Influence of Visceral Adiposity on Cardiovascular Autonomic Neuropathy in Patients with Type 2 Diabetes Mellitus
Article information
Abstract
Background
The aim of this study was to investigate the influences of visceral adiposity on cardiovascular autonomic neuropathy (CAN) in patients with type 2 diabetes mellitus.
Methods
Two hundred eleven patients with type 2 diabetes participated in this study. Anthropometric and metabolic parameters were measured, and the visceral fat area was assessed using computed tomography. CAN was diagnosed using a cardiovascular reflex test. We analyzed the correlation between the visceral fat area and each parameter in this test.
Results
The mean age, body mass index (BMI), and duration of diabetes of the study population were 60±14 years (mean±standard deviation), 25.1±4.2 kg/m2, and 12.3±8.9 years, respectively. The visceral fat area showed positive correlations with age, BMI, waist circumference, and subcutaneous fat area. There was no statistically significant difference in the cardiovascular reflex test outcome between genders. Univariate linear regression analysis showed that an increased visceral fat area diminished good heart rate response to a Valsalva maneuver (R2=4.9%, P=0.013 in an unadjusted model), but only in women. This statistical association was preserved after adjusting for age and BMI (R2=9.8%, P=0.0072).
Conclusion
The results of this study suggest that visceral adiposity contributes to an autonomic imbalance to some degree, as demonstrated by the impaired cardiovascular reflex test among women with type 2 diabetes.
INTRODUCTION
Cardiovascular autonomic neuropathy (CAN) is often overlooked because of vague symptoms and signs [1], although it is a common early complication in patients with diabetes mellitus [2]. Several prospective studies have found that CAN is linked to the increase of cardiovascular mortality and morbidity related with orthostatic hypotension, silent myocardial ischemia, coronary artery disease, stroke, perioperative morbidity, and the limitation of exercise capacity [3-7]. Thus, early detection and proper management of CAN may reduce the potential economic burden on persons with diabetes and entire society.
The prevalence of CAN varies from 2.5% to 50% because of variable diagnostic criteria and diverse diagnostic methods [5]. The American Diabetes Association (ADA) considers the cardiovascular reflex test to be the proper diagnostic test of CAN because it has good sensitivity, specificity, reproducibility, and is easily performed [5]. It is widely used to assess cardiac parasympathetic function based on the time-domain heart rate response to deep breathing, a Valsalva maneuver, and postural change [2,5]. From previous reports, the best-known risk factors for CAN in patients with type 2 diabetes are the duration of diabetes and poor glycemic control [8]. Other factors related to CAN are being male, hypertension, insulin resistance, obesity, high triglyceride concentration, smoking, alcohol consumption, and, more recently suggested, central obesity measured by waist circumference [9-11]. Some studies have shown that visceral obesity is related to metabolic syndrome, insulin resistance, and dyslipidemia in obese patients with or without diabetes but few studies have compared the relationship directly between visceral fat area and CAN in type 2 diabetes [12-16]. Thus, we focused on the correlation between visceral fat area measured by visceral fat computed tomography (CT) scanning and the each parameters of the cardiovascular reflex test in the patients with type 2 diabetes mellitus.
METHODS
Participant recruitment
In this cross-sectional study, 211 consecutive patients were recruited during the period of October 2009 to March 2011 and were referred to the inpatient diabetes services for glycemic control only. The inclusion criteria of this study were: an adult older than 20 years, a diagnosis of type 2 diabetes, and persons with visceral fat area measured using visceral fat CT scanning. We excluded type 1 diabetes characterized by C-peptide levels below 0.3 ng/mL, a history of diabetic ketoacidosis, and other secondary causes of diabetes mellitus like corticosteroid. During the investigation, standardized questionnaires were used to obtain a medical history and lifestyle behavior information. Data were obtained on the duration of diabetes, alcohol consumption, cigarette smoking, and other health-related variables. The study protocol was approved by the Internal Review Board of St. Mary's Hospital (SC11RASI0100).
Study of anthropometry
Body weight and height were measured with the participants wearing light clothing and barefoot, and the measurements were used to calculate the body mass index (BMI). Waist circumference was measured to the nearest 0.1 cm at the narrowest point between the lower limit of the ribcage and the iliac crest [17]. Blood pressure was measured using a mercury sphygmomanometer with the participants in a seated position after a 5-minute rest. A subject was classified hypertensive if the systolic blood pressure (SBP) was ≥140 mm Hg, or the diastolic blood pressure (DBP) was ≥90 mm Hg, or if the subject had been diagnosed with hypertension previously and was taking antihypertensive medications.
Study of diabetic complications
The presence of retinopathy was identified via ophthalmoscopy by a trained ophthalmologist after pupillary dilatation. The eye evaluation and analysis of the photographs for the entire group were performed by an experienced ophthalmologist who was blinded to this study. Based on this examination, retinopathy was classified as either absent or present. The albumin-creatinine ratio was calculated for first-voided spot urine sample. The presence of diabetic nephropathy was defined as microalbuminuria (30 to 300 mg/g creatinine) or overt proteinuria (>300 mg/g creatinine). Diabetic peripheral neuropathy was assessed using the Michigan Neuropathy Screening Instrument, a validated instrument to identify symptoms and signs of clinically evident neuropathy. The presence of diabetic neuropathy was defined as a score over 2.0 on the Michigan Neuropathy Screening Instrument [18].
Biochemical measurements
A venous blood sample was obtained in the morning after an overnight fast. Hemoglobin A1c (HbA1c) level was measured using high-performance liquid chromatography (HLC-723 G7; Tosoh Co., Tokyo, Japan). Fasting plasma glucose concentration was measured in sodium fluoride tubes using the hexokinase method. Serum insulin concentration was measured using an enzyme-linked immunosorbent assay, and the homeostatic model assessment of insulin resistance values (HOMA-IR) was calculated from fasting glucose and fasting C-peptide values using the HOMA2 calculator (http://www.dtu.ox.ac.uk).
Evaluation of visceral obesity
A visceral fat CT scan (General Electric Medical Systems, Milwaukee, WI, USA) at the L4-5 level was performed to measure the cross-sectional area of total abdominal fat, visceral abdominal fat, and subcutaneous abdominal fat according to previously described methods [19].
Cardiovascular autonomic function test
To improve the reproducibility and accuracy of CAN test and to reduce bias, a single experienced expert who was blinded to the study conducted CAN test. Additively we stopped medications that interfere in CAN results such as diuretics, antihistamines, and beta-blockers during preceding 2 days.
Parasympathetic functions were analyzed based on the heart rate response to deep breathing, a Valsalva maneuver, and postural change. Sympathetic function was assessed by measuring the blood pressure response to orthostatic change. The beat-to-beat variability in heart rate during respiration was calculated as the maximum heart rate divided by minimum heart rate according to age-normative data [20]. The heart rate response to standing was assessed by the ratio of the 15th R-R interval to the 30th R-R interval (below 1.00; as abnormal) [20]. The heart rate response to the Valsalva maneuver was evaluated by the ratio of the longest R-R interval to the shortest R-R interval during expiration at 40 mm Hg for 15 seconds with the pressure set using a sphygmomanometer (below 1.10; as abnormal) [20]. Orthostatic hypotension was defined as a decrease in SBP of ≥20 mm Hg during standing [21]. We used the diagnostic criteria for CAN suggested by the recent international ADA consensus [5], which states that the presence of one abnormal cardiovagal test identifies possible or early CAN; at least two abnormal heart rate tests are required for a definite or confirmed diagnosis of CAN; and orthostatic hypotension, in addition to heart rate test abnormalities, identifies severe or advanced CAN.
Statistical analysis
The differences between genders were analyzed by the two-sample t-test or chi-test, as appropriate. The correlation between visceral fat area and metabolic parameters according to gender was analyzed by Spearman's rank correlation analysis. The t-test and chi-test were done for evaluation of cardiovascular reflex test outcomes according to visceral fat area. Univariate linear regression analysis was used to estimate the association between visceral fat area and the cardiovascular reflex test outcome. To exclude the confounding effects of BMI, we adjusted BMI by using multiple regression analysis. A P value of less than 0.05 was considered significant. All values are presented as mean±standard deviation or number (%). Analyses were performed with SAS version 9.1 for Windows (SAS Institute Inc., Cary, NC, USA).
RESULTS
Baseline characteristics of the participants
Table1 presents the charateristics according to gender groups. The mean age, BMI, and duration of diabetes were 60±14 years, 25.1±4.2 kg/m2, and 12.3±8.9 years. The mean value of visceral fat area (VFA) in this study was 133.7±61.9 cm2 and women had higher VFA than men, but there was no significant difference (women, 136.7±65.1 cm2 vs. men, 129.1±56.6 cm2; P=NS). TFA and SFA were significantly higher in women than men. Male patients in this group were younger (56.3±14.1 years old vs. 62.4±13.4 years old, P=0.0019) and had higher triglyceride levels than women (2.2±2.2 mmol/L vs. 1.7±1.1 mmol/L, P=0.023), a higher percentage smoked (50% vs. 3.3%, P<0.0001), and consumed alcohol (40.8% vs. 8.2%, P<0.0001). The prevalence of diabetic complications including CAN, previous history of hypertension, cerebrovascular disease, and cardiovascular disease was not different between genders. Because the two dimensional parameters of fat area using visceral fat CT were different between men and women, further analysis was performed separately.

Baseline characteristics of the participants
Correlation between VFA and metabolic parameters according to gender
VFA showed positive correlation with age, BMI, waist circumference, and other two dimensional fat areas in both genders (Table 2). In analyzing the relationship with parameters of glycemic control, hemoglobin A1c showed a negative correlation with VFA in both genders (r=-0.234, P=0.035 in men; r=-0.175, P=0.047 in women) but fasting glucose was not significantly correlated with VFA. Lipid profile did not have definite relation in men, but in women, VFA had a statically significant and positive relationship with triglyceride (r=0.460, P<0.001) and had a negative relationship with high density lipoprotein (r=-0.301, P=0.001). Fasting serum C-peptide (r=0.369, P<0.001) and calculating homeostasis model assessment of insulin resistance from using fasting glucose and fasting C-peptide (r=0.325, P=0.001) showed a positive relationship in women only.
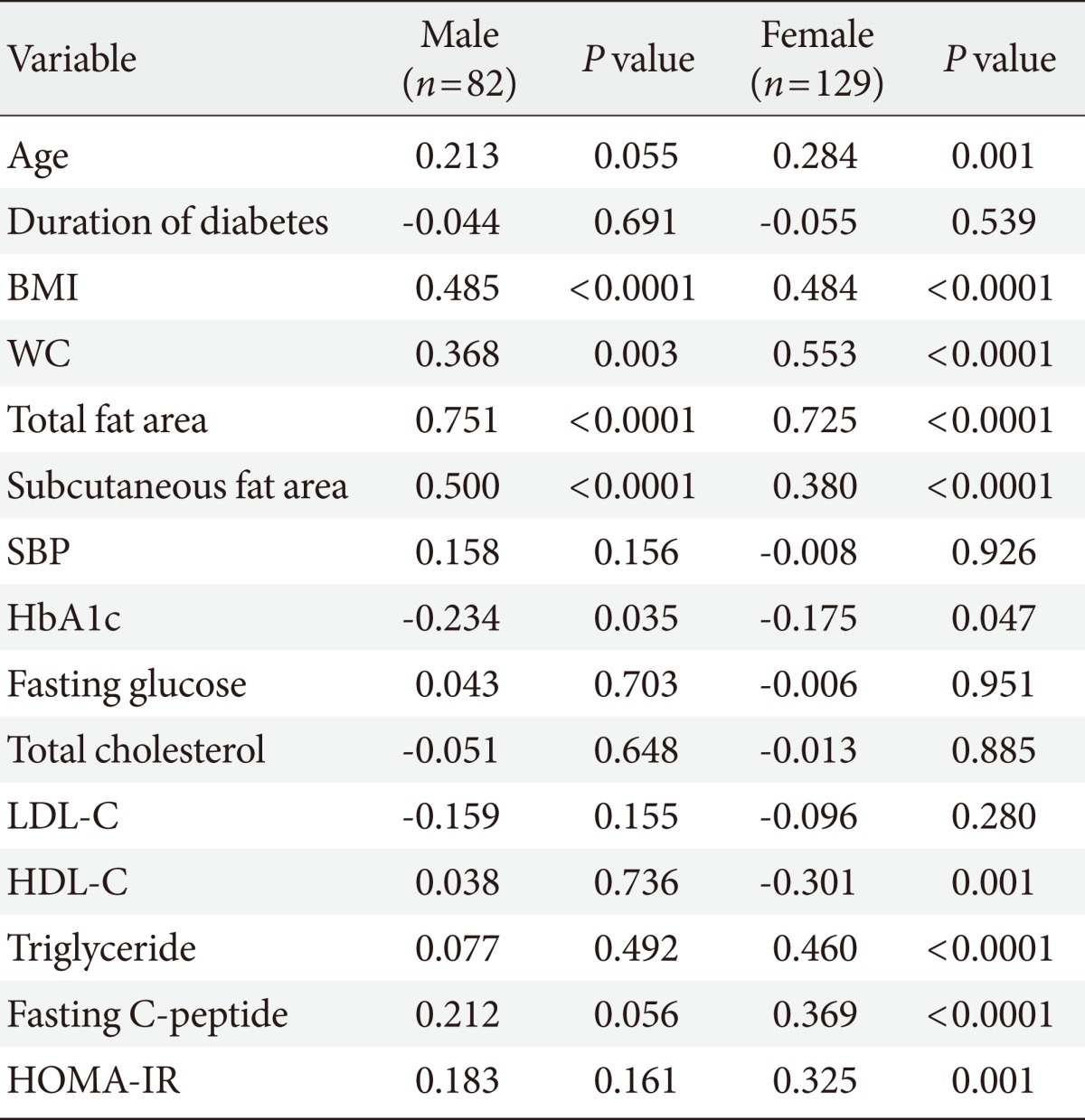
Correlation analysis between visceral fat area and metabolic parameters in type 2 diabetes mellitus
Comparison of results of cardiovascular reflex test according to gender
The prevalence of early CAN in the total study group was 48.3%, definite CAN plus severe CAN was 30.3% (Table 3). There was no significant difference in prevalence of cardiovascular reflex test between genders. However, women showed a slightly higher proportion of abnormality in heart rate response to Valsalva maneuver and prevalence of definite plus severe CAN (35.3% vs. 37.2%, P=NS; 41.8% vs. 12.1%, P=NS).
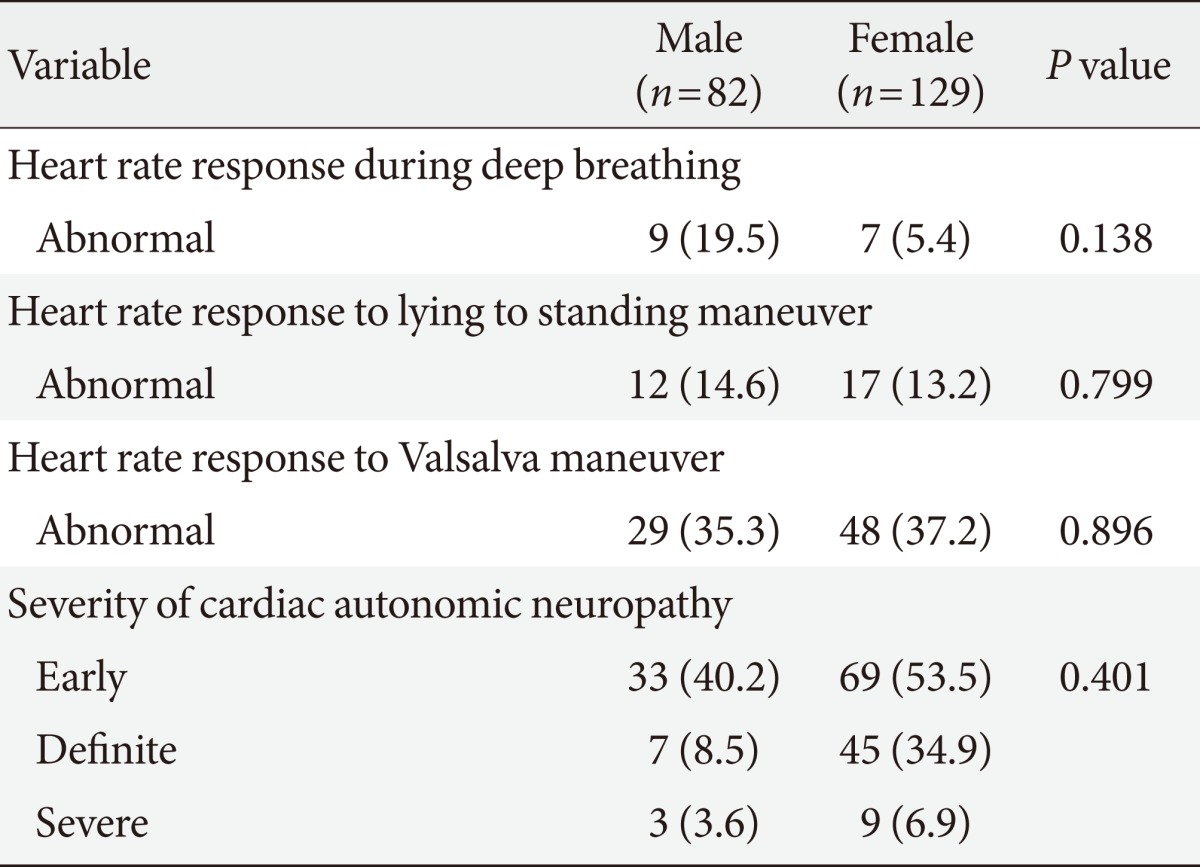
Comparison of cardiovascular reflex tests outcome according to gender
Association of VFA with the each parameter of cardiovascular reflex test by univariate linear regression model and multiple regression model
Fig. 1 shows the comparisons of absolute results in cardiovascular reflex tests according to VFA [22]. Heart rate response to Valsalva maneuver in women was the only test with a statistical difference according to VFA (1.28 vs. 1.19, P=0.01). Table 4 shows no definite association was observed between VFA and parameters of cardiovascular reflex test in men, whether correcting for other parameters or not. But in women, univariate linear regression analysis showed that increased VFA diminished good heart rate responses to Valsalva maneuver (R2=4.9%, P=0.013 in unadjusted model). After adjusting age and BMI as compounding factors to interrupt CAN, the relationship between VFA and heart rate response to Valsalva maneuver was intensified in women only (R2=9.8%, P=0.0072).

Comparison of cardiovascular reflex tests outcome according to visceral fat area (VFA). (A) Male (n=82). (B) Female (n=129).
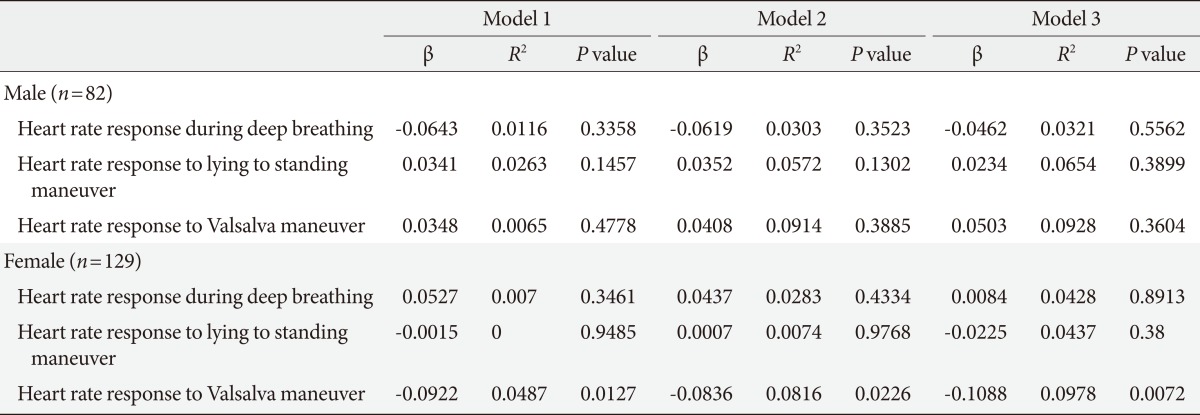
Association of visceral fat area with the results of cardiovascular reflex test by univariate linear regression and multiple regression analysis
DISCUSSION
This study showed a linear relationship between VFA measured using visceral fat CT scanning and cardiovascular reflex test to measure CAN among patients with type 2 diabetes mellitus.
Previous studies demonstrated the association between obesity and CAN in patients with diabetes because of common pathogenic links such as insulin resistance and dyslipidemia [23-26]. Matsuzawa et al. [23] proposed a link between visceral fat accumulation and metabolic and circulatory disorders. Thus, mesenteric fat showed more lipogenic activity than did subcutaneous fat [23]. As a result, it releases free fatty acids more easily into hepatic portal circulation, leading to insulin resistance, hyperlipidemia, glucose intolerance and ultimately to atherosclerosis. Kreier et al. [26], in a study on rats, suggested that parasympathetic innervation to intra-abdominal adipose tissue might mediate intra-abdominal obesity levels by stimulating glucose and free fatty acid uptake directly. The Finnish Diabetes Prevention Study on subjects with impaired glucose tolerance showed elevated levels of triglycerides and increased hypertension. In particular, central obesity according to waist circumference was associated with parasympathetic dysfunction [11]. Voulgari et al. [24] reported an independent relationship between CAN and multiple correctable parameters such as poor glycemic control, hypertension, hypertriglyceridemia, and waist circumference from a total of 600 patients (200 with type 1 diabetes and 400 with type 2). Thus, it is possible that unbalanced autonomic function might be the pathogenic link between visceral obesity and CAN in diabetic patients, according to expert opinions [26]. Central obesity is measured using clinical parameters such as waist circumference or waist-to-hip ratio, but these do not reflect visceral adiposity directly. Thus, more direct and accurate imaging methods need to be applied to measure visceral adiposity, such as CT or magnetic resonance imaging scans of visceral fat. In addition, because the prevalence of metabolically obese and normal weight was higher in Korea than other Western countries that the utility of visceral fat CT to estimate visceral adiposity might be more important [27].
Our study showed a positive correlation between the clinical parameters of waist circumference or BMI and VFA, but no definite association between waist circumference or BMI and parameters of cardiovascular reflex tests (data not shown). Table 4 shows that, after adjusting for confounding factors such as the BMI, there remained an association between VFA and heart rate response to Valsalva maneuver. Therefore, the strength of this study is that it investigated the relationship between visceral obesity using objective CT scanning and showed the clinical effects of visceral obesity on CAN, which was analyzed separately from central obesity.
The association between VFA and CAN in patients with type 2 diabetes showed a gender difference in this study. Some reports have discussed the role of gender-specific factors in the pathogenesis of CAN [26,28,29]. Epidemiologic studies have highlighted the role of smoking, blood pressure, and dyslipidemia in the development of CAN [28], and modifiable lifestyle factors, such as smoking and alcohol consumption, have been suggested as a cause of the gender difference [26]. According to Yufu et al. [29], women have a more depressed baroreflex sensitivity than men among patients with type 2 diabetes. Our study showed the significantly different life styles between genders in Table 1, but no difference in outcome of cardiovascular reflex tests, as shown in Table 3 and Fig. 1. Therefore, larger, well-validated studies are needed to establish the nature and cause of gender differences.
Our study showed a linear correlation between VFA and heart rate in response to a Valsalva maneuver; other parameters of cardiovascular reflex tests failed to show any significant association. We could not explain the exact reason for the relation, but according to May and Arildsen [30], the heart rate response to a Valsalva maneuver was an independent predictor of long-term survival among patients with diabetes between 40 and 75 years, and it may be a valid minimum test to use when screening for CAN.
There were some limitations to our study. First the participants had poor glycemic control (mean HbA1c, 9.8%), a long duration of diabetes (mean, 12.3 years), and a high prevalence of diabetic complications. Therefore, they were not representative of all patients with diabetes. However, compared with previous reports we demonstrated a similar correlation between VFA and other metabolic parameters such as BMI and triglyceride [14-16]. Second, this was a cross-sectional study so it was insufficient to clarify causal relationships without adjusting for other confounding factors during statistical analysis. We believe a larger cohort or prospective study is needed to fully explain the causal relationship between visceral adiposity and CAN.
In conclusion, we show that VFA is an independent negative factor for predicting the heart rate response to Valsalva maneuver among women with type 2 diabetes mellitus after adjusting for age and BMI. Thus, patients with visceral adiposity might need earlier tests of cardiovascular reflexes to detect CAN.
ACKNOWLEDGMENTS
The authors thank Seo Jung Hong for assistance in preparing the manuscript and Kyung Do Han for his effort in statistical analysis.
Notes
No potential conflict of interest relevant to this article was reported.