eugene Han, Mi Kyung Kim, Seung-Soon Im, Byoung Kuk Jang, Hye Soon Kim
Journal of Diabetes and its Complications.2022; 36(8): 108253. CrossRef - Extra-Glycemic Effects of Anti-Diabetic Medications: Two Birds with One Stone?
Eun-Jung Rhee
Endocrinology and Metabolism.2022; 37(3): 415. CrossRef - Plasma Metabolomics and Machine Learning-Driven Novel Diagnostic Signature for Non-Alcoholic Steatohepatitis
Moongi Ji, Yunju Jo, Seung Joon Choi, Seong Min Kim, Kyoung Kon Kim, Byung-Chul Oh, Dongryeol Ryu, Man-Jeong Paik, Dae Ho Lee
Biomedicines.2022; 10(7): 1669. CrossRef - Association Between DPP4 Inhibitor Use and the Incidence of Cirrhosis, ESRD, and Some Cancers in Patients With Diabetes
Yewon Na, Soo Wan Kim, Ie Byung Park, Soo Jung Choi, Seungyoon Nam, Jaehun Jung, Dae Ho Lee
The Journal of Clinical Endocrinology & Metabolism.2022; 107(11): 3022. CrossRef - Nonalcoholic fatty liver disease is associated with early left ventricular diastolic dysfunction in patients with type 2 diabeteS
Walaa Sheba, Eman Morsy, Salah Altahan, Mona Ayaad, Sameh A. Lashen
Alexandria Journal of Medicine.2022; 58(1): 117. CrossRef - The association between changes in hepatic steatosis and hepatic fibrosis with cardiovascular outcomes and mortality in patients with New-Onset type 2 Diabetes: A nationwide cohort study
Jiyun Park, Gyuri Kim, Bong-Sung Kim, Kyung-Do Han, So Yoon Kwon, So Hee Park, You-Bin Lee, Sang-Man Jin, Jae Hyeon Kim
Diabetes Research and Clinical Practice.2022; 194: 110191. CrossRef - Advanced Liver Fibrosis Is Associated with Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease (Diabetes Metab J 2022;46:630-9)
Ji Hye Huh
Diabetes & Metabolism Journal.2022; 46(6): 953. CrossRef - The association of fatty liver index and BARD score with all-cause and cause-specific mortality in patients with type 2 diabetes mellitus: a nationwide population-based study
Goh Eun Chung, Su-Min Jeong, Eun Ju Cho, Ji Won Yoon, Jeong-Ju Yoo, Yuri Cho, Kyu-na Lee, Dong Wook Shin, Yoon Jun Kim, Jung-Hwan Yoon, Kyungdo Han, Su Jong Yu
Cardiovascular Diabetology.2022;[Epub] CrossRef - Non-Albumin Proteinuria (NAP) as a Complementary Marker for Diabetic Kidney Disease (DKD)
Jaehyun Bae, Young Jun Won, Byung-Wan Lee
Life.2021; 11(3): 224. CrossRef - Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease: Diagnosis and Treatment
Sook Jung Lee, Byung-Wan Lee
The Journal of Korean Diabetes.2021; 22(1): 38. CrossRef - Non-alcoholic fatty liver disease
Elizabeth E Powell, Vincent Wai-Sun Wong, Mary Rinella
The Lancet.2021; 397(10290): 2212. CrossRef - Allopurinol ameliorates high fructose diet induced hepatic steatosis in diabetic rats through modulation of lipid metabolism, inflammation, and ER stress pathway
In-Jin Cho, Da-Hee Oh, Jin Yoo, You-Cheol Hwang, Kyu Jeung Ahn, Ho-Yeon Chung, Soung Won Jeong, Ju-Young Moon, Sang-Ho Lee, Sung-Jig Lim, In-Kyung Jeong
Scientific Reports.2021;[Epub] CrossRef - Patient Management in Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus
A. E. Bagriy, A. D. Zubov, M. V. Khomenko, E. S. Mikhailichenko, E. A. Pylaeva, N. A. Khaustova, E. V. Bryukhovetskaya
Russian Journal of Gastroenterology, Hepatology, Coloproctology.2021; 31(2): 14. CrossRef - Liver Fibrosis Indices for the Prediction of Mortality in Korean Subjects: A 16-Year Prospective Cohort Study
Tae Jung Oh, Kyuho Kim, Jae Hoon Moon, Sung Hee Choi, Nam H Cho, Hak Chul Jang
Journal of the Endocrine Society.2021;[Epub] CrossRef - Reduced Rank Regression-Derived Dietary Patterns Related to the Fatty Liver Index and Associations with Type 2 Diabetes Mellitus among Ghanaian Populations under Transition: The RODAM Study
Tracy Bonsu Osei, Anne-Marieke van Dijk, Sjoerd Dingerink, Felix Patience Chilunga, Erik Beune, Karlijn Anna Catharina Meeks, Silver Bahendeka, Matthias Bernd Schulze, Charles Agyemang, Mary Nicolaou, Adriaan Georgius Holleboom, Ina Danquah
Nutrients.2021; 13(11): 3679. CrossRef - Efficacy and Safety of GLP-1 Receptor Agonists in Patients With Type 2 Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis
Yuan Zhu, Jiao Xu, Dong Zhang, Xingyu Mu, Yi Shi, Shangtao Chen, Zengxiang Wu, Shuangqing Li
Frontiers in Endocrinology.2021;[Epub] CrossRef - Liver fibrosis indices are related to diabetic peripheral neuropathy in individuals with type 2 diabetes
Kyuho Kim, Tae Jung Oh, Hyen Chung Cho, Yun Kyung Lee, Chang Ho Ahn, Bo Kyung Koo, Jae Hoon Moon, Sung Hee Choi, Hak Chul Jang
Scientific Reports.2021;[Epub] CrossRef - Evaluation of Grapefruit Juice in terms of Interleukin 18 Gene Expression in Rats with Fatty Liver and Healthy Rats
Simin Bahmanpoor, Noosha Zia-Jahromi
journal of ilam university of medical sciences.2021; 29(4): 74. CrossRef
 PubReader
PubReader Cite
Cite- Figure
-


- Related articles
-
- 2023 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association
- Non-Alcoholic Fatty Liver Disease with Sarcopenia and Carotid Plaque Progression Risk in Patients with Type 2 Diabetes Mellitus
- Advanced Liver Fibrosis Is Associated with Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease (Diabetes Metab J 2022;46:630-9)
- Advanced Liver Fibrosis Is Associated with Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease (Diabetes Metab J 2022;46:630-9)
- Screening for Prediabetes and Diabetes in Korean Nonpregnant Adults: A Position Statement of the Korean Diabetes Association, 2022



