- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 40(2); 2016 > Article
-
Original ArticleOthers The Effect of Glycemic Status on Kidney Stone Disease in Patients with Prediabetes
- Tzu-Hsien Lien1, Jin-Shang Wu1,2, Yi-Ching Yang1,2, Zih-Jie Sun1,3, Chih-Jen Chang1,2
-
Diabetes & Metabolism Journal 2016;40(2):161-166.
DOI: https://doi.org/10.4093/dmj.2016.40.2.161
Published online: April 25, 2016
1Department of Family Medicine, National Cheng Kung University Hospital, Tainan, Taiwan.
2Department of Family Medicine, National Cheng Kung University College of Medicine, Tainan, Taiwan.
3Department of Family Medicine, National Cheng Kung University Hospital, Dou-Liou Branch, Douliu, Taiwan.
- Corresponding author: Chih-Jen Chang. Department of Family Medicine, National Cheng Kung University Hospital, 138 Sheng Li Road, Tainan 70403, Taiwan. em75210@email.ncku.edu.tw
- Corresponding author: Yi-Ching Yang. Department of Family Medicine, National Cheng Kung University Hospital, 138 Sheng Li Road, Tainan 70403, Taiwan. yiching@mail.ncku.edu.tw
• Received: December 17, 2015 • Accepted: March 28, 2016
Copyright © 2016 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- While the evidence supporting a positive association between diabetes mellitus and kidney stone disease (KSD) is solid, studies examining the association between impaired fasting glucose (IFG) and KSD show inconsistent results. Currently, there are no studies examining the relationship between impaired glucose tolerance (IGT) and KSD. The objective of this study is to investigate the effects of different glycemic statuses on KSD. The results may help to motivate patients with diabetes to conform to treatment regimens.
-
Methods
- We conducted a cross sectional study of a population that underwent health check-ups between January 2000 and August 2009 at the Health Evaluation Center of National Cheng Kung University Hospital. A total of 14,186 subjects were enrolled. The following categories of glycemic status were used according to the criteria of the 2009 American Diabetes Association: normal glucose tolerance, isolated IGT, isolated IFG, combined IFG/IGT, and diabetes. The existence of KSD was evaluated using renal ultrasonography, and the presence of any hyperechoic structures causing acoustic shadowing was considered to be indicative of KSD.
-
Results
- The prevalence of KSD was 7.4% (712/9,621), 9.3% (163/1,755), 10.8% (78/719), 12.0% (66/548), and 11.3% (174/1,543) in subjects with NGT, isolated IGT, isolated IFG, combined IFG/IGT, and diabetes, respectively. Isolated IFG, combined IFG/IGT, and diabetes were associated with KSD after adjusting for other clinical variables, but isolated IGT was not. Age (41 to 64 years vs. ≤40 years, ≥65 years vs. ≤40 years), male gender, hypertension, and hyperuricemia were also independently associated with KSD.
-
Conclusion
- Isolated IFG, combined IFG/IGT, and diabetes, but not isolated IGT, were associated with a higher risk of KSD.
- The prevalence of kidney stone disease (KSD) is increasing worldwide, and this increase is seen across sex, race, and age, with dietary changes possibly being a key driving force [1]. Several studies have described the association of KSD with metabolic syndrome and its components, such as central obesity, high blood pressure, hypertriglyceridemia, and hyperglycemia. These associations suggest that KSD is a systemic disease rather than an isolated kidney disorder [23456]. Growing evidence has shown that KSD not only increases the risk of metabolic syndrome, coronary artery disease, osteoporosis, and fracture but also leads to end stage renal disease [78].
- Diabetes mellitus (DM) is a chronic disease that is characterized by hyperglycemia, and its central feature is insulin resistance. The urologic complications associated with DM are an increasingly growing health concern. There is also epidemiological evidence that supports DM as a risk factor for the development of KSD [9]. However, the results of studies examining the associations between impaired fasting glucose (IFG), a component of metabolic syndrome, and KSD are inconsistent [35610111213]. Furthermore, there are currently no studies examining the relationship between impaired glucose tolerance (IGT) and KSD. Therefore, the aim of the current study was to evaluate the relationship between KSD and different glycemic statuses, including normal glucose tolerance (NGT), isolated IFG, isolated IGT, combined IFG/IGT, and DM.
INTRODUCTION
- We conducted a cross-sectional study using secondary data collected from the Prevention Health Center of National Cheng Kung University Hospital (NCKUH). Personal identification data were not included, so informed consent was not needed. This research was approved by the Institutional Review Board of NCKUH in Taiwan. Subjects with a history of any of the following were excluded: hypertension (n=2,023, including diuretics usage), KSD (n=240), primary hyperaldosteronism (n=4), chronic diarrhea (n=1), and intestinal resection surgery (n=5). A total of 14,186 eligible adult participants from Taiwan were enrolled (8,296 male and 5,890 female).
- The baseline data included demographic information, lifestyle habits (alcohol consumption, cigarette smoking, and regular exercise), and medical and medication histories. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Right arm systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured after subjects had been lying in a quiet examination room for five minutes in a supine position. After overnight fasting for at least 12 hours, blood and random urine samples were collected from all subjects. The tests included fasting plasma glucose (FPG), 2-hour postload plasma glucose (2h PG), total cholesterol (TC), triglyceride (TG), high density lipoprotein cholesterol (HDL-C), uric acid, creatinine, and routine urine analyses.
- Current alcohol use was defined as at least one alcoholic drink per week for more than half a year. Current smoking was defined as at least one pack per month for more than half a year. Regular exercise was defined as vigorous exercise for a minimum of 20 minutes each time, three times or more per week. Subjects were considered hypertensive if they had a SBP ≥140 mm Hg, a DBP ≥90 mm Hg, a history of hypertension or were taking anti-hypertensive medication [14]. Following the Nutrition and Health Survey in Taiwan, obesity was defined as a BMI of 27 kg/m2 [15]. Hypertriglyceridemia and high atherosclerotic index were defined as a TG level ≥1.69 mmol/L (150 mg/dL) and a TC/HDL-C level ≥4.5 in females and ≥5 in males [1617]. Male subjects with uric acid levels ≥416.4 µmol/L (7 mg/dL) and female subjects with uric acid levels ≥386.7 µmol/L (6.5 mg/dL) were classified as hyperuricemic based on reference values from the central laboratory. Glycemic status was categorized using the 2009 criteria of the American Diabetes Association [18]. Subjects were considered to have DM if they had a FPG ≥6.9 mmol/L (126 mg/dL), 2h PG ≥11.0 mmol/L (200 mg/dL), positive DM history or used hypoglycemic agents. Subject were considered to have NGT if they had a FPG <5.6 mmol/L (100 mg/dL), 2h PG <7.8 mmol/L (140 mg/dL) and no prior history of DM. Isolated IFG was defined as a FPG between 5.6 mmol/L (100 mg/dL) and 6.9 mmol/L (126 mg/dL) and 2h PG <7.8 mmol/L (140 mg/dL). Isolated IGT was defined as a 2h PG between 7.8 mmol/L (140 mg/dL) and 11 mmol/L (200 mg/dL) and FPG <5.6 mmol/L (100 mg/dL). Combined IFG/IGT was defined as a FPG between 5.6 mmol/L (100 mg/dL) and 6.9 mmol/L (126 mg/dL) and 2h PG between 7.8 mmol/L (140 mg/dL) and 11.0 mmol/L (200 mg/dL). Urine pH was classified into the following categories: pH <5.5, 5.5≤pH≤6.6, and ≥6.7. The existence of KSD was evaluated using renal ultrasonography (Toshiba Xario/SSA=660A Ultrasound Machine; Toshiba, Tokyo, Japan, with a 3.5-MHz transducer) to find any hyperechoic structures causing acoustic shadowing [4].
- The analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), with the data presented as the mean±standard deviations or percentages. Comparisons of clinical characteristics between those with and without KSD were carried out using Pearson chi-square tests for categorical data and independent samples t-tests for continuous data. Multiple logistic regressions were used to determine whether glycemic status was associated independently with the presence of KSD after adjusting for other variables, including age (≤40, 41 to 64, and ≥65 years), sex, TC/HDL-C, hypertriglyceridemia, hyperuricemia, obesity, hypertension, urine pH, current smoking, current alcohol use, and regular exercise. The odds ratios (ORs) and 95% confidence intervals (CIs) of the predictors were derived from the regression model. Statistical significance was defined as a P≤0.05.
METHODS
- The overall prevalence of KSD was 8.4% (1,193/14,186). Table 1 shows a summary of the clinical characteristics of the study population. Males were predominant in the KSD group. Age, BMI, SBP, DBP, TC, TG, FPG, 2h PG, uric acid, and urine pH were all significantly higher than in the non-KSD group, while HDL-C was significantly lower in the KSD group. KSD subjects were more likely to have hypertension than non-KSD subjects. The distributions of the atherosclerotic index, current smoking status, current alcohol use, and regular exercise were similar in both groups.
- Table 2 presents the ORs and 95% CIs of the independent variables for predicting KSD from multiple logistic regression analyses. Isolated IFG, combined IFG/IGT, and DM were positively associated with KSD. However, after adjusting for other clinical variables, isolated IGT was not. Compared with the younger subjects (≤40 years), both the middle-aged (41 to 64 years) and elderly (≥65 years) groups had a higher risk of developing KSD. Other independently associated factors included the male gender and hyperuricemia.
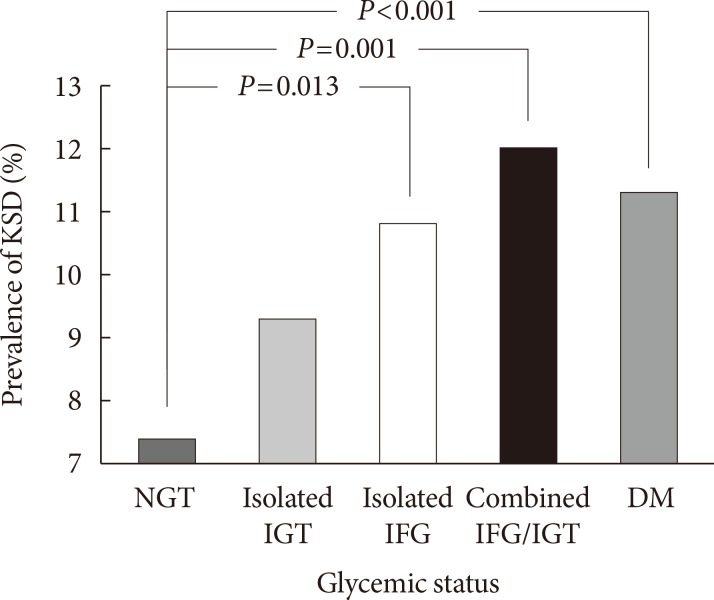
- Fig. 1 shows the comparisons of the KSD prevalence among subjects with different glycemic statuses. There was a significant incremental trend of an increasing KSD prevalence in subjects with NGT, isolated IGT, isolated IFG, and combined IFG/IGT to DM (P for trend <0.001). Based on post hoc analysis, subjects with isolated IFG, combined IFG/IGT, and DM had a significantly higher prevalence of KSD than the NGT group, but subjects with isolated IGT did not.
RESULTS
- The positive association between DM and KSD has been well documented [29], but the relationship between pre-diabetes and KSD is still inconsistent. Some previous studies have found that IFG is independently associated with an increased risk of KSD [1213], while others did not [3561011]. As for the effect of IGT on KSD, no studies to date have been carried out examining this relationship. In addition to DM, the current study shows that combined IFG/IGT and isolated IFG, but not isolated IGT, are associated with an increased risk of KSD. To the best of our knowledge, this study was the first to examine the association between KSD and different glycemic statuses using fasting and postload plasma glucose measurements simultaneously.
- One of the most well-known mechanisms of stone formation in hyperglycemic subjects is insulin resistance. Meanwhile, the severity of insulin resistance is higher in subjects with combined IFG/IGT and IFG than in subjects with IGT [19]. This may explain the different effects of combined IFG/IGT, isolated IFG and isolated IGT on KSD that were observed in this study. Insulin resistance could lead to decreased urinary ammonium excretion and lower urinary citrate excretion through a decrease in ammonia production and Na+/H+ antiport dysfunction [42021]. In addition, hyperglycemia-related glycosuria could cause an isonatric inhibition of proximal tubular sodium, glucose and calcium reabsorption, resulting in higher urinary uric acid and calcium excretion [222324].
- Studies have reported conflicting evidence regarding the association between IFG and KSD. The results observed in this study were in accordance with two other Korean studies that revealed a significant association between IFG and KSD [1213]. However, other studies have reported an insignificant relationship [3561011]. One reason for the difference may be that none of these earlier studies considered postload blood glucose in the classification of glycemic status. Perhaps the IFG subjects in previous studies would have been classified as IGT or DM subjects if postload glucose had been considered, and the lack of these data could have resulted in an overestimation of the association between IFG and KSD. In addition, the different cutoff value for IFG, 6.1 mmol/L instead of 5.6 mmol/L, could also have led to an overstatement of the relationship. Another possible reason may be related to the use of different methods for selecting subjects and KSD components. In summary, this study was the first to adopt a detailed definition of glycemic status and then use these criteria to divide the subjects into additional groups. The results of this work may thus provide more robust evidence for the association between different glycemic statuses and KSD.
- Some of our findings were consistent with those of previous studies reporting that male gender, increasing age and hyperuricemia were associated with an increase in KSD incidence [12526]. However, in contrast to other studies [2728], we did not observe a relationship between urine pH and KSD. The average urine pH of both the KSD (6.2±0.7) and non-KSD groups (6.1±0.7) in this study were higher than those reported in other studies (5.45±0.27 to 6.05±0.42) [2728], which might be the reason for the insignificant association between urine pH and KSD in this paper. Furthermore, the current study lacked the urine pH and biochemical data from the 24-hour urine collections. The subjects in this study were also on random outpatient diets, which may influence urine pH. As for the lack of association between obesity and KSD, the co-linearity effects of hyperglycemia, hyperuricemia, and hypertriglyceridemia may partially explain this insignificant relationship.
- One distinguishing feature of this study was that the analysis included explicit categorizations of different glycemic statuses, comprising NGT, isolated IFG, isolated IGT, combined IFG/IGT, and DM. Meanwhile, the pure isolated IFG and isolated IGT categories have rarely been used in previous studies and are mostly used to cross-reference each other. Several limitations of this study should be mentioned. First, because it was a cross-sectional study performed as a health examination in a university hospital, rather than a longitudinal study, we could not confirm whether a causal relationship existed between glycemic control and the risk of KSD. Second, as mentioned previously, we did not have the biochemical data from the 24-hour urine collections, and the urine pH for this study was measured by dipstick urinalysis using a random spot urine sample. Third, the study was limited by a lack of data from the stone composition analyses. Therefore, we were not able to determine whether the different glycemic statuses were associated with certain urinary components or stone types. Fourth, this study did not include plasma insulin data, which kept us from presenting the insulin resistance index. Finally, the diagnosis was made by ultrasonography instead of non-contrast computed tomography, and this may have led us to an underestimation of the prevalence the KSD [29]. Nonetheless, the sensitivity of ultrasonography in the detection of kidney stones has been documented to be 96% [30]. The European Association of Urology also suggested ultrasonography as a primary diagnostic imaging tool in their 2015 urolithiasis guidelines.
- In conclusion, isolated IFG, combined IFG/IGT, and DM, rather than isolated IGT, were associated with a higher risk of KSD in this study. In addition, subjects of the male gender who were at least forty and had hyperuricemia also exhibited a greater risk of developing KSD.
DISCUSSION
-
Acknowledgements
- I would like to take this opportunity to express gratitude to all of the department faculty members for their help and support. I would also like to express my gratitude to the one and all who, either directly or indirectly, have lent their support to this paper.
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
- 1. Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol 2010;12:e86-e96. PubMedPMC
- 2. Lieske JC, de la Vega LS, Gettman MT, Slezak JM, Bergstralh EJ, Melton LJ 3rd, Leibson CL. Diabetes mellitus and the risk of urinary tract stones: a population-based case-control study. Am J Kidney Dis 2006;48:897-904. ArticlePubMed
- 3. Jeong IG, Kang T, Bang JK, Park J, Kim W, Hwang SS, Kim HK, Park HK. Association between metabolic syndrome and the presence of kidney stones in a screened population. Am J Kidney Dis 2011;58:383-388. ArticlePubMed
- 4. Sakhaee K. Nephrolithiasis as a systemic disorder. Curr Opin Nephrol Hypertens 2008;17:304-309. ArticlePubMed
- 5. Kabeya Y, Kato K, Tomita M, Katsuki T, Oikawa Y, Shimada A, Atsumi Y. Associations of insulin resistance and glycemic control with the risk of kidney stones. Intern Med 2012;51:699-705. ArticlePubMed
- 6. Chang IH, Lee YT, Lee DM, Kim TH, Myung SC, Kim YS, Ahn SH. Metabolic syndrome, urine pH, and time-dependent risk of nephrolithiasis in Korean men without hypertension and diabetes. Urology 2011;78:753-758. ArticlePubMed
- 7. Sakhaee K. Recent advances in the pathophysiology of nephrolithiasis. Kidney Int 2009;75:585-595. ArticlePubMed
- 8. Sakhaee K, Maalouf NM, Kumar R, Pasch A, Moe OW. Nephrolithiasis-associated bone disease: pathogenesis and treatment options. Kidney Int 2011;79:393-403. ArticlePubMed
- 9. Taylor EN, Stampfer MJ, Curhan GC. Diabetes mellitus and the risk of nephrolithiasis. Kidney Int 2005;68:1230-1235. ArticlePubMed
- 10. Kim YJ, Kim CH, Sung EJ, Kim SR, Shin HC, Jung WJ. Association of nephrolithiasis with metabolic syndrome and its components. Metabolism 2013;62:808-813. ArticlePubMed
- 11. Rendina D, Mossetti G, De Filippo G, Benvenuto D, Vivona CL, Imbroinise A, Zampa G, Ricchio S, Strazzullo P. Association between metabolic syndrome and nephrolithiasis in an inpatient population in southern Italy: role of gender, hypertension and abdominal obesity. Nephrol Dial Transplant 2009;24:900-906. ArticlePubMed
- 12. Cho ST, Jung SI, Myung SC, Kim TH. Correlation of metabolic syndrome with urinary stone composition. Int J Urol 2013;20:208-213. ArticlePubMed
- 13. Jung HS, Chang IH, Kim KD, Moon YT, Kim TH, Myung SC, Kim YS, Lee JY. Possible relationship between metabolic syndrome traits and nephrolithiasis: incidence for 15 years according to gender. Korean J Urol 2011;52:548-553. ArticlePubMedPMC
- 14. Pak CY, Sakhaee K, Moe O, Preminger GM, Poindexter JR, Peterson RD, Pietrow P, Ekeruo W. Biochemical profile of stone-forming patients with diabetes mellitus. Urology 2003;61:523-527. ArticlePubMed
- 15. Pan WH, Flegal KM, Chang HY, Yeh WT, Yeh CJ, Lee WC. Body mass index and obesity-related metabolic disorders in Taiwanese and US whites and blacks: implications for definitions of overweight and obesity for Asians. Am J Clin Nutr 2004;79:31-39. ArticlePubMed
- 16. Pejic RN, Lee DT. Hypertriglyceridemia. J Am Board Fam Med 2006;19:310-316. ArticlePubMed
- 17. Millan J, Pinto X, Munoz A, Zuniga M, Rubies-Prat J, Pallardo LF, Masana L, Mangas A, Hernandez-Mijares A, Gonzalez-Santos P, Ascaso JF, Pedro-Botet J. Lipoprotein ratios: physiological significance and clinical usefulness in cardiovascular prevention. Vasc Health Risk Manag 2009;5:757-765. PubMedPMC
- 18. American Diabetes Association. Standards of medical care in diabetes: 2009. Diabetes Care 2009;32(Suppl 1):S13-S61. ArticlePubMedPMCPDF
- 19. Abdul-Ghani MA, Jenkinson CP, Richardson DK, Tripathy D, DeFronzo RA. Insulin secretion and action in subjects with impaired fasting glucose and impaired glucose tolerance: results from the Veterans Administration Genetic Epidemiology Study. Diabetes 2006;55:1430-1435. PubMed
- 20. Cupisti A, Meola M, D'Alessandro C, Bernabini G, Pasquali E, Carpi A, Barsotti G. Insulin resistance and low urinary citrate excretion in calcium stone formers. Biomed Pharmacother 2007;61:86-90. ArticlePubMed
- 21. Sakhaee K, Maalouf NM, Sinnott B. Clinical review. Kidney stones 2012: pathogenesis, diagnosis, and management. J Clin Endocrinol Metab 2012;97:1847-1860. PubMedPMC
- 22. Nagasaka S, Murakami T, Uchikawa T, Ishikawa SE, Saito T. Effect of glycemic control on calcium and phosphorus handling and parathyroid hormone level in patients with non-insulin-dependent diabetes mellitus. Endocr J 1995;42:377-383. ArticlePubMed
- 23. Thalassinos NC, Hadjiyanni P, Tzanela M, Alevizaki C, Philokiprou D. Calcium metabolism in diabetes mellitus: effect of improved blood glucose control. Diabet Med 1993;10:341-344. ArticlePubMed
- 24. Cook DG, Shaper AG, Thelle DS, Whitehead TP. Serum uric acid, serum glucose and diabetes: relationships in a population study. Postgrad Med J 1986;62:1001-1006. ArticlePubMedPMCPDF
- 25. Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol 2000;13(Suppl 3):S45-S50. PubMed
- 26. Gutman AB, Yu TF. Uric acid nephrolithiasis. Am J Med 1968;45:756-779. ArticlePubMed
- 27. Cameron MA, Maalouf NM, Adams-Huet B, Moe OW, Sakhaee K. Urine composition in type 2 diabetes: predisposition to uric acid nephrolithiasis. J Am Soc Nephrol 2006;17:1422-1428. PubMed
- 28. Maalouf NM, Cameron MA, Moe OW, Sakhaee K. Metabolic basis for low urine pH in type 2 diabetes. Clin J Am Soc Nephrol 2010;5:1277-1281. ArticlePubMedPMC
- 29. Portis AJ, Sundaram CP. Diagnosis and initial management of kidney stones. Am Fam Physician 2001;63:1329-1338. PubMed
- 30. Middleton WD, Dodds WJ, Lawson TL, Foley WD. Renal calculi: sensitivity for detection with US. Radiology 1988;167:239-244. ArticlePubMed
REFERENCES
Fig. 1

Prevalence of kidney stone disease (KSD) with different glycemic statuses. Significant differences were observed between the normal glucose tolerance (NGT) and diabetes mellitus (DM) groups (P<0.001), between the NGT and combined impaired glucose tolerance (IGT)/impaired fasting glucose (IFG) groups (P=0.001), and between the NGT and DM groups (P=0.013).
Table 1
![dmj-40-161-i001.jpg]()
Comparison of the clinical parameters of subjects with and without kidney stone disease
Table 2
![dmj-40-161-i002.jpg]()
Multiple logistic regression model for the relationship between glycemic status and kidney stone disease
Figure & Data
References
Citations
Citations to this article as recorded by 
- Related Risk Factor Analysis for Upper Urinary Tract Stones in Patients with Abnormal Glucose Metabolism
泽伟 于
Advances in Clinical Medicine.2022; 12(02): 749. CrossRef - Nephrolithiasis: A Red Flag for Cardiovascular Risk
Alessia Gambaro, Gianmarco Lombardi, Chiara Caletti, Flavio Luciano Ribichini, Pietro Manuel Ferraro, Giovanni Gambaro
Journal of Clinical Medicine.2022; 11(19): 5512. CrossRef - Association between metabolic syndrome components and the risk of developing nephrolithiasis: A systematic review and bayesian meta-analysis
Ilham Akbar Rahman, Ilham Fauzan Nusaly, Syakri Syahrir, Harry Nusaly, Makbul Aman Mansyur
F1000Research.2021; 10: 104. CrossRef - Glycemic Status, Insulin Resistance, and the Risk of Nephrolithiasis: A Cohort Study
Seolhye Kim, Yoosoo Chang, Hyun-Suk Jung, Young Youl Hyun, Kyu-Beck Lee, Kwan Joong Joo, Heung Jae Park, Young-Sam Cho, Hyeonyoung Ko, Eunju Sung, Hocheol Shin, Seungho Ryu
American Journal of Kidney Diseases.2020; 76(5): 658. CrossRef - Associations between nephrolithiasis and diabetes mellitus, hypertension and gallstones: A meta‐analysis of cohort studies
Bing‐Biao Lin, Rong‐Hua Huang, Bing‐Liang Lin, Ying‐Kai Hong, Ming‐En Lin, Xue‐Jun He
Nephrology.2020; 25(9): 691. CrossRef - Risk Factors for Urolithiasis (Review)
В. А. Слободянюк
Health of Man.2020; (1): 75. CrossRef - Re: Evidence of Disordered Calcium Metabolism in Adolescent Girls with Type 1 Diabetes: An Observational Study Using a Dual-Stable Calcium Isotope Technique
Dean G. Assimos
Journal of Urology.2018; 199(2): 335. CrossRef - Metabolic syndrome and uric acid nephrolithiasis: insulin resistance in focus
Leonardo Spatola, Pietro Manuel Ferraro, Giovanni Gambaro, Salvatore Badalamenti, Marco Dauriz
Metabolism.2018; 83: 225. CrossRef - Kidney stones diseases and glycaemic statuses: focus on the latest clinical evidences
Leonardo Spatola, Claudio Angelini, Salvatore Badalamenti, Silvio Maringhini, Giovanni Gambaro
Urolithiasis.2017; 45(5): 457. CrossRef
 PubReader
PubReader Cite
Cite