
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(6); 2011 > Article
-
ReviewCosts of Diabetes Mellitus in Korea
- Kwan Woo Lee
-
Diabetes & Metabolism Journal 2011;35(6):567-570.
DOI: https://doi.org/10.4093/dmj.2011.35.6.567
Published online: December 26, 2011
Department of Endocrinology and Metabolism, Ajou University School of Medicine, Suwon, Korea.
- Corresponding author: Kwan Woo Lee. Department of Endocrinology and Metabolism, Ajou University School of Medicine, San 5 Woncheon-dong, Yeongtong-gu, Suwon 443-721, Korea. LKW65@ajou.ac.kr
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Outcome research focusing on the economics of the medical field began in the mid-1990s and has included studies about costs, cost effectiveness, and policies. According to the American Diabetes Association, the total estimated cost of diabetes in 2007 was $174 billion. The economic burden of patients with diabetes in Canada is expected to be about $12.2 billion in 2010. Recent Korean studies have analyzed the expenses associated with type 2 diabetes for patients in selected general hospitals. Type 2 diabetic patients without complications cost approximately 1,184,563 won (the equivalent of US $1,184) per patient for healthcare annually. In contrast, patients with microvascular disease due to diabetic complications cost up to 4.7 times that amount, and patients with macrovascular disease incur up to 10.7 times the annual costs for patients without diabetic complications. Diabetic complications ultimately impact the quality of life for patients and patient mortality, and are associated with higher direct medical expenses for patients. To avoid increased medical costs, appropriate management techniques must be implemented to ensure timely care for patients with diabetes.
- Diabetes is a serious problem in medical care, health care, and social epidemiology worldwide. The prevalence of diabetes in both advanced and developing countries has increased over the last three decades, as a direct result of increasing population, longer life expectancy, and the spread of a Western lifestyle. These factors have lead to increased incidence, higher prevalence rates, and higher mortality rates due to diabetes [1,2].
- According to the World Health Organization and the International Diabetes Federation, an estimated 135 million patients had diabetes worldwide in 1995. An estimated 194 million people, or 5.1% of the global population between the ages of 20 to 79 years, had diabetes in 2003 [1]. By the year 2025, 300 million people will be affected by diabetes worldwide, an increase of 120% in just 3 decades, according to estimates by both organizations [1]. Studies in Korea in 1972 showed that 1.5% of the population had diabetes. According to the Korean National Health and Nutrition Examination Survey (2005), 9% of males and 7.2% of females among Koreans over the age of 30 years had diabetes [3,4].
INTRODUCTION
- Many studies in the mid-1990s focused on the economic status of people burdened by disease, and these research efforts contributed to the creation, in 1998, of the International Society for Pharmacoeconomics and Outcome Research in Europe [5]. Many studies have explored various aspects of diabetes, including the costs of diabetic care, cost control, and the application of policies that govern care and costs [5-8].
- Cost-effectiveness analysis is a form of economic evaluation applicable only when outcomes are one-dimensional and measured in naturally occurring units such as changes in blood pressure or mortality. As compared with cost effectiveness or cost minimization analyses, cost utility analysis uses a form of economic evaluation that enables broader comparisons between treatments for different disease groups. Using health utilities, multi-dimensional health outcomes are reduced to a single index and expressed as quality adjusted life years (QALYs) and disability adjusted life years of healthy year equivalents. Cost per unit of outcome ratios can then be derived that reflect the costs required to obtain one QALY, which represents 1 year of life without complications for patients burdened by disease. The QALY of patients with diabetes and end stage renal disease is only 0.43 of 1 full year, which numerically represents the decrease in patient quality of life attributable to renal problems associated with diabetes. Cost-benefit analysis is a form of economic evaluation that addresses allocative efficiency questions. Costs and outcomes are valued in a commensurate unit, often money, through techniques such as contingent valuation [5-8].
- Economic costs of disease are classified as direct costs and indirect costs. Direct costs refer specifically to costs associated with direct medical care, hospital outpatient care (OPD), hospital inpatient care (IPD), medication, and consultation. Indirect medical costs include the costs of transportation for hospital visits and caregiver expenses. These types of expenses include both covered services and non-covered services within the Korean National Health Insurance System. Indirect costs include loss of labor and loss of income due to premature death and the costs of medical devices and disposable supplies [5-8].
OUTCOME RESEARCH
- According to the American Diabetes Association, the total estimated cost of diabetes in 2007 was $174 billion, including $116 billion in excess medical expenditures and $58 billion in reduced national productivity. Medical costs attributed to diabetes included $27 billion for directly treating diabetes, $58 billion for treating diabetes-related chronic complications owing to diabetes, and $31 billion for excess general medical costs. The largest components of the medical expenditures were IPD (50% of total cost), diabetes medication and supplies (12%), retail prescriptions to treat complications of diabetes (11%), and physician office visits (9%). People diagnosed with diabetes incur average expenditures of $11,744 per year, of which $6,649 is attributable to diabetes, and have medical expenditures that are 2 to 3 times the expected expenditures in the absence of diabetes [9].
- The economic burden of diabetes in Canada is expected to be about $12.2 billion in 2010, as measured in inflation-adjusted 2005 dollars. This is an increase of $5.9 billion or nearly double compared with the level in 2000. The cost of the disease is expected to rise by another $4.7 billion by 2020. Direct costs of diabetes now account for about 3.5% of public healthcare spending in Canada [10].
- Many studies have shown that the presence of complications has a substantial impact on the costs of managing patients with type 2 diabetes [11-13]. In Europe, the Cost of Diabetes in Europe-Type 2 Diabetes (CODE-2) study, which was conducted with 7,000 patients from 8 different European countries, reported that the number of diabetic patients with microvascular disease or macrovascular disease was 1.7 times or 2 times the number of non-diabetic patients with these diseases, respectively, and in individuals with both microvascular and macrovascular complications, the total cost of management was increased 3.5 fold [11]. The CODE-2 study estimated that 55% of direct medical costs involving patients with diabetes pertain to admission. Moreover, admission costs were mainly related to the treatment of macrovascular complications, including acute myocardial infarction, cerebrovascular infarction, and peripheral artery occlusive disease. Additional money was spent on diagnostic and treatment procedures. When we consider this study, which did not take into account a potential confounding factor, the year in which the complication occurred, we expect to find more pronounced differences in the direct medical costs of the diabetic treatment incurred by diabetic complications [14,15].
- In the CODE-2 study, the prevalence of retinopathy was 20%, whereas the reported incidence of both photocoagulation and vitrectomy was 2%. These findings suggest that the potential for cost savings exists in preventive measures and early retinal screening programs [16].
- According to the Korean Diabetes Association, the total estimated cost of diabetes for adults in 2003 was $11.7 billion, representing 19.1% of the total medical costs for adults [17]. People diagnosed with diabetes have medical expenditures that are 3 times the expenditures in the absence of diabetes [17].
- The economic burden of diabetes in Korea has been studied, and Korea has the most current reports of disease costs for patients with diabetes [18-20]. Fig. 1 shows that the average annual medical costs per patient in Korea were 6,994,415 won (US $6,994) during 2005 [19]. The annual medical costs per patient with microvascular disease and macrovascular disease were 5,546,521 won (US $5,547) and 12,631,592 won (US $12,632), respectively. The annual medical costs per patient with both types of vascular complications were 10,477,356 won (US $10,477). The annual medical costs per patient with microvascular disease, macrovascular disease, or both were 4.7, 10.7, or 8.8 times the annual medical costs per patient without complications (1,184,563 won, or US $1,185).
- Among patients with complications, the costs for OPD and medications were moderately increased to 1.6 to 4.8 times the costs for patients without complications. In contrast, IPD costs were increased approximately 18.9-fold for microvascular disease and 61- to 78.9-fold for macrovascular disease. In Korea, as in other countries where cost analyses have been conducted, patients with diabetic complications tend to have higher costs than patients without complications. Higher costs due to macrovascular complications are particularly prominent for patients in Korea, according to current studies [18-20].
- For patients without diabetic complications, the total cost of the disease comprises OPD and medication costs. In contrast, the total cost of the disease also includes hospital admissions for patients with complications. Among patients admitted to hospitals with macrovascular disease, 65% to 70% of their total expenditures result from admission costs. After the analysis of covariance in this study was adjusted for age and gender, medical costs were found to increase according to the presence of complications, independent of age and gender (P<0.001) [19].
- According to this study, the diabetic complications costing patients the highest annual amounts are nephropathy with end stage renal disease and kidney transplantation, at costs of 24,871,318 won (US $24,871) and 27,361,088 won (US $27,361), respectively. The next highest costs are due to coronary artery disease with percutaneous transluminal coronary angioplasty or coronary artery bypass graft (14,679,647 won, or US $14,680) and diabetic foot amputation (13,960,314 won, or US $13,960). The costs for diabetic patients with non-proliferative retinopathy are 3 times the costs for patients without complications, and the costs for patients with proliferative retinopathy who receive surgery are up to 6.1 times the costs for patients without complications. The costs for diabetic nephropathy vary based on the stage of nephropathy. For diabetic patients who develop microalbuminuria or proteinuria, the costs are 1.3 or 2.4 times the costs for diabetic patients without complications. Diabetic patients who must receive hemodialysis or kidney transplantation incur costs that are 21 or 23.1 times the costs for diabetic patients without complications. Similarly, the costs for diabetic patients with coronary artery disease, stroke, or coronary artery obstructive disease with percutaneous transluminal coronary angioplasty or coronary artery bypass graft are 5.2, 5.3, or 12.4 times the costs for diabetic patients without complications, and the costs due to foot amputation are 11.8-fold [19].
COSTS OF DIABETES
- Complications affect the quality of life and mortality of patients with diabetes and are associated with higher direct medical costs. Accordingly, to avoid increased medical costs, appropriate management techniques must be implemented to ensure timely care for patients with diabetes. As outlined in medical care policies, adequate control of blood sugar, blood pressure, and cholesterol in conjunction with early detection of complications through appropriate screening are critical.
CONCLUSION
- 1. Gan D. International Diabetes Federation. World Diabetes Foundation. Diabetes atlas. 2003. 2nd ed. Brussels: International Diabetes Federation; p. 15-71.
- 2. Bjork S. The cost of diabetes and diabetes care. Diabetes Res Clin Pract 2001;54(Suppl 1):S13-S18. PubMed
- 3. Kim KS, Choi CH, Lee DY, Kim EJ. Epidemiological study on diabetes mellitus among rural Korean. J Korean Diabetes Assoc 1972;1:17-24.
- 4. Korea Centers for Disease Control and Prevention. The Third Korea National Health and Nutrition Examination Survey (KNHANES III), 2005: illness of adults. 2006. Seoul: Korea Centers for Disease Control and Prevention.
- 5. Annemans L. Pharmacoeconomics for decision makers. Paper presented at: ISPOR 10th Annual European Congress 2007 Oct 20-23; Dublin, IE.
- 6. Shiell A, Donaldson C, Mitton C, Currie G. Health economic evaluation. J Epidemiol Community Health 2002;56:85-88. ArticlePubMedPMC
- 7. Zhang P, Engelgau MM, Norris SL, Gregg EW, Narayan KM. Application of economic analysis to diabetes and diabetes care. Ann Intern Med 2004;140:972-977. ArticlePubMed
- 8. Rascati KL, Drummond MF, Annemans L, Davey PG. Education in pharmacoeconomics: an international multidisciplinary view. Pharmacoeconomics 2004;22:139-147. ArticlePubMed
- 9. American Diabetes Association. Economic costs of diabetes in the U.S. In 2007. Diabetes Care 2008;31:596-615. ArticlePubMedPDF
- 10. Canadian Diabetes Association: An economic tsunami: the cost of diabetes in Canada updated 2009 Dec. Available from: http://www.diabetes.ca/documents/get-involved/FINAL_Economic_Report.pdf.
- 11. Williams R, Van Gaal L, Lucioni C. CODE-2 Advisory Board. Assessing the impact of complications on the costs of type II diabetes. Diabetologia 2002;45:S13-S17. ArticlePDF
- 12. Brandle M, Zhou H, Smith BR, Marriott D, Burke R, Tabaei BP, Brown MB, Herman WH. The direct medical cost of type 2 diabetes. Diabetes Care 2003;26:2300-2304. ArticlePubMedPDF
- 13. Clarke P, Gray A, Legood R, Briggs A, Holman R. The impact of diabetes-related complications on healthcare costs: results from the United Kingdom Prospective Diabetes Study (UKPDS Study No. 65). Diabet Med 2003;20:442-450. ArticlePubMed
- 14. O'Brien JA, Patrick AR, Caro JJ. Cost of managing complications resulting from type 2 diabetes mellitus in Canada. BMC Health Serv Res 2003;3:7ArticlePubMedPMCPDF
- 15. Caro JJ, Ward AJ, O'Brien JA. Lifetime costs of complications resulting from type 2 diabetes in the U.S. Diabetes Care 2002;25:476-481. ArticlePubMedPDF
- 16. American Diabetes Association. Standards of medical care in diabetes--2006. Diabetes Care 2006;29(Suppl 1):S4-S42. ArticlePubMedPDF
- 17. Task Force Team for Basic Statistical Study of Korean Diabetes Mellitus. Report of Task Force Team for Basic Statistical Study of Korean Diabetes Mellitus: diabetes in Korea 2007. 2007. 1st ed. Seoul: Goldfishery.
- 18. Moon EJ, Jo YE, Park TC, Kim YK, Jung SH, Kim HJ, Kim DJ, Chung YS, Lee KW. Clinical characteristics and direct medical costs of type 2 diabetic patients. Korean Diabetes J 2008;32:358-365.Article
- 19. Hwang JA, Park TC, Jung SH, Kim HJ, Kim DJ, Kim SH, Nam MS, Kim TH, Lee MK, Lee KW. Direct medical costs of type 2 diabetic patients in the tertiary hospital. Korean Diabetes J 2008;32:259-268.Article
- 20. Chun KH, Lee KW, Kim DJ, Kim HJ, Paek KW, Lee SJ. An analysis of medical costs of diabetic patients in a university hospital (1996~2005). Korean Diabetes J 2008;32:366-376.Article
REFERENCES
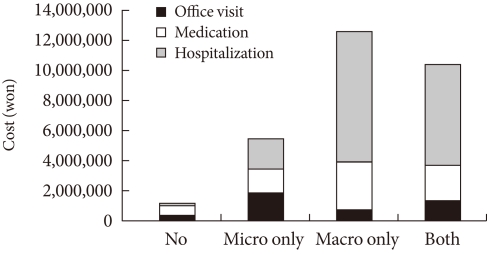
Figure & Data
References
Citations
Citations to this article as recorded by 
- Effect of Mori ramulus on the postprandial blood glucose levels and inflammatory responses of healthy subjects subjected to an oral high-fat/sucrose challenge: A double-blind, randomized, crossover clinical trial
Soo-yeon Park, Oran Kwon, Ji Yeon Kim
Biomedicine & Pharmacotherapy.2022; 146: 112552. CrossRef - Healthcare resource utilization in patients treated with empagliflozin in East Asia
Wayne H‐H Sheu, Yutaka Seino, Elise Chia‐Hui Tan, Daisuke Yabe, Kyoung Hwa Ha, Masaomi Nangaku, Wook‐Jin Chung, Koichi Node, Atsutaka Yasui, Wei‐Yu Lei, Sunwoo Lee, Anastasia Ustyugova, Riho Klement, Anouk Deruaz‐Luyet, Moe H Kyaw, Dae Jung Kim
Journal of Diabetes Investigation.2022; 13(5): 810. CrossRef - Effects of Jerusalem Artichoke Extract and Inulin on Blood Glucose Levels and Insulin Secretion in Streptozotocin Induced Diabetic Mice
Seung Hee Kim, Byung Ki Kim, Boo Yeun Park, Jung Min Kim, Young Jik Lee, Mi Kyung Lee, Sung-Tae Yee, Mi Yeon Kang
The Journal of Korean Diabetes.2021; 22(1): 60. CrossRef - Hospital-Based Korean Diabetes Prevention Study: A Prospective, Multi-Center, Randomized, Open-Label Controlled Study
Sang Youl Rhee, Suk Chon, Kyu Jeung Ahn, Jeong-Taek Woo
Diabetes & Metabolism Journal.2019; 43(1): 49. CrossRef - Cost analysis of type 2 diabetes mellitus treatment in economically developed countries
Sara Ramzan, Peter Timmins, Syed Shahzad Hasan, Zaheer-Ud-Din Babar
Expert Review of Pharmacoeconomics & Outcomes Research.2019; 19(1): 5. CrossRef - High hemoglobin levels are associated with decreased risk of diabetic retinopathy in Korean type 2 diabetes
Min-Kyung Lee, Kyung-Do Han, Jae-Hyuk Lee, Seo-Young Sohn, Jee-Sun Jeong, Mee-Kyoung Kim, Ki-Hyun Baek, Ki-Ho Song, Hyuk-Sang Kwon
Scientific Reports.2018;[Epub] CrossRef - Glucose Control in Intensive Care Unit Patients: Recent Updates
Sang Youl Rhee
Journal of Neurocritical Care.2018; 11(2): 81. CrossRef - Delay of insulin initiation in patients with type 2 diabetes mellitus inadequately controlled with oral hypoglycemic agents (analysis of patient‐ and physician‐related factors): A prospective observational DIPP‐FACTOR study in Korea
Sin Gon Kim, Nam Hoon Kim, Bon Jeong Ku, Ho Sang Shon, Doo Man Kim, Tae Sun Park, Yong‐Seong Kim, In Joo Kim, Dong Seop Choi
Journal of Diabetes Investigation.2017; 8(3): 346. CrossRef - Community-based randomized controlled trial of diabetes prevention study for high-risk individuals of type 2 diabetes: lifestyle intervention using web-based system
Seon-Ah Cha, Sun-Young Lim, Kook-Rye Kim, Eun-Young Lee, Borami Kang, Yoon-Hee Choi, Kun-Ho Yoon, Yu-Bae Ahn, Jin-Hee Lee, Seung-Hyun Ko
BMC Public Health.2017;[Epub] CrossRef - Assessment of hospital length of stay and direct costs of type 2 diabetes in Hubei Province, China
Dajie Chen, Shuai Liu, Xiaodong Tan, Qihan Zhao
BMC Health Services Research.2017;[Epub] CrossRef - Can the Direct Medical Cost of Chronic Disease Be Transferred across Different Countries? Using Cost-of-Illness Studies on Type 2 Diabetes, Epilepsy and Schizophrenia as Examples
Lan Gao, Hao Hu, Fei-Li Zhao, Shu-Chuen Li, Terence J Quinn
PLOS ONE.2016; 11(1): e0147169. CrossRef - Effects of mulberry leaf extract on blood glucose and serum lipid profiles in patients with type 2 diabetes mellitus: A systematic review
Seung-Ok Shin, Hyun-Ju Seo, Hyunyoung Park, Hyun Jin Song
European Journal of Integrative Medicine.2016; 8(5): 602. CrossRef - Current Status of Management in Type 2 Diabetes Mellitus at General Hospitals in South Korea
Jin-Hee Jung, Jung-Hwa Lee, Jin-Won Noh, Jeong-Eun Park, Hee-Sook Kim, Joo-Wha Yoo, Bok-Rye Song, Jeong-rim Lee, Myeong-Hee Hong, Hyang-Mi Jang, Young Na, Hyun-Joo Lee, Jeong-Mi Lee, Yang-Gyo Kang, Sun-Young Kim, Kang-Hee Sim
Diabetes & Metabolism Journal.2015; 39(4): 307. CrossRef - It's Still Not Too Late to Make a Change: Current Status of Glycemic Control in Korea
Sang Yong Kim
Diabetes & Metabolism Journal.2014; 38(3): 194. CrossRef - Preserve Common Limb in Duodenal–Jejunal Bypass Surgery Benefits Rats with Type 2-Like Diabetes
Shi-Yun Zhang, Xue-Jun Sun, Jian-Bao Zheng, Wei Wang, Dong Liu, Nan-Zheng Chen, Sai He, Xiong-Wei Huo, Wanli Smith
Obesity Surgery.2014; 24(3): 405. CrossRef - Increased Risk of Diabetes Development in Subjects with the Hypertriglyceridemic Waist Phenotype: A 4-Year Longitudinal Study
Ki Joong Han, Shin Yeoung Lee, Nam Hee Kim, Hyun Beom Chae, Tae Hoon Lee, Choel Min Jang, Kyung Mo Yoo, Hae Jung Park, Min Kyung Lee, Won Seon Jeon, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
Endocrinology and Metabolism.2014; 29(4): 514. CrossRef - Clinical and Economic Outcomes in Medication-Adherent and -Nonadherent Patients With Type 2 Diabetes Mellitus in the Republic of Korea
So-Yeon An, Hae Jin Kim, Ki Hong Chun, Tae Ho Kim, Ja Young Jeon, Dae Jung Kim, Seung Jin Han, Young Seol Kim, Jeong Taek Woo, Kyu Jeung Ahn, Yongsoo Park, Moonsuk Nam, Sei Hyun Baik, Kwan-Woo Lee
Clinical Therapeutics.2014; 36(2): 245. CrossRef - Comparison of Two Creatinine-Based Equations for Predicting Decline in Renal Function in Type 2 Diabetic Patients with Nephropathy in a Korean Population
Eun Young Lee, Young-Mi Lee, Kyu Hun Choi, Hyun Chul Lee, Byung-Wan Lee, Beom Seok Kim
International Journal of Endocrinology.2013; 2013: 1. CrossRef - Diagnostic Accuracy of 64-Slice MDCT Coronary Angiography for the Assessment of Coronary Artery Disease in Korean Patients with Type 2 Diabetes
Jun Sung Moon, Ji Sung Yoon, Kyu Chang Won, Ihn-Ho Cho, Hyoung Woo Lee
Diabetes & Metabolism Journal.2013; 37(1): 54. CrossRef - Severe Hypoglycemia Is a Serious Complication and Becoming an Economic Burden in Diabetes
Won Chul Ha, Su Jin Oh, Ji Hyun Kim, Jung Min Lee, Sang Ah Chang, Tae Seo Sohn, Hyun Shik Son
Diabetes & Metabolism Journal.2012; 36(4): 280. CrossRef - Severe Hypoglycemia in Patients with Diabetes
Jae Seung Yun, Seung-Hyun Ko
Diabetes & Metabolism Journal.2012; 36(4): 273. CrossRef - Intervention Strategies for Older Adults with Diabetes
Sung-Chul Lim
Journal of Korean Diabetes.2012; 13(1): 52. CrossRef
 PubReader
PubReader Cite
Cite



