- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 42(4); 2018 > Article
-
ReviewComplications Diagnosing Diabetic Neuropathy: Something Old, Something New
-
Ioannis N. Petropoulos, Georgios Ponirakis, Adnan Khan, Hamad Almuhannadi, Hoda Gad, Rayaz A. Malik

-
Diabetes & Metabolism Journal 2018;42(4):255-269.
DOI: https://doi.org/10.4093/dmj.2018.0056
Published online: August 21, 2018
Division of Research, Weill Cornell Medicine Qatar, Doha, Qatar.
- Corresponding author: Rayaz A. Malik. Division of Research, Weill Cornell Medicine Qatar, Qatar Foundation, Education City, P.O. Box 24144, Doha, Qatar. ram2045@qatar-med.cornell.edu
Copyright © 2018 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- There are potentially many ways of assessing diabetic peripheral neuropathy (DPN). However, they do not fulfill U.S. Food and Drug Administration (FDA) requirements in relation to their capacity to assess therapeutic benefit in clinical trials of DPN. Over the past several decades symptoms and signs, quantitative sensory and electrodiagnostic testing have been strongly endorsed, but have consistently failed as surrogate end points in clinical trials. Therefore, there is an unmet need for reliable biomarkers to capture the onset and progression and to facilitate drug discovery in DPN. Corneal confocal microscopy (CCM) is a non-invasive ophthalmic imaging modality for in vivo evaluation of sensory C-fibers. An increasing body of evidence from multiple centers worldwide suggests that CCM fulfills the FDA criteria as a surrogate endpoint of DPN.
- The assessment of diabetic peripheral neuropathy (DPN) may be simple or complex and will be defined by what we are trying to achieve. In a busy clinic it is sufficient to establish whether an individual has symptoms, particularly of painful DPN and indeed through the use of a monofilament examination, whether or not the patient is at high risk of foot ulceration. However, for the assessment of early nerve damage and more precise phenotyping of somatic and autonomic neuropathy, a large number of specialized screening and diagnostic tests are available, which can be easily deployed. Clinically however, there is a nihilistic attitude towards diagnosing diabetic neuropathy. After all, apart from providing relief of painful neuropathic symptoms, there are no currently approved disease-modifying therapies. Therein lies another problem in relation to the modalities used to evaluate an improvement in diabetic neuropathy in clinical trials of new therapies. We have witnessed and will continue to witness spectacular and very costly failures of new therapeutics for DPN and indeed other peripheral and central neurodegenerative disorders. This review will consider the pros and cons of old established and newer methods for both diagnosing and evaluating DPN.
INTRODUCTION
- Damage to the small sensory nerve fibers is one of the earliest manifestations of DPN and may be accompanied by continuous or episodic pain [1]. Evaluation of neuropathic symptoms and signs using validated questionnaires and clinical bedside testing form the mainstay of DPN diagnosis along with a detailed history to exclude other possible causes [23]. In this section we summarize the most commonly used clinical diagnostic modalities (Table 1).
- Symptoms and signs
- The Douleur Neuropathique en 4 (DN4) includes questions for different types of neuropathic pain such as burning, painful cold, electrical shocks, tingling, pins and needles, numbness, and itching and a physical exam to test for touch and pin hypoesthesia and tactile dynamic allodynia and has shown excellent sensitivity (83%) and specificity (90%) for neuropathic pain [4]. The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) scale is similar, elicits five symptoms and two signs of DPN and has a comparable sensitivity and specificity [5]. Other screening tests include the Neuropathic Pain Questionnaire (NPQ) (12 questions) [6], the Neuropathic Pain Symptoms Inventory (NPSI) (12 questions) [78], the Neurological Symptom Score (NSS) (17 questions) [9], Diabetic Neuropathy Symptom (DNS) score (four questions) [10]. These are all interview-based assessments of sensory, motor, and autonomic deficits, with moderate sensitivity and specificity. Several screening tests have also been validated to diagnose and stratify the severity of DPN. The Toronto Clinical Neuropathy Score (TCNS) [11] includes an assessment of symptoms (present or absent), sensory loss (normal or abnormal), and reflexes (normal, reduced, or absent). Based on the outcome a score of 6 to 8 denotes mild neuropathy, 9 to 11 moderate, and ≥12 severe neuropathy. The Michigan Neuropathy Screening Instrument (MNSI) consists of 15 self-administered questions adapted from the neuropathy symptom profile [12] and a score ≥7 is considered abnormal [13]. Similar to other clinical composite tests, the MNSI involves a foot examination, whereby each foot with an ulcer or other findings such as dry skin, infections, calluses, fissures, or deformities is scored 1. Other components include testing for vibration sensation using a 128-Hz tuning fork and Achilles reflexes using the Jendrassic manoeuver. The neuropathy disability score (NDS) [14] is a composite measure of vibration perception with a 128-Hz tuning fork, thermal perception with a metallic rod, pin-prick sensation, and Achilles tendon reflexes. The NDS is commonly used in research studies to stratify DPN severity as none (0 to 2), mild (3 to 5), moderate (6 to 8), and severe (9 to 10). The Utah Early Neuropathy Scale (UENS) is designed to identify signs of a predominantly small fiber neuropathy [15]. It consists of pin sensation, allodynia/hyperesthesia, large fiber and deep tendon reflex examinations and motor deficits, with a maximum score of 42.
- Quantitative sensory testing
- Quantitative sensory testing (QST) can be used to quantify small and large nerve fiber function. Commercially available devices include CASE IV (WR Medical Electronics, Stillwater, MN, USA), the thermoaesthesiometer, the biothesiometer, and the TSA II Neurosensory Analyzer (Medoc Ltd., Ramat Yishai, Israel). These devices create temperature and vibratory stimuli and rely on the subject's response to define sensory thresholds. QST is painless and non-invasive, requires minimal training and is relatively easy to perform, which make it an attractive option to diagnose neuropathy. However, several studies have reported variable sensitivity ranging from as low as 36% to 85% [1617], due to the impact of patient co-operation, enrolment of cohorts of different neuropathic severity and the use of different computers and algorithms to perform QST [18]. Early studies reporting poor reproducibility, which improved in subsequent studies [19] possibly due to improved algorithms and devices and taking into account patient reaction time to an external stimulus. The Neuropathy in Diabetes Study group has recommended the use of QST to diagnose DPN in combination with other tests [20], while the American Academy of Neurology considers QST to be of limited use in individual patients but of possible value in longitudinal studies of large cohorts [18]. Indeed, in a study of 498 patients with type 2 diabetes mellitus (T2DM) and 434 controls a significantly elevated warm detection threshold was the most common abnormality, followed by an abnormal cold detection threshold and sural nerve conduction velocity (NCV), which were related to symptoms and glycemic control [21]. However, a detailed study of 59 subjects with and without DPN showed that warm detection thresholds did not differentiate patients with and without symptoms, unlike cold detection threshold and intra-epidermal nerve fiber density (IENFD) [22]. QST has been employed as an outcome measure in clinical trials of neuropathy primarily due to ease of use, but with mixed results [2324]. Indeed, multi-risk factor control in the Steno-2 study [23] failed to show an improvement in DPN measured by vibration perception. In a phase III trial of human recombinant nerve growth factor, QST as a secondary endpoint failed to detect a significant treatment benefit [24].
CLINICAL DIAGNOSIS OF DIABETIC PERIPHERAL NEUROPATHY
- Diabetic autonomic neuropathy (DAN) often coexists with diabetic somatic neuropathy. DAN may affect a number of different organ systems including the cardiovascular, gastrointestinal, genitourinary and sudomotor systems. Cardiovascular autonomic neuropathy (CAN) is clinically the most important form of DAN and is associated with abnormalities of heart rate control and vascular dynamics. Its prevalence varies from 16.8% to 34.3%, and clinical manifestations include resting tachycardia, exercise intolerance, silent myocardial ischemia, and orthostatic hypotension [25]. The most widely used assessments of CAN are based on the time-domain heart rate response to deep breathing, Valsalva manoeuver and change in posture. Gastrointestinal autonomic neuropathy represents a complex disorder that affects gastrointestinal motor and sensory control and leads to esophageal dysmotility, gastroparesis, constipation, diarrhea, and fecal incontinence [26]. It can be assessed with the Diabetes Bowel Symptom Questionnaire [27] and by evaluating gastric emptying using a radionuclide labeled meal [28]. Bladder dysfunction has an estimated prevalence of 25% to 87% [29] and symptoms may include dysuria, nocturia, incomplete bladder emptying, and recurrent urinary tract infections [20]. Assessments for bladder dysfunction include a lower urinary tract symptoms questionnaire, measurement of peak urinary flow rate and post-void residual volume [30]. Erectile dysfunction complicates around 52.5% [31] of men with diabetes and can be assessed by means of the International Index of Erectile Function and the Sexual Encounter Profile, nocturnal penile tumescence, penile Doppler ultrasound, sacral response, bulbocavernosus reflex, dorsal sensory nerve conduction of the penis, amplitude and latency of penile sympathetic skin response, and pudendal nerve somatosensory-evoked potentials [32]. Sudomotor dysfunction may be one of the earliest manifestations of DAN resulting in loss of sweating and can be evaluated via several modalities. Sympathetic skin response previously failed to detect DPN in a study of 337 patients with diabetes [33], but more recently it was shown to predict the risk of foot ulceration, comparable to abnormalities in NDS and vibration perception [34]. The quantitative sudomotor axon reflex test evaluates postganglionic axonal integrity, whilst the sympathetic skin response assesses polysynaptic pathways and has previously been shown to be superior for detecting early neuropathy compared to the sympathetic skin response in a small series of 31 patients with diabetes [35]. The sweat indicator plaster [36] (Neuropad) is a visual test, which uses a timed color change to define the integrity of skin sympathetic cholinergic innervation. A prospective study of 109 patients with diabetes mellitus (DM) [37] reported that abnormalities on Neuropad in subjects without DPN were a strong predictor for the subsequent development of DPN, within 5 years. This is an important finding given that abnormal sweating is associated with small fiber neuropathy [38] commonly missed with bedside testing. The thermoregulatory sweat test [39] is a method of assessing location specific alterations by delivering a controlled heat stimulus to induce a generalized sweat response. The patient's response is detected by assessing a significant color change in cornstarch, sodium carbonate, or alizarin red, which are applied uniformly over the body. Finally, the Sudoscan test (Impeto Medical, San Diego, CA, USA) assesses electrochemical skin conductance as an indicator of sweat gland function and can differentiate patients with and without neuropathy and controls with high sensitivity and specificity as well as patients with and without CAN [40].
DIABETIC AUTONOMIC NEUROPATHY
- Nerve conduction studies (NCS) are considered to be the gold standard for the diagnosis of DPN. The Toronto consensus [20] recommended the use of abnormal NCS with a symptom or sign to diagnose DPN. The typical electrophysiological findings in DPN are amplitude reduction of the compound muscle action potential, slowing of sensory and motor NCV, prolonged F-wave latency and an absent Hoffman reflex. Although NCS provide an objective means of quantifying peripheral large nerve fiber dysfunction it cannot assess small sensory fiber damage, the earliest manifestation of DPN. A recent study [22] in DM patients with/without sensory symptoms and normal NCS showed that IENFD and thermal thresholds were significantly reduced compared to healthy controls but also differed between the symptomatic and asymptomatic groups. This finding highlights that small fiber injury occurs early in DPN and cannot be captured by NCS. Another major limitation is poor reproducibility and lack of measurement standardization across centers. Dyck et al. [41] found poor interobserver repeatability amongst expert neurophysiologists who independently assessed eight attributes of NCS in the same patients with diabetes on consecutive occasions. The magnitude of variability was a major point of concern and the authors rather than questioning the viability of this test, simply recommended that the same examiners should perform all NCS assessments in clinical trials of neuropathy.
- Several studies [4243444546] have reported NCS abnormalities in patients with impaired glucose tolerance (IGT) and DM. Sumner et al. [42] found a reduction in IENFD, sural nerve amplitude and conduction velocity in patients with IGT and DM, with more marked abnormalities in patients with DM with a predominantly small fiber neuropathy in the IGT group. Glycemic control, DM duration, age, male gender, and height are associated with electrodiagnostic abnormalities in patients with DM [45]. More recently it has been suggested that quantification of the Hoffman reflex as a result of anhidrotic stimulation of type 1a sensory fibers may be a sensitive electrophysiological measure of DPN and a marker of spinal disinhibition [47]. Indeed, Millan-Guerrero et al. [48] reported that the Hoffman reflex was absent in 39.3% of T2DM patients compared to only 9.3% with abnormal NCS. Another recent study [49] found that assessment of rate dependent depression, a measure of change in amplitude of the Hoffman reflex, is able to identify differences in experimental and human DPN in relation to the contribution of spinal inhibitory pathways driving neuropathic pain.
- Despite serial failure as an end point, most clinical trials [5051525354] have used NCS as the primary outcome to assess treatment efficacy. Kennedy et al. [50] failed to demonstrate any improvement in neurophysiological measures of DPN 24 months after simultaneous pancreas and kidney (SPK) transplantation in 61 type 1 diabetes mellitus (T1DM) patients. The Neurological Assessment of Thioctic Acid in Diabetic Neuropathy 1 (NATHAN-1) study [51], a 4-year multicenter randomized controlled trial of alpha lipoic acid demonstrated no benefit in neurophysiology, QST and DPN composite scores. However, Malik et al. [52] demonstrated an improvement in neurophysiology in normotensive patients with DPN and subsequently the Delapril and Manidipine for Nephroprotection in Diabetes (DEMAND) study [53] demonstrated a significant reduction in the odds ratios for DPN assessed by neurophysiology, QST, symptoms and signs, and autonomic dysfunction. A recent 52-week phase III trial [54] of weekly C-peptide replacement compared to placebo in 250 patients with T1DM did not show an improvement in electrophysiological variables. A surprising finding was that at the end of the trial, NCV improvement in the placebo treated group exceeded the gains observed in the active treatment group. This long list of failed clinical trials makes apparent that currently advocated endpoints of neuropathy lack the required sensitivity to capture treatment effects early and are in part responsible for the lack of U.S. Food and Drug Administration (FDA)-approved treatments for DPN.
NEUROPHYSIOLOGY
- Skin biopsy allows morphometric quantification of intra-epidermal nerve fibers (IENFs), expressed as the number of IENFs per length of section (IENF/mm). This technique has good reproducibility and an accurate quantification method has been established for assessing IENF pathology along with normative age-matched ranges [55]. There is an age- and sex-related decline in IENFD, but unlike neurophysiology it is not affected by weight and height [56]. The European Federation of Neurological Societies have published guidelines on its use in the diagnosis of peripheral neuropathies [57]. However, the diagnostic yield of skin biopsy depends on the reference and cutoff values selected and the definition of small fiber neuropathy.
- Several studies have shown loss of IENFD in people with DM and IGT compared to healthy controls [58]. Therefore, the assessment of IENFD is a valid measure of diabetic neuropathy and may also be useful in predicting the development of clinical neuropathy [57]. A lower IENFD can identify early DPN and may be lower in people with painful as compared to painless DPN [59]. A recent study [60] showed a reduction in IENFD in patients with T2DM over 5 years, due to slower nerve regeneration in people with diabetes [61]. Narayanaswamy et al. [62] examined 29 patients with DPN and found that the annual rate of mean IENF loss was 3.76 fibers/mm. A 1-year diet and exercise intervention in people with IGT improved IENFD [63]. An inverse correlation also exists between IENFD and the severity of DPN defined on the basis of neuropathy disability and impairment scores. However, a recent study has demonstrated no correlation between IENFD and the neuropathy symptom score, but interestingly an inverse correlation with the severity of pain [64]. Alam et al. [65] has recently shown that IENFD has a diagnostic sensitivity of 0.61 and specificity of 0.80 for DPN. Because IENFD is considered to be the gold standard for the evaluation of small fiber neuropathy it has been advocated as a measure of treatment response in clinical trials. However, skin biopsy is an invasive technique, which requires experience and expertise to perform reliable IENFD staining with protein gene product 9.5 and subsequent quantification. The chance of bleeding and infection in DM patients also reduces its appeal as a diagnostic test for DPN and it therefore cannot be recommended in longitudinal and interventional studies. Furthermore, it has not been shown to be of value as a measure of therapeutic efficacy in a number of clinical trials in diabetic and human immunodeficiency virus (HIV) neuropathy [66].
SKIN BIOPSY
- Corneal confocal microscopy (CCM) is a non-invasive and reiterative ophthalmic imaging technique, which allows in vivo examination of the cornea. The primary application of CCM was in the diagnosis and management of corneal disease. However, in the early 2000s two landmark studies by Rosenberg et al. [67] and Malik et al. [68] reported a progressive loss of corneal sub-basal nerve fibers in patients with increasing severity of DPN. Subsequently, multiple centers have confirmed these findings in different populations and the use of CCM to study DPN and neurodegeneration more broadly has grown exponentially [69].
- Human corneal innervation
- The cornea is one of the most densely innervated tissues of the human body receiving sensory innervation from the trigeminal ganglion. Myelinated nerve fiber bundles penetrate the peripheral limbal cornea and run towards the anterior central cornea where they terminate at the subbasal nerve plexus (SNP), a dense network of unmyelinated axons (19,000 to 44,000 axons within 90 mm2) equally distributed in the central and peripheral-central cornea. Previous studies [70] using electron-microscopy and immunohistochemistry have confirmed these nerve fibers to be C-fibers. Physiologically, corneal innervation plays an important role in the maintenance of a healthy ocular surface and in wound healing by regulating epithelial cell growth, proliferation and differentiation via the release of soluble growth factors, cytokines and neuropeptides such as substance P and calcitonin gene related peptide amongst others [71]. It is well established that corneal nerve dysfunction due to herpetic infections [72], trigeminal nerve lesions [73], neurosurgical injury [73], or intracranial disease [74] can result in neurotrophic keratitis. Indeed, neurotrophic corneal ulcers have been described in patients with DM as early as 1977 [75].
- Image acquisition with CCM
- The type of CCM used, i.e., white light or laser can significantly impact on the image acquisition process and quality. Over the last decade, the vast majority of research centers have utilized the laser CCM (Heidelberg Retina Tomograph III Rostock Corneal Module; Heidelberg Engineering GmbH, Heidelberg, Germany) due to its superior image quality and rapid scanning time. This CCM offers three modes to capture images namely: section, volume, and sequence. There is currently limited consensus on the optimal method to capture and analyze CCM images to assess the impact of DPN on corneal nerve morphology. In a healthy cornea the SNP is normally visible at 50 to 90 µm with a laser CCM. Section mode allows the examiner to capture images by manually focusing the field of view on the area of interest and may be more suitable for more experienced users. The other two modes, sequence and volume, allow the acquisition of sequential confocal images separated by 1 µm from a pre-specified area of the tissue. Most studies [76] have mostly analyzed five to eight high-quality, non-overlapping images from the central and peripheral-central cornea while others [77] have proposed that one ‘technically sound’ image offers adequate accuracy. A study by Vagenas et al. [78] showed that the selection of five to eight images was optimal to quantify corneal nerve morphology. Schaldemose et al. [79] described an objective method of randomly sampling and analyzing CCM images with the use of software which considers only in-focus nerves for quantification. They found small albeit significant differences when randomized sampling was used compared to human observer selection concluding that with the increased use of CCM worldwide a consensus on sampling is needed. One limitation of CCM is the small field of view (40×40) and some centers [80] have used wide field imaging techniques to produce maps of the SNP. Allgeier et al. [81] showed that an automated algorithm can create mosaics from the SNP within 145 seconds. However, the study population consisted of healthy controls and as the technique requires significant subject co-operation it poses a question regarding feasibility in morbid subjects. Although wide-field imaging allows an enhanced view of corneal nerve morphology it significantly prolongs the examination time, and indeed analysis of the composite image is highly laborious and has questionable added benefit. A recent study [82] estimated the nerve densities from the same participants using either three representative CCM images or wide field composite images and found no significant difference. The authors concluded that analysis of representative CCM images from a single scan provides adequate accuracy and could be used in clinical studies. Nevertheless, wide-field imaging could be more suitable for a research setting in order to study and characterize in detail the onset and extent of corneal nerve pathology in DPN while sampling of five to eight representative images may be the method of choice for a clinical setting.
- CCM image quantification
- The vast majority of studies have reported results from four morphological parameters namely corneal nerve fiber density (CNFD), corneal nerve branch density (CNBD), corneal nerve fiber length (CNFL), the tortuosity coefficient (TC) and more recently the inferior whorl length (IWL) [83]. CNFD refers to the total number of main nerve fibers in a CCM image (fibers/mm2), CNBD is defined as the number of branches connecting to the main nerve fiber (branches/mm2), CNFL is the sum of the length of all nerve fibers and branches in a CCM image (mm/mm2), and the TC is a unit-less measurement of the tortuosity of the main nerve fibers in a CCM image, independent of the orientation of the nerves. IWL is defined as the length of the nerves at the inferior whorl of the SNP, an anatomically distinct area where the nerves are arranged in a whorl like pattern. Other reported parameters include nerve fiber beading (number/100 µm) [84], corneal nerve connection points and average weighted corneal nerve fiber thickness which essentially measures nerve fiber width [85]. Nerve fiber area may be optimal for detecting change in clinical trials of new therapeutics [86]. A recent study proposed that the novel parameter of corneal nerve fractal dimension analysis, a measurement of morphological complexity, could be a useful and highly sensitive parameter to assess neurodegeneration in T1DM [87]. The vast majority of studies report results using either CCMetrics or ImageJ (https://imagej.nih.gov/ij/download.html). CCMetrics is a software capable of manual and fully automated analysis, which has been specifically designed and validated for CCM corneal nerve quantification [76]. ImageJ is a more generic software widely used for image processing and its usability for quantifying nerve morphology can be extended with the use of purpose-built plugins such as NeuronJ [88]. Recently, two novel algorithms for fully automated tracing of corneal nerve density [89] and length [90] in wide-field mosaics have been described but their performance is yet to be validated in larger studies. DPN may also induce clustering of corneal nerve fibers compared to the equally distributed nerve fibers in the healthy cornea. Spatial pattern analysis of CCM mosaics, an advanced computing method which allows the estimation of corneal nerve branching points, has been found to improve the detection of corneal nerve loss when used in combination with conventional measures of nerve morphometry [91].
- CCM in diabetic peripheral neuropathy
- Reduced corneal sensation in diabetes as a result of polyneuropathy was reported as early as 1974 [92]. Schwartz [92] first studied corneal sensitivity in a group of 44 patients with DM and found significantly reduced sensation in clinically normal corneas which was symmetrical, occurred early and was related to disease duration. Another study [75] reported the occurrence of treatment-resistant neurotrophic corneal ulcers in young patients with T1DM. Both studies did not report the DPN status in the study population. In the early 2000s, Rosenberg et al. [67] showed subbasal nerve alterations using CCM in patients with clinically confirmed DPN and Malik et al. [68] showed that the severity of corneal nerve pathology was related to DPN severity.
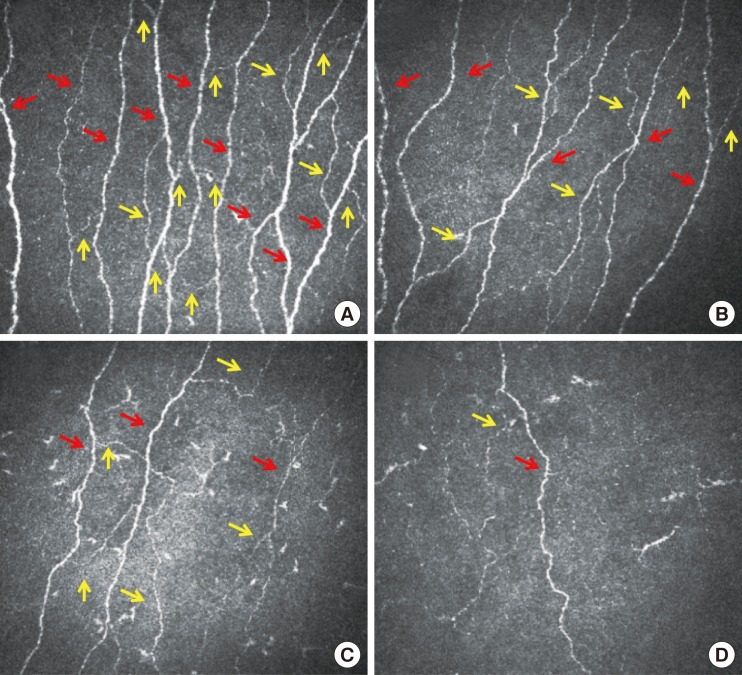
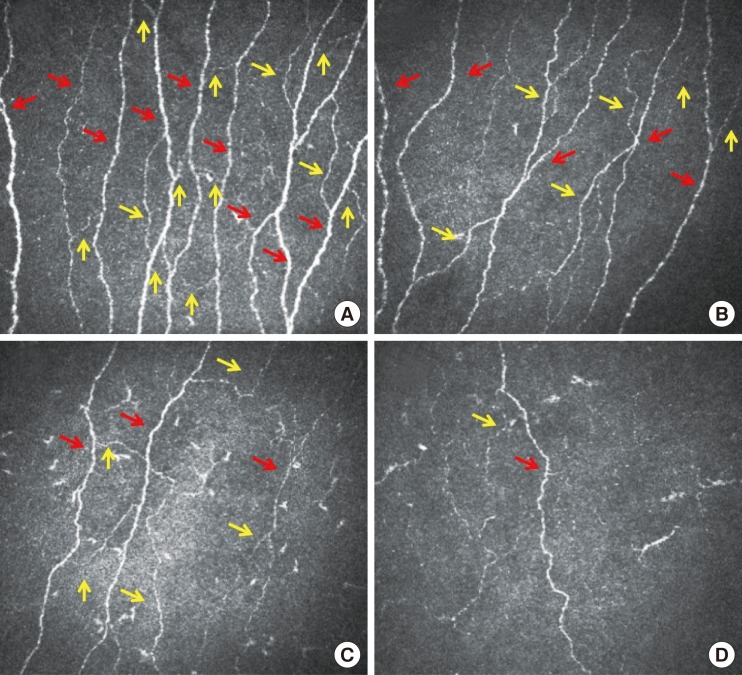
- We, and others have shown that CCM can be used to detect early corneal nerve alterations [8093] with excellent reproducibility between examiners, occasions and quantification methods (Fig. 1) [9495969798]. We have established a multinational normative reference database for corneal nerve morphology [99] and shown that healthy individuals exhibit morphometric stability over time [100]. CNFD significantly correlates with IENFD and QST while corneal and IENF length can differentiate patients with and without painful neuropathy [93]. These results were not confirmed by an independent study employing CCM and IENFD, which reported a patchy pattern of loss between the cornea and skin, suggesting that the exact temporal relationship needed further clarification [80]. However, studies have demonstrated that CCM has comparable diagnostic performance to IENFD with the advantage that it is rapid and non-invasive compared to skin punch biopsy [65]. CNFL has a high sensitivity (91%) and specificity (93%) [77] for the diagnosis of DPN and cardiac autonomic neuropathy [84101] and a reduced CNFD or CNFL are associated with an odds ratio for DPN of 16.5 and 12.9, respectively [76]. A recent study has also shown that reduced corneal innervation is associated with erectile dysfunction [102]. IWL reduction is more prominent in patients with painful neuropathy [103] and its evaluation improves the diagnostic performance of CCM compared to central CNFL, indicating a dying back neuropathy; whilst its distinct morphology could make it an ideal anatomical location for reproducible follow-up assessments [103] in longitudinal studies and particularly in clinical trials [83]. Subtle, albeit significant alterations have been reported even in normoglycemic subjects with elevated glycosylated hemoglobin (HbA1c) indicating the ability of CCM to detect subclinical axonal degeneration [104]. A shorter CNFL is associated with functional deficits in cold detection threshold, laser Doppler image flare, and heart rate variability [105] and corneal nerve alterations precede overt diabetic retinopathy and microalbuminuria [106], which has significant implications for the screening of microvascular complications. A recent study shows significant corneal nerve fiber changes in pediatric T1DM patients, along with thinning of the retinal nerve fiber layer [107].
- A higher HbA1c and lower high density lipoprotein cholesterol impact on subbasal nerve morphology [83] and it has been shown to improve with treatment of glycaemia, blood pressure, and lipids [108] as well as in patients with T1DM on continuous subcutaneous insulin [109]. In the most dramatic example of curing diabetes with a SPK transplantation, CCM was able to detect significant corneal nerve regeneration 12 months after transplantation without an improvement in IENFD, QST, and NCV [110]. Hence CCM can detect early nerve fiber repair, missed by currently advocated measures of DPN. Indeed, recent phase 2 clinical trials have used CCM as a primary co-endpoint to show the efficacy of ARA-290, a novel first-in-class peptide [111] in patients with sarcoidosis-related neuropathy [112113] and T2DM [114]. Daily subcutaneous administration of ARA-290 over 28 days compared to placebo was associated with a significant improvement in CNFD along with an improvement in cutaneous temperature sensitivity and exercise capacity [112]. In a subsequent phase 2b randomized control study, improvement in corneal nerve morphology was strongly correlated with the expression of GAP-43+ IENF, indicating neuronal repair, and an improvement in pain intensity after 28 days [113]. In a pilot trial of seal oil omega-3 polyunsaturated fatty acids supplementation in patients with T1DM over 12 months showed a 29% increase in CNFL, a primary outcome, with no change in the secondary outcomes of NCV and sensory function [115]. Interestingly, a recent trial in T2DM rats showed that a combination therapy of Menhaden oil, alpha lipoic acid, and enalapril for 12-week was most effective for showing an improvement in the primary outcomes of corneal nerve density and sensitivity [116]. The case for inclusion of CCM as an outcome marker for trials of neuropathy is compelling.
- Results from longitudinal studies suggest that CCM has prognostic value. Pritchard et al. [117] reported that the 4-year incidence of DPN amongst non-neuropathic patients with T1DM was 18% and was associated with a lower baseline CNFL, longer diabetes duration, higher triglycerides, worsening retinopathy and nephropathy, impaired sensation to temperature and vibration and slower peroneal and sural nerve conduction velocities. Lovblom et al. [118] reported a 17% incidence of DPN in patients with T1DM followed over approximately 4 years, and a baseline CNFL of <14.9 mm/mm2 was the strongest predictor of new onset DPN. Another prospective study [58119] in subjects with IGT showed that lower baseline CNFD, CNBD, CNFL and mean dendritic length of IENF were the strongest predictors of progression to T2DM. Remarkably, those subjects who returned to normoglycaemia showed a small but significant improvement in their CCM parameters while IENFD continued to decline during the same period of time. The NIH CCM consortium study is an international pooled multi-center analysis to assess the diagnostic validity and determine diagnostic thresholds for identification of DPN by CCM. Early results from 516 participants have shown that measurement of CNFL has high sensitivity and specificity for the detection of DPN and support the implementation of CCM in trials of neuropathy [120]. A recent meta-analysis by Jiang et al. [69] of 13 studies in 1,680 subjects, independently confirmed CNFD, CNFL, and CNBD to be the best parameters to differentiate patients with and without DPN compared to healthy controls.
- CCM beyond diabetic neuropathy
- While there is strong evidence to support the utility of CCM in DPN, multiple studies suggest that CCM could also be used to characterize the extent of axonal injury in many other peripheral neuropathies and central neurodegenerative disorders. We and others have reported corneal nerve alterations in Charcot-Marie-Tooth disease type 1A [121], HIV sensory neuropathy [122], idiopathic small fiber neuropathy [123], Fabry' disease [124], chronic inflammatory demyelinating polyneuropathy [125], chemotherapy induced peripheral neuropathy [126], chronic migraine [127], Parkinson's disease [128], amyotrophic lateral sclerosis [129], stroke [130], and multiple sclerosis [131132133]. Importantly, in most of these studies corneal nerve alterations were associated with clinical and neurological disability and functional outcomes, suggesting that corneal subbasal innervation is a highly sensitive and accessible site to assess neurodegeneration.
CORNEAL CONFOCAL MICROSCOPY
- DPN is a serious and underdiagnosed complication of diabetes of multifactorial etiology. Currently advocated endpoints of neuropathy lack sensitivity to capture early abnormalities before overt neuropathy has developed, are invasive or have repeatedly failed as surrogate end-points of therapeutic efficacy in clinical trials of DPN. CCM has emerged as a powerful diagnostic tool for the detection of small fiber neuropathy, the earliest manifestation of DPN, and has shown prognostic utility in identifying those who develop clinical DPN as well as showing remarkable consistency demonstrating early nerve regeneration in a number of clinical trials. Given the rapid and non-invasive methodology and automated quantification it allows community level screening of DPN, similar to digital retinal photography for diabetic retinopathy.
CONCLUSIONS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
- 1. Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol 2010;9:807-819. ArticlePubMed
- 2. Boulton AJ, Gries FA, Jervell JA. Guidelines for the diagnosis and outpatient management of diabetic peripheral neuropathy. Diabet Med 1998;15:508-514. ArticlePubMed
- 3. Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care 2004;27:1458-1486. ArticlePubMedPDF
- 4. Spallone V, Morganti R, D'Amato C, Greco C, Cacciotti L, Marfia GA. Validation of DN4 as a screening tool for neuropathic pain in painful diabetic polyneuropathy. Diabet Med 2012;29:578-585. ArticlePubMed
- 5. Bennett M. The LANSS pain scale: the Leeds Assessment of Neuropathic Symptoms and Signs. Pain 2001;92:147-157. ArticlePubMed
- 6. Bouhassira D, Attal N, Fermanian J, Alchaar H, Gautron M, Masquelier E, Rostaing S, Lanteri-Minet M, Collin E, Grisart J, Boureau F. Development and validation of the neuropathic pain symptom inventory. Pain 2004;108:248-257. ArticlePubMed
- 7. Dyck PJ, Sherman WR, Hallcher LM, Service FJ, O'Brien PC, Grina LA, Palumbo PJ, Swanson CJ. Human diabetic endoneurial sorbitol, fructose, and myo-inositol related to sural nerve morphometry. Ann Neurol 1980;8:590-596. ArticlePubMed
- 8. Dyck PJ. Detection, characterization, and staging of polyneuropathy: assessed in diabetics. Muscle Nerve 1988;11:21-32. ArticlePubMed
- 9. Meijer JW, Smit AJ, Sonderen EV, Groothoff JW, Eisma WH, Links TP. Symptom scoring systems to diagnose distal polyneuropathy in diabetes: the Diabetic Neuropathy Symptom score. Diabet Med 2002;19:962-965. ArticlePubMed
- 10. Krause SJ, Backonja MM. Development of a neuropathic pain questionnaire. Clin J Pain 2003;19:306-314. ArticlePubMed
- 11. Perkins BA, Olaleye D, Zinman B, Bril V. Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care 2001;24:250-256. ArticlePubMedPDF
- 12. Martin CL, Albers J, Herman WH, Cleary P, Waberski B, Greene DA, Stevens MJ, Feldman EL. DCCT/EDIC Research Group. Neuropathy among the diabetes control and complications trial cohort 8 years after trial completion. Diabetes Care 2006;29:340-344. ArticlePubMedPDF
- 13. Herman WH, Pop-Busui R, Braffett BH, Martin CL, Cleary PA, Albers JW, Feldman EL. DCCT/EDIC Research Group. Use of the Michigan Neuropathy Screening Instrument as a measure of distal symmetrical peripheral neuropathy in type 1 diabetes: results from the diabetes control and complications trial/epidemiology of diabetes interventions and complications. Diabet Med 2012;29:937-944. ArticlePubMedPMCPDF
- 14. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. A multicenter study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia 1993;36:150-154. ArticlePubMedPDF
- 15. Singleton JR, Bixby B, Russell JW, Feldman EL, Peltier A, Goldstein J, Howard J, Smith AG. The Utah Early Neuropathy Scale: a sensitive clinical scale for early sensory predominant neuropathy. J Peripher Nerv Syst 2008;13:218-227. ArticlePubMed
- 16. Hoitsma E, Reulen JP, de Baets M, Drent M, Spaans F, Faber CG. Small fiber neuropathy: a common and important clinical disorder. J Neurol Sci 2004;227:119-130. ArticlePubMed
- 17. Nebuchennykh M, Loseth S, Lindal S, Mellgren SI. The value of skin biopsy with recording of intraepidermal nerve fiber density and quantitative sensory testing in the assessment of small fiber involvement in patients with different causes of polyneuropathy. J Neurol 2009;256:1067-1075. ArticlePubMedPDF
- 18. Shy ME, Frohman EM, So YT, Arezzo JC, Cornblath DR, Giuliani MJ, Kincaid JC, Ochoa JL, Parry GJ, Weimer LH. Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Quantitative sensory testing: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2003;60:898-904. ArticlePubMed
- 19. Dyck PJ, Kratz KM, Lehman KA, Karnes JL, Melton LJ 3rd, O'Brien PC, Litchy WJ, Windebank AJ, Smith BE, Low PA, Service FJ, Rizza RA, Zimmerman BR. The Rochester Diabetic Neuropathy Study: design, criteria for types of neuropathy, selection bias, and reproducibility of neuropathic tests. Neurology 1991;41:799-807. ArticlePubMed
- 20. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G, Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P. Toronto Diabetic Neuropathy Expert Group. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010;33:2285-2293. ArticlePubMedPMCPDF
- 21. Chao CC, Hsieh SC, Yang WS, Lin YH, Lin WM, Tai TY, Hsieh ST. Glycemic control is related to the severity of impaired thermal sensations in type 2 diabetes. Diabetes Metab Res Rev 2007;23:612-620. ArticlePubMed
- 22. Loseth S, Stalberg E, Jorde R, Mellgren SI. Early diabetic neuropathy: thermal thresholds and intraepidermal nerve fibre density in patients with normal nerve conduction studies. J Neurol 2008;255:1197-1202. ArticlePubMedPDF
- 23. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580-591. ArticlePubMed
- 24. Apfel SC. Nerve growth factor for the treatment of diabetic neuropathy: what went wrong, what went right, and what does the future hold? Int Rev Neurobiol 2002;50:393-413. ArticlePubMed
- 25. Ziegler D, Gries FA, Spuler M, Lessmann F. The epidemiology of diabetic neuropathy. Diabetic Cardiovascular Autonomic Neuropathy Multicenter Study Group. J Diabetes Complications 1992;6:49-57. PubMed
- 26. Gatopoulou A, Papanas N, Maltezos E. Diabetic gastrointestinal autonomic neuropathy: current status and new achievements for everyday clinical practice. Eur J Intern Med 2012;23:499-505. ArticlePubMed
- 27. Bytzer P, Talley NJ, Hammer J, Young LJ, Jones MP, Horowitz M. GI symptoms in diabetes mellitus are associated with both poor glycemic control and diabetic complications. Am J Gastroenterol 2002;97:604-611. ArticlePubMed
- 28. Jones KL, Horowitz M, Wishart MJ, Maddox AF, Harding PE, Chatterton BE. Relationships between gastric emptying, intragastric meal distribution and blood glucose concentrations in diabetes mellitus. J Nucl Med 1995;36:2220-2228. PubMed
- 29. Frimodt-Moller C. Diabetic cystopathy: epidemiology and related disorders. Ann Intern Med 1980;92:318-321. ArticlePubMed
- 30. Lee WC, Wu HP, Tai TY, Liu SP, Chen J, Yu HJ. Effects of diabetes on female voiding behavior. J Urol 2004;172:989-992. ArticlePubMed
- 31. Kouidrat Y, Pizzol D, Cosco T, Thompson T, Carnaghi M, Bertoldo A, Solmi M, Stubbs B, Veronese N. High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies. Diabet Med 2017;34:1185-1192. ArticlePubMedPDF
- 32. Kaneko S, Bradley WE. Penile electrodiagnosis. Value of bulbocavernosus reflex latency versus nerve conduction velocity of the dorsal nerve of the penis in diagnosis of diabetic impotence. J Urol 1987;137:933-935. ArticlePubMed
- 33. Bril V, Nyunt M, Ngo M. Limits of the sympathetic skin response in patients with diabetic polyneuropathy. Muscle Nerve 2000;23:1427-1430. ArticlePubMed
- 34. Tentolouris N, Marinou K, Kokotis P, Karanti A, Diakoumopoulou E, Katsilambros N. Sudomotor dysfunction is associated with foot ulceration in diabetes. Diabet Med 2009;26:302-305. ArticlePubMed
- 35. Shimada H, Kihara M, Kosaka S, Ikeda H, Kawabata K, Tsutada T, Miki T. Comparison of SSR and QSART in early diabetic neuropathy: the value of length-dependent pattern in QSART. Auton Neurosci 2001;92:72-75. ArticlePubMed
- 36. Ponirakis G, Fadavi H, Petropoulos IN, Azmi S, Ferdousi M, Dabbah MA, Kheyami A, Alam U, Asghar O, Marshall A, Tavakoli M, Al-Ahmar A, Javed S, Jeziorska M, Malik RA. Automated quantification of Neuropad improves its diagnostic ability in patients with diabetic neuropathy. J Diabetes Res 2015;2015:847854. ArticlePubMedPMCPDF
- 37. Papanas N, Papatheodorou K, Papazoglou D, Kotsiou S, Maltezos E. A prospective study on the use of the indicator test Neuropad® for the early diagnosis of peripheral neuropathy in type 2 diabetes. Exp Clin Endocrinol Diabetes 2011;119:122-125. ArticlePubMed
- 38. Quattrini C, Jeziorska M, Tavakoli M, Begum P, Boulton AJ, Malik RA. The Neuropad test: a visual indicator test for human diabetic neuropathy. Diabetologia 2008;51:1046-1050. ArticlePubMedPDF
- 39. Hsieh C, McNeeley K, Chelimsky TC. The clinical thermoregulatory sweat test induces maximal sweating. Clin Auton Res 2001;11:227-234. PubMed
- 40. Selvarajah D, Cash T, Davies J, Sankar A, Rao G, Grieg M, Pallai S, Gandhi R, Wilkinson ID, Tesfaye S. SUDOSCAN: a simple, rapid, and objective method with potential for screening for diabetic peripheral neuropathy. PLoS One 2015;10:e0138224. ArticlePubMedPMC
- 41. Dyck PJ, Albers JW, Wolfe J, Bolton CF, Walsh N, Klein CJ, Zafft AJ, Russell JW, Thomas K, Davies JL, Carter RE, Melton LJ 3rd, Litchy WJ. Clinical vs. Neurophysiology Trial 3 Investigators. A trial of proficiency of nerve conduction: greater standardization still needed. Muscle Nerve 2013;48:369-374. ArticlePubMedPMCPDF
- 42. Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003;60:108-111. ArticlePubMed
- 43. Feldman EL, Stevens MJ, Thomas PK, Brown MB, Canal N, Greene DA. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care 1994;17:1281-1289. ArticlePubMedPDF
- 44. Kobori M, Yagihashi S, Shiina N, Shiozawa N, Haginoya A, Ojima M, Douguchi S, Tamasawa A, Saitou M, Baba M, Osonoi T. Four-year sequential nerve conduction changes since first visit in Japanese patients with early type 2 diabetes. J Diabetes Investig 2017;8:369-376.ArticlePubMedPDF
- 45. Dunnigan SK, Ebadi H, Breiner A, Katzberg HD, Lovblom LE, Perkins BA, Bril V. Conduction slowing in diabetic sensorimotor polyneuropathy. Diabetes Care 2013;36:3684-3690. ArticlePubMedPMCPDF
- 46. Dahl-Jorgensen K, Brinchmann-Hansen O, Hanssen KF, Ganes T, Kierulf P, Smeland E, Sandvik L, Aagenaes O. Effect of near normoglycaemia for two years on progression of early diabetic retinopathy, nephropathy, and neuropathy: the Oslo study. Br Med J (Clin Res Ed) 1986;293:1195-1199.ArticlePubMedPMC
- 47. Lee-Kubli C, Marshall AG, Malik RA, Calcutt NA. The H-reflex as a biomarker for spinal disinhibition in painful diabetic neuropathy. Curr Diab Rep 2018;18:1ArticlePubMedPMCPDF
- 48. Millan-Guerrero R, Trujillo-Hernandez B, Isais-Millan S, Prieto-Diaz-Chavez E, Vasquez C, Caballero-Hoyos JR, Garcia-Magana J. H-reflex and clinical examination in the diagnosis of diabetic polyneuropathy. J Int Med Res 2012;40:694-700. ArticlePubMedPDF
- 49. Marshall AG, Lee-Kubli C, Azmi S, Zhang M, Ferdousi M, Mixcoatl-Zecuatl T, Petropoulos IN, Ponirakis G, Fineman MS, Fadavi H, Frizzi K, Tavakoli M, Jeziorska M, Jolivalt CG, Boulton AJM, Efron N, Calcutt NA, Malik RA. Spinal disinhibition in experimental and clinical painful diabetic neuropathy. Diabetes 2017;66:1380-1390. ArticlePubMedPMCPDF
- 50. Kennedy WR, Navarro X, Goetz FC, Sutherland DE, Najarian JS. Effects of pancreatic transplantation on diabetic neuropathy. N Engl J Med 1990;322:1031-1037. ArticlePubMed
- 51. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr EJ 3rd, Litchy WJ, O'Brien PC. Challenges in design of multicenter trials: end points assessed longitudinally for change and monotonicity. Diabetes Care 2007;30:2619-2625. PubMed
- 52. Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, Boulton AJ. Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human diabetic neuropathy: randomised double-blind controlled trial. Lancet 1998;352:1978-1981. ArticlePubMed
- 53. Ruggenenti P, Lauria G, Iliev IP, Fassi A, Ilieva AP, Rota S, Chiurchiu C, Barlovic DP, Sghirlanzoni A, Lombardi R, Penza P, Cavaletti G, Piatti ML, Frigeni B, Filipponi M, Rubis N, Noris G, Motterlini N, Ene-Iordache B, Gaspari F, Perna A, Zaletel J, Bossi A, Dodesini AR, Trevisan R, Remuzzi G. DEMAND Study Investigators. Effects of manidipine and delapril in hypertensive patients with type 2 diabetes mellitus: the Delapril and Manidipine for Nephroprotection in Diabetes (DEMAND) randomized clinical trial. Hypertension 2011;58:776-783. ArticlePubMed
- 54. Wahren J, Foyt H, Daniels M, Arezzo JC. Long-acting C-peptide and neuropathy in type 1 diabetes: a 12-month clinical trial. Diabetes Care 2016;39:596-602. ArticlePubMedPDF
- 55. Lauria G, Lombardi R, Camozzi F, Devigili G. Skin biopsy for the diagnosis of peripheral neuropathy. Histopathology 2009;54:273-285. ArticlePubMed
- 56. Bakkers M, Merkies IS, Lauria G, Devigili G, Penza P, Lombardi R, Hermans MC, van Nes SI, De Baets M, Faber CG. Intraepidermal nerve fiber density and its application in sarcoidosis. Neurology 2009;73:1142-1148. ArticlePubMed
- 57. Lauria G, Cornblath DR, Johansson O, McArthur JC, Mellgren SI, Nolano M, Rosenberg N, Sommer C. European Federation of Neurological Societies. EFNS guidelines on the use of skin biopsy in the diagnosis of peripheral neuropathy. Eur J Neurol 2005;12:747-758. ArticlePubMed
- 58. Asghar O, Petropoulos IN, Alam U, Jones W, Jeziorska M, Marshall A, Ponirakis G, Fadavi H, Boulton AJ, Tavakoli M, Malik RA. Corneal confocal microscopy detects neuropathy in subjects with impaired glucose tolerance. Diabetes Care 2014;37:2643-2646. ArticlePubMedPMCPDF
- 59. Sorensen L, Molyneaux L, Yue DK. The relationship among pain, sensory loss, and small nerve fibers in diabetes. Diabetes Care 2006;29:883-887. ArticlePubMedPDF
- 60. Løseth S, Stalberg EV, Lindal S, Olsen E, Jorde R, Mellgren SI. Small and large fiber neuropathy in those with type 1 and type 2 diabetes: a 5-year follow-up study. J Peripher Nerv Syst 2016;21:15-21. ArticlePubMedPDF
- 61. Polydefkis M, Hauer P, Sheth S, Sirdofsky M, Griffin JW, McArthur JC. The time course of epidermal nerve fibre regeneration: studies in normal controls and in people with diabetes, with and without neuropathy. Brain 2004;127(Pt 7):1606-1615. ArticlePubMed
- 62. Narayanaswamy H, Facer P, Misra VP, Timmers M, Byttebier G, Meert T, Anand P. A longitudinal study of sensory biomarkers of progression in patients with diabetic peripheral neuropathy using skin biopsies. J Clin Neurosci 2012;19:1490-1496. ArticlePubMed
- 63. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J, Pollari D, Bixby B, Howard J, Singleton JR. Lifestyle intervention for pre-diabetic neuropathy. Diabetes Care 2006;29:1294-1299. ArticlePubMedPDF
- 64. Loseth S, Mellgren SI, Jorde R, Lindal S, Stalberg E. Polyneuropathy in type 1 and type 2 diabetes: comparison of nerve conduction studies, thermal perception thresholds and intraepidermal nerve fibre densities. Diabetes Metab Res Rev 2010;26:100-106. ArticlePubMed
- 65. Alam U, Jeziorska M, Petropoulos IN, Asghar O, Fadavi H, Ponirakis G, Marshall A, Tavakoli M, Boulton AJM, Efron N, Malik RA. Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fibre density in diabetic neuropathy. PLoS One 2017;12:e0180175. ArticlePubMedPMC
- 66. Luciano CA, Pardo CA, McArthur JC. Recent developments in the HIV neuropathies. Curr Opin Neurol 2003;16:403-409. ArticlePubMed
- 67. Rosenberg ME, Tervo TM, Immonen IJ, Muller LJ, Gronhagen-Riska C, Vesaluoma MH. Corneal structure and sensitivity in type 1 diabetes mellitus. Invest Ophthalmol Vis Sci 2000;41:2915-2921. PubMed
- 68. Malik RA, Kallinikos P, Abbott CA, van Schie CH, Morgan P, Efron N, Boulton AJ. Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage and repair in diabetic patients. Diabetologia 2003;46:683-688. ArticlePubMedPDF
- 69. Jiang MS, Yuan Y, Gu ZX, Zhuang SL. Corneal confocal microscopy for assessment of diabetic peripheral neuropathy: a meta-analysis. Br J Ophthalmol 2016;100:9-14. ArticlePubMed
- 70. Muller LJ, Pels L, Vrensen GF. Ultrastructural organization of human corneal nerves. Invest Ophthalmol Vis Sci 1996;37:476-488. PubMed
- 71. Muller LJ, Marfurt CF, Kruse F, Tervo TM. Corneal nerves: structure, contents and function. Exp Eye Res 2003;76:521-542. ArticlePubMed
- 72. Holland EJ, Schwartz GS. Classification of herpes simplex virus keratitis. Cornea 1999;18:144-154. ArticlePubMed
- 73. Lambiase A, Sacchetti M, Mastropasqua A, Bonini S. Corneal changes in neurosurgically induced neurotrophic keratitis. JAMA Ophthalmol 2013;131:1547-1553. ArticlePubMed
- 74. Bonini S, Rama P, Olzi D, Lambiase A. Neurotrophic keratitis. Eye (Lond) 2003;17:989-995. ArticlePubMedPDF
- 75. Hyndiuk RA, Kazarian EL, Schultz RO, Seideman S. Neurotrophic corneal ulcers in diabetes mellitus. Arch Ophthalmol 1977;95:2193-2196. ArticlePubMed
- 76. Petropoulos IN, Alam U, Fadavi H, Marshall A, Asghar O, Dabbah MA, Chen X, Graham J, Ponirakis G, Boulton AJ, Tavakoli M, Malik RA. Rapid automated diagnosis of diabetic peripheral neuropathy with in vivo corneal confocal microscopy. Invest Ophthalmol Vis Sci 2014;55:2071-2078. ArticlePubMedPMC
- 77. Ahmed A, Bril V, Orszag A, Paulson J, Yeung E, Ngo M, Orlov S, Perkins BA. Detection of diabetic sensorimotor polyneuropathy by corneal confocal microscopy in type 1 diabetes: a concurrent validity study. Diabetes Care 2012;35:821-828. PubMedPMC
- 78. Vagenas D, Pritchard N, Edwards K, Shahidi AM, Sampson GP, Russell AW, Malik RA, Efron N. Optimal image sample size for corneal nerve morphometry. Optom Vis Sci 2012;89:812-817. ArticlePubMed
- 79. Schaldemose EL, Fontain FI, Karlsson P, Nyengaard JR. Improved sampling and analysis of images in corneal confocal microscopy. J Microsc 2017;268:3-12. ArticlePubMedPDF
- 80. Ziegler D, Papanas N, Zhivov A, Allgeier S, Winter K, Ziegler I, Bruggemann J, Strom A, Peschel S, Kohler B, Stachs O, Guthoff RF, Roden M. German Diabetes Study (GDS) Group. Early detection of nerve fiber loss by corneal confocal microscopy and skin biopsy in recently diagnosed type 2 diabetes. Diabetes 2014;63:2454-2463. ArticlePubMedPDF
- 81. Allgeier S, Maier S, Mikut R, Peschel S, Reichert KM, Stachs O, Kohler B. Mosaicking the subbasal nerve plexus by guided eye movements. Invest Ophthalmol Vis Sci 2014;55:6082-6089. ArticlePubMed
- 82. Kheirkhah A, Muller R, Mikolajczak J, Ren A, Kadas EM, Zimmermann H, Pruess H, Paul F, Brandt AU, Hamrah P. Comparison of standard versus wide-field composite images of the corneal subbasal layer by in vivo confocal microscopy. Invest Ophthalmol Vis Sci 2015;56:5801-5807. ArticlePubMedPMC
- 83. Petropoulos IN, Ferdousi M, Marshall A, Alam U, Ponirakis G, Azmi S, Fadavi H, Efron N, Tavakoli M, Malik RA. The inferior whorl for detecting diabetic peripheral neuropathy using corneal confocal microscopy. Invest Ophthalmol Vis Sci 2015;56:2498-2504. ArticlePubMedPMC
- 84. Maddaloni E, Sabatino F, Del Toro R, Crugliano S, Grande S, Lauria Pantano A, Maurizi AR, Palermo A, Bonini S, Pozzilli P, Manfrini S. In vivo corneal confocal microscopy as a novel non-invasive tool to investigate cardiac autonomic neuropathy in type 1 diabetes. Diabet Med 2015;32:262-266. ArticlePubMed
- 85. Kowtharapu BS, Winter K, Marfurt C, Allgeier S, Köhler B, Hovakimyan M, Stahnke T, Wree A, Stachs O, Guthoff RF. Comparative quantitative assessment of the human corneal sub-basal nerve plexus by in vivo confocal microscopy and histological staining. Eye (Lond) 2017;31:481-490. ArticlePubMedPDF
- 86. Brines M, Culver DA, Ferdousi M, Tannemaat MR, van Velzen M, Dahan A, Malik RA. Corneal nerve fiber size adds utility to the diagnosis and assessment of therapeutic response in patients with small fiber neuropathy. Sci Rep 2018;8:4734ArticlePubMedPMCPDF
- 87. Chen X, Graham J, Petropoulos IN, Ponirakis G, Asghar O, Alam U, Marshall A, Ferdousi M, Azmi S, Efron N, Malik RA. Corneal nerve fractal dimension: a novel corneal nerve metric for the diagnosis of diabetic sensorimotor polyneuropathy. Invest Ophthalmol Vis Sci 2018;59:1113-1118. ArticlePubMedPMC
- 88. Meijering E, Jacob M, Sarria JC, Steiner P, Hirling H, Unser M. Design and validation of a tool for neurite tracing and analysis in fluorescence microscopy images. Cytometry A 2004;58:167-176. ArticlePubMed
- 89. Guimaraes P, Wigdahl J, Ruggeri A. A Fast and efficient technique for the automatic tracing of corneal nerves in confocal microscopy. Transl Vis Sci Technol 2016;5:7.
- 90. Allgeier S, Winter K, Bretthauer G, Guthoff RF, Peschel S, Reichert KM, Stachs O, Kohler B. A novel approach to analyze the progression of measured corneal sub-basal nerve fiber length in continuously expanding mosaic images. Curr Eye Res 2017;42:549-556. ArticlePubMed
- 91. Ziegler D, Winter K, Strom A, Zhivov A, Allgeier S, Papanas N, Ziegler I, Bruggemann J, Ringel B, Peschel S, Kohler B, Stachs O, Guthoff RF, Roden M. German Diabetes Study (GDS) Group. Spatial analysis improves the detection of early corneal nerve fiber loss in patients with recently diagnosed type 2 diabetes. PLoS One 2017;12:e0173832. ArticlePubMedPMC
- 92. Schwartz DE. Corneal sensitivity in diabetics. Arch Ophthalmol 1974;91:174-178. ArticlePubMed
- 93. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J, Marshall A, Boulton AJ, Efron N, Malik RA. Surrogate markers of small fiber damage in human diabetic neuropathy. Diabetes 2007;56:2148-2154. ArticlePubMedPDF
- 94. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA. Repeatability of in vivo corneal confocal microscopy to quantify corneal nerve morphology. Cornea 2013;32:e83-e89. ArticlePubMed
- 95. Efron N, Edwards K, Roper N, Pritchard N, Sampson GP, Shahidi AM, Vagenas D, Russell A, Graham J, Dabbah MA, Malik RA. Repeatability of measuring corneal subbasal nerve fiber length in individuals with type 2 diabetes. Eye Contact Lens 2010;36:245-248. ArticlePubMed
- 96. Hertz P, Bril V, Orszag A, Ahmed A, Ng E, Nwe P, Ngo M, Perkins BA. Reproducibility of in vivo corneal confocal microscopy as a novel screening test for early diabetic sensorimotor polyneuropathy. Diabet Med 2011;28:1253-1260. ArticlePubMed
- 97. Kalteniece A, Ferdousi M, Adam S, Schofield J, Azmi S, Petropoulos I, Soran H, Malik RA. Corneal confocal microscopy is a rapid reproducible ophthalmic technique for quantifying corneal nerve abnormalities. PLoS One 2017;12:e0183040. ArticlePubMedPMC
- 98. Scarr D, Lovblom LE, Ostrovski I, Kelly D, Wu T, Farooqi MA, Halpern EM, Ngo M, Ng E, Orszag A, Bril V, Perkins BA. Agreement between automated and manual quantification of corneal nerve fiber length: Implications for diabetic neuropathy research. J Diabetes Complications 2017;31:1066-1073. ArticlePubMed
- 99. Tavakoli M, Ferdousi M, Petropoulos IN, Morris J, Pritchard N, Zhivov A, Ziegler D, Pacaud D, Romanchuk K, Perkins BA, Lovblom LE, Bril V, Singleton JR, Smith G, Boulton AJ, Efron N, Malik RA. Normative values for corneal nerve morphology assessed using corneal confocal microscopy: a multinational normative data set. Diabetes Care 2015;38:838-843. ArticlePubMedPMCPDF
- 100. Dehghani C, Pritchard N, Edwards K, Vagenas D, Russell AW, Malik RA, Efron N. Morphometric stability of the corneal subbasal nerve plexus in healthy individuals: a 3-year longitudinal study using corneal confocal microscopy. Invest Ophthalmol Vis Sci 2014;55:3195-3199. ArticlePubMed
- 101. Tavakoli M, Begum P, McLaughlin J, Malik RA. Corneal confocal microscopy for the diagnosis of diabetic autonomic neuropathy. Muscle Nerve 2015;52:363-370. ArticlePubMed
- 102. Azmi S, Ferdousi M, Alam U, Petropoulos IN, Ponirakis G, Marshall A, Asghar O, Fadavi H, Jones W, Tavakoli M, Boulton AJM, Jeziorska M, Soran H, Efron N, Malik RA. Small-fibre neuropathy in men with type 1 diabetes and erectile dysfunction: a cross-sectional study. Diabetologia 2017;60:1094-1101. ArticlePubMedPMCPDF
- 103. Kalteniece A, Ferdousi M, Petropoulos I, Azmi S, Adam S, Fadavi H, Marshall A, Boulton AJM, Efron N, Faber CG, Lauria G, Soran H, Malik RA. Greater corneal nerve loss at the inferior whorl is related to the presence of diabetic neuropathy and painful diabetic neuropathy. Sci Rep 2018;8:3283. ArticlePubMedPMCPDF
- 104. Wu T, Ahmed A, Bril V, Orszag A, Ng E, Nwe P, Perkins BA. Variables associated with corneal confocal microscopy parameters in healthy volunteers: implications for diabetic neuropathy screening. Diabet Med 2012;29:e297-e303. ArticlePubMed
- 105. Sivaskandarajah GA, Halpern EM, Lovblom LE, Weisman A, Orlov S, Bril V, Perkins BA. Structure-function relationship between corneal nerves and conventional small-fiber tests in type 1 diabetes. Diabetes Care 2013;36:2748-2755. ArticlePubMedPMCPDF
- 106. Petropoulos IN, Green P, Chan AW, Alam U, Fadavi H, Marshall A, Asghar O, Efron N, Tavakoli M, Malik RA. Corneal confocal microscopy detects neuropathy in patients with type 1 diabetes without retinopathy or microalbuminuria. PLoS One 2015;10:e0123517. ArticlePubMedPMC
- 107. Gotze A, von Keyserlingk S, Peschel S, Jacoby U, Schreiver C, Kohler B, Allgeier S, Winter K, Rohlig M, Junemann A, Guthoff R, Stachs O, Fischer DC. The corneal subbasal nerve plexus and thickness of the retinal layers in pediatric type 1 diabetes and matched controls. Sci Rep 2018;8:14PubMedPMC
- 108. Tavakoli M, Kallinikos P, Iqbal A, Herbert A, Fadavi H, Efron N, Boulton AJ, Malik RA. Corneal confocal microscopy detects improvement in corneal nerve morphology with an improvement in risk factors for diabetic neuropathy. Diabet Med 2011;28:1261-1267. ArticlePubMedPMC
- 109. Azmi S, Ferdousi M, Petropoulos IN, Ponirakis G, Fadavi H, Tavakoli M, Alam U, Jones W, Marshall A, Jeziorska M, Boulton AJ, Efron N, Malik RA. Corneal confocal microscopy shows an improvement in small-fiber neuropathy in subjects with type 1 diabetes on continuous subcutaneous insulin infusion compared with multiple daily injection. Diabetes Care 2015;38:e3-e4. ArticlePubMedPDF
- 110. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U, Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA. Corneal confocal microscopy detects early nerve regeneration in diabetic neuropathy after simultaneous pancreas and kidney transplantation. Diabetes 2013;62:254-260. ArticlePubMedPDF
- 111. van Velzen M, Heij L, Niesters M, Cerami A, Dunne A, Dahan A, Brines M. ARA 290 for treatment of small fiber neuropathy in sarcoidosis. Expert Opin Investig Drugs 2014;23:541-550.ArticlePubMed
- 112. Dahan A, Dunne A, Swartjes M, Proto PL, Heij L, Vogels O, van Velzen M, Sarton E, Niesters M, Tannemaat MR, Cerami A, Brines M. ARA 290 improves symptoms in patients with sarcoidosis-associated small nerve fiber loss and increases corneal nerve fiber density. Mol Med 2013;19:334-345. ArticlePubMedPMCPDF
- 113. Culver DA, Dahan A, Bajorunas D, Jeziorska M, van Velzen M, Aarts LPHJ, Tavee J, Tannemaat MR, Dunne AN, Kirk RI, Petropoulos IN, Cerami A, Malik RA, Brines M. Cibinetide improves corneal nerve fiber abundance in patients with sarcoidosis-associated small nerve fiber loss and neuropathic pain. Invest Ophthalmol Vis Sci 2017;58:BIO52-BIO60. ArticlePubMed
- 114. Brines M, Dunne AN, van Velzen M, Proto PL, Ostenson CG, Kirk RI, Petropoulos IN, Javed S, Malik RA, Cerami A, Dahan A. ARA 290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic symptoms in patients with type 2 diabetes. Mol Med 2015;20:658-666. ArticlePubMedPMCPDF
- 115. Lewis EJH, Perkins BA, Lovblom LE, Bazinet RP, Wolever TMS, Bril V. Effect of omega-3 supplementation on neuropathy in type 1 diabetes: a 12-month pilot trial. Neurology 2017;88:2294-2301. ArticlePubMedPMC
- 116. Davidson EP, Coppey LJ, Shevalye H, Obrosov A, Kardon RH, Yorek MA. Impaired corneal sensation and nerve loss in a type 2 rat model of chronic diabetes is reversible with combination therapy of menhaden oil, α-lipoic acid, and enalapril. Cornea 2017;36:725-731. ArticlePubMedPMC
- 117. Pritchard N, Edwards K, Russell AW, Perkins BA, Malik RA, Efron N. Corneal confocal microscopy predicts 4-year incident peripheral neuropathy in type 1 diabetes. Diabetes Care 2015;38:671-675. ArticlePubMedPDF
- 118. Lovblom LE, Halpern EM, Wu T, Kelly D, Ahmed A, Boulet G, Orszag A, Ng E, Ngo M, Bril V, Perkins BA. In vivo corneal confocal microscopy and prediction of future-incident neuropathy in type 1 diabetes: a preliminary longitudinal analysis. Can J Diabetes 2015;39:390-397. ArticlePubMed
- 119. Azmi S, Ferdousi M, Petropoulos IN, Ponirakis G, Alam U, Fadavi H, Asghar O, Marshall A, Atkinson AJ, Jones W, Boulton AJ, Tavakoli M, Jeziorska M, Malik RA. Corneal confocal microscopy identifies small-fiber neuropathy in subjects with impaired glucose tolerance who develop type 2 diabetes. Diabetes Care 2015;38:1502-1508. ArticlePubMedPMCPDF
- 120. Perkins BA, Lovblom LE, Bril V, Edwards K, Pritchard N, Russell A, Pacaud D, Romanchuk K, Mah J, Boulton A, Jeziorska M, Marshall A, Shtein RM, Pop-Busui R, Feldman EL, Lentz SI, Tavakoli M, Efron N, Malik RA. Results of an International Corneal Confocal Microscopy (CCM) Consortium: a pooled multicentre analysis of the concurrent diagnostic validity of CCM to identify diabetic polyneuropathy in type 1 diabetes mellitus. Can J Diabetes 2016;40(5 Suppl):S20.Article
- 121. Tavakoli M, Marshall A, Banka S, Petropoulos IN, Fadavi H, Kingston H, Malik RA. Corneal confocal microscopy detects small-fiber neuropathy in Charcot-Marie-Tooth disease type 1A patients. Muscle Nerve 2012;46:698-704. ArticlePubMedPMCPDF
- 122. Kemp HI, Petropoulos IN, Rice ASC, Vollert J, Maier C, Sturm D, Schargus M, Peto T, Hau S, Chopra R, Malik RA. Use of corneal confocal microscopy to evaluate small nerve fibers in patients with human immunodeficiency virus. JAMA Ophthalmol 2017;135:795-800. ArticlePubMedPMC
- 123. Tavakoli M, Marshall A, Pitceathly R, Fadavi H, Gow D, Roberts ME, Efron N, Boulton AJ, Malik RA. Corneal confocal microscopy: a novel means to detect nerve fibre damage in idiopathic small fibre neuropathy. Exp Neurol 2010;223:245-250. ArticlePubMed
- 124. Tavakoli M, Marshall A, Thompson L, Kenny M, Waldek S, Efron N, Malik RA. Corneal confocal microscopy: a novel noninvasive means to diagnose neuropathy in patients with Fabry disease. Muscle Nerve 2009;40:976-984. ArticlePubMedPDF
- 125. Schneider C, Bucher F, Cursiefen C, Fink GR, Heindl LM, Lehmann HC. Corneal confocal microscopy detects small fiber damage in chronic inflammatory demyelinating polyneuropathy (CIDP). J Peripher Nerv Syst 2014;19:322-327. ArticlePubMedPDF
- 126. Ferdousi M, Azmi S, Petropoulos IN, Fadavi H, Ponirakis G, Marshall A, Tavakoli M, Malik I, Mansoor W, Malik RA. Corneal confocal microscopy detects small fibre neuropathy in patients with upper gastrointestinal cancer and nerve regeneration in chemotherapy induced peripheral neuropathy. PLoS One 2015;10:e0139394. ArticlePubMedPMC
- 127. Shetty R, Deshmukh R, Shroff R, Dedhiya C, Jayadev C. Subbasal nerve plexus changes in chronic migraine. Cornea 2018;37:72-75. ArticlePubMed
- 128. Kass-Iliyya L, Javed S, Gosal D, Kobylecki C, Marshall A, Petropoulos IN, Ponirakis G, Tavakoli M, Ferdousi M, Chaudhuri KR, Jeziorska M, Malik RA, Silverdale MA. Small fiber neuropathy in Parkinson's disease: a clinical, pathological and corneal confocal microscopy study. Parkinsonism Relat Disord 2015;21:1454-1460. ArticlePubMedPMC
- 129. Ferrari G, Grisan E, Scarpa F, Fazio R, Comola M, Quattrini A, Comi G, Rama P, Riva N. Corneal confocal microscopy reveals trigeminal small sensory fiber neuropathy in amyotrophic lateral sclerosis. Front Aging Neurosci 2014;6:278ArticlePubMedPMC
- 130. Khan A, Akhtar N, Kamran S, Ponirakis G, Petropoulos IN, Tunio NA, Dargham SR, Imam Y, Sartaj F, Parray A, Bourke P, Khan R, Santos M, Joseph S, Shuaib A, Malik RA. Corneal confocal microscopy detects corneal nerve damage in patients admitted with acute ischemic stroke. Stroke 2017;48:3012-3018. ArticlePubMed
- 131. Petropoulos IN, Kamran S, Li Y, Khan A, Ponirakis G, Akhtar N, Deleu D, Shuaib A, Malik RA. Corneal confocal microscopy: an imaging endpoint for axonal degeneration in multiple sclerosis. Invest Ophthalmol Vis Sci 2017;58:3677-3681. ArticlePubMed
- 132. Bitirgen G, Akpinar Z, Malik RA, Ozkagnici A. Use of corneal confocal microscopy to detect corneal nerve loss and increased dendritic cells in patients with multiple sclerosis. JAMA Ophthalmol 2017;135:777-782. ArticlePubMedPMC
- 133. Mikolajczak J, Zimmermann H, Kheirkhah A, Kadas EM, Oberwahrenbrock T, Muller R, Ren A, Kuchling J, Dietze H, Pruss H, Paul F, Hamrah P, Brandt AU. Patients with multiple sclerosis demonstrate reduced subbasal corneal nerve fibre density. Mult Scler 2017;23:1847-1853. ArticlePubMedPDF
REFERENCES
Corneal confocal microscopy images of the subbasal nerve plexus from a control subject (A) and patients with mild (B), moderate (C), and severe (D) diabetic neuropathy demonstrating a progressive reduction in corneal nerve fibers (red arrows) and corneal nerve branches (yellow arrows).
Summary of methods for the diagnosis of diabetic peripheral neuropathy
DN4, Douleur Neuropathique en 4; LANSS, Leeds Assessment of Neuropathic Symptoms and Signs; NPQ, Neuropathic Pain Questionnaire; MNSI, Michigan Neuropathy Screening Instrument; DNS, Diabetic Neuropathy Symptom; TCNS, Toronto Clinical Neuropathy Score; NDS, neuropathy disability score; UENS, Utah Early Neuropathy Scale; QSART, Quantitative Sudomotor Axon Reflex Test; NCS, nerve conduction studies; IENFD, intra-epidermal nerve fiber density; HRT III RCM, Heidelberg Retina Tomograph III Rostock Corneal Module.
Figure & Data
References
Citations
- Painful Diabetic Neuropathy: The Need for New Approaches
Andrea M. Yeung, Jingtong Huang, Kevin T. Nguyen, Nicole Y. Xu, Lorenzo T. Hughes, Brajesh K. Agrawal, Niels Ejskjaer, David C. Klonoff
Journal of Diabetes Science and Technology.2024; 18(1): 159. CrossRef - COMMENT ON: Diabetic peripheral neuropathy is associated with diabetic kidney disease and cardiovascular disease: The silesia diabetes-heart project
Laksh Kumar, Syed Ali Arsal
Current Problems in Cardiology.2024; 49(4): 102227. CrossRef - Risk factors for peripheral artery disease and diabetic peripheral neuropathy among patients with type 2 diabetes
Tian Chen, Shengjue Xiao, Zhengdong Chen, Yiqing Yang, Bingquan Yang, Naifeng Liu
Diabetes Research and Clinical Practice.2024; 207: 111079. CrossRef - Laser-Induced Graphene-Based Smart Insole to Measure Plantar Temperature
Amith Khandakar, Md. Ahasan Atick Faisal, Muhammad E. H. Chowdhury, Mamun Bin Ibne Reaz, Sawal Hamid Md Ali, Mohd Ibrahim bin Shapiai Abd. Razak, Ahmad Ashrif A. Bakar, Sakib Mahmud, Rayaz A. Malik
IEEE Sensors Journal.2024; 24(2): 1190. CrossRef - Morphometry of the sural nerve in diabetic neuropathy: a systematic review
Zhang Ludi, Matthias Yi Quan Liau, Bryan Song Jun Yong, Amanda Sze Yen Auyong, Quah Hui Ting Lynette, Samuel Jianjie Yeo, Khin Swee Elizabeth Tan, Sreenivasulu Reddy Mogali, Ramya Chandrasekaran, Vivek Perumal, Ranganath Vallabhajosyula
Journal of Ultrasound.2024;[Epub] CrossRef - Understanding the Clinical Relationship Between Diabetic Retinopathy, Nephropathy, and Neuropathy: A Comprehensive Review
Aditi Kulkarni, Archana R Thool, Sachin Daigavane
Cureus.2024;[Epub] CrossRef - Development and validation of risk prediction model for diabetic neuropathy among diabetes mellitus patients at selected referral hospitals, in Amhara regional state Northwest Ethiopia, 2005–2021
Negalgn Byadgie Gelaw, Achenef Asmamaw Muche, Adugnaw Zeleke Alem, Nebiyu Bekele Gebi, Yazachew Moges Chekol, Tigabu Kidie Tesfie, Tsion Mulat Tebeje, Jacopo Sabbatinelli
PLOS ONE.2023; 18(8): e0276472. CrossRef - Biomarkers in diabetic neuropathy
Kaveri M. Adki, Yogesh A. Kulkarni
Archives of Physiology and Biochemistry.2023; 129(2): 460. CrossRef - Early detection and treatment device for diabetic foot neuropathy
Hunduma Tolossa Kumsa, Lelisa Getaneh Abdisa, Lelisa Tesema Tolessa, Sosina Ayele Wubneh, Wadajo Feyisa Kusa, Shimelis Nigusu Hordofa, Hundessa Daba Nemomssa
Irish Journal of Medical Science (1971 -).2023; 192(1): 143. CrossRef - Differences in motor unit behavior during isometric contractions in patients with diabetic peripheral neuropathy at various disease severities
Mateus André Favretto, Felipe Rettore Andreis, Sandra Cossul, Francesco Negro, Anderson Souza Oliveira, Jefferson Luiz Brum Marques
Journal of Electromyography and Kinesiology.2023; 68: 102725. CrossRef - Association of peripheral neuropathy with subclinical left ventricular dysfunction in patients with type 2 diabetes
Yanyan Chen, Yi Wang, Ying Zhang, Mengying Li, Weiqing Zhang, Yingni Zhou, Xiangyang Liu, Jianfang Fu, Zuowei Lu, Qian Xu, Tao Liu, Zeping Li, Xiaomiao Li, Jie Zhou
Journal of Diabetes and its Complications.2023; 37(2): 108406. CrossRef - Quantifying gait intralimb coordination patterns in individuals with different levels of diabetic neuropathy: a vector coding analysis
Michelle Bazilio Milan, Guilherme Augusto Gomes De Villa, Eneida Yuri Suda, Isabel de Camargo Neves Sacco, Marcus Fraga Vieira
Research on Biomedical Engineering.2023; 39(1): 311. CrossRef - Mechanisms underlying altered neuromuscular function in people with DPN
Antonin Le Corre, Nathan Caron, Nicolas A. Turpin, Georges Dalleau
European Journal of Applied Physiology.2023; 123(7): 1433. CrossRef - Peripheral Neuropathy in Diabetes Mellitus: Pathogenetic Mechanisms and Diagnostic Options
Raffaele Galiero, Alfredo Caturano, Erica Vetrano, Domenico Beccia, Chiara Brin, Maria Alfano, Jessica Di Salvo, Raffaella Epifani, Alessia Piacevole, Giuseppina Tagliaferri, Maria Rocco, Ilaria Iadicicco, Giovanni Docimo, Luca Rinaldi, Celestino Sardu, T
International Journal of Molecular Sciences.2023; 24(4): 3554. CrossRef - Nerve conduction velocity is independently associated with bone mineral density in type 2 diabetes mellitus
Xiao-jing Chen, Xiao-feng Wang, Zheng-can Pan, Deng Zhang, Ke-cheng Zhu, Tao Jiang, Xiao-ke Kong, Rui Xie, Li-hao Sun, Bei Tao, Jian-min Liu, Hong-yan Zhao
Frontiers in Endocrinology.2023;[Epub] CrossRef - Precision of Michigan Neuropathy Screening Instrument (MNSI) Tool for the Diagnosis of Diabetic Peripheral Neuropathy Among People with Type 2 Diabetes—A Study from South India
Vijay Viswanathan, Balkhiwala Ahmed Khan, Sukanya Nachimuthu, Satyavani Kumpatla
The International Journal of Lower Extremity Wounds.2023; : 153473462311632. CrossRef - Ankle Fractures in Diabetic Patients
Ellen M. Goldberg, William S. Polachek, Kelly Hynes
JBJS Reviews.2023;[Epub] CrossRef - Comparing the Ipswich Touch Test (IpTT) and 10gm-SMWF (10-gm Semmes–Weinstein mono-filament) in Indian population subset with type 2 diabetes mellitus to detect diabetes neuropathy
Sivasubramaniyam Senthilkumar, Ramesh Dasarathan, Pushkar Pazhani, Archana Gaur, Varatharajan Sakthivadivel
Irish Journal of Medical Science (1971 -).2023; 192(6): 2793. CrossRef - Diabetic neuropathy: Pathogenesis and evolving principles of management
Basem Zaino, Rashika Goel, Sanjana Devaragudi, Ananya Prakash, Yogeshkumar Vaghamashi, Yashendra Sethi, Neil Patel, Nirja Kaka
Disease-a-Month.2023; 69(9): 101582. CrossRef - Association between Diabetic Peripheral Neuropathy as Measured Using a Point-of-Care Sural Nerve Conduction Device and Urinary Albumin Excretion in Patients with Type 2 Diabetes
Tatsuya Fukuda, Akiko Fujii, Taro Akihisa, Naoya Otsubo, Masanori Murakami, Tetsuya Yamada, Chisato Maki
Journal of Clinical Medicine.2023; 12(12): 4089. CrossRef - Sudomotor dysfunction in diabetic peripheral neuropathy (DPN) and its testing modalities: A literature review
Muhammad Akbar, Alvian Wandy, Gita Vita Soraya, Yudy Goysal, Mimi Lotisna, Muhammad Iqbal Basri
Heliyon.2023; 9(7): e18184. CrossRef - Novel insights into the nervous system affected by prolonged hyperglycemia
Kamila Zglejc-Waszak, Konark Mukherjee, Agnieszka Korytko, Bogdan Lewczuk, Andrzej Pomianowski, Joanna Wojtkiewicz, Marta Banach, Michał Załęcki, Natalia Nowicka, Julia Jarosławska, Bernard Kordas, Krzysztof Wąsowicz, Judyta K. Juranek
Journal of Molecular Medicine.2023; 101(8): 1015. CrossRef - (Pre)diabetes and a higher level of glycaemic measures are continuously associated with corneal neurodegeneration assessed by corneal confocal microscopy: the Maastricht Study
Sara B. A. Mokhtar, Frank C. T. van der Heide, Karel A. M. Oyaert, Carla J. H. van der Kallen, Tos T. J. M. Berendschot, Fabio Scarpa, Alessia Colonna, Bastiaan E. de Galan, Marleen M. J. van Greevenbroek, Pieter C. Dagnelie, Casper G. Schalkwijk, Rudy M.
Diabetologia.2023; 66(11): 2030. CrossRef - Potential Retinal Biomarkers in Alzheimer’s Disease
Mariana Yolotzin García-Bermúdez, Rupali Vohra, Kristine Freude, Peter van Wijngaarden, Keith Martin, Maj Schneider Thomsen, Blanca Irene Aldana, Miriam Kolko
International Journal of Molecular Sciences.2023; 24(21): 15834. CrossRef - The effect of polyneuropathy severity on nerve conduction and pain syndrome in patients with type 2 diabetes
A.Ya. Sabovchyk, M.M. Oros
INTERNATIONAL NEUROLOGICAL JOURNAL.2023; 19(6): 161. CrossRef - Artificial intelligence utilising corneal confocal microscopy for the diagnosis of peripheral neuropathy in diabetes mellitus and prediabetes
Frank G. Preston, Yanda Meng, Jamie Burgess, Maryam Ferdousi, Shazli Azmi, Ioannis N. Petropoulos, Stephen Kaye, Rayaz A. Malik, Yalin Zheng, Uazman Alam
Diabetologia.2022; 65(3): 457. CrossRef - 10.6-μm infrared laser as adjuvant therapy for diabetic peripheral neuropathy: study protocol for a double-blind, randomized controlled trial
Lin Lin, Yi Chen, Yuxia Li, Ke Cheng, Haiping Deng, Jianping Lu, Ling Zhao, Xueyong Shen
Trials.2022;[Epub] CrossRef - Diabetic corneal neuropathy as a surrogate marker for diabetic peripheral neuropathy
WeiZheng So, NatalieShi Qi Wong, HongChang Tan, MollyTzu Yu Lin, IsabelleXin Yu Lee, JodhbirS Mehta, Yu-Chi Liu
Neural Regeneration Research.2022; 17(10): 2172. CrossRef - SUDOSCAN in Combination with the Michigan Neuropathy Screening Instrument Is an Effective Tool for Screening Diabetic Peripheral Neuropathy
Tae Jung Oh, Yoojung Song, Hak Chul Jang, Sung Hee Choi
Diabetes & Metabolism Journal.2022; 46(2): 319. CrossRef - Performance Analysis of Conventional Machine Learning Algorithms for Diabetic Sensorimotor Polyneuropathy Severity Classification Using Nerve Conduction Studies
Fahmida Haque, Mamun B. I. Reaz, Muhammad E. H. Chowdhury, Serkan Kiranyaz, Sawal H. M. Ali, Mohammed Alhatou, Rumana Habib, Ahmad A. A. Bakar, Norhana Arsad, Geetika Srivastava, Paolo Crippa
Computational Intelligence and Neuroscience.2022; 2022: 1. CrossRef - The Presence of Clonal Hematopoiesis Is Negatively Associated with Diabetic Peripheral Neuropathy in Type 2 Diabetes
Tae Jung Oh, Han Song, Youngil Koh, Sung Hee Choi
Endocrinology and Metabolism.2022; 37(2): 243. CrossRef - An overview of painful diabetic peripheral neuropathy: Diagnosis and treatment advancements
Jonathan M. Hagedorn, Alyson M. Engle, Tony K. George, Jay Karri, Newaj Abdullah, Erik Ovrom, Jhon E. Bocanegra-Becerra, Ryan S. D'Souza
Diabetes Research and Clinical Practice.2022; 188: 109928. CrossRef - Prevalence and risk of diabetic complications in young-onset versus late-onset type 2 diabetes mellitus
Yongin Cho, Hye-Sun Park, Byung Wook Huh, Seong Ha Seo, Da Hea Seo, Seong Hee Ahn, Seongbin Hong, Young Ju Suh, So Hun Kim
Diabetes & Metabolism.2022; 48(6): 101389. CrossRef - Artificial Intelligence and Corneal Confocal Microscopy: The Start of a Beautiful Relationship
Uazman Alam, Matthew Anson, Yanda Meng, Frank Preston, Varo Kirthi, Timothy L. Jackson, Paul Nderitu, Daniel J. Cuthbertson, Rayaz A. Malik, Yalin Zheng, Ioannis N. Petropoulos
Journal of Clinical Medicine.2022; 11(20): 6199. CrossRef - INvesTigating the Abnormality of detrusor ConTractility by uroflowmetry in diabetic children (INTACT Trial): protocol of a prospective, observational study
Ágnes Rita Martonosi, Piroska Pázmány, Szabolcs Kiss, Annamária Zsákai, László Szabó
BMJ Open.2022; 12(11): e062198. CrossRef - Diabetic foot ulcers: A devastating complication of diabetes mellitus continues non-stop in spite of new medical treatment modalities
Gamze Akkus, Murat Sert
World Journal of Diabetes.2022; 13(12): 1106. CrossRef - Corneal nerves in diabetes—The role of the in vivo corneal confocal microscopy of the subbasal nerve plexus in the assessment of peripheral small fiber neuropathy
Anna M. Roszkowska, Carmelo Licitra, Giuseppe Tumminello, Elisa I. Postorino, Michele R. Colonna, Pasquale Aragona
Survey of Ophthalmology.2021; 66(3): 493. CrossRef - Association between Sleep Quality and Painless Diabetic Peripheral Neuropathy Assessed by Current Perception Threshold in Type 2 Diabetes Mellitus
Dughyun Choi, Bo-Yeon Kim, Chan-Hee Jung, Chul-Hee Kim, Ji-Oh Mok
Diabetes & Metabolism Journal.2021; 45(3): 358. CrossRef - Glycaemic control for painful diabetic peripheral neuropathy is more than fasting plasma glucose and glycated haemoglobin
Y.-W. Pai, C.-L. Tang, C.-H. Lin, S.-Y. Lin, I.-T. Lee, M.-H. Chang
Diabetes & Metabolism.2021; 47(1): 101158. CrossRef - Diagnosis of Neuropathy and Risk Factors for Corneal Nerve Loss in Type 1 and Type 2 Diabetes: A Corneal Confocal Microscopy Study
Maryam Ferdousi, Alise Kalteniece, Shazli Azmi, Ioannis N. Petropoulos, Georgios Ponirakis, Uazman Alam, Omar Asghar, Andrew Marshall, Catherine Fullwood, Maria Jeziorska, Caroline Abbott, Giuseppe Lauria, Catharina G. Faber, Handrean Soran, Nathan Efron,
Diabetes Care.2021; 44(1): 150. CrossRef - Widespread sensory neuropathy in diabetic patients hospitalized with severe COVID-19 infection
Ariel Odriozola, Lucía Ortega, Lidia Martinez, Samantha Odriozola, Ainhoa Torrens, David Corroleu, Silvia Martínez, Meritxell Ponce, Yolanda Meije, Mercedes Presas, Alejandra Duarte, M. Belén Odriozola, Rayaz A. Malik
Diabetes Research and Clinical Practice.2021; 172: 108631. CrossRef - Lost in Translation? Measuring Diabetic Neuropathy in Humans and Animals
Heung Yong Jin, Seong-Su Moon, Nigel A. Calcutt
Diabetes & Metabolism Journal.2021; 45(1): 27. CrossRef - Early Detection of Diabetic Peripheral Neuropathy: A Focus on Small Nerve Fibres
Jamie Burgess, Bernhard Frank, Andrew Marshall, Rashaad S. Khalil, Georgios Ponirakis, Ioannis N. Petropoulos, Daniel J. Cuthbertson, Rayaz A. Malik, Uazman Alam
Diagnostics.2021; 11(2): 165. CrossRef - Role of interdigital sensory nerve conduction study as a noninvasive approach for early diagnosis of diabetic peripheral neuropathy
Hamid R. Fateh, Seyed Pezhman Madani
Journal of Diabetes & Metabolic Disorders.2021; 20(1): 71. CrossRef - Performance Analysis of Conventional Machine Learning Algorithms for Diabetic Sensorimotor Polyneuropathy Severity Classification
Fahmida Haque, Mamun Bin Ibne Reaz, Muhammad Enamul Hoque Chowdhury, Geetika Srivastava, Sawal Hamid Md Ali, Ahmad Ashrif A. Bakar, Mohammad Arif Sobhan Bhuiyan
Diagnostics.2021; 11(5): 801. CrossRef - Advances in Screening, Early Diagnosis and Accurate Staging of Diabetic Neuropathy
Josie Carmichael, Hassan Fadavi, Fukashi Ishibashi, Angela C. Shore, Mitra Tavakoli
Frontiers in Endocrinology.2021;[Epub] CrossRef - Vibration Perception Threshold and Related Factors for Balance Assessment in Patients with Type 2 Diabetes Mellitus
Jisang Jung, Min-Gyu Kim, Youn-Joo Kang, Kyungwan Min, Kyung-Ah Han, Hyoseon Choi
International Journal of Environmental Research and Public Health.2021; 18(11): 6046. CrossRef - Diabetic Peripheral Neuropathy Affects Pinch Strength and Hand Dexterity in Elderly Patients
Qi Zhang, Yifang Lin, Xinhua Liu, Li Zhang, Yan Zhang, Dong Zhao, Qi Lu, Jie Jia, Jia-Jia Wu
Neural Plasticity.2021; 2021: 1. CrossRef - Association of Combined TCF7L2 and KCNQ1 Gene Polymorphisms with Diabetic Micro- and Macrovascular Complications in Type 2 Diabetes Mellitus
Rujikorn Rattanatham, Nongnuch Settasatian, Nantarat Komanasin, Upa Kukongviriyapan, Kittisak Sawanyawisuth, Phongsak Intharaphet, Vichai Senthong, Chatri Settasatian
Diabetes & Metabolism Journal.2021; 45(4): 578. CrossRef - Neuropeptide Y: a potential theranostic biomarker for diabetic peripheral neuropathy in patients with type-2 diabetes
Noo Ree Cho, Yeuni Yu, Chang-Kyu Oh, Dai Sik Ko, Kyungjae Myung, Yoonsung Lee, Hee Sam Na, Yun Hak Kim
Therapeutic Advances in Chronic Disease.2021; 12: 204062232110419. CrossRef - Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques
Dae Youp Shin, Bora Lee, Won Sang Yoo, Joo Won Park, Jung Keun Hyun
Journal of Clinical Medicine.2021; 10(19): 4576. CrossRef - Reduced association between dendritic cells and corneal sub‐basal nerve fibers in patients with fibromyalgia syndrome
Alexander Klitsch, Dimitar Evdokimov, Johanna Frank, Dominique Thomas, Nadine Saffer, Caren Meyer zu Altenschildesche, Marco Sisignano, Daniel Kampik, Rayaz A. Malik, Claudia Sommer, Nurcan Üçeyler
Journal of the Peripheral Nervous System.2020; 25(1): 9. CrossRef - Diet-Induced Rodent Models of Diabetic Peripheral Neuropathy, Retinopathy and Nephropathy
Inês Preguiça, André Alves, Sara Nunes, Pedro Gomes, Rosa Fernandes, Sofia D. Viana, Flávio Reis
Nutrients.2020; 12(1): 250. CrossRef - Diabetic Distal Symmetrical Polyneuropathy: Correlation of Clinical, Laboratory, and Electrophysiologic Studies in Patients with Type 2 Diabetes Mellitus
Yi-Ching Weng, Sung-Sheng Tsai, Rong-Kuo Lyu, Chun-Che Chu, Long-Sun Ro, Ming-Feng Liao, Hong-Shiu Chang, Chiung-Mei Chen, Jawl-Shan Hwang, Hung-Chou Kuo
Journal of Diabetes Research.2020; 2020: 1. CrossRef - Diabetic Peripheral Neuropathy: Is it Underdiagnosed?
Rizaldy T. Pinzon, M. Kes, Rosa De Lima R. Sa
Asian Journal of Biological Sciences.2020; 13(2): 168. CrossRef - Deterioration of Sleep Quality According to Glycemic Status
Myung Haeng Hur, Mi-Kyoung Lee, Kayeon Seong, Jun Hwa Hong
Diabetes & Metabolism Journal.2020; 44(5): 679. CrossRef - Microvascular Complications of Type 2 Diabetes Mellitus
Charles Faselis, Alexandra Katsimardou, Konstantinos Imprialos, Pavlos Deligkaris, Manolis Kallistratos, Kiriakos Dimitriadis
Current Vascular Pharmacology.2020; 18(2): 117. CrossRef - Computational methods for automated analysis of corneal nerve images: Lessons learned from retinal fundus image analysis
Tooba Salahuddin, Uvais Qidwai
Computers in Biology and Medicine.2020; 119: 103666. CrossRef - TIR generated by continuous glucose monitoring is associated with peripheral nerve function in type 2 diabetes
Fengwen Li, Yinan Zhang, Huizhi Li, Jingyi Lu, Lan Jiang, Robert A. Vigersky, Jian Zhou, Congrong Wang, Yuqian Bao, Weiping Jia
Diabetes Research and Clinical Practice.2020; 166: 108289. CrossRef - A Phase 2 Clinical Trial on the Use of Cibinetide for the Treatment of Diabetic Macular Edema
Noemi Lois, Evie Gardner, Margaret McFarland, David Armstrong, Christine McNally, Nuala Jane Lavery, Christina Campbell, Rita I Kirk, Daiva Bajorunas, Ann Dunne, Anthony Cerami, Michael Brines
Journal of Clinical Medicine.2020; 9(7): 2225. CrossRef - Diabetic neuropathy and neuropathic pain: a (con)fusion of pathogenic mechanisms?
Nigel A. Calcutt
Pain.2020; 161(Supplement): S65. CrossRef - Lumos for the long trail: Strategies for clinical diagnosis and severity staging for diabetic polyneuropathy and future directions
Tatsuhito Himeno, Hideki Kamiya, Jiro Nakamura
Journal of Diabetes Investigation.2020; 11(1): 5. CrossRef - Corneal confocal microscopy detects small nerve fibre damage in patients with painful diabetic neuropathy
Alise Kalteniece, Maryam Ferdousi, Shazli Azmi, Womba M. Mubita, Andrew Marshall, Giuseppe Lauria, Catharina G. Faber, Handrean Soran, Rayaz A. Malik
Scientific Reports.2020;[Epub] CrossRef - The Association of Fasting C-peptide with Corneal Neuropathy in Patients with Type 2 Diabetes
Anju Zuo, Chuan Wang, Lili Li, Jingru Qu, Juan Cao, Li Chen, Solomon Tesfaye, Wenjuan Li, Xinguo Hou, Vincenza Spallone
Journal of Diabetes Research.2020; 2020: 1. CrossRef - Performance analysis of noninvasive electrophysiological methods for the assessment of diabetic sensorimotor polyneuropathy in clinical research: a systematic review and meta-analysis with trial sequential analysis
Fahmida Haque, Mamun Bin Ibne Reaz, Sawal Hamid Md Ali, Norhana Arsad, Muhammad Enamul Hoque Chowdhury
Scientific Reports.2020;[Epub] CrossRef - Tear film substance P: A potential biomarker for diabetic peripheral neuropathy
Shyam Sunder Tummanapalli, Mark D.P. Willcox, Tushar Issar, Aimy Yan, Jana Pisarcikova, Natalie Kwai, Ann M. Poynten, Arun V. Krishnan, Maria Markoulli
The Ocular Surface.2019; 17(4): 690. CrossRef - Characterizing distal peripheral neuropathy in type 2 diabetes mellitus in a semi-urban community setting in Peru
Meera F Iyengar, Antonio Bernabe-Ortiz
Journal of Global Health Reports.2019;[Epub] CrossRef - Diabetic peripheral neuropathy: advances in diagnosis and strategies for screening and early intervention
Dinesh Selvarajah, Debasish Kar, Kamlesh Khunti, Melanie J Davies, Adrian R Scott, Jeremy Walker, Solomon Tesfaye
The Lancet Diabetes & Endocrinology.2019; 7(12): 938. CrossRef - Diabetic Peripheral Neuropathy as a Risk Factor for Sarcopenia
Tae Jung Oh, Yoojung Song, Jae Hoon Moon, Sung Hee Choi, Hak Chul Jang
Annals of Geriatric Medicine and Research.2019; 23(4): 170. CrossRef - Diabetic Neuropathy: New Insights to Early Diagnosis and Treatments
Mark Yorek, Rayaz A. Malik, Nigel A. Calcutt, Aaron Vinik, Soroku Yagihashi
Journal of Diabetes Research.2018; 2018: 1. CrossRef - Use of parenteral vitamin B complexes in treatment of polyneuropathy
O. V. Kurushina, A. E. Barulin, O. I. Agarkova
Medical Council.2018; (18): 62. CrossRef - Circulating microRNAs as biomarkers for diabetic neuropathy: A novel approach
Eleni Xourgia, Athanasia Papazafiropoulou, Andreas Melidonis
World Journal of Experimental Medicine.2018; 8(3): 18. CrossRef
 PubReader
PubReader Cite
Cite