Being Metabolically Healthy, the Most Responsible Factor for Vascular Health
Article information

Abstract
The prevalence of obesity is rapidly increasing worldwide. One-thirds of world population is suffering from the deleterious effects of excessive fat and adipose tissue in their body. At the same time, the average life expectancy is becoming higher and higher every decade. Therefore, living healthy and longer is the dream for everyone. Simply being obese is not the primary cause for the consequence of obesity; rather, the depot where the fat is accumulated, is the primary key for the deleterious effects of obesity. Results from historical research suggest that visceral fat increases the risk for cardiovascular and metabolic diseases, such as diabetes, myocardial infarction and ischemic stroke, not subcutaneous fat. Therefore, body mass index (BMI), which reflects body weight relative to height might not reflect the appropriate size of metabolic burden of fat in our body. In contrast, waist circumference, which reflects abdominal obesity, would mirror the metabolic burden of fat better than BMI. Visceral fat is the marker of ectopic fat accumulation. In this review, I will introduce my researches mainly involved in uncovering the clues to the link between metabolic health and cardiovascular disease.
INTRODUCTION
Obesity is renowned for its comorbid diseases, such as diabetes, atherosclerosis, metabolic syndrome (MetS) and sleep apnea [123]. The prevalence of obesity in adults older than 30 is reaching 30% worldwide, and this high rate of obesity is more pronounced in Asians, due to the rapid change of diet patterns and sedentary life style [4]. The propensity of Asians for high prevalence of visceral obesity contributes for the markedly increasing prevalence of diabetes and MetS [5]. The results of recent studies focus not only on the obesity itself, but on the depots where the fat is actually accumulating [67].
Abdominal obesity is known to be a major risk factor for diabetes and cardiovascular disease (CVD) [8]. The cluster of diseases, that is, ‘syndrome’ caused by abdominal obesity is called MetS [9]. It has long been considered as the main cause for the increased risk for CVD in subjects with abdominal obesity and many kinds of metabolic disease. The components of MetS insulin resistance, hypertension, hyperglycemia, systemic inflammation, atherogenic dyslipidemia and consequently, atherosclerosis (Fig. 1).
The components of metabolic health and metabolic syndrome.
Kangbuk Samsung Health Study (KSHS) is one of the largest health screening cohort prospectively and retrospectively ongoing in Koreans, and it is known to screening more than 100,000 subjects every year. As a clinical and researcher working in Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, the author could have full access to the dataset of KSHS. In this review, I would like to discuss about the clinical implication and current knowledge about MetS and metabolically healthy obesity (MHO) and their impacts on vascular health, mainly focusing on the results analyzed from KSHS data.
PREVALENCE AND DEFINITION OF MetS
The prevalence of MetS is consistently being reported to be around 30% of the study population, which shows pretty constant rate in spite of different study population [10]. In a study performed in more than 40,698 Korean participants in KSHS, the prevalence of MetS differed according to the criteria used to diagnose MetS, and this study was the first study that suggested that different definition of abdominal obesity should be used in Asian population compared to that in Caucasians in the diagnosis of MetS [11].
A very initial study from our research group reported the relationship between systemic inflammation and insulin resistance [12]. In this study, we reported that MetS and insulin resistance are associated with systemic inflammation assessed by high C-reactive protein (CRP). In another study by Park et al. [13], those with high insulin resistance index assessed by homeostasis model assessment of insulin resistance (HOMA-IR) had significantly high risk for MetS compared with those with low HOMA-IR. In addition, we reported that in those with impaired fasting glucose, the insulin resistance index and high-sensitivity CRP (hs-CRP) increased gradually even in the normal fasting glucose range [14]. In reverse, in the study by Jung et al. [15], the risk for future MetS was the highest in those with the highest quartile of hs-CRP, suggesting the increased risk for MetS in those with high systemic inflammation.
MetS AND CARDIOVASCULAR RISK FACTORS
We reported some studies regarding the relationship between surrogate markers or indices related with glycemia and MetS. In 40,155 participants in KSHS, a glycosylated hemoglobin of 5.45% predicted the presence of MetS [16]. In the study by Park et al. [17], in 465 participants in whom adipocytokines were measured, those with higher baseline serum fatty-acid binding protein (FABP)-4 levels showed significant association with future development of MS after 4 years of follow-up. In another study by Sung et al. [18], in which 2,350 subjects were followed up for 4 years, those with high baseline fasting insulin levels were independently associated with future development of MetS. In the study by Kim et al. [19], higher serum alkaline phosphatase levels was a significant predictor for future MetS development, and Jung et al. [20] showed significant association of elevated white blood cell count with incident MetS.
MetS AND CARDIOVASCULAR RISK
Many studies already reported increased cardiovascular risk in subjects with MetS. Results from meta-analyses report 2- to 5-fold increased risk for cardiovascular mortality in subjects with MS [21]. The mechanisms for increased CVD risk in subjects with MetS are explained by the definition of MetS, in that, MetS itself is the cluster of cardiovascular risk factors [22]. Hyperinsulinemia, hyperglycemia, increased systemic inflammation and visceral obesity and dyslipidemia, all attribute to the development of atherosclerosis and consequent CVD.
In 155,971 participants in KSHS from 2002 to 2009 with mean age of 42 years without previous history of CVD (median follow-up of 3.7 years), mortality data were obtained based on nationwide death certificate data of Korea National Statistical Office [23]. We observed an increased risk for all-cause and CVD mortality in subjects with MetS. However, these increased risk were attenuated after exclusion of subjects with diabetes or hypertension, suggesting that inclusion of these extreme metabolic disease accounts for the increased CVD mortality attributable to MetS. The result of our study suggests reconciliation of existence of MetS or the need for re-definition of MetS.
THE DELETERIOUS EFFECTS OF ABDOMINAL OBESITY
Obesity could be defined by many parameters, such as increased waist circumference (WC), increased body mass index (BMI), increased weight, increased waist-hip ratio (WHR) and recently increased waist-height ratio (WHtR) [2425]. Recent researches support the deleterious effect of abdominal obesity versus affirmative effect of subcutaneous fat [26]. However, due to the convenience and the reproducibility, BMI is still frequently used in the screening of obesity in large study population.
Coronary artery calcification (CAC) is considered as a non-invasive, convenient, and accurate surrogate marker for the prediction of cardiovascular burden and CVD event from the results of many famous cohort studies [27]. In KSHS, around 10% of the participants perform coronary artery calcium score (CACS) test every year. Therefore, KSHS has a large cohort of CACS, followed up for many years.
Park et al. [28], analyzed the association among WC, BMI, and CAC. In 33,433 participants in KSHS in whom CACS were available, the risk for CAC increased as BMI increased with 1.3-fold increased risk of CAC in the obese group versus normal group. When the participants were divided into six groups according to BMI and WC, obese group defined by BMI with abdominal obesity showed the highest risk for CAC followed by those with BMI in the overweight range with abdominal obesity defined by WC, suggesting the WC as a marker of obesity is more predictive of CAC than BMI.
In 945 participants in KSHS, the association of body composition with CAC was analyzed [29]. Body composition analyses were performed with bioelectrical impedance analysis method and WHR was used as the marker of abdominal obesity. The subjects with high CACS showed significantly higher mean WHRs and lower mean values of Lean body mass compared with those without CAC. In logistic regression analysis with CAC as the dependent variable, those with the highest quartile of WHR showed a 3-fold increased risk for CAC compared with the lowest quartile of WHR, suggesting WHR was the significant predictor for CAC.
Recent studies suggest WHtR as an easy and inexpensive adiposity index that reflects central obesity [30]. In 2,900 nondiabetic participants in KSHS, Son et al. [31] analyzed the association between baseline WHtR and development of diabetes after 4 years. The cutoff of WHtR for diabetes development was 0.51, and WHtR showed almost similar predictive effect for diabetes development as WC. In another study by Oh et al. [32], 1,048 male participants in KSHS were analyzed for the association between baseline WHtR and progression of CAC after 4 years. In this study, they showed that increased baseline WHtR was associated with increased risk of CAC progression after 4 years, suggesting WHtR might be a useful tool to identify individuals at high risk for subclinical atherosclerosis.
Nonalcoholic fatty liver disease (NAFLD) is considered as the marker of insulin resistance and ectopic fat accumulation [33]. Recent studies suggest NAFLD as the cardiovascular risk factors due to multiple mechanisms [34]. We wondered whether NAFLD or WC would predict CAC better than the other. In 21,335 male participants of KSHS in whom CACS data were available, we analyzed the association between NAFLD, abdominal obesity and CAC [35]. In logistic regression analysis with CAC as the dependent variable, those with NAFLD and abdominal obesity showed significantly increased risk of CAC compared with those without either abnormality. Interestingly, those with NAFLD but without abdominal obesity showed significantly increased risk for CAC with odds ratio of 1.286. In contrast, those with only abdominal obesity but without NAFLD did not show increased risk of CAC compared with those without either abnormalities, suggesting that NAFLD is more closely related with CAC than abdominal obesity.
Hypertriglyceridemic waist (HTGW) phenotype is a recently recommended concept that reflects those with high risk for CVD and also those with metabolically unhealthiness [36]. We divided 32,186 participants in KSHS into four groups with normal WC-normal triglyceride (TG) levels, normal WC-high TG levels, enlarged WC-normal TG levels, and enlarged WC-high TG levels [37], and analyzed their association with CAC. Those with enlarged WC and high TG levels showed the highest mean value of CACS followed by those with normal WC and high TG levels, suggesting this HTGW phenotype as a useful marker for detection of subjects with high cardiometabolic risk. In another study performed in 2,900 participants in KSHS, Han et al. [38] analyzed this HTGW phenotype with incident diabetes after 4 years. Those with enlarged WC and high TG showed 2.4-fold increased risk for diabetes development after 4 years, suggesting this HTGW phenotype could be a useful marker to detect those with high risk for diabetes.
Visceral adiposity index (VAI) is a mathematical tool that reflects a subject's visceral adiposity and insulin resistance [39]. Recent studies have noted an association between VAI and cardiovascular event [40]. We analyzed the association between VAI and CACS in 33,468 participants in KSHS [41]. CACS was positively correlated with VAI and subjects with high CACS had significantly higher VAI compared to those with CACS of zero. The subjects with the highest tertile of VAI had significantly increased odds ratio for CACS >0 compared to subject in the lowest tertile. These results suggested that high VAI reflects increased risk for subclinical atherosclerosis.
The last concept that defines metabolic health we've been interested, was triglyceridemic glucose (TyG) index [42]. This index is calculated from fasting TG levels and fasting glucose levels and is used to detect those with high risk for cardiometabolic risk. 2,900 non-diabetic participants in KSHS in whom health checkup was performed for 5 consecutive years, were divided into four groups according to the quartile groups of baseline TyG index [43]. Those with the highest quartile of TyG index showed significantly increased risk for diabetes development compared to the first quartile of TyG index. In addition, those with high TyG index (≥8.8) and BMI ≥25 kg/m2 showed significantly increased risk of diabetes development. From the results of this study, we found that TyG index could be a valuable marker for predicting diabetes.
THE CONCEPT OF ‘METABOLICALLY HEALTHY OBESITY’
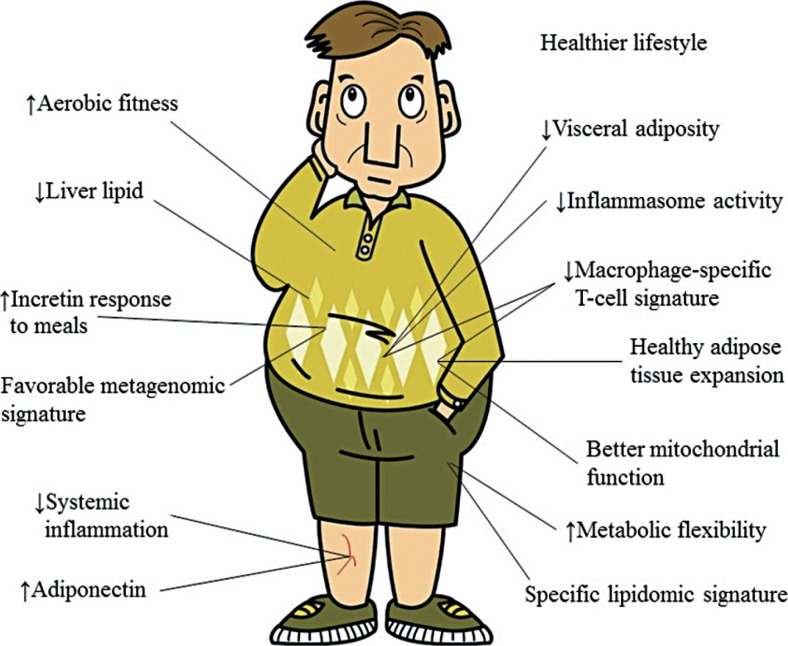
In 2012, there was interesting news by Reuter with the headline “Obesity not always tied to higher heart risk” [44]. This news was raised from a study by Hamer and Stamatakis [45], reporting the association of MHO with cardiovascular mortality. In 22,203 men and women without known history of CVD at baseline, the subjects were divided into four groups; metabolically healthy non-obese, metabolically unhealthy non-obese, MHO, and metabolically unhealthy obese. The definition of metabolic health was made based on high blood pressure, low high density lipoprotein cholesterol, diagnosis of diabetes, enlarged WC and CRP ≥3 mg/L. Those with less than two components among these were defined as metabolically healthy. After adjustment for multiple risk factors, metabolically unhealthy obese subjects showed 1.6-fold increased risk for CVD mortality compared with metabolically healthy non-obese subjects. Interestingly, MHO subjects, that is, BMI in obese range but did not have sufficient metabolically unhealthy components, showed similar risk for CVD mortality compared to those with metabolically healthy non-obese subjects. After the release of this study, many studies were published regarding this concept [4647]. MHO subjects seem to show very distinct features of decreased liver fat, increased mitochondrial function, decreased visceral adiposity and increased metabolic flexibility (Fig. 2).
We analyzed the association of MHO and CAC in KSHS cohort [48]. In 24,063 participants in KSHS in whom CACS data were available, metabolic health was defined by similar criteria as previously published studies. The subjects were divided into four groups according to metabolic health and obesity defined by BMI ≥25 kg/m2. Metabolically unhealthy obese subjects had significantly increased (upto 1.9-fold) risk for CAC compared to those with metabolically healthy non-obese subjects. Similar to the previous study, MHO subjects did not show significantly increased risk for CAC, suggesting the existence of MHO. In another study performed in 6,748 non-diabetic subjects in KSHS, MHO subjects showed not increased risk for diabetes development after 4 years compared to metabolic healthy non-obese subjects, supporting the existence of MHO.
The last proof of importance of metabolic health was the study performed using adipocytokines [49]. In 456 non-diabetic participants in KSHS in whom adipocytokines were measured, the subjects were divided into four groups according to obesity status and metabolic health. There were no significant differences in interleukin 6 or monocyte chemoattractant protein-1 levels among the groups, but levels of tumor necrosis factor α and FABP-4 were significantly higher in the metabolically unhealthy non-obese group compared to the metabolically healthy non-obese group, suggesting the association of adipocytokines with metabolic health.
CONCLUSIONS
In this review, I introduced numerous studies performed with the dataset of KSHS, most of which are my own work. Our data has the advantages of multiple metabolic parameters and the abundance in cardiometabolic risk factors. The strongest point is the large number of the participants in many years of repetitive health checkup. Although they are retrospective data, we could arrange the dataset as the cross-sectional, retrospective and consecutive dataset.
From the analyses of our data, we published many papers on the prevalence and definition of MetS initially, and its association with CVD. In addition, we could uncover the relationship between cardiometabolic risk factors and MetS. Recently, we are focusing on the importance of abdominal obesity and metabolic health in the prevention of CVD. We could conclude that not just being obese, but having abdominal obesity is more deleterious for metabolic health and subsequent CVD risk. Therefore, we have to inform our patients that to prevent development of diabetes and atherosclerosis, healthy life style and weight control is important more than any other strategies.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.