- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 44(4); 2020 > Article
-
Brief ReportComplications Short-Term Walking Outcomes in Diabetic and Non-Diabetic Unilateral Transtibial Amputees
-
Dong Gyu Kwak1
 , Jeong-Yong Hur2, Jun Sung Moon3, Min Cheol Chang1
, Jeong-Yong Hur2, Jun Sung Moon3, Min Cheol Chang1 -
Diabetes & Metabolism Journal 2020;44(4):614-618.
DOI: https://doi.org/10.4093/dmj.2019.0080
Published online: November 4, 2019
- 4,125 Views
- 85 Download
1Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea.
2Shinsegae Prosthesis & Orthosis Center, Korea.
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea.
- Corresponding author: Jun Sung Moon. Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea. mjs7912@yu.ac.kr
- Corresponding author: Min Cheol Chang. Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea. wheel633@ynu.ac.kr
Copyright © 2020 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- This study compared short-term walking outcomes in diabetic amputees after prosthesis fitting compared to that in non-diabetic amputees. We retrospectively investigated walking outcomes at 3 months after starting gait training with a prosthesis. Forty-four unilateral transtibial amputees with (n=18) and without diabetes (n=26) were included. At 3 months after gait training with a prosthesis, only 2/18 (11.1%) and 3/18 (16.7%) diabetic amputees were capable of independent outdoor and indoor walking without cane, respectively. However, 21/26 (80.8%) and 24/26 (92.3%) non-diabetic amputees were capable of independent outdoor and indoor walking without cane, respectively. With assistance of cane, most of non-diabetic amputees (n=24, 92.3%) were capable of walking in both outdoor and indoor but only seven (38.9%) and nine (50.0%) diabetic amputees were capable, respectively. Thus, short-term walking outcome were poor in transtibial amputee with diabetes compare to those without diabetes, and these results suggest intensive rehabilitation would be needed to them.
- Transtibial amputation (TTA) is the most frequently performed lower limb amputation, and patients after TTA experience drastic changes in function and lifestyle. The recovery of walking ability is most important because quality of life after TTA is closely associated with mobility, and reduced walking ability with a prosthesis adversely affects daily living and social activities [1]. Previous studies have been reported that age, muscle strength, pain, contracture, amputation level, social support, motivation, and cognition have been associated with walking outcomes [2].
- Diabetes (or diabetic foot) is one of the most frequent causes of TTA, and the number of diabetic amputees has also rapidly increased [3]. People with diabetes may have muscle atrophy, slowing of muscle contraction, loss of muscle power and endurance, and sensory deficits [45], so these can contribute to impaired mobility. However, little is known about the influence of diabetes on walking ability after TTA.
- The current study compared short-term walking outcomes in diabetic amputees after prosthesis fitting compared to that in non-diabetic amputees.
INTRODUCTION
- Subjects
- This retrospective study enrolled 44 amputees who were transferred to the Department of Rehabilitation Medicine of Yeungnam University Hospital between January 2006 and January 2018, following unilateral TTA in the Department of Orthopedic Surgery, according to the following criteria: (1) unilateral TTA; (2) age 20 to 79 years; (3) received walking training with a prosthesis; (4) independent outdoor walking without assist prior to TTA; (5) absence of hip, knee, or ankle pain; (6) absence of severe cognitive impairment, as evidenced by a score of >24 points on the Mini-Mental Status Exam; and (7) absence of serious medical complications which require hospitalization during the study. A permanent prosthesis was fitted after use of a temporary prosthesis for 3 to 4 weeks. All amputees used a silicone sleeve, a silicone liner, a silicone suction suspension with vacuum valve, and a solid ankle cushion heel foot. Participants were diagnosed as having type 2 diabetes mellitus (T2DM) based on a previously documented diagnosis of T2DM or reported use of hypoglycemic agents. We collected current smoking, weight, height, Blood test data via medical record review and individualized questionnaires. The venous blood sampling was done after at least 8 hours of overnight fasting and analyzed at a certified laboratory at Yeungnam University Hospital. Written informed consent by the patients was waived due to a retrospective nature of our study. This study was approved by the Yeungnam University Hospital Institutional Review Board (2018-04-041).
- Walking ability
- All participants were assessed walking outcomes at 3 months after the start of walking training with a prosthesis. (1) Outdoor and indoor independent walking ability without cane was evaluated, (2) walking ability with a cane. The ability to walk 100 m without rest was considered acceptable. The time limit in walking 100 m was 10 minutes [6].
- Statistical analysis
- Data were analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The demographic data and walking outcomes of diabetic and non-diabetic amputees were compared using the Mann-Whitney U test and Fisher's exact test.
METHODS
- The study subjects were subdivided into diabetes (n=18) and non-diabetes (n=26) amputee groups. Whereas all amputees with diabetes had diabetic foot ulcer, non-diabetic amputation was performed for the following reasons: peripheral vascular disease (n=5), trauma (n=17), and cancer (n=2).
- Demographic data, including age, the postoperative time at which walking training was initiated, sex, and body mass index were not significantly different between the diabetic and non-diabetic amputees (P>0.05) (Table 1). The mean disease duration of the diabetic amputees was 25.3±12.1 years, and 55.6% of diabetes group was receiving renal replacement therapy
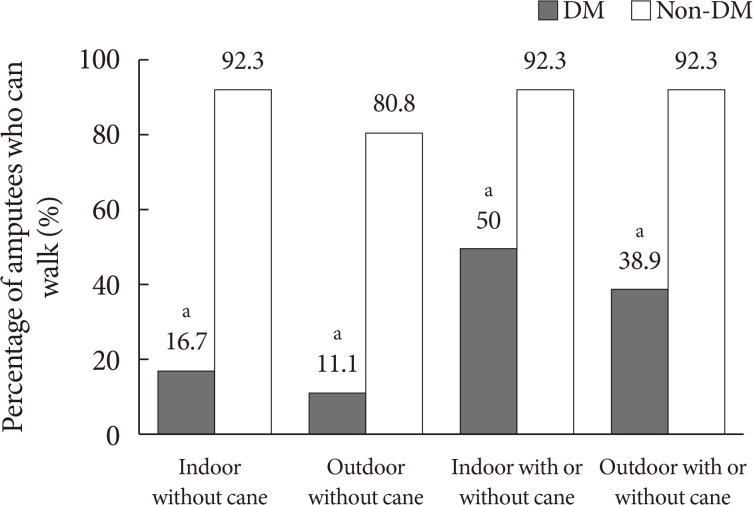
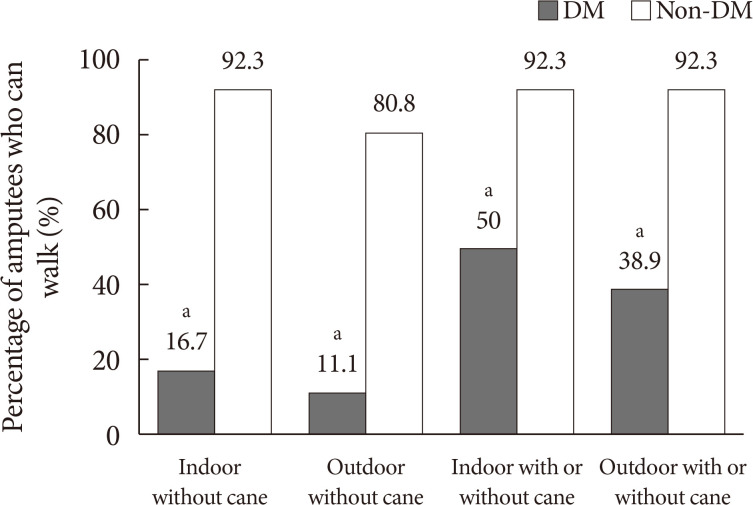
- At 3 months after training with a prosthesis, only two of 18 diabetic amputees (11.1%) were capable of independent outdoor walking without cane. However, 21 of 26 non-diabetic patients (80.8%) were capable of independent outdoor walking without cane (Fig. 1). While three diabetic amputees (16.7%) were capable of independent indoor walking without cane, 24 non-diabetic amputees (92.3%) were capable of indoor walking without cane. All patients capable of walking outdoor independently were capable of walking indoor independently. Therefore, with regards to independent outdoor and indoor walking without cane, amputees with diabetes showed significantly lower successful rates compared to those without diabetes (P<0.001).
- In regard to walking using a cane, five diabetic amputees (27.8%) should use a cane when walking outdoor, but only three patients (11.5%) required it in non-diabetics. Six amputees (33.3%) with diabetes could walk indoor under the assistance of a cane but none of non-diabetic amputees used a cane for indoor gait. Thus, at 3 months after rehabilitation training, 24 non-diabetic amputees (92.3%) were capable of walking regardless of the cane use, whereas only seven (38.9%) and nine (50.0%) diabetic amputees could walk at outdoor and indoor regardless of the cane use. Amputees who were capable of indoor and outdoor walking with a cane was significantly higher in patients with diabetes (P<0.001).
RESULTS
- In this study, we found that short term walking performance was significantly impaired in amputee with diabetes and most of them need the cane even they were capable of walking after prosthesis training.
- Previous studies reported walking rates with prostheses after lower limb amputation in the range of 50% to 90% [789]. Our study showed only 10% to 20% were able to walk at outdoor and indoor in patients with diabetes and it is quite low proportion compared with prior results. There are several reasons for this difference between the two groups. First, diabetes could reduce maximum muscle strength by approximately 30% to 50% in both the upper and lower leg [10]. In patients with diabetes, insulin resistance redounded consistent hyperglycemia and the severity of hyperglycemia was associated with decreased muscle strength, mass, and quality [11]. Perry and Schoneberger [12] reported that hip abductors, hip extensors, and knee extensors are key muscle groups used in walking. Weakness in hip abductors, hip extensors, and knee extensors in patients with diabetes is thought to cause difficulty in walking after TTA [13]. Second, distal symmetric polyneuropathy (DSPN) occurs in approximately 20% to 40% of all diabetic patients. DSPN occurs mainly in the distal lower extremities, and predominantly involves sensory nerve fibers [14]. Damage to large sensory fibers results in diminished proprioception, which can affect balance and postural control [15]. Poor walking outcomes in diabetic amputees may partly be attributed to deficits in proprioception. Lastly, several studies reported that patients with diabetes showed worse cognitive function compared with controls without diabetes [45]. Depression was more common in patients with diabetes [16]. Cognitive deficits and depressed mood are predictors of poor walking outcome in amputees after rehabilitation [17]. Although we did not assess cognitive dysfunction or depressed mood, those might have resulted in poor walking outcomes in diabetic amputees.
- To the best of our knowledge, this is the first study to investigate the walking outcome of the people with diabetes after the TTA. Only four previous studies evaluated walking outcomes after TTA [718192021]. However, amputation level, definition of walking outcome and time point of post-amputation evaluation were heterogenous among studies. Evans et al. [20] evaluated walking outcomes in 25 diabetic transtibial amputees with an average follow-up of 1,000 days after amputation. Sixteen patients (64%) were able to ambulate and it is relatively higher than that of our study. This difference could be due to different definitions of walking ability and follow-up evaluation. Evans et al. [20] and Nehler et al. [7] did not compare diabetic amputees with non-diabetic amputees. Therefore, the present study is the first to compare diabetic and non-diabetic amputees.
- Some limitations should be considered. First, this was a retrospective study. Thus, we could not evaluate extremity muscle strength, proprioception, cognitive function, or depression to assess the reasons for the different walking outcomes between groups. Second, our sample size was relatively small. Third, we did not evaluate long-term walking outcomes. Fourth, we could not exclude the effect of renal dysfunction on the results of this study. Renal dysfunction is reported the risk factor of muscle mass loss [21], and most of diabetes group in this study needed renal replacement therapy. However, most diabetic foot patients requiring major amputation are more likely to have chronic kidney disease, and both factors might have complicated effects on the outcome. Further studies to address these limitations are warranted.
- In conclusion, at 3 months after walking training with prostheses, significantly more non-diabetic amputees were capable of indoor/outdoor walking, compared with diabetic amputees. Our results may be useful for development of specific rehabilitation strategies after lower limb amputation.
DISCUSSION
-
Acknowledgements
- The present study was supported by a National Research Foundation of Korea grant funded by the Korean goverment (grant no. NRF-2019R1F1A1061348 and NRF-2019M3E5D1A02068242).
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS:
NOTES
- 1. Collin C, Wade DT, Cochrane GM. Functional outcome of lower limb amputees with peripheral vascular disease. Clin Rehabil 1992;6:13-21.ArticlePDF
- 2. Pohjolainen T, Alaranta H. Predictive factors of functional ability after lower-limb amputation. Ann Chir Gynaecol 1991;80:36-39. PubMed
- 3. Putting feet first in diabetes. Lancet 2005;366:1674.Article
- 4. Grodstein F, Chen J, Wilson RS, Manson JE. Nurses' Health Study. Type 2 diabetes and cognitive function in community-dwelling elderly women. Diabetes Care 2001;24:1060-1065. ArticlePubMedPDF
- 5. Sinclair AJ, Girling AJ, Bayer AJ. Cognitive dysfunction in older subjects with diabetes mellitus: impact on diabetes self-management and use of care services. All Wales Research into Elderly (AWARE) Study. Diabetes Res Clin Pract 2000;50:203-212. PubMed
- 6. Hamamura S, Chin T, Kuroda R, Akisue T, Iguchi T, Kohno H, Kitagawa A, Tsumura N, Kurosaka M. Factors affecting prosthetic rehabilitation outcomes in amputees of age 60 years and over. J Int Med Res 2009;37:1921-1927. ArticlePubMedPDF
- 7. Nehler MR, Coll JR, Hiatt WR, Regensteiner JG, Schnickel GT, Klenke WA, Strecker PK, Anderson MW, Jones DN, Whitehill TA, Moskowitz S, Krupski WC. Functional outcome in a contemporary series of major lower extremity amputations. J Vasc Surg 2003;38:7-14. ArticlePubMed
- 8. Roberts TL, Pasquina PF, Nelson VS, Flood KM, Bryant PR, Huang ME. Limb deficiency and prosthetic management. 4. Comorbidities associated with limb loss. Arch Phys Med Rehabil 2006;87(3 Suppl 1):S21-S27. ArticlePubMed
- 9. Webster JB, Hakimi KN, Williams RM, Turner AP, Norvell DC, Czerniecki JM. Prosthetic fitting, use, and satisfaction following lower-limb amputation: a prospective study. J Rehabil Res Dev 2012;49:1493-1504. ArticlePubMed
- 10. IJzerman TH, Schaper NC, Melai T, Meijer K, Willems PJ, Savelberg HH. Lower extremity muscle strength is reduced in people with type 2 diabetes, with and without polyneuropathy, and is associated with impaired mobility and reduced quality of life. Diabetes Res Clin Pract 2012;95:345-351. ArticlePubMed
- 11. Kalyani RR, Tra Y, Yeh HC, Egan JM, Ferrucci L, Brancati FL. Quadriceps strength, quadriceps power, and gait speed in older U.S. adults with diabetes mellitus: results from the National Health and Nutrition Examination Survey, 1999-2002. J Am Geriatr Soc 2013;61:769-775. ArticlePubMedPMCPDF
- 12. Perry J, Schoneberger B. Chapter 4, Ankle foot complex. Gait analysis: normal and pathological function. Thorofare: Slack; 1992. p. 51-87.
- 13. Raya MA, Gailey RS, Fiebert IM, Roach KE. Impairment variables predicting activity limitation in individuals with lower limb amputation. Prosthet Orthot Int 2010;34:73-84. ArticlePubMedPDF
- 14. Menz HB, Lord SR, St George R, Fitzpatrick RC. Walking stability and sensorimotor function in older people with diabetic peripheral neuropathy. Arch Phys Med Rehabil 2004;85:245-252. ArticlePubMed
- 15. Emam AA, Gad AM, Ahmed MM, Assal HS, Mousa SG. Quantitative assessment of posture stability using computerised dynamic posturography in type 2 diabetic patients with neuropathy and its relation to glycaemic control. Singapore Med J 2009;50:614-618. PubMed
- 16. Holt RI, de Groot M, Golden SH. Diabetes and depression. Curr Diab Rep 2014;14:491. ArticlePubMedPMCPDF
- 17. Schoppen T, Boonstra A, Groothoff JW, de Vries J, Goeken LN, Eisma WH. Physical, mental, and social predictors of functional outcome in unilateral lower-limb amputees. Arch Phys Med Rehabil 2003;84:803-811. PubMed
- 18. Houghton AD, Taylor PR, Thurlow S, Rootes E, McColl I. Success rates for rehabilitation of vascular amputees: implications for preoperative assessment and amputation level. Br J Surg 1992;79:753-755. ArticlePubMedPDF
- 19. Munin MC, Espejo-De Guzman MC, Boninger ML, Fitzgerald SG, Penrod LE, Singh J. Predictive factors for successful early prosthetic ambulation among lower-limb amputees. J Rehabil Res Dev 2001;38:379-384. PubMed
- 20. Evans KK, Attinger CE, Al-Attar A, Salgado C, Chu CK, Mardini S, Neville R. The importance of limb preservation in the diabetic population. J Diabetes Complications 2011;25:227-231. ArticlePubMed
- 21. Miller PD. Chronic kidney disease and osteoporosis: evaluation and management. Bonekey Rep 2014;3:542. ArticlePubMedPMC
REFERENCES
Walking outcomes with and without a cane in diabetic and non-diabetic amputees. Indoor/outdoor included walking outcome with and without cane. DM, diabetes mellitus. aSignificantly different between the diabetic and non-diabetic amputees, P<0.001.
 PubReader
PubReader ePub Link
ePub Link Cite
Cite