Association between the Thigh Muscle and Insulin Resistance According to Body Mass Index in Middle-Aged Korean Adults
Article information

Abstract
Background
We examined the associations between thigh muscle area (TMA) and insulin resistance (IR) according to body mass index (BMI) in middle-aged Korean general population.
Methods
TMA was measured using quantitative computed tomography and corrected by body weight (TMA/Wt) in 1,263 men, 788 premenopausal women, and 1,476 postmenopausal women all aged 30 to 64 years. The tertiles of TMA/Wt were calculated separately for men and for premenopausal and postmenopausal women. Homeostatic model assessment for insulin resistance (HOMA-IR) was performed using fasting blood glucose and insulin levels, and increased IR was defined according to sex-specific, top quartiles of HOMA-IR. Associations between the TMA/Wt tertiles and increased IR according to the BMI categories (<25 and ≥25 kg/m2) were assessed using multivariable logistic regression analysis.
Results
In men with higher BMIs, but not in those with lower BMIs, the presence of an increased IR had significantly higher odds ratios in the lower TMA/Wt tertiles, even after adjustment for visceral fat area. However, in premenopausal and postmenopausal women, there was no significant inverse association between TMA/Wt tertiles and increased IR, regardless of BMI category.
Conclusion
Our findings suggest that the thigh muscle is inversely associated with IR in men, particularly in those with higher BMIs.
INTRODUCTION
Sarcopenia, the degenerative loss of skeletal muscle mass, could be associated with a cardio-metabolic risk, metabolic disease, and psychological disorders [123]. Many studies have reported a significant inverse association between muscle mass and insulin resistance (IR). However, most of these studies were conducted in older adults or people with chronic conditions, such as diabetes mellitus, chronic obstructive pulmonary disease, or end-stage renal disease [45678]. Some studies have been conducted in general populations [24891011], but only few of them targeted middle-aged population [211]. And the results were inconsistent. One study found a significant association between low muscle mass and higher IR in a middle-aged population [11]. Another noted a significant association between low muscle mass and higher IR in an older adult population, but was unable to document the same association in a middle-aged population [2]. Although the initiation of muscle decline starts in the middle age, little information is available regarding the independent impact of low muscle mass and IR in the middle-aged general population.
Several lifestyle factors, including smoking, alcohol consumption, exercise, and protein intake, could be determinants of decreases in muscle mass and function, and age-related muscle decline could be more prominent in men than in women [12]. Although many characteristics differ between men and women, most studies on associations between muscle mass and IR have only addressed these differences in their analyses by adjustment, instead of stratification. Also, previous studies have demonstrated different trends in muscle and obesity indicators, including visceral fat, according to the menopausal status of women [13]. These differences according to sex and menopausal status could modify the relationships between muscle mass and IR, but there are not enough studies and the mechanisms are not well established. In addition, it should be investigated whether the impacts of the muscle mass on IR are independent from those of known risk factors, including lifestyle factors and obesity status [141516].
Accordingly, we sought to evaluate the independent relationship between thigh muscle area (TMA) measured using quantitative computed tomography (QCT) and IR according to different body mass index (BMI) categories in middle-aged, relatively healthy, men and premenopausal and postmenopausal women.
METHODS
Study population
The present study utilized data from the Cardiovascular and Metabolic Disease Etiology Research Center (CMERC) cohort study, which was designed to recruit members of the general population residing in four districts (Seoul, Goyang, Gimpo, and Incheon) in South Korea. The inclusion criteria were 30 to 64 years of age, residing more than 8 months of the year at current residence with no plans to move over the next 2 years, and having the ability to provide verbal or written consent to participate in the study. Participants were excluded if they had been diagnosed with cancer within the last 2 years or were currently being treated for cancer; had a history of myocardial infarction, stroke, or heart failure; were currently involved in pharmaceutical trials; or were currently pregnant or reported the possibility of being pregnant on the day of registration. The detailed methods for the CMERC cohort study have been reported elsewhere [17]. This study initially enrolled 4,060 participants between 2013 and 2017. All participants completed health questionnaires and examinations according to a predefined protocol. Those with missing TMA variables (n=268), those who were treated for diabetes mellitus (n=190), and those with a BMI under 18.5 kg/m2 (n=75) were excluded from the current analysis. Finally, a cross-sectional analysis was conducted of the remaining 1,263 men, 788 premenopausal women, and 1,476 postmenopausal women. All participants provided written informed consent, and the study protocol was approved by the Institutional Review Board of Severance Hospital at Yonsei University College of Medicine (IRB No. 4-2013-0661).
Measurements
All participants were individually interviewed using standardized questionnaires to obtain information regarding demographics, health behaviors, and medication use. Trained interviewers conducted face-to-face interviews and administered questionnaires according to a standard protocol. Health behaviors included smoking status (current smoker, former smoker, or non-smoker), alcohol intake (current heavy drinker, current non-heavy drinker, former drinker, or non-drinker), physical activity, and sleep duration. Average alcohol consumption (in grams per drinking day) was calculated using the average number of alcoholic beverages consumed and the frequency of alcohol consumption, and then converted into the amount of ethanol in grams. Current heavy drinking was defined as drinking >40 g ethanol per drinking day for men and >20 g per drinking day for women for two or more times a week [18]. Physical activity was assessed using the International Physical Activity Questionnaire-Short Form. For this study, high activity referred to activities that considerably increased an individual's respiratory effort, whereas moderate activity referred to those that moderately increased respiratory effort. Regular exercise was defined as moderate-to-high-intensity physical activity performed at least three times per week. Sleep duration was recorded in hours per day (hr/day) and as the average over the past year. Medication use (antihypertensive and lipid-lowering) was assessed by self-reports.
The study participants wore lightweight clothing for convenient and reliable examinations. BMI was calculated as the body weight divided by the standing height squared (kg/m2). Waist circumference was assessed to the nearest 0.1 cm at the midpoint between the lower border of the rib cage and the iliac crest using an ergonomic circumference-measuring tape (SECA 201; SECA, Hamburg, Germany). Participants rested for 5 minutes before the blood pressure measurement, and systolic and diastolic blood pressures were repeatedly measured three times at 2-minute intervals. The average of the second and third measurements was used for analysis. Hypertension was defined as a systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or a self-report of current use of an antihypertensive medication.
Blood samples were collected from the antecubital vein after the patients had fasted for at least 8 hours. Fasting blood glucose concentrations were measured using a colorimetry method (ADVIA 1800 Auto Analyzer; Siemens Medical Solutions, Malvern, PA, USA). Serum insulin concentrations were measured with a radioimmunoassay (SR-300; Stratec, Birkenfeld, Germany). Glycosylated hemoglobin concentrations were assessed using high-performance liquid chromatography (Variant II TURBO; Bio-Rad, Berkeley, CA, USA) according to the National Glycohemoglobin Standardization Program guidelines. IR was evaluated using the homeostasis model assessment of IR (HOMA-IR) and was calculated as follows: fasting plasma glucose (mg/dL)×fasting plasma insulin (mIU/mL)/405 [19]. Increased IR was defined as ranking in the top 25th percentile of HOMA-IR values separately for men (≥2.711), premenopausal women (≥2.148), and postmenopausal women (≥2.318) [20]. Pre-diabetes was defined as a fasting glucose level of 100 to 126 mg/dL or a glycosylated hemoglobin level of 5.7 to 6.5% according to the American Diabetes Association criteria [21]. Total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglyceride levels were measured using enzymatic methods (ADVIA 1800 Auto Analyzer). Dyslipidemia was defined as a total cholesterol level ≥240 mg/dL, or a high-density lipoprotein cholesterol level ≤40 mg/dL, or a low-density lipoprotein cholesterol level ≥160 mg/dL, or a triglycerides level ≥200 mg/dL according to the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults or as people who were taking lipid-lowering medication. C-reactive protein concentrations were determined with a turbidimetric immunoassay (ADVIA 1800 Auto Analyzer).
TMA and visceral fat area were measured by QCT using a Somatom Definition AS+ 128-channel CT (Siemens Healthcare, Forchheim, Germany), a Somatom sensation 64-channel CT (Siemens Healthcare), or a GE Lightspeed VCT scanner (General Electric Medical System, Milwaukee, WI, USA). Scanning was performed at 120 kVp and 150 mAs and a pitch of 1.0. Images were reconstructed with a 3-mm slice thickness. Voxels were separated into fat and muscle tissue according to Hounsfield units (HU): −190 to −30 HU for fat and 30 to 100 HU for muscle. All scanned data were analyzed using Aquarius intuition Viewer version 4.4.12 software (Terarecon, Foster City, CA, USA). TMA was recorded as the mean of right and left TMA values. TMA was found to be correlated with body size (r=0.566 in men, r=0.491 in premenopausal women, and r=0.463 in postmenopausal women), indicating that participants with a larger body size may have larger TMA. Therefore, TMA was corrected by body weight (TMA/Wt, cm2/kg) [22]. The participants were divided into three groups according to sex and menopausal-specific TMA/Wt tertiles: <338.9, 338.9−377.7, and ≥377.8 for men; <276.5, 276.5–309.1, and ≥309.2 for premenopausal women; and <261.0, 261.0–292.4, and ≥292.5 for postmenopausal women.
Statistical analysis
We evaluated differences in demographic characteristics among the three groups based on the TMA/Wt tertiles, and we used one-way analysis of variance for normally distributed variables, Kruskal-Wallis test for skewed variables, and chi-square test for categorical variables. The P for trend was calculated using a contrast to test for linear trends in continuous variables and the Cochran-Armitage test for categorical variables.
Multivariable logistic regression analyses were used to assess independent associations between TMA/Wt (using tertiles and continuous variables) and the likelihood of an increased IR in three adjusted models: [1] adjusted for age; [2] additionally adjusted for systolic blood pressure, triglyceride level, smoking, alcohol intake, exercise, and sleep duration; and [3] additionally adjusted for visceral fat area. We conducted the above-mentioned analyses separately for men, premenopausal, and postmenopausal women, because there were significant interactions between sex and TMA/Wt (P for interaction=0.028) and a borderline interaction between menopausal status and TMA/Wt (P for interaction=0.065) in the presence of an increased IR and because both TMA/Wt and HOMA-IR significantly differed according to sex and menopausal status in women (Supplementary Table 1).
The associations between TMA/Wt (using tertiles and continuous variables) and the likelihood of an increased IR were also assessed in people with lower (<25.0 kg/m2) and higher BMIs (≥25.0 kg/m2) using the same models. Then, we also analyzed interactions between TMA/Wt tertiles and BMI categories for the presence of an increased IR in men and in premenopausal and postmenopausal women. All statistical tests were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was defined as a two-sided P value <0.05.
RESULTS
The general characteristics of the study participants are presented in Supplementary Table 1. This study included 1,263 men, 788 premenopausal women, and 1,476 postmenopausal women, with mean ages of 49.8, 43.0, and 57.1 years, respectively. Both mean TMA/Wt and median HOMA-IR values were significantly higher in men than in women. Mean TMA/Wt was significantly higher in premenopausal than in postmenopausal women. Conversely, the median HOMA-IR was significantly higher in postmenopausal than in premenopausal women.
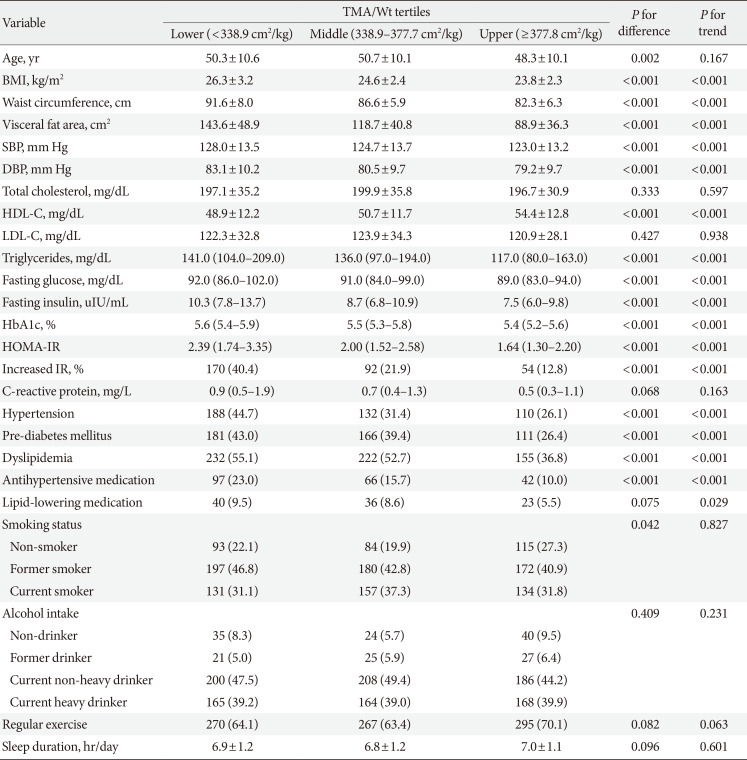
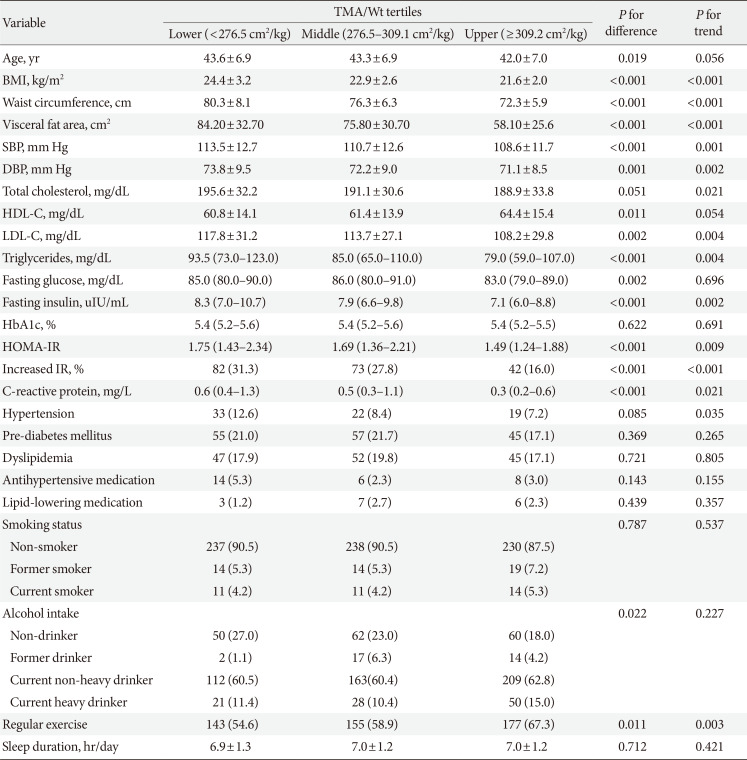
Table 1 shows the general characteristics of the men according to TMA/Wt tertiles. Men in the lower TMA/Wt tertiles tended to have higher obesity indices, blood pressure, triglycerides, and HOMA-IR values; higher frequencies of former smokers; and higher frequencies of hypertension, pre-diabetes mellitus, and dyslipidemia. Tables 2 and 3 show the general characteristics of the premenopausal and postmenopausal women, respectively, according to TMA/Wt tertiles. Both premenopausal and postmenopausal women in the lower TMA/Wt tertiles tended to have higher obesity indices, blood pressure, lipid profile, HOMA-IR, C-reactive, and protein levels; higher frequencies of hypertension; and lower frequencies of regular exercise. Postmenopausal women in the lower TMA/Wt tertiles tended to have higher frequencies of pre-diabetes mellitus and dyslipidemia and lower frequencies of current heavy drinking, unlike premenopausal women.

Characteristics in men (n=1,263) according to TMA/Wt tertiles

Characteristics in premenopausal women (n=788) according to TMA/Wt tertiles

Characteristics in postmenopausal women (n=1,476) according to TMA/Wt tertiles
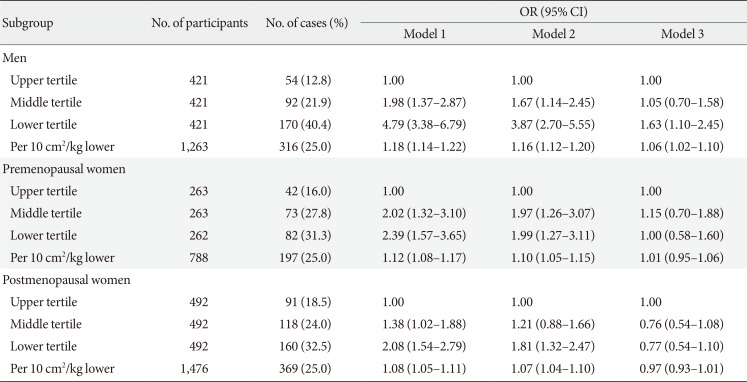
Table 4 presents the results of the multivariable logistic regression models for the associations between TMA/Wt (as tertiles and continuous variables) and increased IR in men, premenopausal, and postmenopausal women. In men, even after adjustment for potential confounders, including visceral fat area, the presence of an increased IR was significantly higher in the lower TMA/Wt tertile (odds ratio [OR], 1.63; 95% confidence interval [CI], 1.10 to 2.45), but was not significant in the middle tertile (OR, 1.05; 95% CI, 0.70 to 1.58), relative to the upper tertile. In this model, which included TMA/Wt as a continuous variable, the multivariable-adjusted OR increased by 1.06 (95% CI, 1.02 to 1.10) per 10 cm2/kg lower TMA/Wt. However, in both premenopausal and postmenopausal women, an association between TMA/Wt and increased IR was not observed after additionally adjustment for visceral fat area. We also repeated the analysis using fasting glucose and fasting insulin levels as dependent variables instead of HOMA-IR and observed similar results (data not shown).

Association between TMA/Wt and increased IR in men and premenopausal and postmenopausal women
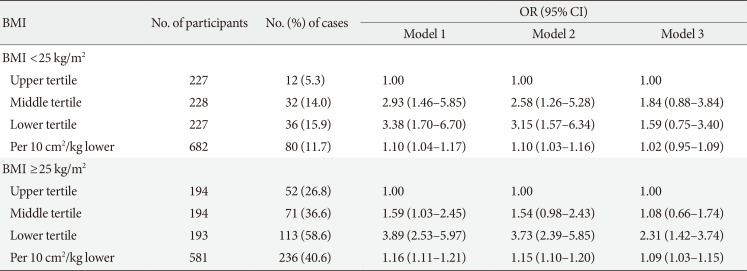
Table 5 presents the associations between TMA/Wt and increased IR according to the BMI categories in men. Among men with lower BMIs, the presence of an increased IR had higher, but non-significant, ORs in the lower and middle TMA/Wt tertiles. However, among men with higher BMIs, the presence of an increased IR showed significantly higher ORs in the lower TMA/Wt tertiles than in the upper TMA/Wt tertile. There was a significant interaction between the TMA/Wt tertiles and BMI categories in the presence of an increased IR in men (P for interaction=0.046).

Association between TMA/Wt and increased IR according to BMI categorization in men
Conversely, there were no significant associations between TMA/Wt and increased IR, regardless of BMI category, in premenopausal and postmenopausal women. Also, there were no significant interactions between TMA/Wt tertiles and BMI categories in the presence of an increased IR in premenopausal (P for interaction=0.093) or postmenopausal (P for interaction= 0.853) women (Supplementary Table 2).
DISCUSSION
The current study found that a lower thigh muscle was independently associated with a higher IR, even after adjustment for traditional risk factors, in a cohort of middle-aged Korean men with higher BMIs, but not in men with lower BMIs. This trend was not observed in premenopausal and postmenopausal women, regardless of the BMI category.
Associations between muscle mass and IR have been reported in animal [23] and human studies [121124252627], including a gene analysis [28]. One of these results is consistent [24] with ours, and one is inconsistent [25]. Some studies are incomparable [2112627] because they did not stratify by the obesity status. One study [24] reported that people with a lower muscle mass and higher BMIs had significantly higher ORs for IR, particularly in a middle-aged population. Another study [25] suggested that people with a lower muscle mass and lower BMIs had a significantly higher OR for IR. This inconsistent results might be due to not adjusting for central obesity, which could be highly correlated with the IR, particularly in the lower-BMI population [29]. Other studies [2112627] had similar results with ours; however, comparison is difficult because a stratified analysis according to sex and obesity status was not performed in those studies. Although two of them [2627] conducted a longitudinal analysis between low muscle mass and higher IR it might be hard to identify an independent effect of the low muscle because it was not adjusted by the body size. Except for one study [26], most previous studies used an estimated muscle mass, instead of a measured muscle area.
Unlike previous studies, we measured TMA using QCT in a large general population and excluded the potential effect of antidiabetic treatment on the association between thigh muscle and IR, excluding the patients who were taking antidiabetic medications. We also tried to control for confounders not only by adjusting for risk factors, including central obesity, but also by stratifying by sex, menopausal status, and overall obesity status.
The underlying mechanisms of the association between low muscle mass and higher IR are not fully understood. One of the potential explanations is that muscle tissue is the primary tissue responsible for insulin-mediated glucose disposal; hence, a low muscle mass could cause a decreased insulin-mediated glucose disposal, followed by higher IR. Another explanation could be in lifestyle factors, including smoking, alcohol intake, and physical activity. In the present study, after adjusting for these lifestyle factors, ORs were slightly weakened, but still remained significant in men. This suggested that lifestyle factors might partially, but not fully, explain the association between low muscle mass and higher IR. In the current study, according to stratification analyses by BMI categories, a significant inverse association was only observed in men with higher BMIs. Interestingly, while age-related muscle loss has been shown to be due to a reduction in muscle fibers and fiber atrophy [30], participants with obesity [313233], particularly men [34], also have increased ceramides in their muscle fibers, as well as fewer muscle fibers, which plays an important role in IR.
In women, regardless of menopausal status, the significant association disappeared after adjusting for the visceral fat area. This finding could suggest that the differences in body composition between men and women may modify the relationship between muscle and IR. First, age-related decreases in skeletal muscle mass and muscle strength are inevitable in both men and women; however, they are more prominent in men than in women [12]. This could be affected by the sex-specific effects of sex hormones. In men, testosterone levels generally control changes in skeletal muscle mass, and in women, there is much less of an absolute decline in testosterone levels with aging than that in men. Thus, women may not experience the effects of testosterone decline on skeletal muscle mass. Additionally, female sex hormones, especially estrogen, have been found to provide protective effects on adipocyte inflammation, oxidative stress, and IR in an animal study [35]. Second, fat distributions are different between men and women. Adipose tissue primarily accumulates around the trunk and abdomen in men, but around the hips and thighs in women [3637]. According to previous studies, although the absolute amount of visceral fat area is higher in men than in women, the risk of visceral fat area on cardiometabolic abnormalities is higher in women than in men [38]. A possible reason for this is that the thigh muscle might have a relatively smaller impact on the IR in women than in men [39], due to the preexisting risk of fat on metabolic imbalance [40]. In this regard, women would likely be less affected by muscle declines than men.
After stratification according to menopausal status, lower thigh muscle tended to be associated with higher IR in premenopausal women, whereas higher thigh muscle was tended to be associated with higher IR in postmenopausal women. Nevertheless, both of these trends were not significant. Instead of thigh muscle mass, age and visceral fat area were significantly associated with increased IR in premenopausal women, while blood pressure, triglycerides, and visceral fat area were significantly associated with increased IR in postmenopausal women (Supplementary Table 3). Several previous studies [414243] have reported that postmenopausal women have greater abdominal fat, higher blood pressure, higher lipid profiles than premenopausal women even after adjustment for age, and these risk factors could have great harmful impact on higher IR than protective effect of greater muscle mass. Further studies are needed to confirm which ways associations differ between premenopausal and postmenopausal women, as well as between men and women.
The current study had a few limitations. First, TMA was measured using QCT, but more detailed characteristics such as thigh intramuscular or intermuscular fat content were not measured. Previous research has indicated that there are sex differences in mid-thigh composition, such as muscle density, which is a marker of muscle fat infiltration [4445]. Although fat infiltration in a muscle accounts for a relatively small portion of the muscle, not considering muscle fat infiltration may not represent the muscles of women well. Second, we used HOMA-IR as a surrogate marker for IR. However, it is frequently used for assessing IR in large population-based studies, because it takes minimal time, is not invasive, and shows excellent predictability for IR [46]. Third, both the thigh muscle and IR were measured only once; therefore, we cannot exclude the possibility of random measurement errors that might have weakened the observed association. Fourth, we might not have completely accounted for all residual confounders. Finally, this study was cross-sectional in nature; therefore, a causal association between low thigh muscle mass and higher IR is uncertain.
In conclusion, we found an association between lower thigh muscle mass and higher IR in men, particularly those with higher BMIs, but not in those with lower BMIs, even after adjusting for traditional risk factors. Our findings suggest that the maintenance of both an appropriate BMI and thigh muscle is important for normal IR in middle-aged Korean men.
ACKNOWLEDGMENTS
This work was supported by the Korea Health Technology R&D Project (grant number: HI13C0715) funded by the Ministry of Health and Welfare of the Republic of Korea.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS:
Conception or design: J.E.H., H.C.K.
Acquisition, analysis, or interpretation of data: J.E.H., J.S.S., H.C.K.
Drafting the work or revising: J.E.H., H.L., H.C.K.
Final approval of the manuscript: J.E.H., J.S.S., H.L., H.C.K.
References
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2019.0110.
Supplementary Table 1
Characteristics of the study participants
Supplementary Table 2
Association between TMA/Wt and increased IR according to BMI categorization in premenopausal and postmenopausal women
Supplementary Table 3
Determinants of increased IR in premenopausal and postmenopausal women