- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 37(5); 2013 > Article
-
Original ArticleComplications Ruboxistaurin for the Treatment of Diabetic Peripheral Neuropathy: A Systematic Review of Randomized Clinical Trials
- Dipika Bansal1, Yogesh Badhan1, Kapil Gudala1, Fabrizio Schifano2
-
Diabetes & Metabolism Journal 2013;37(5):375-384.
DOI: https://doi.org/10.4093/dmj.2013.37.5.375
Published online: October 17, 2013
1Clinical Research Unit, Department of Pharmacy Practice, National Institute of Pharmaceutical and Education Research, Mohali, India.
2Clinical Pharmacology and Therapeutics, University of Hertfordshire, Hertfordshire, UK.
- Corresponding author: Dipika Bansal. Clinical Research Unit, Department of Pharmacy Practice, National Institute of Pharmaceutical Education and Research, Sector 67, S.A.S. Nagar, Mohali 160062, India. dipikabansal079@gmail.com
Copyright © 2013 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Diabetic peripheral neuropathy (DPN) is a common complication of diabetes mellitus. Protein kinase C (PKC) inhibitor's has been thought to be a potential disease modifying drug's in DPN as it slows or reverse neuropathy's progression. To assesses the efficacy and safety of ruboxistaurin on the progression of symptoms, signs, or functional disability in DPN.
-
Methods
- A systematic review of the literature databases like PubMed, ProQuest, EBSCO, EMBASE, and Cochrane Central was performed up to August 2012. We included randomized controlled trials (RCTs) comparing PKC inhibitor ruboxistaurin (RBX) with control and lasting at least 6 months. Our primary outcome measure was change in neurological examination, measured by neurological total symptom score (NTSS) and vibration detection threshold (VDT). Secondary outcome measures were total quality of life (QoL), skin microvascular blood flow and others.
-
Results
- Six RCTs were included in review. Change in neurological function assessed by NTSS was reported in six studies, out of which significant difference between the RBX and placebo group seen in four studies favouring treatment group while remaining two studies reported no significant difference. VDT was assessed in only one study in which no significant difference seen between RBX and placebo group. Two studies reported significant improvement in QoL data. Safety data was reported in only two studies in which none of side effect was related to RBX.
-
Conclusion
- RBX had effects on DPN in some studies, but the evidence is not enough for meta-analysis and firm conclusion.
- Neuropathy is the one of the most common and debilitating long term complication of diabetes affecting up to 50% of patients [1-4]. Diabetic peripheral neuropathy (DPN) is defined in the clinical practice as the presence of symptoms and/or signs of peripheral nerve dysfunction in people with diabetes after the exclusion of other causes [5]. Prevalence of DPN may vary from 30% to 40% in type 1 and 2 diabetic patients [6]. Signs and symptoms of DPN vary depending on fiber type involved, with large fiber disease impairing proprioception and light touch. Small fiber disease impairs pain and temperature perception, leading to paresthesias, dysesthesias, and/or neuropathic pain. DPN may cause muscle weakness and diminished or absent deep-tendon reflexes, especially the Achilles tendon reflex. More advanced disease may lead to foot deformities like hammer toes, collapse of the mid foot, ulceration or neuroarthropathy (Charcot joints) of the foot may occur [7]. Symptoms may go unnoticed for a long period. Spread of the untreated infection to bone may lead to amputation. The immense physical, psychological, and economic cost of diabetic neuropathy underscore the need for causally targeted therapies [7].
- Several pathogenetic mechanisms have been proposed for diabetic neuropathy (DN) like polyol pathway, glycation, myoinositol, oxidative stress, nerve hypoxia, and protein kinase C (PKC), etc. [8]. The classes of drugs used to treat DPN based on these mechanisms are aldose reductase inhibitor (ARI) [9], vasodilators, PKC-β inhibitors [10], and others [8]. The prevention of the onset or modifying the natural history of DPN by targeting known pathogenetic mechanisms is mostly in experimental stages and not therefore available for clinical usage at present.
- ARIs like sorbinil, tolrestat, ponalrestat, zopolrestat, zenarestat, epalrestat, ranirestat, and fidarestat have been found to be acting on the progression of DN [9]. Recent Cochrane review of 32 clinical trials (n=4,970) revealed no statistically significant overall benefit of ARI in DN [11]. Only one ARI molecule epalrestat is approved for clinical use in Japan [12].
- Another important class of drug to be used in DPN is PKC-β inhibitors. The putative mechanism is that intracellular hyperglycaemia cause increase in diacylglycerol (DAG) levels, activating PKC formation, leading to multiple pathogenetic consequences including altered expression of endothelial nitric oxide synthetase and angiogenic protein vascular endothelial growth factor (VEGF). This leads to the development of diabetic complications like neuropathy. PKC pathway activation alters vasoconstriction and capillary permeability, and can cause hypoxia, angiogenesis, basement membrane thickening, and endothelial proliferation. These changes in neurovascular blood flKC are the likely source of PKC's role in neuropathy. Thus PKC inhibitor has been thought to be a potential disease modifying drug in DPN [10].
- Ruboxistaurin (RBX) is an orally active PKC-β inhibitor. It binds to the active site of PKC-β, thus interfering with adenosine triphosphate binding and inhibiting phosphorylation of substrates. RBX gets metabolized by CYP3A4 to its main equipotent metabolite, N-desmethyl RBX [13]. The half-life of RBX and its metabolite combined is 24 hours, thereby allowing once daily dosing. Studies showed that the primary excretion route in humans for these substances was faecal with renal elimination playing a minor role. Thus, renal impairment does not preclude its use [14]. RBX can also be used for other diabetic complications like retinopathy, nephropathy, and heart failure.
- Treatments that could prevent, improve, or even slow the progression of DPN would result in decreased morbidity, cost and improved quality of life (QoL) of patients with diabetes mellitus. RBX is therefore considered a valuable target molecule for therapeutic intervention. The present systematic review assesses the efficacy and safety data available of RBX on the progression of symptoms, signs or functional disability in DPN.
INTRODUCTION
- Search strategy
- We searched for randomized controlled clinical trials on RBX in databases PubMed, ProQuest, EBSCO, EMBASE, and Cochrane Central up to August 2012. Keywords included: 'Ruboxistaurin, PKC inhibitor, LY 333531 AND Neuropathy, DPN, Diabetic polyneuropathy' where we kept limits namely 'Human' and 'Clinical trials.' We have also searched on American Diabetes Association website for conference proceedings. We also searched electronic registers of ongoing trials such as the Current Controlled Trials register (http://www.controlled-trials.com/). Bibliographies of the identified randomized trials were also searched. We also tried to contact the authors to identify additional published or unpublished data. We also searched (http://www.clinicaltrials.gov/) and found two registered clinical trials with clinical trial registry number NCT00044408 and NCT00044395; full published studies regarding these trials could not be retrieved.
- We included randomized controlled trials (RCTs), regardless of publication status, language, or period of patient inclusion. Intervention used was PKC inhibitor, i.e., RBX and compared with placebo and/or active comparator. As rate of progression of DPN is slow, any short-duration intervention will not produce a detectable effect. Therefore, only trials with treatment lasting at least 6 months and in which criteria for diagnosis of DPN was mentioned clearly with appropriate investigations to rule out other causes of neuropathy were included.
- Data collection and analysis
- An initial inclusion/exclusion form was used to assess study inclusion in the review. The titles and abstracts of every record retrieved by the searching process were scanned. The citations were divided alphabetically by first author and each citation was assessed for inclusion independently by two review authors. Discrepancies between assessments were resolved by discussion and when necessary, in consultation with the third review author. If disagreements could not be resolved at this stage, the full article was collected and assessed. If a trial was excluded at any time after this point, a record of both the article and exclusion criteria was kept in record.
- The methodological details and data from publications or unpublished study reports were extracted independently by two reviewers. The data extraction sheet included details of: 1) publication type and date; 2) study design including use of placebo; 3) duration and dose of treatment; 4) duration of follow-up; 5) details of the inclusion and exclusion criteria of the participants, numbers of participants, number of withdrawals, and reasons for withdrawals; 6) baseline characteristics; 7) outcome measures of study; 8) results of study; and 9) adverse drug reaction.
- Each included study was evaluated for the methodological quality. The characteristics assessed were; randomization methods, adequacy of allocation concealment, methods of patient and observer blinding. Each characteristic was graded as adequate, unclear, inadequate, or not done. Differences in grading by the evaluators were discussed and resolved by consensus.
- Improvement of sensory symptoms and nerve function were considered to be important end points [15]. For our review we considered assessment of change in neurological examination as a primary outcome. This can be done by measuring sensory symptoms and nerve function, for which neurological total symptom score scale (NTSS-6) [16] and vibration detection threshold (VDT) [17] are used respectively. As secondary outcome measure, change in neurological impairment score (NIS) [18], skin microvascular blood flow (SkBF) [19], QoL [20], safety profile and tolerability were considered.
- For assessment of QoL self administered 47 item Norfolk-DN questionnaire used to measure relationship between symptomatic DN and QoL from the perspective of patient. It is composed of two parts: questions related to symptoms experienced by patient and questions related to the impact of patient's neuropathy on activities of daily life [18].
- Statistical analysis
- No meta-analysis or quantitative analysis was possible due to significant heterogeneity between included studies in terms of study size, data reports, and procedure. Further, the inconsistencies in outcomes reported and the paucity of statistical data prevented quantitative meta-analysis. The review therefore consists of a qualitative assessment and narrative analysis to compare the studies. For the assessment of risk of bias in the included studies, analyses were undertaken using Review Manager 5 (RevMan; The Nordic Cochrane Centre, Copenhagen, Denmark). RevMan is the Cochrane collaboration's software for preparing and maintaining Cochrane reviews. Age of participant's at baseline of three studies has been compared using independent t-test using GraphPad Instat Demo 3 statistical software (GraphPad InStat Software, San Diego, CA, USA).
METHODS
Selection of studies
Data extraction and management
Assessment of risk of bias in included studies
Measures of treatment effect
- Search result
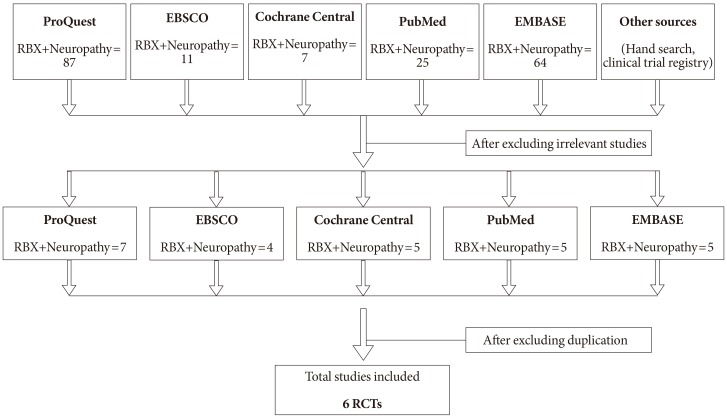
- Of the 296 studies retrieved from the literature databases, two conference abstracts [21,22] and four full text articles [17,19,20,23] met the inclusion criteria (Fig. 1). Six of these described RCTs were of at least six months duration. A study by Tesfaye et al. [24] was excluded as no intervention was administered and patients were only followed to understand the natural progression of DPN.
- We found three studies (one full text and two conference abstracts) [19,21,22] by same author name Carolina M. Casellini. We tried to find out whether those studies were done on same population by comparing the trial results. But study samples included in studies were found to be different and all three studies were included in our review. Casellini et al. [22] was performed as pilot study.
- Description of studies
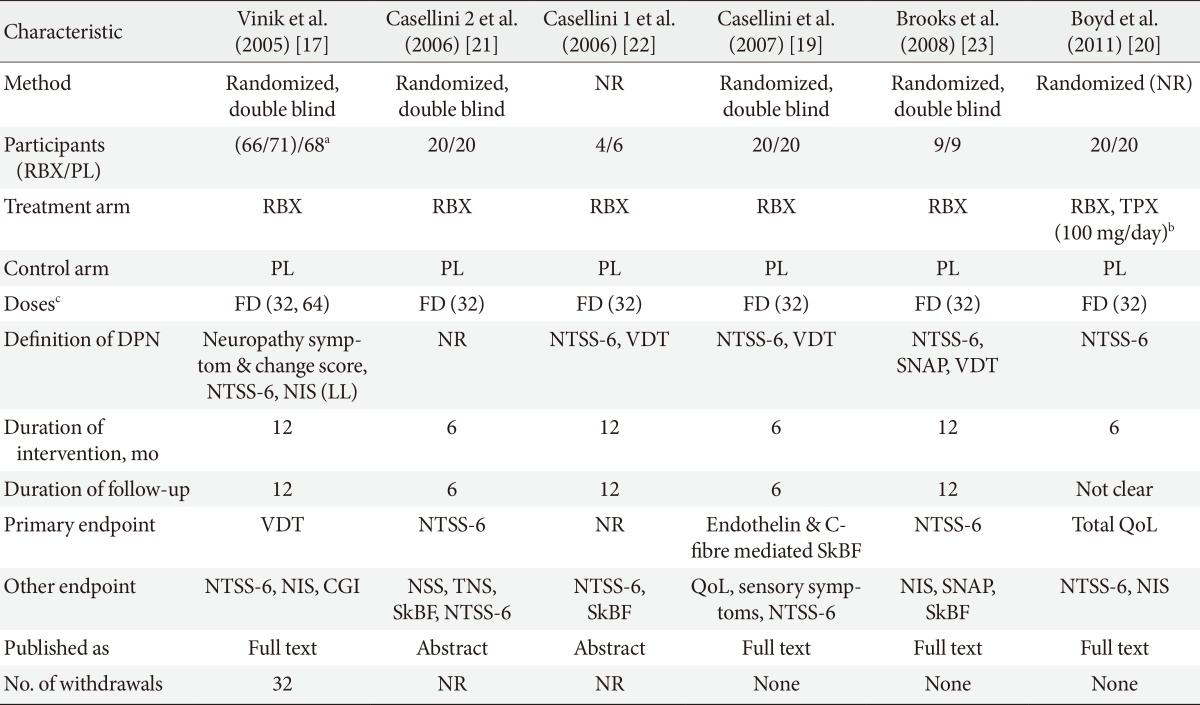
- Participants in the included studies received RBX (32 mg/day) or placebo as oral tablets for the specified duration of the study. In one study, Vinik et al. [17] two arms of RBX were used in which one received 32 mg/day and other received 64 mg/day dose of RBX.
- The included studies were all randomized and double blind except for two full text studies by Boyd et al. [20] and Casellini et al. [22] in which information regarding randomization and blinding was not reported (Table 1). Most studies lasted for 6 to 12 months and involved comparison of RBX (32 or 64 mg/day) and placebo. However, in study by Boyd et al. [20], topiramate (100 mg/day) was also used and compared with placebo. Diagnostic criterion for diabetes was not explicitly stated in most studies. Criteria for the diagnosis of DPN and the severity of the neuropathy, varied considerably from study to study. In most studies there was a reasonable attempt to exclude other causes of neuropathy.
- All studies recruited adult participants of 18 years and older. The six studies involved a total of 353 subjects, of which 210 received RBX, 123 received placebo, and 20 received topiramate. Both type 1 and 2 diabetic patients were recruited except in study by Boyd et al. [20] in which only type 2 diabetic patients were recruited.
- An attempt was also made to compare the baseline characteristics of participants in the included studies (Table 2). Only three studies by Vinik et al. [17], Boyd et al. [20], and Brooks et al. [23] had reported complete data regarding participant's age for the statistical analysis. The participants in the studies by Vinik et al. [17] and Brooks et al. [23] were significantly younger than in the study by Boyd et al. [20]. The other characteristics could not be compared because of lack of documented data.
- Fig. 2 shows the overall risk of bias involved in the studies based on sequence generation, allocation concealment, and blinding. There was unclear risk of bias in the majority of the studies based on random sequence generation and allocation concealment while high risk of bias was observed based on blinding of participants and observer.
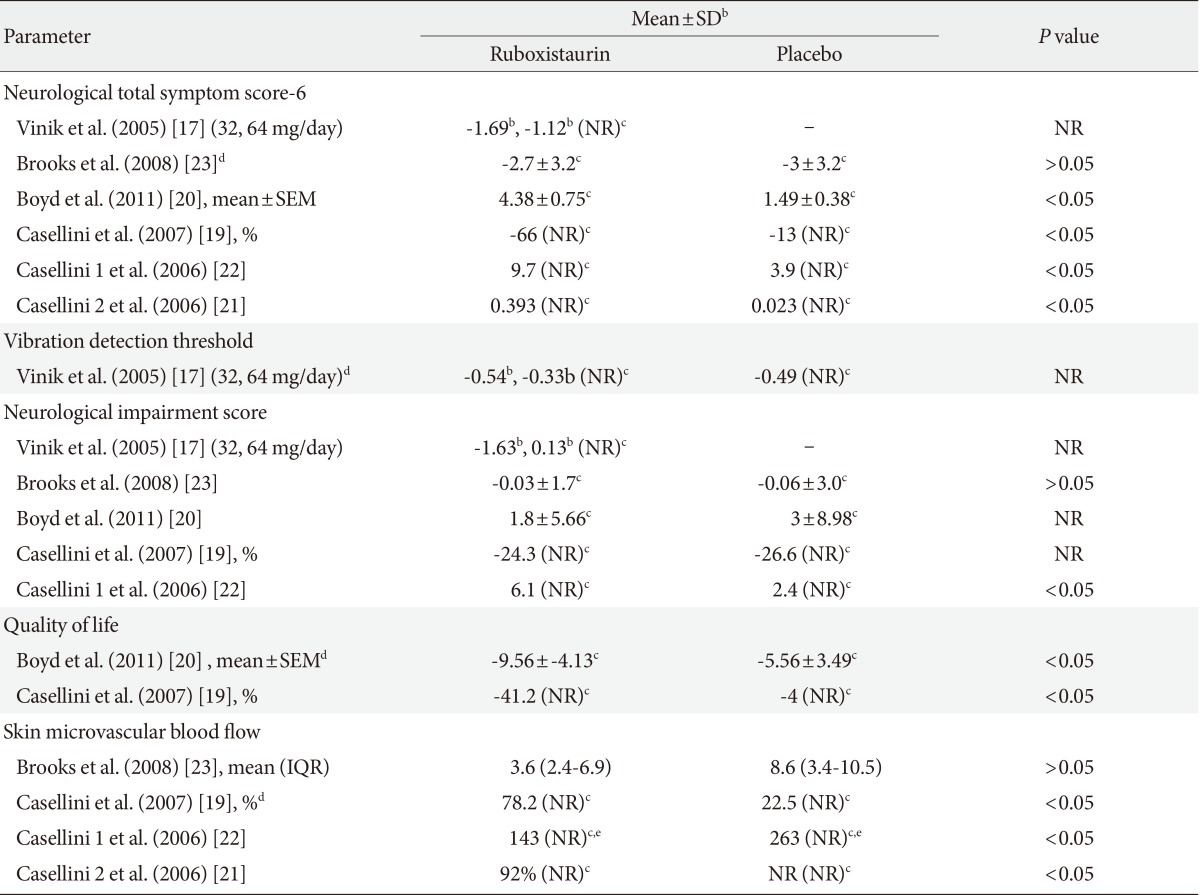
- Most studies presented outcome data numerically in tables. Graphical presentation was also seen in some cases. The comparisons were done between RBX and placebo in all the studies. None of study compared RBX with active comparator (Table 3).
- Change in NTSS-6 was assessed in all included studies. Change in VDT was the outcome measure seen in one study by Vinik et al. only [17].
- Neurological total symptom score
- Change in NTSS-6 was assessed in 353 participants. Decrease in NTSS score indicates improvement. Significant decrease in NTSS score was found in RBX treated group as compared to placebo in studies three studies by Casellini et al. [19] (P<0.037), Boyd et al. [20] (P<0.001), Casellini et al. [22] (P<0.04), and Casellini et al. [21] (P<0.0006) where total of 64 participants received RBX.
- No significant difference was observed in two studies conducted by Brooks et al. [23] and Vinik et al. [17]. But in Vinik et al. [17] study, a subgroup of patients with clinically significant symptoms (defined as NTSS-6 score >6) at baseline (n=83), significant change in NTSS was observed at 12 months of follow-up in RBX 64 mg/day treated patients (n=71) (P=0.015) but not in RBX 32 mg/day group (n=66) as compared to placebo group. Similarly, in a subgroup of patients with clinically significant symptoms and less severe DPN (n=50) (defined as sural nerve action potential ≥0.5 µv and NTSS-6 rating >6) there was a statistically significant reduction in NTSS-6 total score with RBX 64 mg/day (P=0.006).
- Vibration detection threshold
- Change in VDT was assessed in only one study by Vinik et al. [17] study. Decrease in VDT units represents improvement. No significant improvement (P=not reported) was observed in VDT in both RBX treated groups (32, 64 mg/day) as compared to placebo in total of 205 patients. Decrease in VDT units was observed in a subgroup of patients with clinically significant symptoms (NTSS-6 score >6). Significant decrease in VDT units was also observed in a subgroup of patients with clinically significant symptoms and less severe DPN (n=50), for RBX 32 mg/day (P=0.012) and 64 mg/day (P=0.026) as compared with placebo group.
- Secondary outcome measure
- Change in SkBF (endothelium dependent) was assessed in four studies [19,21-23]. Increase in SkBF represents improvement. In three studies with total of 44 RBX treated subjects, significant increase in SkBF from baseline was observed in RBX treated group as compared to placebo (P<0.03, P<0.013, and P<0.002 respectively). In Brooks et al. [23] study, no significant (P=0.233) improvement in SkBF was found in RBX treated group (n=9) as compared to placebo group (n=9).
- Change in total QoL (by Norfolk QoL-DN) was assessed in two studies recruiting a total of 80 participants. Increase in score indicates improvement. In Boyd et al. [20] study, significant improvement was observed in two aspects of QoL including total QoL score (P<0.04) and symptom subscore (P<0.004) in RBX group (n=20) as compared to placebo group (n=20). In Casellini et al. [19] study, significant improvement in symptom subscore was observed in RBX treated subjects as compared to placebo treated subjects (P=0.041). Significant improvement from baseline was observed in RBX group (P=0.01) but not in patients under placebo group. Similarly significant improvement of total QoL score was also observed in RBX treated group (P=0.04) at 6 months as compared to placebo. No significant difference for other aspects of QoL reported in either study.
- Change in NIS was assessed in five studies in 242 participants (RBX treated group only) [17,19,20,22,23]. Decrease in NIS score indicates improvement. Significant decrease in NIS score was observed in RBX group as compared to placebo group in study by Casellini et al. [22] where data from 10 participants was used (P<0.01). No significant decrease in NIS score was observed in the remaining studies in RBX group as compared to placebo group.
- Safety profile
- According to European Medicine Agency (EMA) report, common observed adverse effects (AEs) with the use of RBX in diabetic retinopathy are QT prolongation, creatinine phospokinase elevation. Safety was assessed in only two studies. In Casellini et al. [19] study 35 patients experienced treatment emergent adverse events (TEAE). No AE were considered to be study drug related. Four serious AEs were also reported in the same study in RBX group: bacterial pneumonia, myocardial ischemia, coronary artery disease with stent placement, and death resulting from acute myocardial infarction. None of serious AEs were considered to be study drug related except for myocardial ischemia, for which causal relationship could not be ruled out. In Vinik et al. [17] study, 161 patients experienced TEAE but none were found to be relevant. In this study 26 patients reported serious AEs (placebo-12, RBX 32 mg/day-9, RBX 64 mg/day-5). No documentation regarding AE was found in other four studies.
- Tolerability
- Two studies documented the number and reasons of withdrawals. In Vinik et al. [17] study (n=205), 32 (15.6%) discontinued treatment. In this, AEs caused withdrawal in nine patients (RBX 32 mg/day, one; RBX 64 mg/day, four; placebo, four), lost to follow-up caused withdrawal in eight patients (RBX 32 mg/day, three; RBX 64 mg/day, one; placebo, four), withdrawal by patient decision in 11 patients (RBX 32 mg/day, three; RBX 64 mg/day, five; placebo, three) and withdrawal by physician or sponsor decision in four patients (RBX 32 mg/day, three; RBX 64 mg/day, one). Casellini et al. [19] study reported no patient withdrawal. While in remaining studies patient withdrawal data was not reported.
RESULTS
Interventions
Study design
Participants
Risk of bias
Effect of interventions
Primary outcome measure
Skin microvascular blood flow
Total quality of life
Neurological impairment score
- DPN has been found to be a common long term microvascular complication in patients with diabetes mellitus. It is well known that hyperglycaemia leads to elevated levels of DAG, which is a potent activator of PKC. It also results in the deregulation of several cellular processes in which PKC isoenzymes are involved, including those which lead to inhibition of Na-K ATPase, increasing permeability and stimulation of proliferation in different cell types. RBX is a specific inhibitor of PKC-β enzyme which plays important role in pathogenesis of endothelial damage associated with diabetic microvascular complications [25-28].
- RBX showed significant results in animal studies for indications such as neuropathy, retinopathy, and nephropathy associated with diabetes. Several drugs with wide array of mechanisms are under clinical investigation, such as fidarestat [8] and AS-3201 [29] (both increases polyol pathway), α-lipoic acid [8], phVEGF 165 gene transfer [8], and C-peptide [8].
- New drug application for marketing authorization was filed by Eli Lilly for RBX (Arxxant) on February 2006 to U.S. Food and Drug Administration (USFDA) and on 30 May 2006 to the EMA for diabetic retinopathy. Approvable letter issued from USFDA, with a request for an additional clinical trial. Eli Lilly withdrew its marketing application for RBX for diabetic retinopathy due to non provision of the additional required data within the allowed timeframe [30]. Three clinical trials of RBX have been published since 2006. At present, no clinical trial is being registered within USFDA, EMA, and Canada. Only one clinical trial is found to be ongoing in Japan registry while no other trial is registered in other registries. There is no other molecule in PKC-β inhibitor category which could explored to be used in diabetic microvascular complications.
- Improvement of sensory symptoms and nerve function are considered to be important end points. DPN is primarily a sensory disorder and measurement of sensory symptoms and nerve function must be an important outcome of therapeutic trials.
- In our systematic review we observed various parameters for the assessment of DPN. NTSS-6 was assessed in all included studies out of which four observed significant decrease in NTSS-6 score in RBX group while two studies [17,23] did not observe significant fall in NTSS-6. Also, no significant increase in VDT was observed [17]. This may be due to relatively short period of follow-up (12 months), since progression of DPN is slow and might require up to 3 years of follow-up to demonstrate clinically significant difference [31]. However, patients with less severe DPN were found to be more responsive to RBX. Measurements of SkBF showed significant improvement with RBX in three studies [19,21,22]. Significant improvement in QoL was also observed in two studies [19,20].
- Safety assessment was not done in majority of the studies except for two where none of the AE was related to RBX except for one case of myocardial ischemia in Casellini et al. [19] study. The safety profile was consistent with that reported in previous safety profile evaluations of RBX in healthy volunteers or patients with DM.
- Some limitations of our review process must be noted. It was difficult to clarify details of study methodology of included studies. The total number of subjects in the included six studies is too small to come to firm conclusion. We could not receive any information regarding the two registered large clinical trials (n=200 each) of RBX in DPN. A key limitation and challenge in synthesizing and interpreting this body of evidence is the issue of heterogeneous patient populations across and within studies. There are important issues of methodological quality involving most of these studies; in a substantial number we had incomplete information about concealment of treatment allocation and methods of randomization and blinding. Moreover, most of the studies included in this systematic review lacked proper reporting the statistical values which precluded the quantitative pooling of the results by doing meta-analysis.
- The current development status of RBX in DPN is not clear. If any further clinical trials of PKC-β inhibitor are undertaken, we feel it is essential that it should be of at least 1 year duration with the use of clear methods of randomization, allocation concealment, and blinding and having good follow-up of subjects. Also results should be reported properly with all statistical values.
- In conclusion, implications for practice: RBX had effects on DPN in some studies which the evidence is not enough for firm conclusion. Implications for research: further research with PKC inhibitors should only involve compounds with substantial biological or preclinical advantages over RBX. Any future trials should last at least 1 year, use rigorous methodology, and employ clinically relevant outcome measures.
DISCUSSION
- 1. Cabezas-Cerrato J. Neuropathy Spanish Study Group of the Spanish Diabetes Society (SDS). The prevalence of clinical diabetic polyneuropathy in Spain: a study in primary care and hospital clinic groups. Diabetologia 1998;41:1263-1269. ArticlePubMedPDF
- 2. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM, O'Brien PC, Melton LJ 3rd, Service FJ. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993;43:817-824. ArticlePubMed
- 3. Kumar S, Ashe HA, Parnell LN, Fernando DJ, Tsigos C, Young RJ, Ward JD, Boulton AJ. The prevalence of foot ulceration and its correlates in type 2 diabetic patients: a population-based study. Diabet Med 1994;11:480-484. ArticlePubMed
- 4. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia 1993;36:150-154. ArticlePubMedPDF
- 5. Boulton AJ, Gries FA, Jervell JA. Guidelines for the diagnosis and outpatient management of diabetic peripheral neuropathy. Diabet Med 1998;15:508-514. ArticlePubMed
- 6. Harris M, Eastman R, Cowie C. Symptoms of sensory neuropathy in adults with NIDDM in the U.S. population. Diabetes Care 1993;16:1446-1452. ArticlePubMedPDF
- 7. Edwards JL, Vincent AM, Cheng HT, Feldman EL. Diabetic neuropathy: mechanisms to management. Pharmacol Ther 2008;120:1-34. ArticlePubMedPMC
- 8. Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA, Maser RE, Sosenko JM, Ziegler D. American Diabetes Association. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care 2005;28:956-962. PubMed
- 9. Masson EA, Boulton AJ. Aldose reductase inhibitors in the treatment of diabetic neuropathy: a review of the rationale and clinical evidence. Drugs 1990;39:190-202. ArticlePubMed
- 10. Veves A, King GL. Can VEGF reverse diabetic neuropathy in human subjects? J Clin Invest 2001;107:1215-1218. ArticlePubMedPMC
- 11. Chalk C, Benstead TJ, Moore F. Aldose reductase inhibitors for the treatment of diabetic polyneuropathy. Cochrane Database Syst Rev 2007;(4):CD004572ArticlePubMedPMC
- 12. Ramirez MA, Borja NL. Epalrestat: an aldose reductase inhibitor for the treatment of diabetic neuropathy. Pharmacotherapy 2008;28:646-655. ArticlePubMed
- 13. Ring BJ, Gillespie JS, Binkley SN, Campanale KM, Wrighton SA. The interactions of a selective protein kinase C beta inhibitor with the human cytochromes P450. Drug Metab Dispos 2002;30:957-961. ArticlePubMed
- 14. Burkey JL, Campanale KM, Barbuch R, O'Bannon D, Rash J, Benson C, Small D. Disposition of [14C]ruboxistaurin in humans. Drug Metab Dispos 2006;34:1909-1917. ArticlePubMed
- 15. Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, Kojima Y, Furuyoshi N, Shichiri M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract 1995;28:103-117. ArticlePubMed
- 16. Bastyr EJ 3rd, Price KL, Bril V. MBBQ Study Group. Development and validity testing of the neuropathy total symptom score-6: questionnaire for the study of sensory symptoms of diabetic peripheral neuropathy. Clin Ther 2005;27:1278-1294. ArticlePubMed
- 17. Vinik AI, Bril V, Kempler P, Litchy WJ, Tesfaye S, Price KL, Bastyr EJ 3rd. MBBQ Study Group. Treatment of symptomatic diabetic peripheral neuropathy with the protein kinase C beta-inhibitor ruboxistaurin mesylate during a 1-year, randomized, placebo-controlled, double-blind clinical trial. Clin Ther 2005;27:1164-1180. PubMed
- 18. Bril V. NIS-LL: the primary measurement scale for clinical trial endpoints in diabetic peripheral neuropathy. Eur Neurol 1999;41(Suppl 1):8-13. ArticlePubMedPDF
- 19. Casellini CM, Barlow PM, Rice AL, Casey M, Simmons K, Pittenger G, Bastyr EJ 3rd, Wolka AM, Vinik AI. A 6-month, randomized, double-masked, placebo-controlled study evaluating the effects of the protein kinase C-beta inhibitor ruboxistaurin on skin microvascular blood flow and other measures of diabetic peripheral neuropathy. Diabetes Care 2007;30:896-902. PubMed
- 20. Boyd A, Casselini C, Vinik E, Vinik A. Quality of life and objective measures of diabetic neuropathy in a prospective placebo-controlled trial of ruboxistaurin and topiramate. J Diabetes Sci Technol 2011;5:714-722. ArticlePubMedPMCPDF
- 21. Casellini CM, Barlow PM, Rice AL, Casey ME, Simmons K, Pittenger G, Bastyr E, Vinik A. Effect of ruboxistaurin (RBX) on quantitative measures of diabetic peripheral neuropathy (DPN) In: 66th Scientific Session 2006; June 9-13; Washington, DC. Alexandria: American Diabetes Association; 2006.
- 22. Casellini CM, Barlow PM, Rice AL, Vinik AA. Effect of ruboxistaurin (RBX) on skin microvascular blood flow (SBF), sensory symptoms, and sensory perception in patients with diabetic peripheral neuropathy (DPN) In: 66th Scientific Session 2006; June 9-13; Washington, DC. Alexandria: American Diabetes Association; 2006.
- 23. Brooks B, Delaney-Robinson C, Molyneaux L, Yue DK. Endothelial and neural regulation of skin microvascular blood flow in patients with diabetic peripheral neuropathy: effect of treatment with the isoform-specific protein kinase C beta inhibitor, ruboxistaurin. J Diabetes Complications 2008;22:88-95. PubMed
- 24. Tesfaye S, Tandan R, Bastyr EJ 3rd, Kles KA, Skljarevski V, Price KL. Ruboxistaurin Study Group. Factors that impact symptomatic diabetic peripheral neuropathy in placebo-administered patients from two 1-year clinical trials. Diabetes Care 2007;30:2626-2632. ArticlePubMedPDF
- 25. Craven PA, Davidson CM, DeRubertis FR. Increase in diacylglycerol mass in isolated glomeruli by glucose from de novo synthesis of glycerolipids. Diabetes 1990;39:667-674. ArticlePubMed
- 26. Hempel A, Maasch C, Heintze U, Lindschau C, Dietz R, Luft FC, Haller H. High glucose concentrations increase endothelial cell permeability via activation of protein kinase C alpha. Circ Res 1997;81:363-371. PubMed
- 27. Kishimoto A, Takai Y, Mori T, Kikkawa U, Nishizuka Y. Activation of calcium and phospholipid-dependent protein kinase by diacylglycerol, its possible relation to phosphatidylinositol turnover. J Biol Chem 1980;255:2273-2276. ArticlePubMed
- 28. Xia P, Inoguchi T, Kern TS, Engerman RL, Oates PJ, King GL. Characterization of the mechanism for the chronic activation of diacylglycerol-protein kinase C pathway in diabetes and hypergalactosemia. Diabetes 1994;43:1122-1129. ArticlePubMedPDF
- 29. Oates PJ. Aldose reductase, still a compelling target for diabetic neuropathy. Curr Drug Targets 2008;9:14-36. ArticlePubMed
- 30. European Medicines Agency: Withdrawal assessment report for arxxant: Ruboxistaurin (as mesilate monohydrate) updated 2007 May 24. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Application_withdrawal_assessment_report/2010/01/WC500068826.pdf.
- 31. The DCCT Research Group. Epidemiology of severe hypoglycemia in the diabetes control and complications trial. Am J Med 1991;90:450-459. ArticlePubMed
REFERENCES

Casellini 1 and Casellini 2 are conference abstracts while Casellini is full text article.
NR, not reported; RBX, ruboxistaurin; PL, placebo; TPX, topiramate; FD, fixed dose; DPN, diabetic peripheral neuropathy; NTSS-6, neurological total symptom score (points); NIS (LL), neuropathy impairment score of lower limbs; VDT, vibration detection threshold; SNAP, sural neurological action potential (µv); SkBF, skin microvascular blood flow; QoL, quality of life; NIS, neurological impairment score (points); CGI, clinician global impression; NSS, neuropathy symptom score (points); TNS, total neurological score (points).
aSixty-six were assigned to 32 mg/day & 71 to 64 mg/day group, bTPX vs. PL and RBX vs. PL was separately compared, cFixed dose given in mg/day.
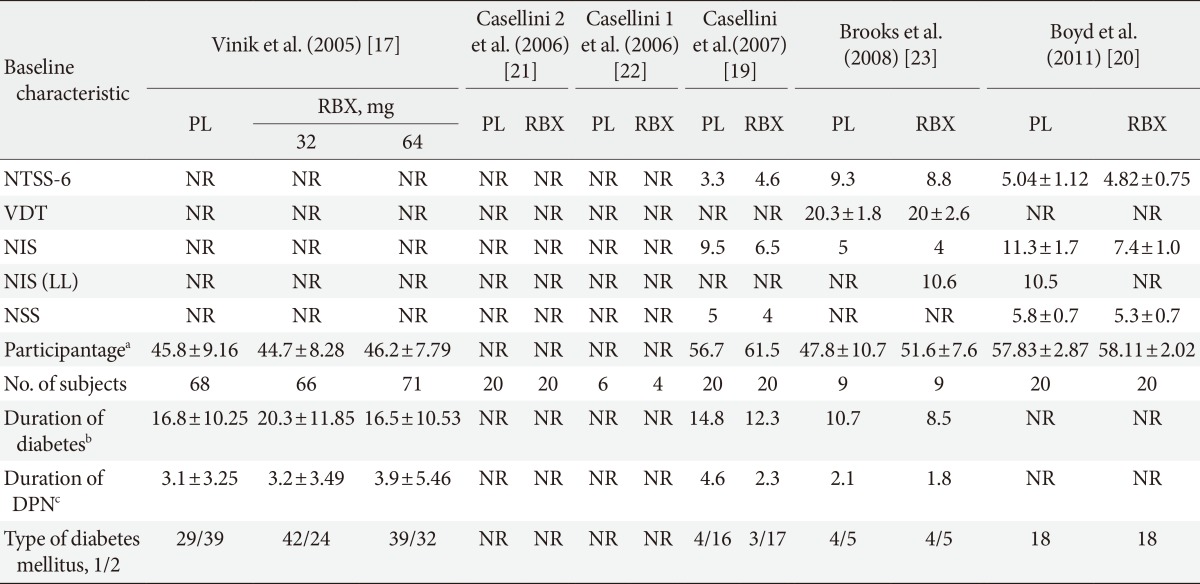
PL, placebo; RBX, ruboxistaurin; NTSS-6, neurological total symptom score (points); NR, not reported; VDT, vibration detection threshold; NIS, neurological impairment score (points); NIS (LL), neurological impairment score of lower limbs; NSS, neuropathy symptom score (points); DPN, diabetic peripheral neuropathy.
aParticipants age is expressed in years (here mean±standard deviation [SD] is mentioned), except for Boyd (mean±standard error of mean [SEM]) and Casellini (mean±interquartile range [IQR]), bDuration of diabetes is expressed in years (here mean±SD is mentioned), except for Boyd (mean±SEM), cDuration of DPN is expressed in years (here mean±SD is mentioned), except for Boyd (mean±SEM).
NR, not reported; SEM, standard error of mean; IQR, interquartile range.
aAt dose of 32 mg/day, bDifference between ruboxistaurin and placebo is mentioned, cValues mentioned are difference between baseline and posttreatment, dRefers to parameter used as a primary end point in that particular study, eValues are expressed in area under the curve×103 blood flow units measured at proximal calf.
Figure & Data
References
Citations
- Painful Diabetic Neuropathy: The Need for New Approaches
Andrea M. Yeung, Jingtong Huang, Kevin T. Nguyen, Nicole Y. Xu, Lorenzo T. Hughes, Brajesh K. Agrawal, Niels Ejskjaer, David C. Klonoff
Journal of Diabetes Science and Technology.2024; 18(1): 159. CrossRef - Cell metabolism pathways involved in the pathophysiological changes of diabetic peripheral neuropathy
Yaowei Lv, Xiangyun Yao, Xiao Li, Yuanming Ouyang, Cunyi Fan, Yun Qian
Neural Regeneration Research.2024; 19(3): 598. CrossRef - Diabetic sensory neuropathy and insulin resistance are induced by loss of UCHL1 in Drosophila
Daewon Lee, Eunju Yoon, Su Jin Ham, Kunwoo Lee, Hansaem Jang, Daihn Woo, Da Hyun Lee, Sehyeon Kim, Sekyu Choi, Jongkyeong Chung
Nature Communications.2024;[Epub] CrossRef - Non-Muscle Myosin IIC as a Prognostic and Therapeutic Target in Cancer
Ghulam Jilany Khan, Sajal Salman, Zhu Chen, Song Li, Hui Chen, Yan Deng, Nongyue He
Journal of Biomedical Nanotechnology.2024; 20(3): 438. CrossRef - New Horizons in Diabetic Neuropathies: An Updated Review on their
Pathology, Diagnosis, Mechanism, Screening Techniques, Pharmacological,
and Future Approaches
Namra Aziz, Biswajit Dash, Pranay Wal, Prachi Kumari, Poonam Joshi, Ankita wal
Current Diabetes Reviews.2024;[Epub] CrossRef - Nanoformulations of flavonoids for diabetes and microvascular diabetic complications
Kopal Agarawal, Yogesh Anant Kulkarni, Sarika Wairkar
Drug Delivery and Translational Research.2023; 13(1): 18. CrossRef - Determination of Ruboxistaurin analysis in rat plasma utilizing LC–MS/MS technique
Bushra T. AlQuadeib, Fadilah S. Aleanizy, Fulwah Y. Alqahtani, Rehab A. Alshammari, Amal Aldarwesh, Ibrahim Alsarra
Saudi Pharmaceutical Journal.2023; 31(4): 547. CrossRef - New perspectives in diabetic neuropathy
Stephanie A. Eid, Amy E. Rumora, Bogdan Beirowski, David L. Bennett, Junguk Hur, Masha G. Savelieff, Eva L. Feldman
Neuron.2023; 111(17): 2623. CrossRef - Issues and challenges in diabetic neuropathy management: A narrative review
Che Aishah Nazariah Ismail
World Journal of Diabetes.2023; 14(6): 741. CrossRef - Plasma Metabolomics and Lipidomics Differentiate Obese Individuals by Peripheral Neuropathy Status
Kai Guo, Masha G Savelieff, Amy E Rumora, Fadhl M Alakwaa, Brian C Callaghan, Junguk Hur, Eva L Feldman
The Journal of Clinical Endocrinology & Metabolism.2022; 107(4): 1091. CrossRef - The crosstalk among TLR2, TLR4 and pathogenic pathways; a treasure trove for treatment of diabetic neuropathy
Seyed Hossein Aghamiri, Khalil Komlakh, Mehran Ghaffari
Inflammopharmacology.2022; 30(1): 51. CrossRef - 10.6-μm infrared laser as adjuvant therapy for diabetic peripheral neuropathy: study protocol for a double-blind, randomized controlled trial
Lin Lin, Yi Chen, Yuxia Li, Ke Cheng, Haiping Deng, Jianping Lu, Ling Zhao, Xueyong Shen
Trials.2022;[Epub] CrossRef - Is Nerve Electrophysiology a Robust Primary Endpoint in Clinical Trials of Treatments for Diabetic Peripheral Neuropathy?
Dalal Y. Al-Bazz, Andrew J. Nelson, Jamie Burgess, Ioannis N. Petropoulos, Jael Nizza, Anne Marshall, Emily Brown, Daniel J. Cuthbertson, Andrew G. Marshall, Rayaz A. Malik, Uazman Alam
Diagnostics.2022; 12(3): 731. CrossRef - Prospective dietary radical scavengers: Boon in Pharmacokinetics, overcome insulin obstruction via signaling cascade for absorption during impediments in metabolic disorder like Diabetic Mellitus
Varuna Suresh, John Kunnath, Amala Reddy
Journal of Diabetes & Metabolic Disorders.2022; 21(1): 1149. CrossRef - The Treatment of Painful Diabetic Neuropathy
Gordon Sloan, Uazman Alam, Dinesh Selvarajah, Solomon Tesfaye
Current Diabetes Reviews.2022;[Epub] CrossRef - Effect of Cognitive-Behavioral Therapy or Mindfulness Therapy on Pain and Quality of Life in Patients with Diabetic Neuropathy: A Systematic Review and Meta-Analysis
Yuan Bai, Jun-Hong Ma, Ying Yu, Zhi-Wen Wang
Pain Management Nursing.2022; 23(6): 861. CrossRef - Emerging drugs for the treatment of diabetic nephropathy
Yoon Kook Kim, Xinyuan Ning, Kashif M. Munir, Stephen N. Davis
Expert Opinion on Emerging Drugs.2022; 27(4): 417. CrossRef - Novel treatment modalities for painful diabetic neuropathy
A. Rastogi, E.B. Jude
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2021; 15(1): 287. CrossRef - Effectiveness and safety of low-level laser therapy in diabetic peripheral neuropathy: a protocol for a systematic review and meta-analysis
Lin Lin, Jingjing Li, Jingshan Lin, Shiheng Tang, Yuxia Li
Systematic Reviews.2021;[Epub] CrossRef - Plasma lipid metabolites associate with diabetic polyneuropathy in a cohort with type 2 diabetes
Amy E. Rumora, Kai Guo, Fadhl M. Alakwaa, Signe T. Andersen, Evan L. Reynolds, Marit E. Jørgensen, Daniel R. Witte, Hatice Tankisi, Morten Charles, Masha G. Savelieff, Brian C. Callaghan, Troels S. Jensen, Eva L. Feldman
Annals of Clinical and Translational Neurology.2021; 8(6): 1292. CrossRef - Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy
Gordon Sloan, Dinesh Selvarajah, Solomon Tesfaye
Nature Reviews Endocrinology.2021; 17(7): 400. CrossRef - Diabetic neuropathy: an insight on the transition from synthetic drugs to herbal therapies
Komal Arora, Pushpa C. Tomar, Vandana Mohan
Journal of Diabetes & Metabolic Disorders.2021; 20(2): 1773. CrossRef - Synthesis and Antiplasmodial Activity of Bisindolylcyclobutenediones
Duc Hoàng Lande, Abed Nasereddin, Arne Alder, Tim W. Gilberger, Ron Dzikowski, Johann Grünefeld, Conrad Kunick
Molecules.2021; 26(16): 4739. CrossRef - High-content image-based analysis and proteomic profiling identifies Tau phosphorylation inhibitors in a human iPSC-derived glutamatergic neuronal model of tauopathy
Chialin Cheng, Surya A. Reis, Emily T. Adams, Daniel M. Fass, Steven P. Angus, Timothy J. Stuhlmiller, Jared Richardson, Hailey Olafson, Eric T. Wang, Debasis Patnaik, Roberta L. Beauchamp, Danielle A. Feldman, M. Catarina Silva, Mriganka Sur, Gary L. Joh
Scientific Reports.2021;[Epub] CrossRef - Management of diabetic neuropathy
Simona Cernea, Itamar Raz
Metabolism.2021; 123: 154867. CrossRef - 29th Annual GP2A Medicinal Chemistry Conference
Jean-Jacques Helesbeux, Laura Carro, Florence O. McCarthy, Vânia M. Moreira, Francesca Giuntini, Niamh O’Boyle, Susan E. Matthews, Gülşah Bayraktar, Samuel Bertrand, Christophe Rochais, Pascal Marchand
Pharmaceuticals.2021; 14(12): 1278. CrossRef - Understanding Diabetic Neuropathy: Focus on Oxidative Stress
Lei Pang, Xin Lian, Huanqiu Liu, Yuan Zhang, Qian Li, Yin Cai, Haichun Ma, Xin Yu
Oxidative Medicine and Cellular Longevity.2020; 2020: 1. CrossRef - Treatment of Diabetic Cardiovascular Autonomic, Peripheral and Painful Neuropathy. Focus on the Treatment of Cardiovascular Autonomic Neuropathy with ACE Inhibitors
Triantafyllos Didangelos, Aristidis Veves
Current Vascular Pharmacology.2020; 18(2): 158. CrossRef - Mechanisms of small nerve fiber pathology
Franziska Gross, Nurcan Üçeyler
Neuroscience Letters.2020; 737: 135316. CrossRef - Whole-Genome Sequencing of Finnish Type 1 Diabetic Siblings Discordant for Kidney Disease Reveals DNA Variants associated with Diabetic Nephropathy
Jing Guo, Owen J. L. Rackham, Niina Sandholm, Bing He, Anne-May Österholm, Erkka Valo, Valma Harjutsalo, Carol Forsblom, Iiro Toppila, Maija Parkkonen, Qibin Li, Wenjuan Zhu, Nathan Harmston, Sonia Chothani, Miina K. Öhman, Eudora Eng, Yang Sun, Enrico Pe
Journal of the American Society of Nephrology.2020; 31(2): 309. CrossRef - SP6616 as a Kv2.1 inhibitor efficiently ameliorates peripheral neuropathy in diabetic mice
Xialin Zhu, Yun Chen, Xu Xu, Xiaoju Xu, Yin Lu, Xi Huang, Jinpei Zhou, Lihong Hu, Jiaying Wang, Xu Shen
EBioMedicine.2020; 61: 103061. CrossRef - Targeting Mitochondrial Fission-Fusion Imbalance in Heart Failure
Thiago N. Menezes, Lisley S. Ramalho, Luiz R. G. Bechara, Julio Cesar Batista Ferreira
Current Tissue Microenvironment Reports.2020; 1(4): 239. CrossRef - Recent advances in the pathogenesis of microvascular complications in diabetes
Sungmi Park, Hyeon-Ji Kang, Jae-Han Jeon, Min-Ji Kim, In-Kyu Lee
Archives of Pharmacal Research.2019; 42(3): 252. CrossRef - Novel Target Sites for Drug Screening: A Special Reference to Cancer, Rheumatoid Arthritis and Parkinson’s Disease
Neeraj Kumar, Anita Singh, Dinesh Kumar Sharma, Kamal Kishore
Current Signal Transduction Therapy.2019; 14(2): 107. CrossRef - Molecular mechanism of diabetic neuropathy and its pharmacotherapeutic targets
Saikat Dewanjee, Sonjit Das, Anup Kumar Das, Niloy Bhattacharjee, Anjum Dihingia, Tarun K. Dua, Jatin Kalita, Prasenjit Manna
European Journal of Pharmacology.2018; 833: 472. CrossRef - Interventions for Neuropathic Pain: An Overview of Systematic Reviews
Svjetlana Dosenovic, Antonia Jelicic Kadic, Maja Miljanovic, Marina Biocic, Krste Boric, Marija Cavar, Nikolina Markovina, Katarina Vucic, Livia Puljak
Anesthesia & Analgesia.2017; 125(2): 643. CrossRef - New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain
Eva L. Feldman, Klaus-Armin Nave, Troels S. Jensen, David L.H. Bennett
Neuron.2017; 93(6): 1296. CrossRef - Rutin suppresses high glucose-induced ACTA2 and p38 protein expression in diabetic nephropathy
Chun-Shan Han, Kai Liu, Ning Zhang, Shi-Wen Li, Hai-Cheng Gao
Experimental and Therapeutic Medicine.2017; 14(1): 181. CrossRef - Protein kinase C participation in the mechanisms of vascular tone disturbance upon diabetes mellitus. Part 4
I. Kizub, O. Kharchenko, O. Kostiuk, L. Ostapchenko, K. Klymenko, A. Soloviev
Bulletin of Taras Shevchenko National University of Kyiv. Series: Problems of Physiological Functions Regulation.2016; 21(2): 61. CrossRef - Emerging drugs for diabetic peripheral neuropathy and neuropathic pain
Nikolaos Papanas, Dan Ziegler
Expert Opinion on Emerging Drugs.2016; 21(4): 393. CrossRef - Pancreatic β Cell Mass Death
Husnia I. Marrif, Salma I. Al-Sunousi
Frontiers in Pharmacology.2016;[Epub] CrossRef - Efficacy and safety of prostaglandin E1 plus lipoic acid combination therapy versus monotherapy for patients with diabetic peripheral neuropathy
De-Qi Jiang, Ming-Xing Li, Yan-Jiao Ma, Yan Wang, Yong Wang
Journal of Clinical Neuroscience.2016; 27: 8. CrossRef - Nonbiological pharmacotherapies for the treatment of diabetic macular edema
Aniruddha Agarwal, Jacob Parriott, Sibel Demirel, Colby Argo, Yasir Jamal Sepah, Diana V Do, Quan Dong Nguyen
Expert Opinion on Pharmacotherapy.2015; 16(17): 2625. CrossRef - Present and Future in the Treatment of Diabetic Kidney Disease
Borja Quiroga, David Arroyo, Gabriel de Arriba
Journal of Diabetes Research.2015; 2015: 1. CrossRef - Choosing drugs for the treatment of diabetic neuropathy
Majed Alabdali, Mohammad Qrimli, Carolina Barnett, Alon Abraham, Ari Breiner, Hans D Katzberg, Danah Aljaafari, Hana Albulaihe, Bruce A Perkins, Vera Bril
Expert Opinion on Pharmacotherapy.2015; 16(12): 1805. CrossRef - Burning through the pain: treatments for diabetic neuropathy
S. Javed, U. Alam, R. A. Malik
Diabetes, Obesity and Metabolism.2015; 17(12): 1115. CrossRef - Protein Kinase C-Independent Inhibition of Organic Cation Transporter 1 Activity by the Bisindolylmaleimide Ro 31-8220
Abdullah Mayati, Arnaud Bruyere, Amélie Moreau, Elodie Jouan, Claire Denizot, Yannick Parmentier, Olivier Fardel, Jeff M Sands
PLOS ONE.2015; 10(12): e0144667. CrossRef - Targeting caveolin-3 for the treatment of diabetic cardiomyopathy
Lucy Murfitt, Gareth Whiteley, Mohammad M. Iqbal, Ashraf Kitmitto
Pharmacology & Therapeutics.2015; 151: 50. CrossRef - Protein kinase C in enhanced vascular tone in diabetes mellitus
Igor V. Kizub, Kateryna I. Klymenko, Anatoly I. Soloviev
International Journal of Cardiology.2014; 174(2): 230. CrossRef - Meta-analysis of methylcobalamin alone and in combination with prostaglandin E1 in the treatment of diabetic peripheral neuropathy
Houliang Deng, JinJin Yin, JingJing Zhang, Qian Xu, Xiaoxia Liu, Li Liu, Zhuomin Wu, Aimin Ji
Endocrine.2014; 46(3): 445. CrossRef - Efficacy of α-lipoic acid in diabetic neuropathy
Nikolaos Papanas, Dan Ziegler
Expert Opinion on Pharmacotherapy.2014; 15(18): 2721. CrossRef
 PubReader
PubReader Cite
Cite