
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 47(6); 2023 > Article
-
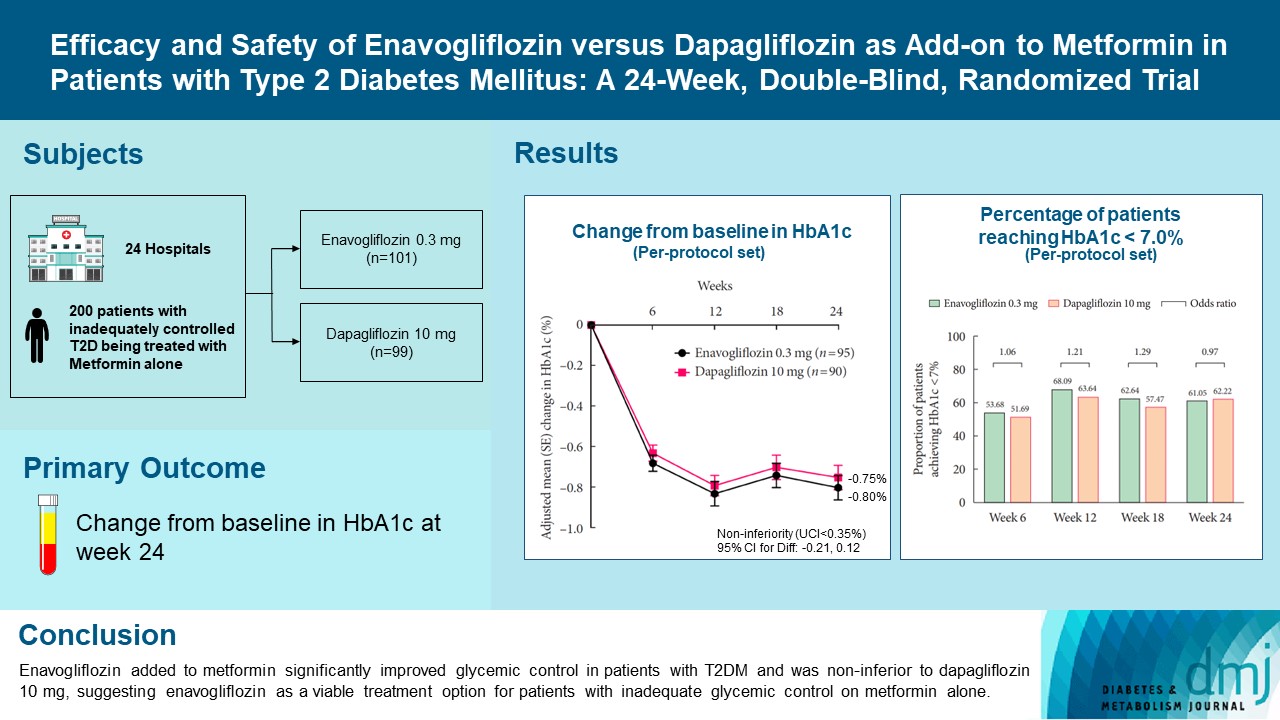
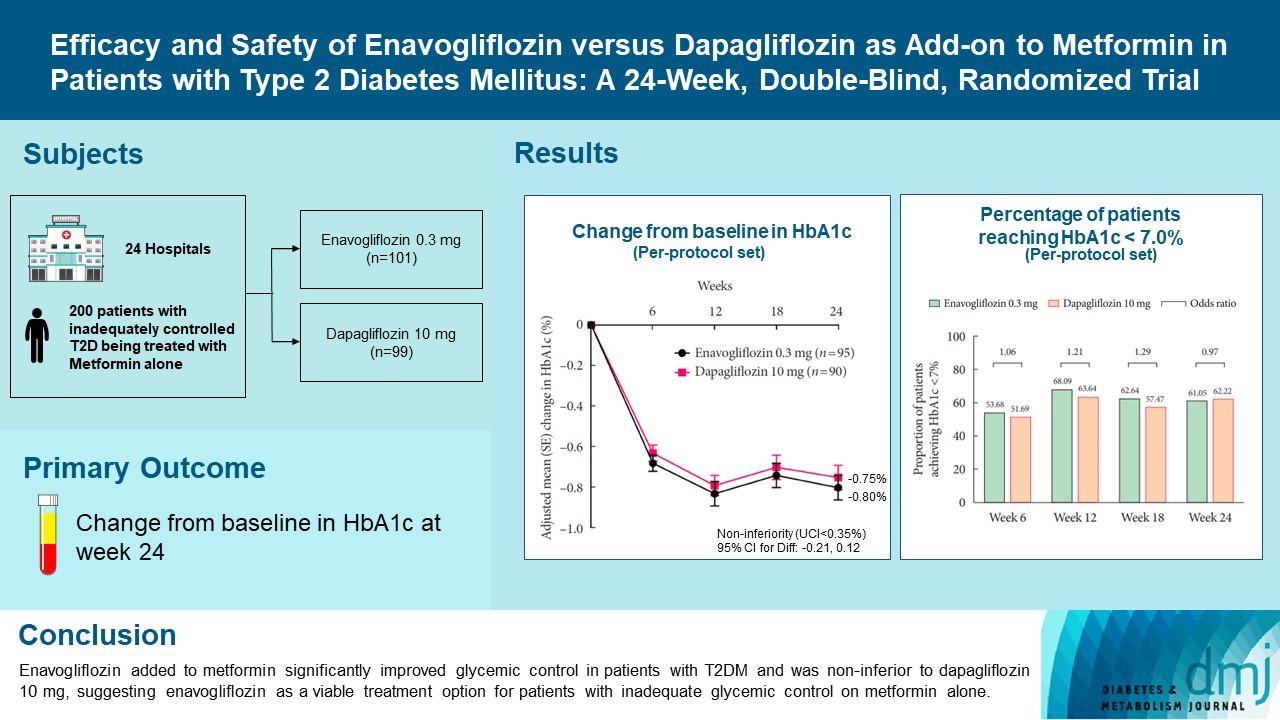
Original ArticleDrug/Regimen Efficacy and Safety of Enavogliflozin versus Dapagliflozin as Add-on to Metformin in Patients with Type 2 Diabetes Mellitus: A 24-Week, Double-Blind, Randomized Trial
-
Kyung Ah Han1
 , Yong Hyun Kim2, Doo Man Kim3, Byung Wan Lee4, Suk Chon5, Tae Seo Sohn6, In Kyung Jeong7, Eun-Gyoung Hong8, Jang Won Son9, Jae Jin Nah10, Hwa Rang Song10, Seong In Cho10, Seung-Ah Cho10, Kun Ho Yoon11
, Yong Hyun Kim2, Doo Man Kim3, Byung Wan Lee4, Suk Chon5, Tae Seo Sohn6, In Kyung Jeong7, Eun-Gyoung Hong8, Jang Won Son9, Jae Jin Nah10, Hwa Rang Song10, Seong In Cho10, Seung-Ah Cho10, Kun Ho Yoon11 -
Diabetes & Metabolism Journal 2023;47(6):796-807.
DOI: https://doi.org/10.4093/dmj.2022.0315
Published online: February 9, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University, Seoul, Korea
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Bundang Jesaeng Hospital, Seongnam, Korea
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Seoul, Korea
4Division of Endocrinology and Metabolism, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Kyung Hee University Hospital, Seoul, Korea
6Division of Endocrinology and Metabolism, Department of Internal Medicine, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
7Division of Endocrinology and Metabolism, Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Korea
8Division of Endocrinology and Metabolism, Department of Internal Medicine, Hallym University Dongtan Sacred Heart Hospital, Hwaseong, Korea
9Division of Endocrinology and Metabolism, Department of Internal Medicine, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea
10Clinical Development Center, Daewoong Pharmaceutical Co. Ltd., Seoul, Korea
11Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
-
Corresponding author: Kun Ho Yoon Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea E-mail: yoonk@catholic.ac.kr
Copyright © 2023 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Enavogliflozin is a novel sodium-glucose cotransporter-2 inhibitor currently under clinical development. This study evaluated the efficacy and safety of enavogliflozin as an add-on to metformin in Korean patients with type 2 diabetes mellitus (T2DM) against dapagliflozin.
-
Methods
- In this multicenter, double-blind, randomized, phase 3 study, 200 patients were randomized to receive enavogliflozin 0.3 mg/day (n=101) or dapagliflozin 10 mg/day (n=99) in addition to ongoing metformin therapy for 24 weeks. The primary objective of the study was to prove the non-inferiority of enavogliflozin to dapagliflozin in glycosylated hemoglobin (HbA1c) change at week 24 (non-inferiority margin of 0.35%) (Clinical trial registration number: NCT04634500).
-
Results
- Adjusted mean change of HbA1c at week 24 was –0.80% with enavogliflozin and –0.75% with dapagliflozin (difference, –0.04%; 95% confidence interval, –0.21% to 0.12%). Percentages of patients achieving HbA1c <7.0% were 61% and 62%, respectively. Adjusted mean change of fasting plasma glucose at week 24 was –32.53 and –29.14 mg/dL. An increase in urine glucose-creatinine ratio (60.48 vs. 44.94, P<0.0001) and decrease in homeostasis model assessment of insulin resistance (–1.85 vs. –1.31, P=0.0041) were significantly greater with enavogliflozin than dapagliflozin at week 24. Beneficial effects of enavogliflozin on body weight (–3.77 kg vs. –3.58 kg) and blood pressure (systolic/diastolic, –5.93/–5.41 mm Hg vs. –6.57/–4.26 mm Hg) were comparable with those of dapagliflozin, and both drugs were safe and well-tolerated.
-
Conclusion
- Enavogliflozin added to metformin significantly improved glycemic control in patients with T2DM and was non-inferior to dapagliflozin 10 mg, suggesting enavogliflozin as a viable treatment option for patients with inadequate glycemic control on metformin alone.
- Type 2 diabetes mellitus (T2DM) is a major chronic metabolic disorder posing a risk of cardiovascular disease, renal failure, and retinopathy, with the number of newly diagnosed cases estimated at more than 460 million annually and steadily increasing prevalence [1]. The preferred first-line therapy in patients with T2DM is metformin [2]. Several other therapies are available as add-on treatments for those who do not respond adequately to metformin alone, including sulfonylureas, thiazolidinedione, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon like peptide-1 receptor agonists, and sodium-glucose cotransporter 2 (SGLT-2) inhibitors [3,4].
- SGLT-2 inhibitors selectively and reversibly inhibit SGLT-2 transporters in the proximal convoluted tubule, preventing the renal reabsorption of glucose, with a resultant increase in its urinary excretion [5]. The glucose-lowering effects of SGLT-2 inhibitors, whether in monotherapy or in combination with other agents, are well-established [5]. Those drugs act independently of insulin function and, aside from improving glycemic control in patients with T2DM, were also shown to exert a cardioprotective effect and to promote weight loss [6-10].
- Enavogliflozin is a novel SGLT-2 selective inhibitor that is currently under clinical development stage. Pharmacokinetic, pharmacodynamic and safety profiles of enavogliflozin were analyzed in vitro and in healthy volunteers [11-13]. In a randomized controlled trial (RCT) in healthy volunteers, enavogliflozin induced glucosuria in a dose-dependent manner, and the steady state urinary glucose excretion was 50 to 60 g/day after multiple doses in the range of 0.3 to 2.0 mg. The drug was rapidly absorbed with the time to peak plasma concentration of 1.0 to 3.0 hours and a mean elimination half-life of 13 to 29 hours. The systemic exposure to enavogliflozin increased proportionally with multiple-dose administrations in the range of 0.1 to 2.0 mg. The drug was well-tolerated in single oral doses of up to 5.0 mg and multiple oral doses of up to 2.0 mg [13]. The efficacy and safety of enavogliflozin were later demonstrated in another RCT involving Korean patients with T2DM. In that study, using enavogliflozin monotherapy at 0.1, 0.3, and 0.5 mg, a significant reduction in glycosylated hemoglobin (HbA1c) was observed at week 12, by 0.74%, 0.86%, and 0.84%, respectively [14].
- The aim of the present 24-week RCT was to verify the efficacy and safety of enavogliflozin 0.3 mg as an add-on to metformin in Korean patients with T2DM against dapagliflozin 10 mg, another SGLT-2 inhibitor, as an active comparator.
INTRODUCTION
- Ethics statement
- This study was conducted according to the principles of the Helsinki declaration and good clinical practice and approved by the Ministry of Food and Drug Safety in Korea and the Institutional Review Board (IRB) of each hospital. The list of IRBs and IRB approval numbers are provided in Supplementary Table 1. Written informed consent was obtained from all participants before any study-related procedure was initiated. The study was prospectively registered on ClinicalTrials.gov (identifier: NCT04634500).
- Study design and study population
- This was a multicenter, double-blind, randomized study conducted in 24 hospitals in South Korea to evaluate the efficacy and safety of enavogliflozin 0.3 mg compared with dapagliflozin 10 mg in patients with T2DM receiving metformin therapy. Patients with inadequate glycemic control (HbA1c 7.0% to 10.5%) after at least 8 weeks of stable-dose metformin monotherapy (≥1,000 mg/day) were considered for screening. Patients treated with a combination of metformin and other antihyperglycemic agent(s) whose HbA1c had been between 6.5% and 10.0% could be screened as well if HbA1c levels were within the eligible range (7.0% to 10.5%) after at least 8 weeks of washout from antihyperglycemic agent(s) other than metformin. Other eligibility criteria were as follows: age between 19 and 80 years, body mass index (BMI) between 20 and 45 kg/m2, and fasting plasma glucose (FPG) <270 mg/dL. Patients with any of the following condition(s) were excluded from the study: severe heart failure, defined as New York Heart Association classes III to IV; systolic blood pressure >180 mm Hg or diastolic blood pressure >110 mm Hg; estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2; aspartate aminotransferase or alanine aminotransferase >three times the upper limit of normal; or other clinically significant conditions (Supplementary Table 2). Also, the use of a systemic corticosteroid (2 weeks before screening) and/or an antihyperglycemic agent other than metformin (8 weeks before screening) and/or weight reduction medication (12 weeks before screening) were the reasons for exclusion.
- Eligible patients underwent the single-blinded (patient-only blinded) run-in phase for 2 weeks, during which they took two placebo tablets (placebo enavogliflozin, placebo dapagliflozin) orally once a day, in addition to the ongoing metformin treatment. If the run-in phase compliance was 70% to 130% and the reassessed HbA1c was 7.0% to 10.5%, the patient was randomly assigned to the enavogliflozin or dapagliflozin group at a 1:1 ratio. Stratified block randomization was done centrally via an interactive web response system. Stratification factors included previous (24 weeks before screening) treatment for T2DM (metformin monotherapy vs. combination of two or more drugs, including metformin) and HbA1c level at screening (≥8% vs. <8%). Each randomized patient took two tablets (randomized drug, placebo of another drug) orally once a day for 24 weeks. Metformin treatment was continued without a change in dose, dosing frequency, or product type (immediate-release vs. extended-release). Other antihyperglycemic agents, glucagon or glucose injection, weight reduction medications, iodized contrast media, or drugs that may interact with study drugs or metformin, such as organic cation transporter-1 (OCT-1) inhibitors or OCT-2 inhibitors, were prohibited during the study. Patients were asked to keep following the prescribed diet and exercise routine, to record medication information of metformin on the diary provided, and to bring back any unused study drugs in the original bottle. Post-randomization visits were made every 6 weeks (6, 12, 18, and 24 weeks) for efficacy and safety assessments.
- Efficacy and safety assessments
- Changes from baseline (randomization) in major glycemic parameters, i.e., HbA1c and FPG, were included as efficacy endpoints. The primary endpoint was HbA1c change at week 24. Percentages of patients reaching HbA1c <7.0% and of patients achieving therapeutic glycemic response, defined as HbA1c reduction >0.5% or HbA1c level <7.0%, were also evaluated. As exploratory efficacy endpoints, changes from baseline in body weight, urine albumin-creatinine ratio (UACR), urine glucose-creatinine ratio (UGCR), homeostasis model assessment of β-cell function (HOMA-β) and homeostasis model assessment of insulin resistance (HOMA-IR), fasting lipid profile, adiponectin, and leptin were included. Blood samples were collected after at least 8-hour of fasting and prior to taking the study drug on the day of the visit. For the calculation of UACR and UGCR, a spot random urine sample was collected. All biological samples (blood and urine samples) for efficacy parameters were sent to a central laboratory for analysis. For safety assessment, treatment-emergent adverse events (TEAEs) were collected. Particular interest was given to monitoring the occurrence of hypoglycemia, urinary tract infection (UTI), genital infection, polyuria, and pollakiuria. Complete blood count, serum chemistry, and pregnancy test (only for women of childbearing potential) were done at all visits. A 12-lead electrocardiogram was done once or twice (if washout was needed) before the run-in phase and repeated at week 24/last visit.
- Statistical analysis
- A sample size of 71 per group was calculated to provide 80% of power at one-sided significance level of 2.5% for the non-inferiority test on the primary endpoint, assuming the non-inferiority margin of 0.35%, the true mean difference of 0%, and the standard deviation of 0.74%. Considering a drop-out rate of 25%, a total of 190 patients were targeted to be randomized (95 per group). The non-inferiority margin was based on the margins suggested in the regulatory guidelines on the clinical trial of diabetes and those used in the clinical trials of other SGLT-2 inhibitors [15-19].
- Changes from baseline in efficacy endpoints were compared between the groups using analysis of covariance (ANCOVA) with baseline values and randomization stratification factors as covariates. For HbA1c change at week 24, if the upper bound of the 95% confidence interval (CI) for least square mean difference (enavogliflozin–dapagliflozin) was less than the predefined margin of 0.35%, non-inferiority of enavogliflozin to dapagliflozin was to be declared. For changes in HbA1c and FPG, sensitivity and subgroup analyses were carried out to test robustness of the main findings. The sensitivity analyses were performed using a mixed effect model for repeated measures that used groups, visits, baseline values, randomization stratification factors, and interaction between the group and visit as fixed effects. Preplanned subgroup analyses included subgroups according to stratification factors and eGFR (<90 or ≥90 mL/min/1.73 m2) at screening. As ad hoc analyses, HbA1c and UACR changes in a subgroup of patients with moderately or severely increased albuminuria (baseline UACR ≥30 mg/g) were analyzed (n=18 in enavogliflozin group, n=22 in dapagliflozin group). To test between-group difference in the percentages of patients achieving the target HbA1c, the odds ratio and its 95% CI were calculated using logistic regression analysis with a randomization stratification factor as the covariate. Continuous variables were presented with descriptive statistics, and group difference was tested using a two-sample t-test or Wilcoxon’s rank sum test. Categorical variables were summarized with the frequency (%), and group difference was tested using the chi-square test or Fisher’s exact test. Definitions of analysis sets are presented in Supplementary Table 3. For efficacy endpoints analyzed with ANCOVA, changes from baseline are presented with adjusted mean change. Except for the non-inferiority test for the primary endpoint, all statistical tests were two-sided at a significance level of 5%. Statistical analyses were performed using the SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Adverse events were coded using MedDRA version 24.0 (MedDRA, Herndon, VA, USA).
METHODS
- Participant disposition and characteristics
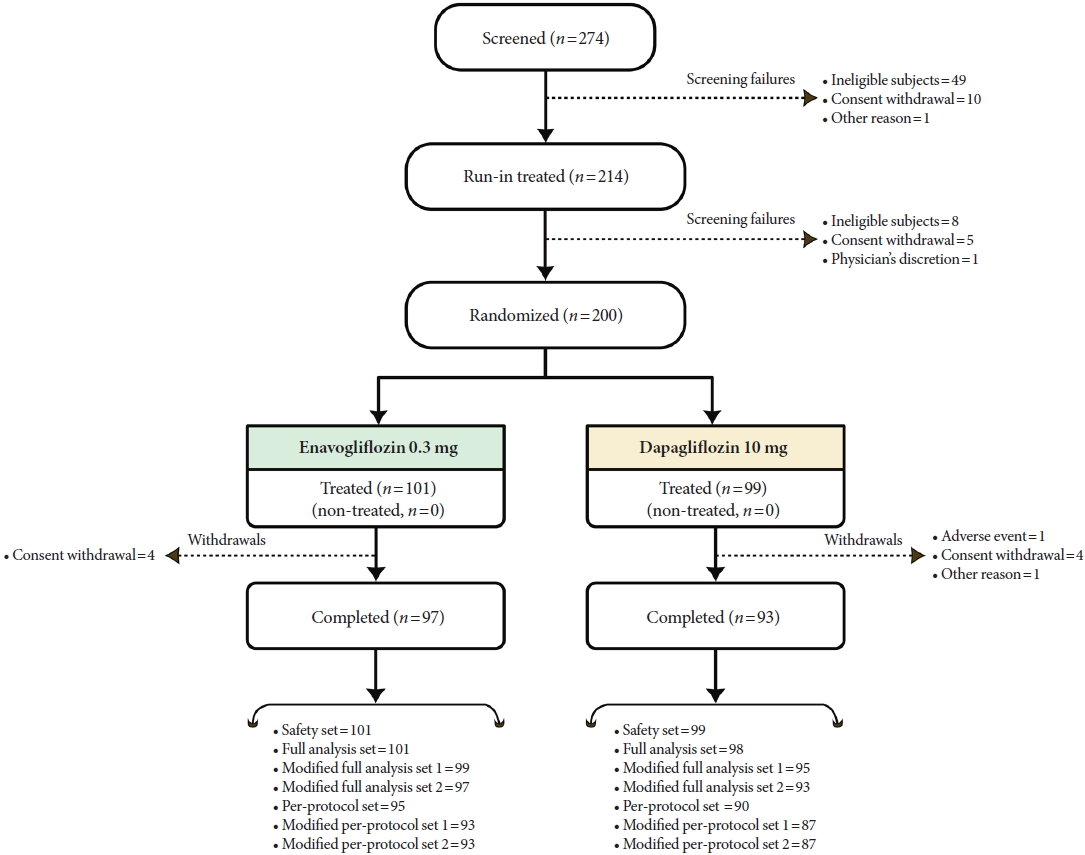
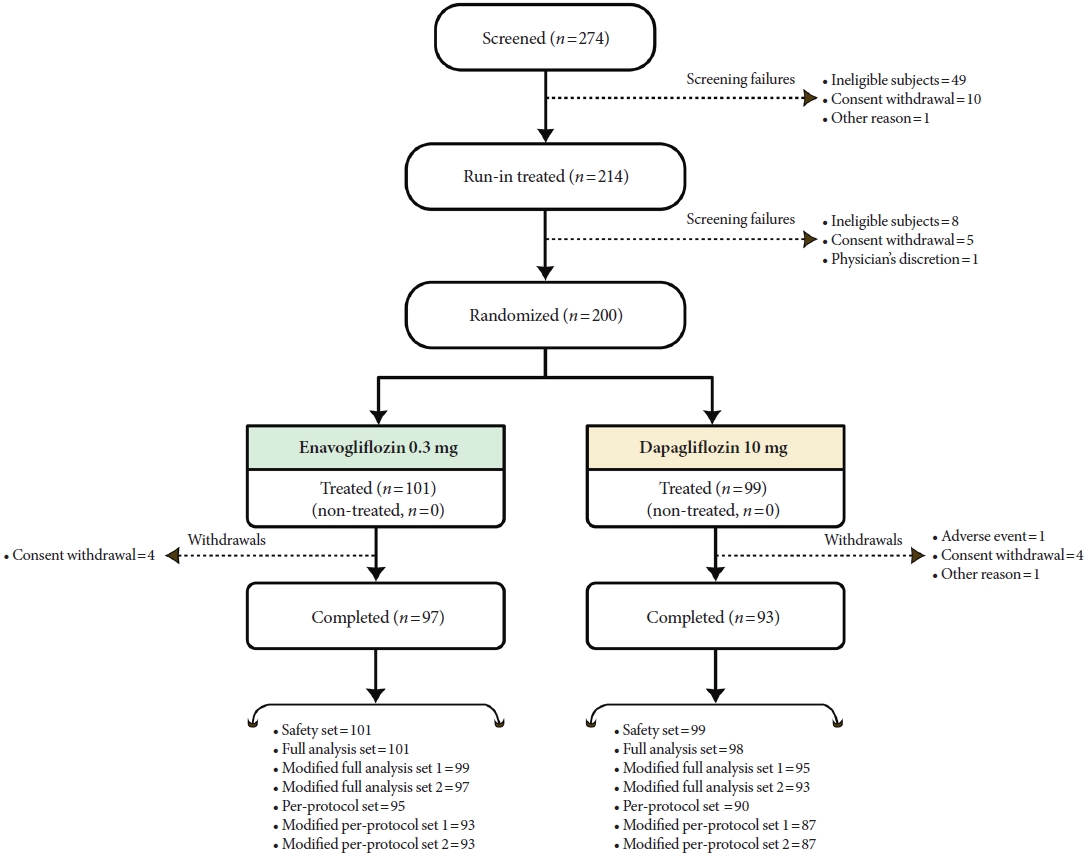
- Between 2 December 2020 and 3 November 2022, a total of 274 patients were screened, 200 were randomized (enavogliflozin group=101, dapagliflozin group=99), and 190 completed the study (enavogliflozin group=97, dapagliflozin group= 93). The number and the reasons for screening failures and early withdrawals from the study are presented in Fig. 1. Demographic and baseline characteristics were comparable between the groups (Table 1). Age ranged from 20 to 79 years (mean age, 59 years in enavogliflozin group, 60 years in dapagliflozin group) with a mean duration of diabetes of 8.9 and 8.2 years, respectively. The mean BMI in both groups was 26 kg/m2, which is higher than the cutoff of obesity (25 kg/m2) in the Asian-Pacific population [20]. In both groups, 31% of patients had HbA1c ≥8.0% at screening. Compared with dapagliflozin group, enavogliflozin group had lower mean eGFR (88.06 mL/min/1.73 m2 vs. 94.72 mL/min/1.73 m2, P=0.0161) and higher proportion of patients with eGFR <90 mL/min/1.73 m2 (60% vs. 46%, P=0.0483) at screening. However, the difference was attenuated after run-in phase and between-group difference at baseline was not statistically significant (mean eGFR: 88.04 mL/min/1.73 m2 vs. 94.00 mL/min/1.73 m2, P=0.0610; proportion of patients with eGFR <90 mL/min/1.73 m2: 59% vs. 53%, P=0.2878). Forty-two percent of patients in the enavogliflozin group and 40% in the dapagliflozin group have been treated with the combination of metformin and other antidiabetic agent(s); among them, DPP-4 inhibitors were the most common add-on drug to metformin (51%[enavogliflozin], 49%[dapagliflozin]) followed by SGLT-2 inhibitors (32%[enavogliflozin], 31%[dapagliflozin]). Metabolism and nutrition disorders are the most common concurrent diseases (85%[enavogliflozin], 91%[dapagliflozin]), mostly diagnosed with dyslipidemia or hyperlipidemia. Vascular disorders were also commonly accompanied by: hypertension or essential hypertension in 50% in the enavogliflozin group, 52% in the dapagliflozin group, and arteriosclerosis in 34% and 36% in each group.
- Exposure to the treatment and compliance
- In the enavogliflozin group, the means of treatment compliance of enavogliflozin and dapagliflozin placebo were 98.36% and 98.48%, respectively. In the dapagliflozin group, the means of treatment compliance of dapagliflozin and enavogliflozin placebo were 98.50% and 98.51%, respectively. Mean compliance to metformin treatment in both groups was also similar (99.06% vs. 99.10%), with a median daily dose of 1,275 and 1,264 mg, respectively.
- Efficacy
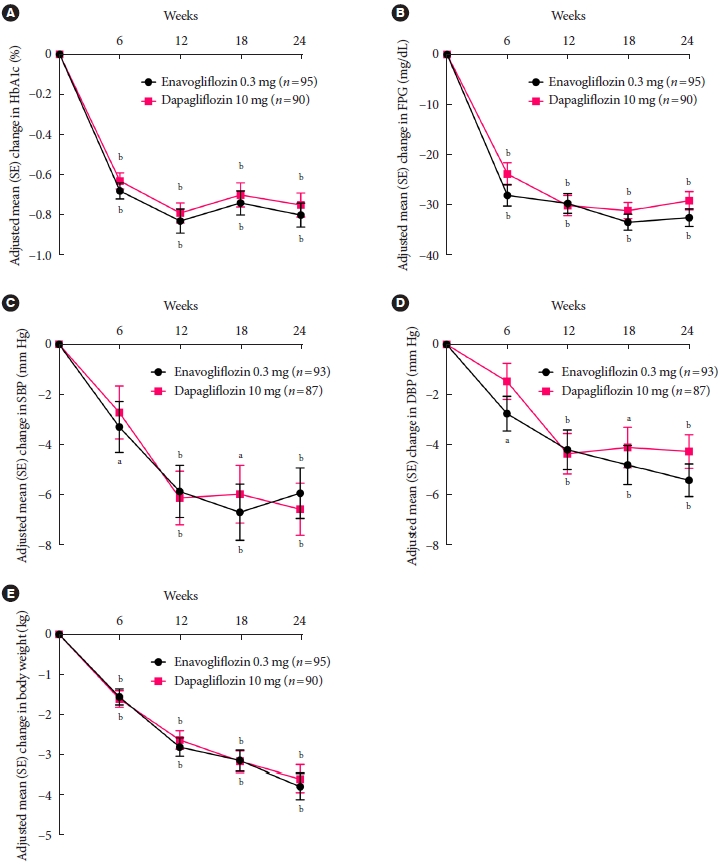
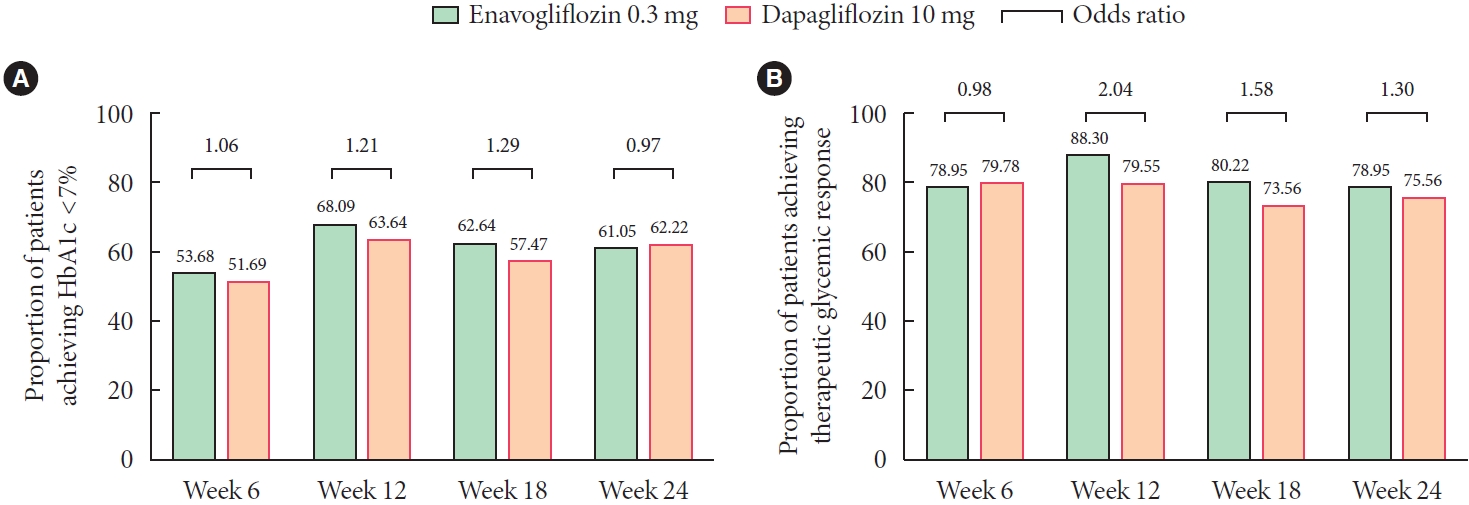
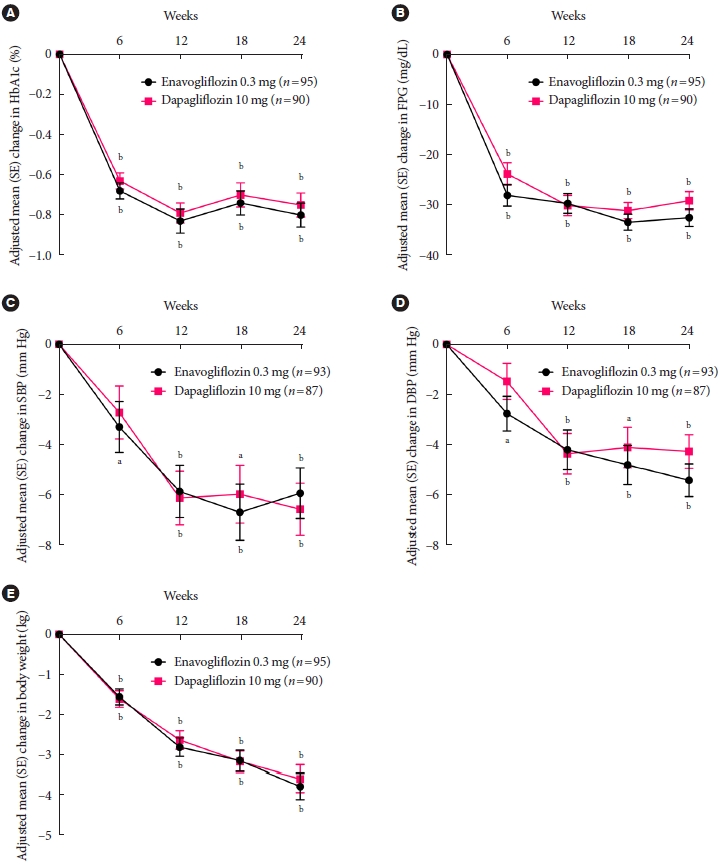
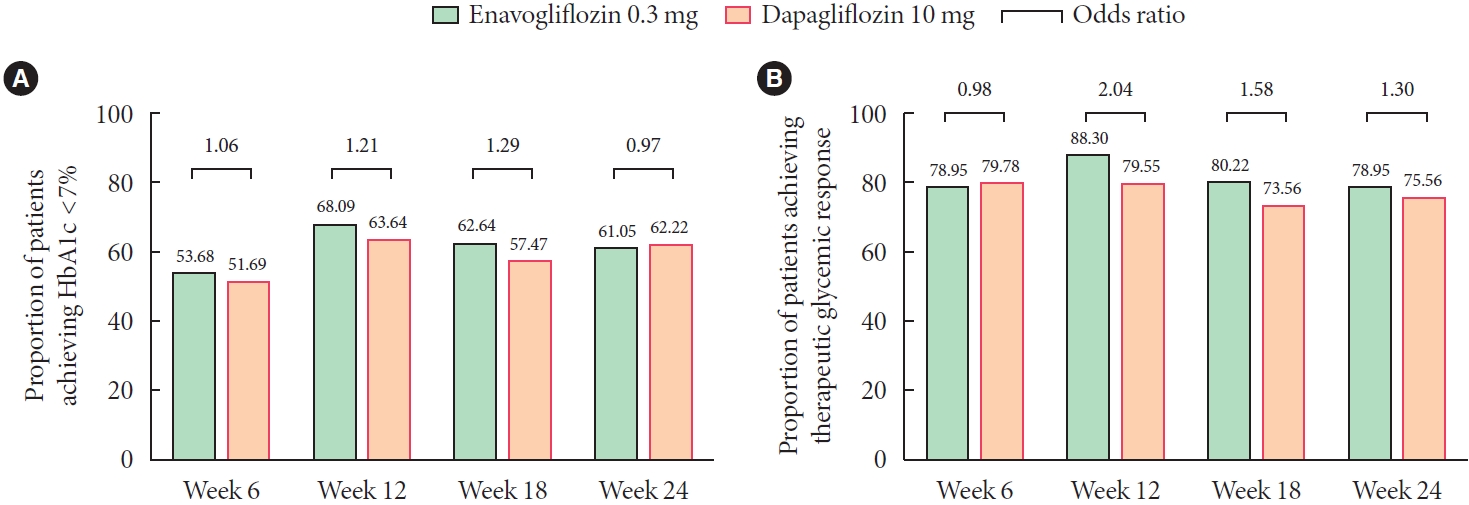
- Major efficacy results are summarized in Table 2. HbA1c significantly decreased in both groups at week 6 (P<0.0001), further decreased till week 12, and the level was maintained till week 24 (Fig. 2). The level of HbA1c reduction at week 24 was similar between the groups (–0.80%[enavogliflozin] vs. –0.75%[dapagliflozin]), and the 95% CI of the between-group difference (–0.21% to 0.12%) did not cross the prespecified non-inferiority margin (0.35%), proving the non-inferiority of enavogliflozin to dapagliflozin. Similar HbA1c reduction was observed in a subgroup of patients with eGFR <90 mL/min/1.73 m2 (–0.80%[enavogliflozin] vs. –0.72%[dapagliflozin], P= 0.4357) at screening and in a subgroup of patients with moderately/severely increased albuminuria (–0.69% in both groups, P=0.9707) (Supplementary Table 4). Aside from the significant reduction in HbA1c, a substantial proportion of patients reached the target HbA1c in both groups (Fig. 3.) The level of FPG reduction at week 24 was also similar between the groups (–32.53 mg/dL[enavogliflozin] vs. –29.14 mg/dL[dapagliflozin], P=0.1633). Sensitivity analyses also showed no significant between-group difference in HbA1c and FPG changes at week 24, both with per-protocol set and full-analysis set. No significant between-group difference was found in either HbA1c or FPG changes for the preplanned subgroups except in a subgroup of patients with baseline HbA1c ≥8%, where enavogliflozin showed better FPG reduction than dapagliflozin at week 24 (–47.45 mg/dL vs. –38.03 mg/dL, P=0.0256) (Supplementary Table 4 and 5). Significant (P<0.0001) body weight reduction trend was continuous throughout the study in both groups (Fig. 2).
- In both groups, UACR started significantly decreasing from week 12 and the reduction trend was maintained till week 24 (–24.29 mg/g[enavogliflozin] vs. –17.37 mg/g[dapagliflozin], P=0.1399). The significant reduction in UACR at week 24 from baseline was also confirmed in a subgroup of patients with moderately/severely increased albuminuria (–122.21 mg/g vs. –83.80 mg/g, P=0.0529) (Supplementary Table 6). Meanwhile, UGCR significantly increased from week 6 and increased urinary glucose excretion was observed till week 24 in both groups (60.48 g/g [enavogliflozin] vs. 44.94 g/g[dapagliflozin], P<0.0001). The level of UGCR increase was significantly greater with enavogliflozin than dapagliflozin at all assessment points (P<0.0001). A significant increase in HOMA-β was observed from week 6 (enavogliflozin group) or week 12 (dapagliflozin group), and the change at week 24 was comparable between the groups (6.94[enavogliflozin] vs. 11.93[dapagliflozin], P=0.2545). Meanwhile, HOMA-IR decreased significantly (P<0.0001) in both groups at week 6, and the level of reduction at week 24 was significantly greater in the enavogliflozin group than in the dapagliflozin group (–1.85 vs. –1.31; difference, –0.53; 95% CI, –0.90 to –0.17; P=0.0041).
- Blood pressure (systolic/diastolic) gradually decreased with time, and the reductions at week 24 were statistically significant (P<0.0001) in both groups (–5.93/–5.41 mm Hg[enavogliflozin] vs. –6.57/–4.26 mm Hg[dapagliflozin]).
- Plasma adiponectin significantly increased at week 6 (0.92 mg/L[enavogliflozin] vs. 0.80 mg/L[dapagliflozin], P=0.7474) and further degree of increase was observed at week 24 (1.67 mg/L[enavogliflozin] vs. 1.69 mg/L[dapagliflozin], P=0.9688). Leptin, on the other hand, significantly decreased at week 6 (–2.43 µg/L[enavogliflozin] vs. –1.62 µg/L[dapagliflozin], P=0.2035) and the level was maintained till week 24 (–2.40 µg/L[enavogliflozin] vs. –1.28 µg/L[dapagliflozin], P= 0.1151). No significant between-group differences were detected in the lipid profile (Supplementary Table 7).
- Safety
- The incidence of TEAEs was similar between the groups (24% [enavogliflozin] vs. 22%[dapagliflozin], P=0.7958). Most of the events were mild in intensity (35 out of 36 events in the enavogliflozin group, 30 out of 34 events in the dapagliflozin group) and did not affect the intended treatment. Four adverse events of special interest occurred, one (cystitis) in the enavogliflozin group and three (cystitis, hypoglycemia, and pollakiuria) in the dapagliflozin group. None of the three serious adverse events (mechanical ileus in the enavogliflozin group, prostate cancer and benign prostatic hyperplasia in the dapagliflozin group) were assessed to be drug-related. Adverse drug reactions (ADRs) occurred more frequently in the dapagliflozin group (1.0% vs. 7.1%, P=0.0341); however, all ADRs in both groups were mild or moderate in intensity and within the known profile of side effects of the drug class (Table 3). No ADRs led to drug discontinuation or fatality. No medically significant changes were found in the laboratory results and electrocardiogram.
RESULTS
- This 24-week, double-blind, randomized trial demonstrated that enavogliflozin 0.3 mg, a novel SGLT-2 inhibitor, was noninferior to dapagliflozin 10 mg in terms of efficacy and safety in Korean patients with T2DM inadequately controlled with metformin. No significant differences were found between enavogliflozin and dapagliflozin groups in terms of glycemic control, body weight, and blood pressure reduction. Additionally, enavogliflozin provided a greater increase in UGCR and better HOMA-IR reduction than dapagliflozin. The therapeutic implications of those findings have been addressed in detail below.
- At week 24, the increase in UGCR was significantly greater in the enavogliflozin group than in the dapagliflozin group (adjusted mean change: 60.48 g/g vs. 44.94 g/g). This observation is consistent with the results of previous studies of enavogliflozin pharmacokinetics. In an in vitro study comparing the novel molecule with currently used SGLT-2 inhibitors [11], among them dapagliflozin, the value of the lowest half-maximal inhibitory concentration (IC50) of enavogliflozin to SGLT-2 was half of the IC50 for dapagliflozin (0.8±03 nM vs. 1.6± 0.3 nM). Additionally, enavogliflozin showed higher kidney distribution than dapagliflozin and had longer t1/2 in the kidney than that agent. Finally, the kidney concentration of enavogliflozin was maintained over 72 hours after oral administration at 1 mg/kg [11]. Those findings were later confirmed in a recently published randomized double-blind, placebo-and active-controlled, single- and multiple-dose study of healthy volunteers [13]. In that study, a dose-dependent increase in urinary glucose excretion was observed after a single dose of enavogliflozin, and the steady state urinary glucose excretion was 50 to 60 g/day after multiple doses in the dose range of 0.3 to 2.0 mg [13]. Taken altogether, the results of the present study and the findings mentioned above imply that the effect of enavogliflozin on urinary glucose excretion is more potent than that of dapagliflozin, even at a much lower dose of 0.3 mg/day used in the present study.
- In the present study, enavogliflozin 0.3 mg was shown to be non-inferior to dapagliflozin 10 mg in terms of mean reductions in HbA1c at week 24, with a mean reduction of –0.80% and –0.75% for enavogliflozin group and dapagliflozin group, respectively. The robustness of the HbA1c reduction effect of enavogliflozin was verified both in sensitivity and subgroup analyses. Although this study was not powered to investigate the efficacy in patients with renal failure, the effect of enavogliflozin on HbA1c reduction in patients with mildly decreased renal function in terms of eGFR is worth emphasizing, given that at the baseline, more than half of the patients had eGFR <90 mL/min/1.73 m2 (59%[enavogliflozin], 53%[dapagliflozin]). A similar result was also consistently confirmed in a small subgroup of patients with moderately/severely increased albuminuria. The mean reduction in HbA1c in the dapagliflozin group was similar to that reported in previous trials of this agent. In a randomized, double-blind placebo-controlled study involving exclusively Asian patients, predominantly from China (86%) [21], the mean reduction in HbA1c at week 24 in patients treated with dapagliflozin 10 mg as an add-on to metformin was –0.85%. Also, in a similarly designed study conducted in a predominantly Western population [22], the mean change in HbA1c at week 24 was within a similar range as described above, –0.84% for dapagliflozin 10 mg.
- Aside from the reduction in HbA1c, a substantial proportion of patients participating in the present study, 61% in the enavogliflozin group and 62% in the dapagliflozin group, achieved HbA1c <7.0% at week 24, and the percentages of patients achieving a therapeutic glycemic response in the two groups were 79% and 76%, respectively. Finally, the mean change from baseline in FPG at week 24 was –32.53 mg/dL in the enavogliflozin group and –29.14 mg/dL in the dapagliflozin group, with no significant between-group difference in this parameter. Considering those findings, as well as the previously mentioned observation that enavogliflozin had a more profound pharmacokinetic effect on urinary glucose excretion, the efficacy of the new molecule in terms of glycemic control seems to be at least similar to that of dapagliflozin. Further, given the results of previous studies documenting the lack of meaningful differences in glycemic control after dapagliflozin in Asian and Western patients [23-26], enavogliflozin is also likely to show a similar efficacy regardless of patient ethnicity.
- Both enavogliflozin and dapagliflozin contributed to a modest, similar degree decrease in body weight, with adjusted mean change at week 24 of –3.77 and –3.58 kg in the enavogliflozin group and dapagliflozin group, respectively. Given that even a modest-degree decrease in body weight is an established contributor to improved glycemic control [27], and considering the fact that glucose-lowering agents whose mechanism of action depends on insulin secretion or insulin activity are frequently associated with weight gain [23], the weight-lowering effect of enavogliflozin constitutes an added benefit in patients with T2DM.
- Also, other beneficial effects of enavogliflozin documented in the present study are worth emphasizing, namely, a significant increase in HOMA-β and a significant decrease in HOMA-IR (adjusted mean changes at week 24: 6.9 and –1.9, respectively). Importantly, in the case of HOMA-IR, enavogliflozin contributed to a more evident decrease than dapagliflozin 10 mg. Previous studies demonstrated that, lowering plasma glucose concentration through enhanced glucosuria, dapagliflozin significantly improved insulin sensitivity in skeletal muscles in patients with T2DM and ameliorated pancreatic β-cell glucose toxicity [28-30]. In line with those findings, a more evident improvement in insulin resistance observed in the present study in the enavogliflozin group might have been associated with a significantly greater increase in UGCR found in patients treated with the novel agent.
- Both enavogliflozin and dapagliflozin contributed to a modest albeit significant decrease in blood pressure at week 24, –5.93/–5.41 mm Hg and –6.57/–4.26 mm Hg in the enavogliflozin group and dapagliflozin group, respectively. Moreover, both drugs resulted in a significant reduction in albuminuria in the overall population at week 24, by 24.29 and 17.37 mg/g in the enavogliflozin group and dapagliflozin group, respectively. In particular, in the subgroup with moderately/severely increased albuminuria, the level of reduction was more prominent in the enavogliflozin group (–122.21 mg/g vs. –83.80 mg/g, P=0.0529) considering that 95% CI for the group difference (–77.31 to 0.51 mg/g) was more stretched to the side favoring enavogliflozin. This observation, along with the improvement in glycemic control, body weight reduction and favorable changes in blood pressure, implies that enavogliflozin might reduce cardiovascular risk in patients with T2DM. The cardioprotective effect of dapagliflozin in Asian and Western patients has already been confirmed in a large clinical trial Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction 58 (DECLARE TIMI–58) [10].
- This study had high retention rates, with 97/101 patients from the enavogliflozin group and 93/99 patients from the dapagliflozin group completing the trial. Only one episode of hypoglycemia was recorded in the dapagliflozin group, which is consistent with the mechanism of action of both drugs, independent of insulin action. Also, UTI rates were low, with single cases of cystitis observed in each group. The low UTI rate is worth emphasizing, given that the risk of developing urinary tract and genital infections is generally increased in patients with T2DM [31,32], and administration of SGLT-2 inhibitors poses an additional risk, especially for genital infections [33-35]. While ADRs occurred more frequently in the dapagliflozin group (1.0% vs. 7.1%, P=0.0341), all were mild or moderate in intensity and within the known profile of side effects of the drug class, and none of them led to drug discontinuation or fatality.
- One weakness of the present study is its short duration, which raises a question about the durability of the beneficial effects of enavogliflozin documented herein. This issue will be addressed ultimately after analyzing the results of the currently ongoing extension trial. However, in the case of pharmacokinetically and pharmacodynamically similar comparator, dapagliflozin, the results of some long-term studies conducted in Western populations demonstrated that the beneficial effects on glycemic control, body weight and blood pressure persisted for up to 4 years [34-38]. Aside from the high retention rates, the strengths of the present trial include high compliance with the study drug and the fact that the treatment groups were relatively well balanced in terms of demographic and baseline characteristics.
- In summary, the study showed that enavogliflozin added to metformin significantly improved glycemic control in Korean patients with T2DM. Additionally, the study drug contributed to beneficial changes in body weight, blood pressure, and albuminuria. The effects of enavogliflozin were non-inferior to those of dapagliflozin, and the novel molecule performed better than the latter in terms of urinary glucose excretion and insulin resistance improvement. The treatment was safe and well-tolerated. Taken altogether, these findings point to enavogliflozin as an attractive alternative for patients with inadequate glycemic control on metformin alone.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 4.
Supplementary Table 5.
Supplementary Table 6.
Supplementary Table 7.
-
CONFLICTS OF INTEREST
In-Kyung Jeong has been honorary editors of the Diabetes & Metabolism Journal since 2022. She was not involved in the review process of this article. Jae Jin Nah, Hwa Rang Song, Seong In Cho, and Seung-Ah Cho are full-time employees of Daewoong Pharmaceutical, Co. Ltd., the sponsoring company. Kyung Ah Han, Yong Hyun Kim, Doo Man Kim, Byung Wan Lee, Suk Chon, Tae Seo Sohn, In Kyung Jeong, Eun-Gyoung Hong, Jang Won Son, and Kun Ho Yoon declare that they have no competing interests.
-
AUTHOR CONTRIBUTIONS
Conception or design: K.A.H., K.H.Y.
Acquisition, analysis, or interpretation of data: K.A.H., Y.H.K., D.M.K., B.W.L., S.C., T.S.S., I.K.J., E.G.H., J.W.S., H.R.S., S.I.C., K.H.Y.
Drafting the work or revising: all authors.
Final approval of the manuscript: all authors.
-
FUNDING
The study was sponsored by Daewoong Pharmaceutical Co. Ltd. The sponsor participated in the study design, data management and analysis, and preparation of this manuscript.
NOTES
-
Acknowledgements
- None
| Characteristic | Enavogliflozin 0.3 mg (n=101) | Dapagliflozin 10 mg (n=99) |
|---|---|---|
| Age, yr | 59.03±11.45 | 60.35±10.62 |
| Male sex | 59 (58.42) | 54 (54.55) |
| Body weight, kg | 70.74±11.19 | 69.99±12.09 |
| Body mass index, kg/m2 | 26.45±3.30 | 26.20±3.48 |
| eGFR, mL/min/1.73 m2 | 88.06±15.72a | 94.72±18.75a |
| eGFR <90 mL/min/1.73 m2 | 61 (60.40)b | 46 (46.46)b |
| HbA1c, % | 7.82±0.74 | 7.81±0.74 |
| HbA1c ≥8% | 31 (30.69) | 31 (31.31) |
| FPG, mg/dL | 162.34±32.26 | 156.22±31.99 |
| Duration of diabetes, yr | 8.94±5.96 | 8.18±5.65 |
| Oral antidiabetic drugs | ||
| Metformin alone | 59 (58.42) | 59 (59.60) |
| Add-on therapy to metformin | 42 (41.58) | 40 (40.40) |
| Metformin dose, mg | 1,369.55±399.82 | 1,389.90±450.13 |
Values are presented as mean±standard deviation or number (%). Data were analyzed using the randomized set.
eGFR, estimated glomerular filtration rate; HbA1c, glycosylated hemoglobin; FPG, fasting plasma glucose.
a Statistically significant between-group difference (P=0.0161),
b Statistically significant between-group difference (P=0.0483).
| Variable | Enavogliflozin 0.3 mg (n=95) | Dapagliflozin 10 mg (n=90) | ||
|---|---|---|---|---|
| HbA1c, % | ||||
| Baseline | 7.75 (0.82) | 7.68 (0.73) | ||
| Week 24 | 6.98 (0.61) | 6.97 (0.72) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –0.80 (0.06) | –0.75 (0.06) | ||
| LS mean difference (95% CI) | –0.04 (–0.21 to 0.12) | |||
| FPG, mg/dL | ||||
| Baseline | 145.35 (26.60) | 149.33 (31.85) | ||
| Week 24 | 113.58 (17.21) | 117.91 (19.38) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –32.53 (1.76) | –29.14 (1.82) | ||
| LS mean difference (95% CI), P value | –3.38 (–8.15 to 1.39), P=0.1633 | |||
| Systolic blood pressure, mm Hg | ||||
| Baseline | 129.72 (13.64) | 127.44 (14.12) | ||
| Week 24 | 123.38 (12.55) | 121.40 (11.90) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –5.93 (1.01) | –6.57 (1.04) | ||
| LS mean difference (95% CI), P value | 0.63 (–2.13 to 3.39), P=0.6512 | |||
| Diastolic blood pressure, mm Hg | ||||
| Baseline | 77.04 (9.72) | 75.92 (10.50) | ||
| Week 24 | 71.65 (9.39) | 72.05 (8.44) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –5.41 (0.65) | –4.26 (0.67) | ||
| LS mean difference (95% CI), P value | –1.15 (–2.94 to 0.63), P=0.2044 | |||
| Body weight, kg | ||||
| Baseline | 70.17 (11.06) | 70.52 (11.81) | ||
| Week 24 | 66.39 (10.90) | 66.92 (11.89) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –3.77 (0.33) | –3.58 (0.34) | ||
| LS mean difference (95% CI), P value | –0.18 (–1.08 to 0.71), P=0.6840 | |||
| UACR, mg/g | ||||
| Baseline | 38.19 (163.98) | 57.42 (198.64) | ||
| Week 24 | 19.93 (29.10) | 31.37 (76.71) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –24.29 (3.38) | –17.37 (3.48)a | ||
| LS mean difference (95% CI), P value | –6.93 (–16.14 to 2.29), P=0.1399 | |||
| UGCR, g/g | ||||
| Baseline | 1.54 (8.70) | 1.83 (7.49) | ||
| Week 24 | 60.43 (20.76) | 45.27 (20.91) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | 60.48 (2.12) | 44.94 (2.18)a | ||
| LS mean difference (95% CI), P value | 15.54 (9.77 to 21.31), P<0.0001 | |||
| HOMA-β | ||||
| Baseline | 45.53 (36.34) | 44.44 (25.03) | ||
| Week 24 | 52.32 (40.75) | 56.67 (38.17) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | 6.94 (3.17) | 11.93 (3.25) | ||
| LS mean difference (95% CI), P value | –4.99 (–13.60 to 3.62), P=0.2545 | |||
| HOMA-IR | ||||
| Baseline | 3.45 (3.42) | 3.85 (2.49) | ||
| Week 24 | 1.76 (1.07) | 2.39 (1.67) | ||
| Change from baseline at week 24 | ||||
| LS mean (SE) | –1.85 (0.13) | –1.31 (0.14) | ||
| LS mean difference (95% CI), P value | –0.53 (–0.90 to –0.17), P=0.0041 | |||
Values are presented as the per-protocol set except blood pressure results which were presented with the modified per-protocol set 2.
HbA1c, glycosylated hemoglobin; SE, standard error; CI, confidence interval; FPG, fasting plasma glucose; UACR, urine albumin-creatinine ratio; UGCR, urine glucose-creatinine ratio; HOMA-β, homeostasis model assessment of β-cell function; HOMA-IR, homeostasis model assessment of insulin resistance.
a As one patient did not have baseline value, total 89 patients’ data were used for calculation of change from baseline.
| System organ class (preferred term) | Enavogliflozin 0.3 mg (n=101) | Dapagliflozin 10 mg (n=99) | |
|---|---|---|---|
| Patients with TEAEs | 24 (23.76) [36] | 22 (22.22) [34] | |
| Patients with ADRs | 1 (0.99) [1] | 7 (7.07) [7] | |
| Dyspepsia | 0 | 2 (2.02) [2]a[1],b[1] | |
| Cystitis | 1 (0.99) [1]a | 1 (1.01) [1]b | |
| Hypoglycemia | 0 | 1 (1.01) [1]a | |
| Pollakiuria | 0 | 1 (1.01) [1]a | |
| Vulvovaginal pruritus | 0 | 1 (1.01) [1]a | |
| Pruritus | 0 | 1 (1.01) [1]a | |
| Patients with SAEs | 1 (0.99) [1] | 1 (1.01) [2] | |
| Mechanical ileus | 1 (0.99) [1]c | 0 | |
| Benign prostatic hyperplasia | 0 | 1 (1.01) [1]c | |
| Prostate cancer | 0 | 1 (1.01) [1]c | |
Values are presented as number (%) [number of events]. Data were analyzed using the safety set.
TEAE, treatment-emergent adverse event; ADR, adverse drug reaction; SAE, serious adverse event.
a Adverse event of mild in intensity,
b Adverse event of moderate in intensity,
c Adverse event of severe in intensity.
- 1. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843.ArticlePubMed
- 2. Neumiller JJ, Umpierrez GE. 2018 Standards of care update: pharmacologic approaches to glycemic management in people with type 2 diabetes. Diabetes Spectr 2018;31:254-60.ArticlePubMedPMCPDF
- 3. Dash RP, Babu RJ, Srinivas NR. Comparative pharmacokinetics of three SGLT-2 inhibitors sergliflozin, remogliflozin and ertugliflozin: an overview. Xenobiotica 2017;47:1015-26.ArticlePubMed
- 4. Garcia-Ropero A, Badimon JJ, Santos-Gallego CG. The pharmacokinetics and pharmacodynamics of SGLT2 inhibitors for type 2 diabetes mellitus: the latest developments. Expert Opin Drug Metab Toxicol 2018;14:1287-302.ArticlePubMed
- 5. Sheu WH, Chan SP, Matawaran BJ, Deerochanawong C, Mithal A, Chan J, et al. Use of SGLT-2 inhibitors in patients with type 2 diabetes mellitus and abdominal obesity: an Asian perspective and expert recommendations. Diabetes Metab J 2020;44:11-32.ArticlePubMedPMCPDF
- 6. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 7. Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644-57.ArticlePubMed
- 8. Cai X, Yang W, Gao X, Chen Y, Zhou L, Zhang S, et al. The association between the dosage of SGLT2 inhibitor and weight reduction in type 2 diabetes patients: a meta-analysis. Obesity (Silver Spring) 2018;26:70-80.ArticlePubMedPDF
- 9. Gill HK, Kaur P, Mahendru S, Mithal A. Adverse effect profile and effectiveness of sodium glucose co-transporter 2 inhibitors (SGLT2i): a prospective real-world setting study. Indian J Endocrinol Metab 2019;23:50-5.ArticlePubMedPMC
- 10. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347-57.ArticlePubMed
- 11. Choi MK, Nam SJ, Ji HY, Park MJ, Choi JS, Song IS. Comparative pharmacokinetics and pharmacodynamics of a novel sodium-glucose cotransporter 2 inhibitor, DWP16001, with dapagliflozin and ipragliflozin. Pharmaceutics 2020;12:268.ArticlePubMedPMC
- 12. Kim JH, Kim DK, Choi WG, Ji HY, Choi JS, Song IS, et al. In vitro metabolism of DWP16001, a novel sodium-glucose cotransporter 2 inhibitor, in human and animal hepatocytes. Pharmaceutics 2020;12:865.ArticlePubMedPMC
- 13. Hwang JG, Lee S, Huh W, Han J, Oh J, Jang IJ, et al. Dose-dependent glucosuria of DWP16001, a novel selective sodiumglucose cotransporter-2 inhibitor, in healthy subjects. Br J Clin Pharmacol 2022;88:4100-10.ArticlePubMedPDF
- 14. Yang YS, Min KW, Park SO, Kim KS, Yu JM, Hong EG, et al. Efficacy and safety of monotherapy with enavogliflozin in Korean patients with type 2 diabetes mellitus: results of a 14 week, multi-center, randomized, double-blind, placebo-controlled, phase 2 trial. 2020 International Congress of Diabetes and Metabolism; 2020 Sep 18-19; Online. Available from: https:// icdm2020.diabetes.or.kr/program/oral_list.php.
- 15. Food and Drug Administration: Draft guidance for industry on diabetes mellitus. Developing drugs and therapeutic biologics for treatment and prevention: guidance document. Available from: https://www.regulations.gov/document/FDA-2008-D-0118-0003 (cited 2023 Feb 1).
- 16. European Medicines Agency: Clinical investigation of medicinal products in the treatment or prevention diabetes mellitus. Available from: https://www.ema.europa.eu/en/clinical-investigation-medicinal-products-treatment-prevention-diabetes-mellitus (cited 2023 Feb 1).
- 17. Nauck MA, Del Prato S, Meier JJ, Duran-Garcia S, Rohwedder K, Elze M, et al. Dapagliflozin versus glipizide as add-on therapy in patients with type 2 diabetes who have inadequate glycemic control with metformin: a randomized, 52-week, double-blind, active-controlled noninferiority trial. Diabetes Care 2011;34:2015-22.PubMedPMC
- 18. Henry RR, Murray AV, Marmolejo MH, Hennicken D, Ptaszynska A, List JF. Dapagliflozin, metformin XR, or both: initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. Int J Clin Pract 2012;66:446-56.ArticlePubMed
- 19. Dharmalingam M, Aravind SR, Thacker H, Paramesh S, Mohan B, Chawla M, et al. Efficacy and safety of remogliflozin etabonate, a new sodium glucose co-transporter-2 inhibitor, in patients with type 2 diabetes mellitus: a 24-week, randomized, double-blind, active-controlled trial. Drugs 2020;80:587-600.ArticlePubMedPMCPDF
- 20. World Health Organization. Regional Office for the Western Pacific. The Asia-Pacific perspective: redefining obesity and its treatment. Sydney: Health Communications Australia; 2000 [cited 2023 Feb 1]. Available from: https://apps.who.int/iris/handle/10665/206936.
- 21. Yang W, Han P, Min KW, Wang B, Mansfield T, T’Joen C, et al. Efficacy and safety of dapagliflozin in Asian patients with type 2 diabetes after metformin failure: a randomized controlled trial. J Diabetes 2016;8:796-808.ArticlePubMedPDF
- 22. Bailey CJ, Gross JL, Pieters A, Bastien A, List JF. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with metformin: a randomised, double-blind, placebo-controlled trial. Lancet 2010;375:2223-33.ArticlePubMed
- 23. Ferrannini E, Ramos SJ, Salsali A, Tang W, List JF. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care 2010;33:2217-24.PubMedPMC
- 24. Strojek K, Yoon KH, Hruba V, Elze M, Langkilde AM, Parikh S. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with glimepiride: a randomized, 24-week, double-blind, placebo-controlled trial. Diabetes Obes Metab 2011;13:928-38.ArticlePubMed
- 25. Rosenstock J, Vico M, Wei L, Salsali A, List JF. Effects of dapagliflozin, an SGLT2 inhibitor, on HbA(1c), body weight, and hypoglycemia risk in patients with type 2 diabetes inadequately controlled on pioglitazone monotherapy. Diabetes Care 2012;35:1473-8.ArticlePubMedPMCPDF
- 26. Kasichayanula S, Liu X, Lacreta F, Griffen SC, Boulton DW. Clinical pharmacokinetics and pharmacodynamics of dapagliflozin, a selective inhibitor of sodium-glucose co-transporter type 2. Clin Pharmacokinet 2014;53:17-27.ArticlePubMedPDF
- 27. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364-79.ArticlePubMedPMCPDF
- 28. Merovci A, Solis-Herrera C, Daniele G, Eldor R, Fiorentino TV, Tripathy D, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest 2014;124:509-14.ArticlePubMedPMC
- 29. Kaneto H, Obata A, Kimura T, Shimoda M, Kinoshita T, Matsuoka TA, et al. Unexpected pleiotropic effects of SGLT2 inhibitors: pearls and pitfalls of this novel antidiabetic class. Int J Mol Sci 2021;22:3062.ArticlePubMedPMC
- 30. Op den Kamp YJ, Gemmink A, de Ligt M, Dautzenberg B, Kornips E, Jorgensen JA, et al. Effects of SGLT2 inhibitor dapagliflozin in patients with type 2 diabetes on skeletal muscle cellular metabolism. Mol Metab 2022;66:101620.ArticlePubMedPMC
- 31. Chen SL, Jackson SL, Boyko EJ. Diabetes mellitus and urinary tract infection: epidemiology, pathogenesis and proposed studies in animal models. J Urol 2009;182(6 Suppl):S51-6.ArticlePubMed
- 32. Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 2003;26:510-3.ArticlePubMedPDF
- 33. Geerlings S, Fonseca V, Castro-Diaz D, List J, Parikh S. Genital and urinary tract infections in diabetes: impact of pharmacologically-induced glucosuria. Diabetes Res Clin Pract 2014;103:373-81.ArticlePubMed
- 34. Nauck MA, Del Prato S, Duran-Garcia S, Rohwedder K, Langkilde AM, Sugg J, et al. Durability of glycaemic efficacy over 2 years with dapagliflozin versus glipizide as add-on therapies in patients whose type 2 diabetes mellitus is inadequately controlled with metformin. Diabetes Obes Metab 2014;16:1111-20.ArticlePubMed
- 35. Bailey CJ, Morales Villegas EC, Woo V, Tang W, Ptaszynska A, List JF. Efficacy and safety of dapagliflozin monotherapy in people with type 2 diabetes: a randomized double-blind placebo-controlled 102-week trial. Diabet Med 2015;32:531-41.ArticlePubMedPDF
- 36. Wilding JP, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, et al. Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin: a randomized trial. Ann Intern Med 2012;156:405-15.ArticlePubMed
- 37. Bailey CJ, Gross JL, Hennicken D, Iqbal N, Mansfield TA, List JF. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, doubleblind, placebo-controlled 102-week trial. BMC Med 2013;11:43.ArticlePubMedPMCPDF
- 38. Nauck MA. Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. Drug Des Devel Ther 2014;8:1335-80.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Efficacy and safety of enavogliflozin vs. dapagliflozin as add-on therapy in patients with type 2 diabetes mellitus based on renal function: a pooled analysis of two randomized controlled trials
Young Sang Lyu, Sangmo Hong, Si Eun Lee, Bo Young Cho, Cheol-Young Park
Cardiovascular Diabetology.2024;[Epub] CrossRef - A 52‐week efficacy and safety study of enavogliflozin versus dapagliflozin as an add‐on to metformin in patients with type 2 diabetes mellitus: ENHANCE‐M extension study
Tae Seo Sohn, Kyung‐Ah Han, Yonghyun Kim, Byung‐Wan Lee, Suk Chon, In‐Kyung Jeong, Eun‐Gyoung Hong, Jang Won Son, JaeJin Na, Jae Min Cho, Seong In Cho, Wan Huh, Kun‐Ho Yoon
Diabetes, Obesity and Metabolism.2024;[Epub] CrossRef - The effect of renal function on the pharmacokinetics and pharmacodynamics of enavogliflozin, a potent and selective sodium‐glucose cotransporter‐2 inhibitor, in type 2 diabetes
Sae Im Jeong, Mu Seong Ban, Jun‐Gi Hwang, Min‐Kyu Park, Soo Lim, Sejoong Kim, Soon Kil Kwon, Yoonjin Kim, Jae Min Cho, Jae Jin Na, Wan Huh, Jae‐Yong Chung
Diabetes, Obesity and Metabolism.2024;[Epub] CrossRef - Role of novel sodium glucose co-transporter-2 inhibitor enavogliflozin in type-2 diabetes: A systematic review and meta-analysis
Deep Dutta, B.G. Harish, Beatrice Anne, Lakshmi Nagendra
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2023; 17(8): 102816. CrossRef - Characteristics of the Latest Therapeutic Agent for Diabetes
Nuri Yun
The Journal of Korean Diabetes.2023; 24(3): 148. CrossRef - Prospects of using sodium-glucose co-transporter-2 (SGLT-2) inhibitors in patients with metabolic-associated fatty liver disease (MAFLD)
Iryna Kostitska, Nadia Protas, Liliia Petrovska
Diabetes Obesity Metabolic Syndrome.2023; (5): 8. CrossRef - Navigating the Future of Diabetes Treatment with New Drugs: Focusing on the Possibilities and Prospects of Enavogliflozin
Sang Youl Rhee
Diabetes & Metabolism Journal.2023; 47(6): 769. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Efficacy and Safety of Evogliptin Add-on Therapy to Dapagliflozin/Metformin Combinations in Patients with Poorly Controlled Type 2 Diabetes Mellitus: A 24-Week Multicenter Randomized Placebo-Controlled Parallel-Design Phase-3 Trial with a 28-Week Extension
- Clinical and Lifestyle Determinants of Continuous Glucose Monitoring Metrics in Insulin-Treated Patients with Type 2 Diabetes Mellitus
- Safety of COVID-19 Vaccines among Patients with Type 2 Diabetes Mellitus: Real-World Data Analysis
- Comparison of Serum Ketone Levels and Cardiometabolic Efficacy of Dapagliflozin versus Sitagliptin among Insulin-Treated Chinese Patients with Type 2 Diabetes Mellitus
- Efficacy and Safety of Self-Titration Algorithms of Insulin Glargine 300 units/mL in Individuals with Uncontrolled Type 2 Diabetes Mellitus (The Korean TITRATION Study): A Randomized Controlled Trial



