
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 41(6); 2017 > Article
-
Original ArticleObesity and Metabolic Syndrome Prediction of Gestational Diabetes Mellitus in Pregnant Korean Women Based on Abdominal Subcutaneous Fat Thickness as Measured by Ultrasonography
-
Sung Hee Yang1, Changsoo Kim2, Hyun Sook An1, Hyun An3, Jin Soo Lee4

-
Diabetes & Metabolism Journal 2017;41(6):486-491.
DOI: https://doi.org/10.4093/dmj.2017.41.6.486
Published online: September 22, 2017
1Department of Obstetrics and Gynecology, Ilsin Christian Hospital, Busan, Korea.
2Department of Radiological Science, College of Health Sciences, Catholic University of Pusan, Busan, Korea.
3Department of Radiology, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
4Department of Radiology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- Corresponding author: Jin Soo Lee. Department of Radiology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, 875 Haeun-daero, Haeundae-gu, Busan 48108, Korea. 033941@paik.ac.kr
Copyright © 2017 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study was performed to verify the correlation between abdominal subcutaneous fat thickness (ASFT) measured by ultrasonography (US) during the first trimester of pregnancy and gestational diabetes mellitus (GDM) of the second trimester in Korean women and to establish a standard of ASFT for predicting GDM.
-
Methods
- A total of 333 singleton pregnant women participated in this study. Their ASFT was measured by US during the 10+6 to 13+6 weeks of pregnancy; then a GDM confirmatory test (100 g oral glucose tolerance test) was conducted during the 24 to 28 week period of pregnancy. Based on the GDM tests, comparative analyses of the ages of the subjects, pre-pregnancy body mass index (BMI), and weight gain during pregnancy were conducted.
-
Results
- The ages of the subjects and weight gains during pregnancy were not correlated to the GDM of the second trimester of pregnancy, but the pre-pregnancy BMIs (22±3.3 kg/m2) and the ASFT (1.9±0.5 cm) measurements between the control group and subjects during the first trimester of pregnancy were found to show significant differences (P<0.001). The cut-off value of the ASFT for predicting GDM was determined to be 2.4 cm (area under the curve=0.90, sensitivity 75.61%, specificity 91.78%, P<0.001). The odds ratio was 2.91 (95% confidence interval, 1.07 to 7.92; P=0.034), which was higher than the 2.4 cm ASFT.
-
Conclusion
- It was determined that ASFT as measured by US during the first trimester of pregnancy can be used to predict the risk of developing GDM during the second trimester of pregnancy and for prognosis.
- Gestational diabetes mellitus (GDM) can be defined as glucose intolerance either first developed or found during pregnancy regardless of the degree of symptoms. It is a type of diabetes or impaired glucose tolerance developed during pregnancy and one of the most common medical complications of pregnancy [1]. GDM develops in approximately 3% to 4% of pregnant women, and mothers with GDM have a high risk of developing diabetes after delivery as well as their children who also risk developing obesity. It has been reported that GDM increases the frequency of pre-eclampsia, eclampsia, infectious disease, and the birth rate of large for gestational age fetuses in mothers. It also increases perinatal morbidity by increasing the risk of infantile respiratory distress syndrome, metabolic disorders, and hyperbilirubinemia in fetuses [2]. For the tests to diagnose GDM as a screening test, a 50 g oral glucose tolerance test (OGTT) during the 24 to 28 weeks of pregnancy is utilized. Subjects with blood glucose levels measured 1 hour after oral ingestion of glucose of 140 mg/dL (7.8 mol/L) or more are considered positive for the screening test, and for a confirmatory test, a 100 g OGTT is conducted following 12 hours of fasting [3]. Once GDM is confirmed, depending on the level of fasting blood glucose and post-meal (2-hour) blood glucose, diet therapy and exercise or insulin therapy can be conducted. Through such therapies, GDM-related complications in both mothers and their fetuses can be reduced [4].
- The age of a mother, her pre-pregnancy body mass index (BMI), the amount of obesity, family history, and weight gain during pregnancy are GDM-related factors, but among these, obesity is the most serious risk factor [56]. Obesity is known to be highly correlated to abdominal subcutaneous fat thickness (ASFT) [7]. Although computed tomography (CT) is the most credible method for measuring ASFT, it is avoided for pregnant women due to its high cost and X-ray exposure. On the other hand, ultrasonography (US) imaging-based measurement of ASFT is very useful for pregnant subjects because the results are highly correlated to CT and there is no risk of X-ray exposure due to its relatively simple measuring process [8].
- In this study, we intended to analyze the correlation between ASFT as measured by US in pregnant subjects during the first trimester of pregnancy in order to suggest an ASFT cut-off value as a predictive factor for GDM during the second trimester of pregnancy.
INTRODUCTION
- Study design and subjects
- The subjects of this study were 333 singleton pregnant women ages 19 to 41 and in their the first trimester of pregnancy (10+6 to 13+6 weeks) who were under the prenatal care of the Obstetrics and Gynecology Clinic at Ilsin Christian Hospital in South Korea during the period of February 2015 to June 2016. For all subjects, a pre-pregnancy BMI was calculated, and the weight gain during pregnancy was obtained by subtracting the pre-pregnancy weight from the weight measured during the 24 to 28 weeks of pregnancy. The menstrual cycles of both the GDM high-risk group and a control group were shown to be regular, with the last menstrual periods being on time. Subjects having type 1 or type 2 diabetes mellitus, a history of smoking, and/or other medical conditions such as high blood pressure and metabolic syndrome were excluded from the study.
- ASFT measurement and blood testing
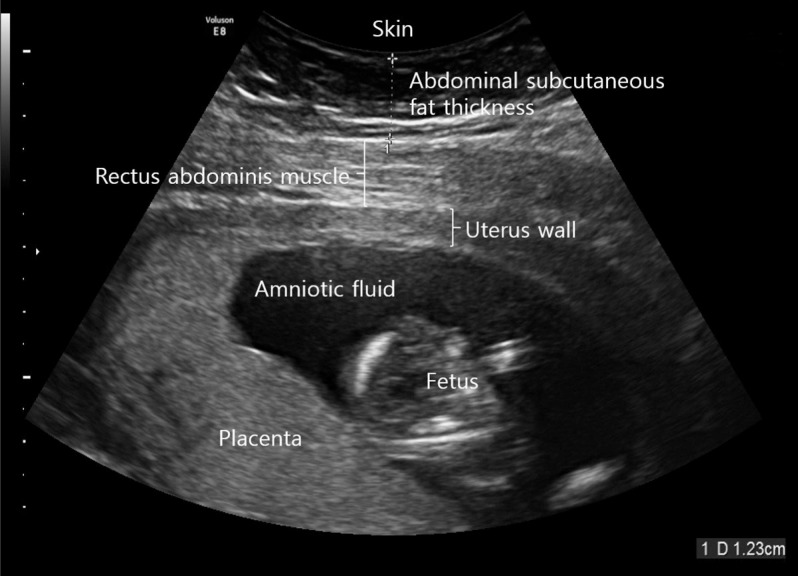
- The ultrasound device was operated by one sonographer using a high-resolution convex array probe (Voluson E8 Expert; GE Healthcare, Chicago, IL, USA) at a frequency of 2 to 8 MHz. The subjects were all placed in a comfortable supine position and then the maximum depth from the skin to the rectus abdominis muscle was measured at 1 cm above the umbilicus using a longitudinal scan [9] at the end of expiration (Fig. 1).
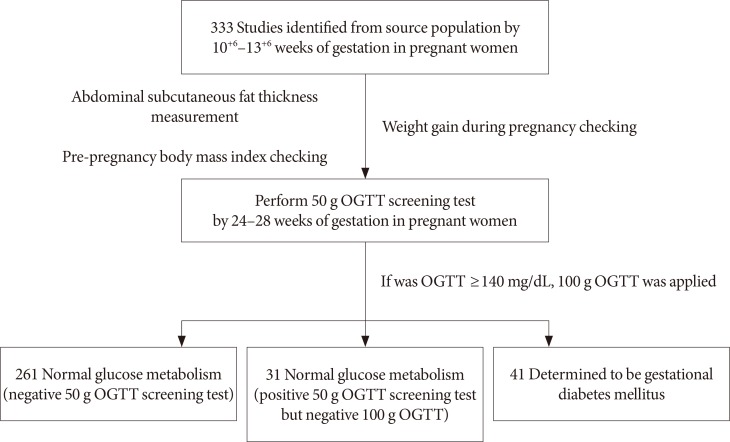
- The subjects whose ASFT were measured during their 10+6 to 13+6 weeks of pregnancy were subjected to a hexokinase glucose test taken from the veins during their 24- to 28-week period of pregnancy by taking glucose (Diasol-S Solution 50 g; Taejoon Pharm, Seoul, Korea) regardless of eating but fasting for at least 1 hour. If the result of the 50 g OGTT was 140 mg/dL or more, the subject was considered positive and an additional confirmatory OGTT was conducted using 100 g glucose. For this diagnostic test to confirm GDM, the screened positive subjects fasted for 12-hour prior to confirmatory testing with blood collected the next morning. The subjects were administered glucose (Diasol 100 g) orally and then at 1, 2, and 3 hours after taking the glucose, venous blood was collected and the glucose measured. Using the criteria of the national diabetes data group (fasting blood glucose, 105 mg/dL; 1 hour after 100 g Diasol, 190 mL/dL; 2 hours after 100 g Diasol, 165 mg/dL; 3 hours after 100 g Diasol, 145 mg/dL), if the measured values exceeded any two of those criteria, the subject was determined to be GDM (Fig. 2) [10].
- Statistical analysis
- All data were presented as a mean±standard deviation. To test the mean difference of the baseline characteristics between the GDM high-risk group and the control group, independent sample t-tests were used for both continuous variables and discrete variables, respectively. To determine the cut-off value for predicting GDM, a receiver operating characteristic (ROC) curve analysis was conducted, with the area under the curve (AUC), sensitivity, and specificity calculated. A logistic regression analysis was then conducted to calculate the odds ratio for the ASFT-mediated risk of GDM. MedCalc statistical software version 15.8 (MedCalc Software bvba, Ostend, Belgium) was used for the statistical analysis with a P value of less than 0.05 being considered statistically significant.
METHODS
- General characteristics of test subjects
- Among the 333 subjects, 261 (78%) were screened as negative and 72 (22%) were screened as positive during the GDM screening test (50 g OGTT). The number of subjects who initially screened positive but turned out to be negative as a result of the GDM confirmatory test (100 g OGTT) was 31 (9%), with 41 (12%) being determined to be GDM as they were positive for both the screening and confirmatory tests. The average age of the subjects was 32±3.9 (range, 19 to 41) and there was no significant difference among groups (P=0.210). The average pre-pregnancy BMI was 22.0±3.3 kg/m2 (range, 15.7 to 34 kg/m2). According to the Asian standard criteria [11], 37 subjects (11%) were grouped as underweight, 180 (54%) as normal, and 116 (35%) as overweight. Among the 41 subjects diagnosed as having GDM, 23 (26.9±2.6 kg/m2) were deemed overweight (BMI ≥23 kg/m2). This ratio was higher than in the underweight and normal groups (P=0.005). Weight gain during pregnancy was 4.5±2.3 kg (range, 4.5 to 12.0 kg) with no significant difference (P=0.500). ASFT was 1.9±0.5 cm (range, 0.9 to 4.1 cm) with a statistically significant difference (P<0.001) (Table 1).
- GDM and ROC curve analysis
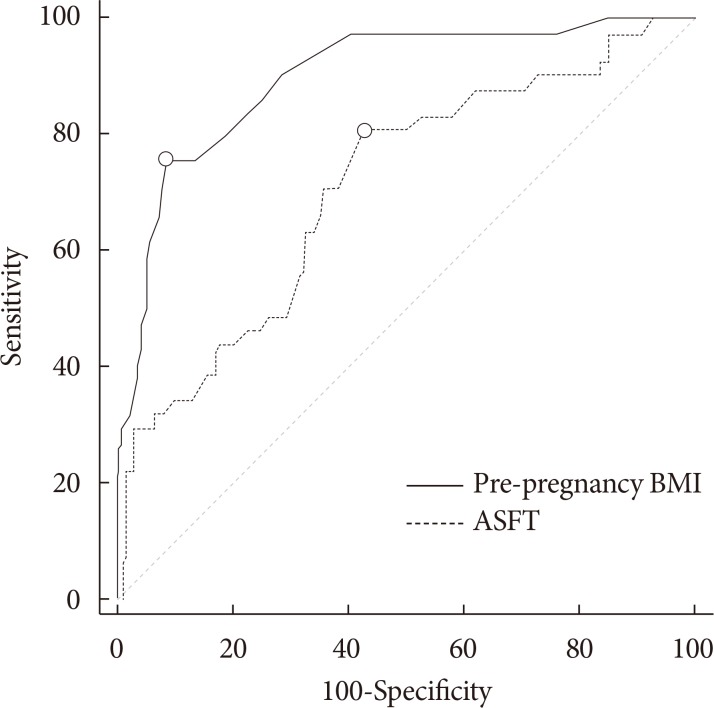
- To determine an effective cut-off value for predicting GDM, a ROC analysis was conducted using the AUC of independent variables as accuracy criteria. As a result, we determined that the sensitivity and specificity of the pre-pregnancy BMI were 80.49% and 57.19%, respectively, and determined a cut-off value of 21.8 kg/m2 (AUC=0.71) with a Youden index of 0.377. The sensitivity and specificity of the ASFT were 75.61% and 91.78%, respectively, and the cut-off value was 2.4 cm (AUC=0.90) with a Youden index of 0.674 (Table 2, Fig. 3).
- Logistic regression analysis
- An elevated ASFT was significantly associated with positive GDM. Using the 2.4 cm ASFT cut-off value, the odds ratio of GDM in 72 pregnant women who underwent the 100 g OGTT was 2.91 (95% confidence interval [CI], 1.07 to 7.92; P=0.034). Even after adjusting for the pre-pregnancy BMI, the odds ratio was 2.96 (95% CI, 0.95 to 9.24; P=0.062) (Table 3).
RESULTS
- Although the frequency of GDM varies depending on the country, ethnicity, populations screened, and diagnostic criteria, it is commonly reported as 1% to 10% and its incidence rate is generally increasing due to factors such as the increase in maternal age and obesity among mothers. This can further increase the incidence of GDM-related complications and can also cause fatal conditions to fetuses such as dyspnea at birth. For this reason there is presently a dire need to be able to predict and prevent GDM [12]. The most common method for diagnosing GDM is to conduct a 100 g OGTT for those showing blood glucose levels of 140 mg/dL or more in the 50 g OGTT conducted during the 24 to 28 weeks of pregnancy. This test is conducted at the second trimester of pregnancy, so it is difficult to detect GDM at its early stage. Because the incidence rate of obstetric complications varies depending on the time of diagnosis, early detection and active management is required to prevent GDM-related obstetric complications [13].
- This study was conducted in the hopes of finding a predictive factor relating to GDM in pregnant Korean women using as independent variables the ages of the mothers, pre-pregnancy BMI, weight gain during pregnancy, and ASFT as measured by ultrasound imaging conducted during the first trimester of pregnancy. To date, studies of the early detection of GDM have been ongoing. A large scale study indicated that pre-pregnancy BMI significantly increases along with the incidence of GDM during the second trimester of pregnancy as the age of a mother increases and when categorized based on ethnicity, the age of a mother and her BMI play more significant roles as risk factors in South Asian and black African women compared to white European or black Caribbean women [14]. Nevertheless, there was no significant correlation between the increased age of the mothers and GDM in this study (P=0.210), and for pre-pregnancy BMI, the incidence of GDM significantly increased as BMI increased from the Asian standard criterion. In particular, the impact was more significant in the overweight group (P=0.005) suggesting the importance of pre-pregnancy weight management for mothers. Further, although Choi [6] reported that the excess weight (or obesity) of a mother or excessive weight gain during pregnancy induced GDM, there was no significant correlation between the weight gain and GDM in this study (P=0.500).
- Recently, as numerous metabolic and cardiovascular diseases related to obesity have been observed, methods to accurately evaluate abdominal fat have been gaining attention. Among such methods, despite its drawback of possible measurement error due to interoperator variation, measuring abdominal fat thickness using ultrasound is actively being studied because it can easily be applied to pregnant women and its reproducibility has been reported [15]. The results of a longitudinal cohort study of 1,510 pregnant women in Australia suggested the potential of ASFT as an independent predictor of GDM [16]. The correlation between maternal obesity and GDM has already been reported, and in particular, a study was recently published that examined the relationship between central obesity and the progression of GDM during the second trimester of pregnancy [17].
- In a study of Caucasian subjects by De Souza et al. [18], the mean ASFT depth was 1.9±0.80 cm (range, 0.56 to 5.1 cm), consistent with the mean depth of 1.9±0.5 cm (range, 0.9 to 4.1 cm) in this study. However, although De Souza et al. [18] reported that ASFT was not a statistically significant predictor of GDM based on composite outcomes, this study observed a significant difference in GDM according to ASFT as indicated by the significant increase in GDM (P<0.001).
- Based on these results, the cut-off value of 2.4 cm (AUC=0.90, P<0.001) was determined and an elevated ASFT was significantly associated with a positive GDM (unadjusted odds ratio, 2.91; 95% CI, 1.07 to 7.92; P=0.034). Therefore, when ASFT at the first trimester of pregnancy is 2.4 cm or more, adequate management is required and care practitioners should be alerted to the possibility of GDM and make efforts to manage diabetes during pregnancy.
- One limitation of this study was the inclusion of pregnant women who were admitted to a single general hospital; therefore, these subjects are not representative of the entire population of pregnant women in Korea. Furthermore, various studies have reported different lengths of US-determined visceral fat and subcutaneous fat, and our results did not yield sufficient intraobserver reliability. This suggests the need for standardized measurement methods. In future studies, an identical ASFT measurement method must be applied to a larger population of patients, and this process should be used to standardize the measurement methods.
- In conclusion, the results of this study demonstrated that ASFT as measured by ultrasound during the first trimester of pregnancy can be a valuable indicator for predicting GDM during the second trimester. Thus, ASFT, information that can be easily obtained during the first trimester of pregnancy, is expected to be increasingly utilized as an auxiliary diagnostic criterion for predicting the risk of GDM during the second trimester of pregnancy.
DISCUSSION
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
- 1. Metzger BE, Coustan DR. Summary and recommendations of the Fourth International Workshop-Conference on Gestational Diabetes Mellitus. The Organizing Committee. Diabetes Care 1998;21(Suppl 2):B161-B167. PubMed
- 2. Kang HJ, Kwak HM, Kim YS, Park JS, Yoon G, Choi SJ, Oh SY, Kim JH, Roh CR. Obstetric and neonatal outcomes after treatment of gestational diabetes mellitus class A1 and class A2. Korean J Obstet Gynecol 2010;53:681-686.Article
- 3. National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979;28:1039-1057. ArticlePubMedPDF
- 4. Crowther CA, Hiller JE, Moss JR, McPhee AJ, Jeffries WS, Robinson JS. Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. ACHOIS) Trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med 2005;352:2477-2486. ArticlePubMed
- 5. Kim MJ, Lee SK, Lee JA, Lee PR, Park HS. Risk factors for gestational diabetes mellitus in Korean women. Korean J Obes 2013;22:85-93.Article
- 6. Choi HM. Perinatal outcomes associated with prepregnancy body mass index and weight gain during pregnancy. Korean J Obstet Gynecol 2010;53:981-987.Article
- 7. Bray GA, Jablonski KA, Fujimoto WY, Barrett-Connor E, Haffner S, Hanson RL, Hill JO, Hubbard V, Kriska A, Stamm E, Pi-Sunyer FX. Diabetes Prevention Program Research Group. Relation of central adiposity and body mass index to the development of diabetes in the Diabetes Prevention Program. Am J Clin Nutr 2008;87:1212-1218. ArticlePubMed
- 8. Sadro CT, Dubinsky TJ. CT in pregnancy: risks and benefits. Appl Radiol 2013;42:6-16.Article
- 9. Bartha JL, Marin-Segura P, Gonzalez-Gonzalez NL, Wagner F, Aguilar-Diosdado M, Hervias-Vivancos B. Ultrasound evaluation of visceral fat and metabolic risk factors during early pregnancy. Obesity (Silver Spring) 2007;15:2233-2239. ArticlePubMed
- 10. Landy HJ, Gomez-Marin O, O'Sullivan MJ. Diagnosing gestational diabetes mellitus: use of a glucose screen without administering the glucose tolerance test. Obstet Gynecol 1996;87:395-400. ArticlePubMed
- 11. World Health Organization. Regional Office for the Western Pacific. The Asia-Pacific perspective: redefining obesity and its treatment. Sydney: Health Communications Australia; 2000.
- 12. Metzger BE. Long-term outcomes in mothers diagnosed with gestational diabetes mellitus and their offspring. Clin Obstet Gynecol 2007;50:972-979. ArticlePubMed
- 13. Park MI, Kim JJ, Lee JH, Kim SR, Ahn YH. The significance of 50 gm-oral glucose tolerance test in the screening of gestational diabetes mellitus. Korean J Obstet Gynecol 1998;41:2126-2130.
- 14. Makgoba M, Savvidou MD, Steer PJ. An analysis of the interrelationship between maternal age, body mass index and racial origin in the development of gestational diabetes mellitus. BJOG 2012;119:276-282. ArticlePubMed
- 15. Philipsen A, Carstensen B, Sandbaek A, Almdal TP, Johansen NB, Jorgensen ME, Witte DR. Reproducibility of ultrasonography for assessing abdominal fat distribution in a population at high risk of diabetes. Nutr Diabetes 2013;3:e82. ArticlePubMedPMCPDF
- 16. Kennedy NJ, Peek MJ, Quinton AE, Lanzarone V, Martin A, Benzie R, Nanan R. Maternal abdominal subcutaneous fat thickness as a predictor for adverse pregnancy outcome: a longitudinal cohort study. BJOG 2016;123:225-232. ArticlePubMed
- 17. Gur EB, Ince O, Turan GA, Karadeniz M, Tatar S, Celik E, Yalcin M, Guclu S. Ultrasonographic visceral fat thickness in the first trimester can predict metabolic syndrome and gestational diabetes mellitus. Endocrine 2014;47:478-484. ArticlePubMedPDF
- 18. De Souza LR, Berger H, Retnakaran R, Maguire JL, Nathens AB, Connelly PW, Ray JG. First-trimester maternal abdominal adiposity predicts dysglycemia and gestational diabetes mellitus in midpregnancy. Diabetes Care 2016;39:61-64. ArticlePubMedPDF
REFERENCES
Measuring abdominal subcutaneous fat thickness using a high-resolution ultrasonography at 1 cm above the umbilical level.
A flow chart of the study design (normal group [n=292], gestational diabetes mellitus group [n=41]). OGTT, oral glucose tolerance test.
Receiver operating characteristic curve of predicting gestational diabetes mellitus measured pre-pregnancy body mass index (BMI) and abdominal subcutaneous fat thickness (ASFT) using ultrasonography.
Differences between normal groups (control and NGT) and gestational diabetes mellitus (n=333)
Receiver operating characteristic prediction curve analysis of variables
Elevated abdominal subcutaneous fat thickness in the first trimester of pregnancy and associated risk of an elevated glucose challenge test (100 g OGTT) in the second trimester of pregnancy
| NGT (n=31) | Gestational diabetes mellitus (n=41) | |||
|---|---|---|---|---|
| No. | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | ||
| ASFT <2.4 cm | 15 | 10 | 1.0 (reference) | 1.0 (reference) |
| ASFT ≥2.4 cm | 16 | 31 | 2.91 (1.07–7.92) | 2.96 (0.95–9.25) |
Figure & Data
References
Citations
- Abdominal subcutaneous fat thickness combined with a 50-g glucose challenge test at 24-28 weeks of pregnancy in predicting gestational diabetes mellitus
Süleyman Cemil Oğlak, Emine Zeynep Yılmaz, Mehmet Şükrü Budak
Journal of Obstetrics and Gynaecology.2024;[Epub] CrossRef - The Value of Maternal Upper Abdominal Ad-ipose Thickness in Predicting GDM in Early Pregnancy
娜娜 郭
Advances in Clinical Medicine.2023; 13(03): 4702. CrossRef - Evaluating the Adipose Tissue Depth as a Predictor Factor for Gestational Diabetes in Later Pregnancy—A Systematic Review
Bianca-Margareta Salmen, Valeria-Anca Pietrosel, Cristiana-Elena Durdu, Teodor Salmen, Cosmina Theodora Diaconu, Ioana-Cristina Bica, Claudia Gabriela Potcovaru, Florentina Gherghiceanu, Roxana-Adriana Stoica, Anca Pantea Stoian
Biomedicines.2023; 11(5): 1492. CrossRef - The Association Between Body Fat Index and Gestational Diabetes Mellitus: A Prospective Cohort Study
Sawanya Benchahong, Prasert Sunsaneevithayakul, Dittakarn Boriboonhirunsarn
Cureus.2023;[Epub] CrossRef - Ultrasound evaluation of subcutaneous and visceral abdominal fat as a predictor of gestational diabetes mellitus: a systematic review
Fernanda Teixeira Benevides, Edward Araujo Júnior, Carla Soraya Costa Maia, Renan Magalhães Montenegro Junior, Francisco Herlânio Costa Carvalho
The Journal of Maternal-Fetal & Neonatal Medicine.2022; 35(11): 2216. CrossRef - The Early Sonographic Prediction of Gestational Diabetes in Women From India
Shivani Gupta, Arjun Gupta, C. P. Swarnakar, Monika Rathore, Ramesh Beniwal, Kiran Meena, Anita Simlot, Nidhi Gupta
Journal of Diagnostic Medical Sonography.2022; 38(1): 18. CrossRef - Can maternal abdominal fat thickness predict antenatal insulin therapy in patients with gestational diabetes mellitus?
Sedat Akgöl, Mehmet Şükrü Budak, Süleyman Cemil Oğlak, Fatma Ölmez, Mehmet Emin Dilek, Serhat Kartal
Journal of Obstetrics and Gynaecology Research.2022; 48(3): 634. CrossRef - Prediction of gestational diabetes mellitus by different obesity indices
Zhimin Song, Yan Cheng, Tingting Li, Yongfang Fan, Qingying Zhang, Haidong Cheng
BMC Pregnancy and Childbirth.2022;[Epub] CrossRef - Association between maternal adiposity measures and adverse maternal outcomes of pregnancy: Systematic review and meta‐analysis
Nicola Heslehurst, Lem Ngongalah, Theophile Bigirumurame, Giang Nguyen, Adefisayo Odeniyi, Angela Flynn, Vikki Smith, Lisa Crowe, Becky Skidmore, Laura Gaudet, Alexandre Simon, Louise Hayes
Obesity Reviews.2022;[Epub] CrossRef - Association of body composition in early pregnancy with gestational diabetes mellitus: A meta-analysis
Fatemeh Alsadat Rahnemaei, Fatemeh Abdi, Reza Pakzad, Seyedeh Hajar Sharami, Fatemeh Mokhtari, Elham Kazemian, Rajakumar Anbazhagan
PLOS ONE.2022; 17(8): e0271068. CrossRef - Early Gestational Diabetes Detection Using Neural Network
Tanzina Rahman Hera, Md. Ashikur Rahman Khan, Nishu Nath
WSEAS TRANSACTIONS ON BIOLOGY AND BIOMEDICINE.2021; 18: 1. CrossRef - The association of general obesity, central obesity and visceral body fat with the risk of gestational diabetes mellitus: Evidence from a systematic review and meta-analysis
Sura M. Alwash, H. David McIntyre, Abdullah Mamun
Obesity Research & Clinical Practice.2021; 15(5): 425. CrossRef - Abdominal skin subcutaneous fat thickness over the gestational period in Korean pregnant women: a descriptive observational study
Moon Sook Hwang
Korean Journal of Women Health Nursing.2021; 27(4): 318. CrossRef - Relationship between Maternal Central Obesity and the Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Cohort Studies
Da Yao, Qing Chang, Qi-Jun Wu, Shan-Yan Gao, Huan Zhao, Ya-Shu Liu, Yu-Ting Jiang, Yu-Hong Zhao
Journal of Diabetes Research.2020; 2020: 1. CrossRef - Maternal Adipose Tissue Expansion, A Missing Link in the Prediction of Birth Weight Centile
Eleanor M Jarvie, Frances M Stewart, Jane E Ramsay, E Ann Brown, Barbara J Meyer, Gunilla Olivecrona, Bruce A Griffin, Dilys J Freeman
The Journal of Clinical Endocrinology & Metabolism.2020; 105(3): e814. CrossRef - Ultrasound assessment of maternal adipose tissue during 1st trimester screening for aneuploidies and risk of developing gestational diabetes
Francesco D’Ambrosi, Gabriele Rossi, Chiara M. Soldavini, Matteo Di Maso, Ilma F. Carbone, Giulia E. Cetera, Enrico Colosi, Enrico Ferrazzi
Acta Obstetricia et Gynecologica Scandinavica.2020; 99(5): 644. CrossRef - Vitamin D Deficiency at Mid-Pregnancy Is Associated with a Higher Risk of Postpartum Glucose Intolerance in Women with Gestational Diabetes Mellitus
Kyung-Soo Kim, Seok Won Park, Yong-Wook Cho, Soo-Kyung Kim
Endocrinology and Metabolism.2020; 35(1): 97. CrossRef - Fetal pancreatic hyperechogenicity may be an early ultrasonographic sign of gestational diabetes mellitus
Hatice Akkaya, Barış Büke, Gülsüm Uysal
The Journal of Maternal-Fetal & Neonatal Medicine.2020; 33(14): 2387. CrossRef The Body Composition in Early Pregnancy is Associated with the Risk of Development of Gestational Diabetes Mellitus Late During the Second Trimester
Yanping Liu, Jing Liu, Yinjie Gao, Dan Zheng, Wei Pan, Min Nie, Liangkun Ma
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2020; Volume 13: 2367. CrossRef- New Diagnostic Criteria for Gestational Diabetes Mellitus and Pregnancy Outcomes in Korea
Kyu Yeon Hur
Diabetes & Metabolism Journal.2019; 43(6): 763. CrossRef - Inter and intra-reliability of ultrasonography for the measurement of abdominal subcutaneous & visceral adipose tissue thickness at 12 weeks gestation
Alexandra Cremona, Kevin Hayes, Clodagh S. O’Gorman, Ciara Ní Laighin, Khadijah I. Ismail, Alan E. Donnelly, Jill Hamilton, Amanda Cotter
BMC Medical Imaging.2019;[Epub] CrossRef - Maternal abdominal subcutaneous fat thickness as a simple predictor for gestational diabetes mellitus
Mehmet Sukru Budak, Ilker Kahramanoglu, Salvatore Giovanni Vitale, Sedat Akgol, Mehmet Emin Dilek, Serhat Kartal, Salvatore Caruso, Bekir Kahveci, Mehmet Obut, Muhammed Hanifi Bademkiran, Antonio Cianci
Journal of Perinatal Medicine.2019; 47(6): 605. CrossRef - Hypertriglyceridemia and Waist Phenotype as Markers in the Prediction of Gestational Diabetes in Iraqi Women
Faris Anwer Rasheed, Raghad Hasan Mshattat, Ulfat Mohammad Alnakkash, Saad Abdulrahma
Research Journal of Obstetrics and Gynecology.2018; 11(1): 25. CrossRef - The importance of treating mild hyperglycemia in pregnant women with diabetes
Kyung-Soo Kim
The Korean Journal of Internal Medicine.2018; 33(6): 1079. CrossRef - Anthropometric and ultrasound measures of maternal adiposity in the first trimester of pregnancy
Narelle Kennedy, Ann Quinton, Michael John Peek, Valeria Lanzarone, Ron Benzie, Ralph Nanan
Australasian Journal of Ultrasound in Medicine.2018; 21(3): 147. CrossRef - Simple Screening Using Ultrasonography for Prediction of Gestational Diabetes Mellitus
Seung Min Chung, Jun Sung Moon
Diabetes & Metabolism Journal.2017; 41(6): 438. CrossRef
 PubReader
PubReader Cite
Cite





