Clinical Efficacy of Sodium-Glucose Cotransporter 2 Inhibitor and Glucagon-Like Peptide-1 Receptor Agonist Combination Therapy in Type 2 Diabetes Mellitus: Real-World Study (Diabetes Metab J 2022;46: 658–62)
Article information

We appreciate Dr. Tomoyuki Kawada’s comments on our recent article, “Clinical efficacy of sodium-glucose cotransporter 2 inhibitor and glucagon-like peptide-1 receptor agonist combination therapy in type 2 diabetes mellitus: real-world study” [1]. It is an honor to have the opportunity to respond to Dr. Kawada’s letter to Diabetes and Metabolism Journal.
First, we agree with Dr. Kawada that factors such as comorbidities, concurrent medications, and lifestyle could affect the results. However, as our study analyzed retrospectively collected data from medical chart reviews, information regarding lifestyle factors, such as exercise and nutritional intake, was insufficient. The primary aim of our study was to present evidence of combined sodium-glucose cotransporter 2 (SGLT2) inhibitor and glucagon-like peptide-1 (GLP-1) receptor agonist therapy in real-world practice. We believe that a prospective controlled study is necessary to consider all possible contributing factors.
Second, Dr. Kawada suggested undertaking a multiple regression analysis stratified by sex and the presentation of squared values of multiple regression coefficients (R2). We appreciate Dr. Kawada’s comment regarding the increase in the prevalence of dyslipidemia and obesity in menopause, which provided us with a different perspective for analyzing our results. First, the baseline characteristics were analyzed according to sex (Table 1). In our study population, dyslipidemia and obesity were more prevalent in males. We further conducted multiple regression analysis stratified by sex, and baseline glycosylated hemoglobin (HbA1c) was the only factor significantly affecting reduction in HbA1c level following combination therapy in both sexes (Table 2). The R2 values of baseline HbA1c were 0.172 for the total population and 0.149 and 0.189 for males and females, respectively. We believe that the relatively low R2 values are due to the small sample size of our study.
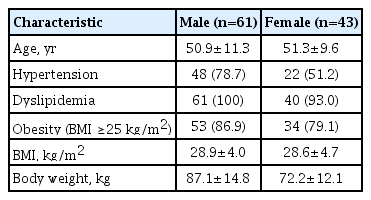
Baseline characteristics according to sex

Multiple linear regression analysis of HbA1c reduction after 1 year stratified by sex
Last, Dr. Kawada proposed a discussion regarding the cardiovascular benefits of the combination of SGLT2 inhibitor and GLP-1 receptor agonist. We agree that these two drug classes, both individually and combined, are effective in reducing the risk of cardiovascular disease and death by different mechanisms [2–4]. However, this aspect is out of the scope of this study, as the primary outcome of our study was the efficacy of the combination therapy in terms of glycemic control for at least 1 year. As our study was not designed to show cardiovascular or renal protection effects and merely showed maintenance of glycemic control following combination therapy in real-world clinical practice, we did not focus on the mechanism of each drug for improving glucose metabolism and cardiovascular outcomes. We believe that a succeeding study analyzing the cardiovascular and renal benefits in real-world practice could provide better evidence on this subject.
We are grateful for Dr. Kawada’s comprehensive review and valuable comments on our study. The limitations Dr. Kawada identified in our study will be appropriately handled in future studies.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.